Contents
Poster Presentation - Oral Presentation
Patient Safety
Racial disparities in rate of central-line–associated bloodstream infections and catheter-associated urinary tract infections
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s84-s85
-
- Article
-
- You have access
- Open access
- Export citation
-
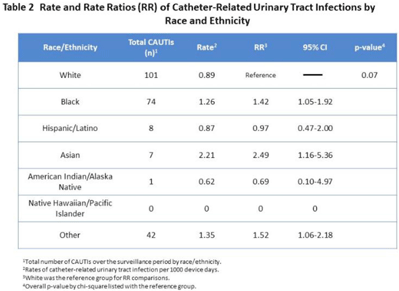
Background: Racial and ethnic disparities in healthcare access, medical treatment, and outcomes have been extensively reported. However, the impact of racial and ethnic differences in patient safety, including healthcare-associated infections, has not been well described. Methods: We performed a retrospective review analyzing prospectively collected data on central-line–associated bloodstream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI) rates per 1,000 device days. Data for adult patients admitted to an academic medical center between 2018 and 2021 were stratified by 7 racial and ethnic groups: non-Hispanic White, non-Hispanic Black, Hispanic/Latino, Asian, American Indian/Alaska Native, Native Hawaiian/Pacific Islander, and othe. The “other” group was composed of bi- or multiracial patients, or those for whom no data were reported. We compared the CLABSI and CAUTI rates between the different racial and ethnic groups using Poisson regression. Results: Compared to non-Hispanic White patients, the rate of CLABSI was significantly higher in non-Hispanic Black patients (1.27; 95% CI, 1.02–1.58; P < .03) and those in the “other” race category (1.79; 95% CI, 1.39–2.30; P < .001, respectively), and these trends increased in Hispanic/Latino patients (Table 1). Similarly, Black patients had higher rates of CAUTI (1.42; 95% CI, 1.05–1.92; P < .02), as did Asian patients (2.49; 95% CI, 1.16–5.36; P < .02), and patients in the “other” category (1.52; 95% CI, 1.06–2.18; P < .02) (Table 2). Conclusions: Racial and ethnic minorities may be vulnerable to a higher rate of patient safety events, including CLABSIs and CAUTIs. Additional analyses controlling for potential confounding factors are needed to better understand the relationship between race or ethnicity, clinical management, and healthcare-associated infections. This evaluation is essential to inform mitigation strategies and to provide optimum, equitable care for all.
Funding: None
Disclosures: None



Respiratory Viruses
Assessing alternatives to HEPA air purification requirements to reduce viral pathogen transmission in healthcare HVAC systems
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s85
-
- Article
-
- You have access
- Open access
- Export citation
Clinical factors associated with antibiotic de-escalation after a positive multiplex molecular respiratory panel
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s85-s86
-
- Article
-
- You have access
- Open access
- Export citation
-
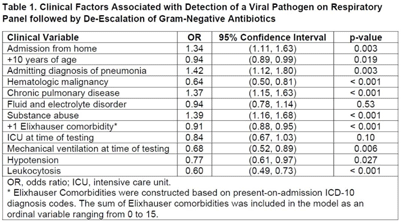
