



Case report
A 37-year-old woman underwent routine obstetric ultrasound examination at 20 weeks’ gestation at our institution. She had consulted elsewhere and had been given a poor prognosis for her pregnancy, as the foetus showed an abnormally shaped left ventricle and a hyperechogenic endocardium, and endocardial fibroelastosis was suspected. As our team had previously diagnosed two patients with this malformation, Reference Ruiz Martín, Ortiz Garrido, Zabala Argüelles and Urbano Carrillo1 we were familiar with the key features of Isolated left ventricular apical hypoplasia.
Both ventricles showed a normal contractile function. Heart rhythm was normal. A specific feature (not reported in older patients) found in this foetus was a hyperechogenic endocardium restricted to the interventricular septum. This characteristic became gradually less evident as the pregnancy evolved. After discussing with the parents the suspected diagnosis and the evidence shown in the literature about possible outcomes, the pregnancy was continued, and an asymptomatic 3720 g girl was delivered at 40 weeks of gestation. Follow up showed absence of symptoms, with good weight gain and no other health issues. Close cardiological follow-up with serial echocardiographic evaluations revealed a systolic left heart function in the lower limit, with an left ventricle ejection fraction of 55%. Other echocardiographic parameters indicated a preserved left ventricular function (biphasic mitral inflow, normal inflow from left ventricle to the ascending aorta and aortic arch, and right-left flow through the foramen ovale). She is currently asymptomatic at one year of age.
Discussion
First described in 2004, Reference Fernandez-Valls, Srichai, Stillman and White2 and although being a very rare heart malformation, an increasing number of case reports are being published Reference Liao, Jin, Miao and Huang3,Reference Bassareo, Duignan, James, Dunne, McMahon and Walsh4 in recent years in adults and children, as clinicians are getting aware of its existence.
In the adult, symptoms can range from the asymptomatic patient to patients with heart failure and rhythm anomalies, such as atrial fibrillation. Reference Liao, Jin, Miao and Huang3–Reference Román, Anchante, Menacho and Medina5 Paediatric cases have also been reported. Reference Ruiz Martín, Ortiz Garrido, Zabala Argüelles and Urbano Carrillo1,Reference Liao, Jin, Miao and Huang3–Reference Marin, Sanchez, Maroto, Ossaba, Ruiz and Zabala6
Foetal reports of this malformation are exceptional, possibly in part because of lack of diffusion of the features of this rare heart malformation among obstetricians, or because it might evolve during pregnancy.
Detailed description of the anatomy of the normal foetal heart and its correlation with prenatal echocardiography can be found in the literature. Reference Picazo-Angelin, Zabala-Argüelles, Anderson and Sánchez-Quintana7
In the normal heart, the ventricular apex is formed by the left ventricle (Figure 1). In contrast to the normal heart, in isolated left ventricular apical hypoplasia, the apex of the heart will not be formed by the left ventricle, but by the apex of the right ventricle (Figure 2). The foetal ultrasound will include key echocardiographic features such as an elongated right ventricle wrapping around the deficient left ventricular apex, a spherical left ventricle, and abnormal papillary muscles’ origin from the left ventricular apex. Reference Román, Anchante, Menacho and Medina5 We add a specific feature in the foetus, not described in post-natal life: a hyperechogenic interventricular septum (Figure 2).
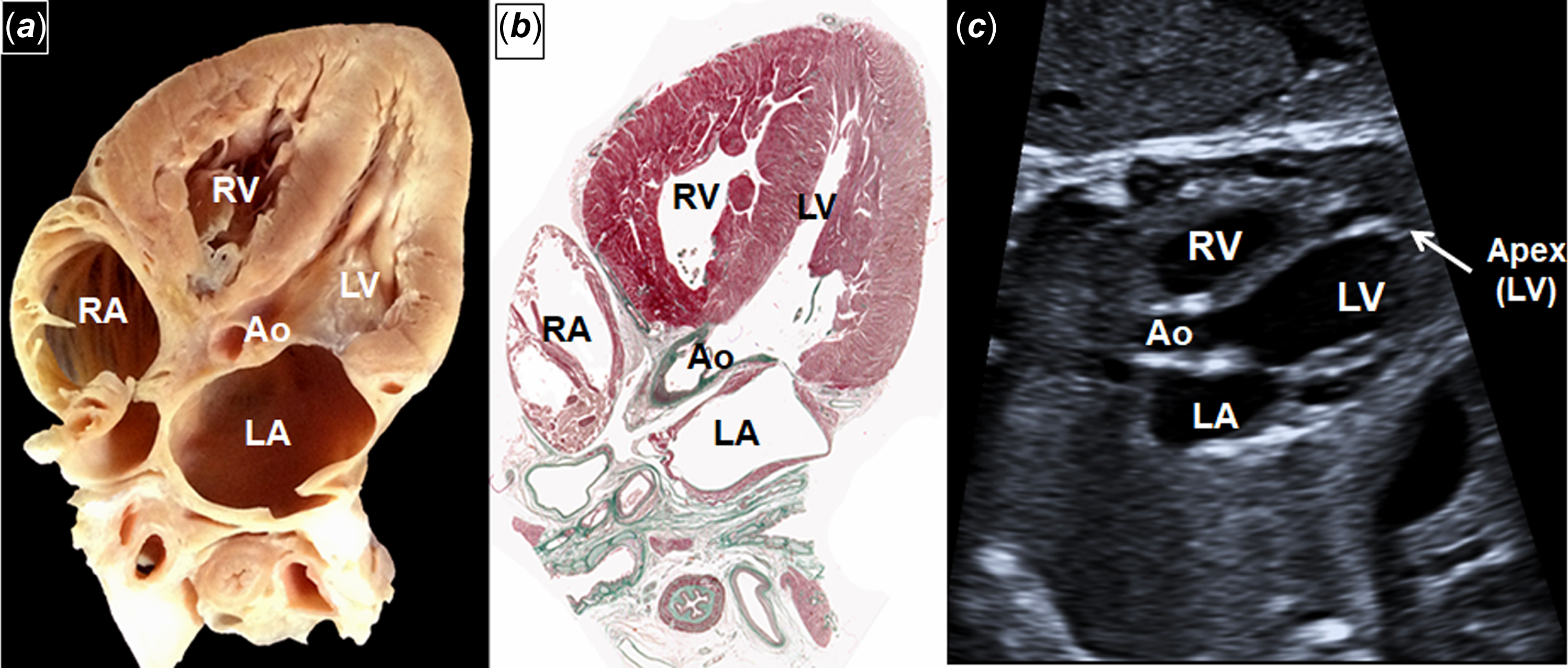
Figure 1. A composite of dissection ( a ), histological section ( b ), and normal foetal echocardiography ( c ) showing a NORMAL left ventricular apex. The normal apex of the heart is formed by the left ventricle. Ao: Aorta, RA: Right atrium, LA: Left atrium, RV: Right ventricle, LV: Left ventricle.