Background: Under ideal circumstances, multiplex molecular respiratory panels can support early all discontinuation of unnecessary antibiotics by facilitating diagnosis of viral infection. Our goal was to identify clinic situations in which a positive respiratory panel was associated with antibiotic de-escalation. We focused on gram-negative antibiotics in recognition of the urgent threat posed by gram-negative resistance. Methods: The sample included hospitalized adults tested by respiratory panel while receiving gram-negative antibiotics at the University of Maryland Medical Center from 2015 to 2020. Only the first respiratory panel performed during hospitalization was included. The primary outcome was the combination of a positive result on respiratory panel indicating detection of a viral pathogen and de-escalation of gram-negative antibiotics. De-escalation was assessed based on antibiotics administered on day 3 after testing and was defined by discontinuation or switch to an agent with a narrower spectrum of activity. Least absolute shrinkage and selection operator (LASSO) regression was used to construct the multivariable logistic regression model. Classification and regression tree (CART) analysis was used to identify subgroups with a higher likelihood of the primary outcome. Results: Of 8,326 patients, 1,462 (17.6%) tested positive by respiratory panel. The most common pathogen was rhinovirus (7.9% of the sample). Gram-negative–targeted antibiotics were de-escalated in 4,456 cases (53.5% of the sample), including 887 patients with a positive result on respiratory panel indicating a viral pathogen (60.7% of patients with a positive viral result). LASSO regression was used to select 12 variables (Table 1). Admitting diagnosis of pneumonia (OR, 1.42), comorbid substance abuse (OR, 1.39), chronic pulmonary disease (OR, 1.39), and admission from home (OR, 1.34) were associated with antibiotic de-escalation in conjunction with a positive respiratory panel. Leukocytosis (OR, 0.59), hematologic malignancy (OR, 0.64), mechanical ventilation at time of testing (OR, 0.68), and hypotension (OR, 0.77) were associated with decreased likelihood of antibiotic de-escalation in conjunction with a positive respiratory panel. CART analysis identified patients tested within 40 hours of admission as having a higher likelihood of a positive result in conjunction with antibiotic de-escalation. Among patients tested within 40 hours of admission, the probability of a positive result followed by antibiotic de-escalation was 11.9% (95% CI, 11.1%–12.8%). For patients tested >40 hours after admission, the probability was 6.0% (95% CI, 4.8%–7.2%). Conclusions: Targeted use of respiratory panel testing may increase the likelihood of an informative result that can drive decision making related to antibiotic use. Our exploratory analysis suggests that respiratory panel testing in the first 2 days
Funding: None
Disclosures: None

SSI
Characterization of MRSA and ESBL pathogens from patients with surgical-site infections in Accra, Ghana
-
- Published online by Cambridge University Press:
- 16 May 2022, p. s86
-
- Article
-
- You have access
- Open access
- Export citation
Surveillance/Public Health
Bacterial contamination on used face masks in healthcare personnel
-
- Published online by Cambridge University Press:
- 16 May 2022, pp. s86-s87
-
- Article
-