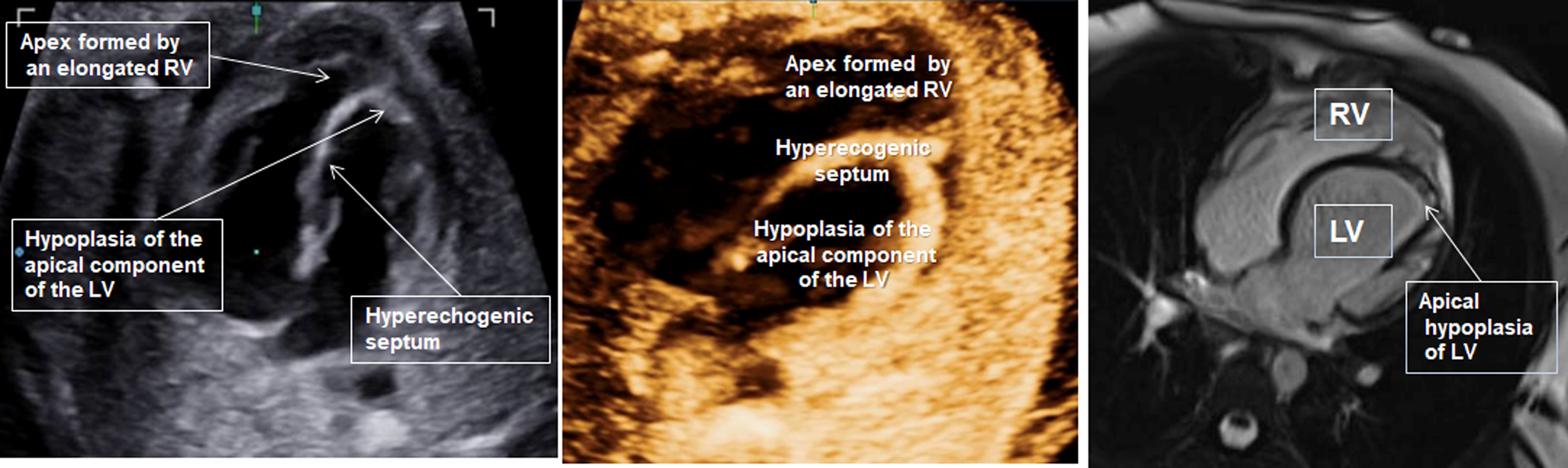
Figure 2. To compare with Figure 1, here is depicted an ABNORMAL left ventricular apex with hypoplasia of the apical component of the LV, the apex of the heart being formed by the elongated right ventricle that wraps around the left ventricle, and the feature we add to the previously described, a hyperechogenic interventricular septum as seen in the foetal scan (left). The apex of the heart in Isolated Left Ventricular Apical Hypoplasia (ILVAH) is formed by the right ventricle. These features can be enhanced by 3D Echocardiography (centre) and cardiac MRI (right).
Differential diagnosis should include hypoplastic left heart syndrome, endocardial fibroeslastosis, Reference Yan, Zhou and Zhang8 and aneurysm of the left ventricle. To look for the wrapping of the right apex around the missing left apex (Figure 2) and the hyperechogenic septum will be two valuable clues for the diagnosis in the foetus.
Information to the family needs to include the fact that it is a rare and not well-known heart malformation with an uncertain evolution, which frequently goes unnoticed, and that most cases described in the literature in young people remain asymptomatic, with symptoms such as heart failure and rhythm disturbances developing in adulthood, generally responding to medical treatment.
A prenatal consult with a paediatric cardiologist is advised, and follow up during childhood needs to be scheduled. Cardiac MRI (Figure 2) is becoming a valuable tool in order to follow up the ventricular function in these patients, and it offers additional information, such as the imaging of fatty tissue at the hypoplastic apex. Reference Meléndez, Muñoz and Meave9
The aim of this paper is to draw attention to this abnormal development of the left ventricle, as the use of foetal echocardiography for screening expands worldwide.
Many of us have learned from our teachers and mentors in medical school that “the eyes cannot see what the mind does not know.” Now we know.
Acknowledgements
We thank Prof. Dr Damian Sanchez-Quintana for the macroscopic anatomical and histological imaging.
Author contribution
B.P.A. drafted the manuscript, G.C.R. provided clinical care, and A.O.G. provided cardiac MRI imaging. All authors participated in the care of the patient and have read and approved the final version of the manuscript.
Financial support
Funding for open access charge: Universidad de Málaga.
Competing interests
The authors declare none.
Ethical standard
The authors confirm that consent for submission and publication of this case report has been obtained from the patient.
hashtag PedsCards. Suggested tweet: ILVAH: how to spot it.



 Open access
Open access