- You have access
- Open access
- Export citation
-
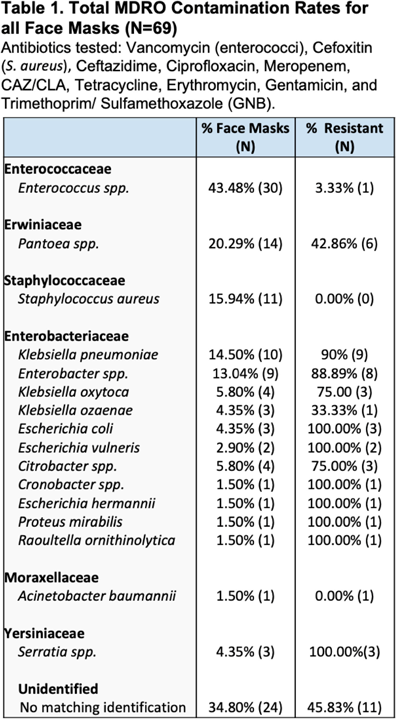
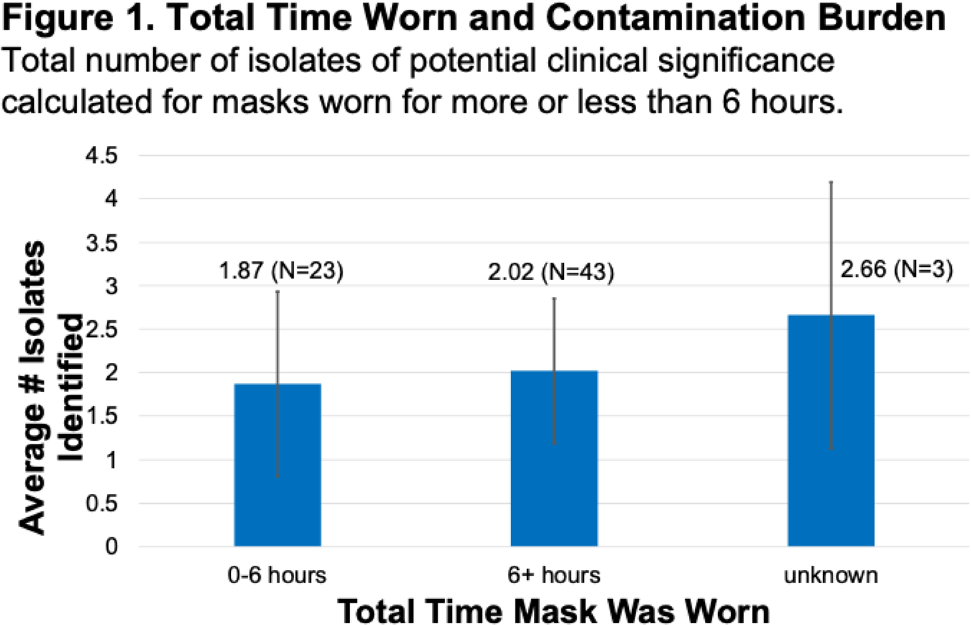
Background: Face masks have been worn universally and for long periods of time by healthcare personnel during the COVID-19 pandemic. They are frequently touched or adjusted with the hands and may come in contact with various surfaces and high-touch sites when taken off and on even briefly. These activities present opportunities for face masks to become contaminated with microorganisms. Nursing homes have high rates of multidrug-resistant bacteria and low PPE compliance; therefore, contamination of face masks in this setting may be of great interest. We investigated bacterial colonization status on used face masks in healthcare personnel, including assessing the presence of clinically important and multidrug-resistant bacteria. Methods: At a nursing home serving mostly post–acute-care patients, we collected 69 face masks from personnel at the end of the user’s work shift. Information about the mask and the user was also collected via a self-reported survey. Face masks were incubated in BHI broth overnight at 36°C and 10 μL was then plated on selective and differential plates. Methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), and gram-negative bacteria (GNB) resistant to several antibiotic classes were identified using standard microbiological methods. Resistance testing for cefoxitin (S. aureus), ciprofloxacin, meropenem, tetracycline, erythromycin, gentamicin, trimethoprim–sulfamethoxazole, and ceftazidime with and without clavulanic acid (gram-negative bacteria) was performed using the disc diffusion technique on Mueller-Hinton plates (Kirby Bauer). Results: The job categories of face mask users were competency-evaluated nursing assistant or nursing assistant (22.73%), nurse (12.12%), and other or administrative (37.88%). Overall face mask contamination rates for MRSA (0%) and VRE (3.3%) were low; however, methicillin-susceptible S. aureus was found on 11 masks (15.9%). High contamination and resistance rates were found for gram-negative bacteria, with 113 isolates. Among them, 69 (60.9%) were resistant to at least 1 antibiotic, most commonly was erythromycin (59.4%). Additionally, higher rates of clinically important pathogenic gram-negative bacteria were identified: 14.3% of masks were contaminated with Klebsiella pneumoniae, 13.0% were contaminated with Enterobacter spp, and 4.2% were contaminated with Escherichia coli. Importantly, there were no significant differences in the total number of isolates of potential clinical significance recovered from masks worn >6 hours versus those worn <6 hours. Conclusions: Among nursing-home healthcare workers, face masks were often contaminated with multiple organisms, including potentially pathogenic bacteria and antibiotic-resistant gram-negative organisms. This contamination may pose a risk for transmission if face masks are not properly used and/or disposed of after wearing. Prolonged duration of face-mask wearing, however, was not associated with increased contamination rates.
Funding: None
Disclosures: None