



Introduction
Cancer is a leading cause of global mortality, accounting for approximately 9·7 million deaths in 2022 alone. Reference Bray, Laversanne and Sung1 Radiotherapy is a critical component of comprehensive cancer care, recommended for about 50% of patients, either as a standalone treatment or in combination with other therapies for curative or palliative purposes. Reference Atun, Jaffray and Barton2,Reference Yaromina, Krause and Baumann3 However, access to radiotherapy is significantly limited in low- and middle-income countries (LMICs). Reference Abdel-Wahab, Bourque and Pynda4,Reference Atun, Jaffray and Barton5 According to the International Atomic Energy Agency (IAEA), many African countries have limited access to advanced radiotherapy equipment, with fewer than 10% of the continent’s healthcare facilities equipped with linear accelerators. 6 In Africa, where approximately 70% of countries rely on cobalt-60 machines for cancer treatment, Reference Makasi, Mwanza and Kamanzi7 radiation protection practices are critical.
Cobalt-60, a radioactive isotope commonly used in external beam radiotherapy (EBRT), remains the primary source of radiation in many sub-Saharan African countries due to its cost-effectiveness and simpler technology compared to linear accelerators. Reference Makasi, Mwanza and Kamanzi7 However, the relatively lower energy of cobalt-based radiation and its associated treatment techniques require effective radiation shielding to ensure treatment precision, especially in settings where advanced quality control systems are lacking. Modern radiotherapy machines employ multi-leaf collimators for the shielding of critical structures. However, radiotherapy centres that still have cobalt-60 therapy machines in service typically rely on shielding blocks composed of Cerrobend.
Shielding blocks are critical in protecting healthy tissues during EBRT, making their efficacy vital for patient safety. Cerrobend, a low-melting-point alloy, is commonly used for custom radiation shielding due to its excellent attenuation properties, ease of fabrication, and affordability. Reference Das, McGee and Cullip8 It is composed of 50% bismuth, 10% cadmium, 13·3% tin and 26·7% lead. Reference Iftikhar, Wazir and Kakakhail9–Reference Iftikhar, Ali and Shahid11 Cerrobend shielding blocks are custom-made for each patient, according to treatment-specific needs, taking beam divergence into consideration. It has a low fusion temperature of about 70 °C which makes it easy to handle, recycle and cast into many different shapes. Cerrobend has largely replaced lead as a shielding material primarily because of the environmental toxicity of the latter. The interaction between electron beams and pure lead produces bremsstrahlung radiation which reduces the efficiency of pure lead as a shielding material, thus increasing the risk of exposure of radiotherapy staff and patients to harmful radiation. The ability of a shielding block to attenuate the radiation going through it is quantified by the transmission factor which is defined as the ratio between the absorbed dose at a certain point of a blocked field and the absorbed dose at the same point in an open field. It accounts for both primary radiation (originating directly from the beam) and dispersed radiation (scattered prior to reaching the patient or scattered within the patient). The performance of Cerrobend blocks depends on factors such as material composition, block thickness and beam energy. An optimal shielding block should limit radiation transmission to 5% or less, a standard necessary to ensure patient safety and therapeutic efficacy. Reference Khan and Gibbons12
Budget constraints and limited access to advanced technologies in LMICs demand cost-effective and reliable EBRT-shielding solutions. Reference Akudugu, Dauda and Adu-Gyamfi13 Despite the extensive use of Cerrobend in sub-Saharan Africa, studies on its attenuation properties under local conditions are scarce, leaving critical gaps in knowledge regarding its effectiveness in these settings. Reference Iftikhar, Ali and Shahid11 This knowledge gap presents a challenge to achieving optimal radiation protection and treatment accuracy at radiotherapy centres in sub-Saharan Africa, where cobalt-60 teletherapy machines are commonly used.
This study employed a quantitative experimental design to evaluate the attenuation efficacy of Cerrobend shielding blocks of varying thicknesses using cobalt-60 beams at a leading cancer treatment centre in sub-Saharan Africa. It aimed to establish the optimal block thickness required to achieve a 95% attenuation threshold, providing practical and evidence-based insights to improve radiation protection standards in resource-constrained settings. This work complements recent research on radiotherapy safety and infrastructure challenges in LMICs (Zubizarreta et al., 2021; Muren et al., 2023).
Methods
Study setting
The research was a quantitative experimental study conducted at the National Radiotherapy, Oncology, and Nuclear Medicine Centre (NRONMC), Korle Bu Teaching Hospital, Ghana. The centre was established in 1997 and is currently the largest of three radiotherapy centres in the country, serving as a leading oncology referral hub in the West African subregion. The centre is equipped with a 1·25 MeV cobalt-60 teletherapy machine (Equinox) and a 6 MV linear accelerator (Varian) for the delivery of EBRT.
Materials and instruments
The materials utilized in the study included Cerrobend shielding blocks of varying thicknesses (1 cm, 2 cm, 3 cm, 4 cm and 5 cm) for attenuation testing. A 0·6 cm3 plexiglass ionization chamber was used for precise radiation intensity measurements, whereas an electrometer was used to record the output from the ionization chamber (Figure 1). Perspex was used to hold and stabilize the shielding blocks during experiments, while a barometer and thermometer were employed to monitor and maintain consistent environmental conditions throughout the study.
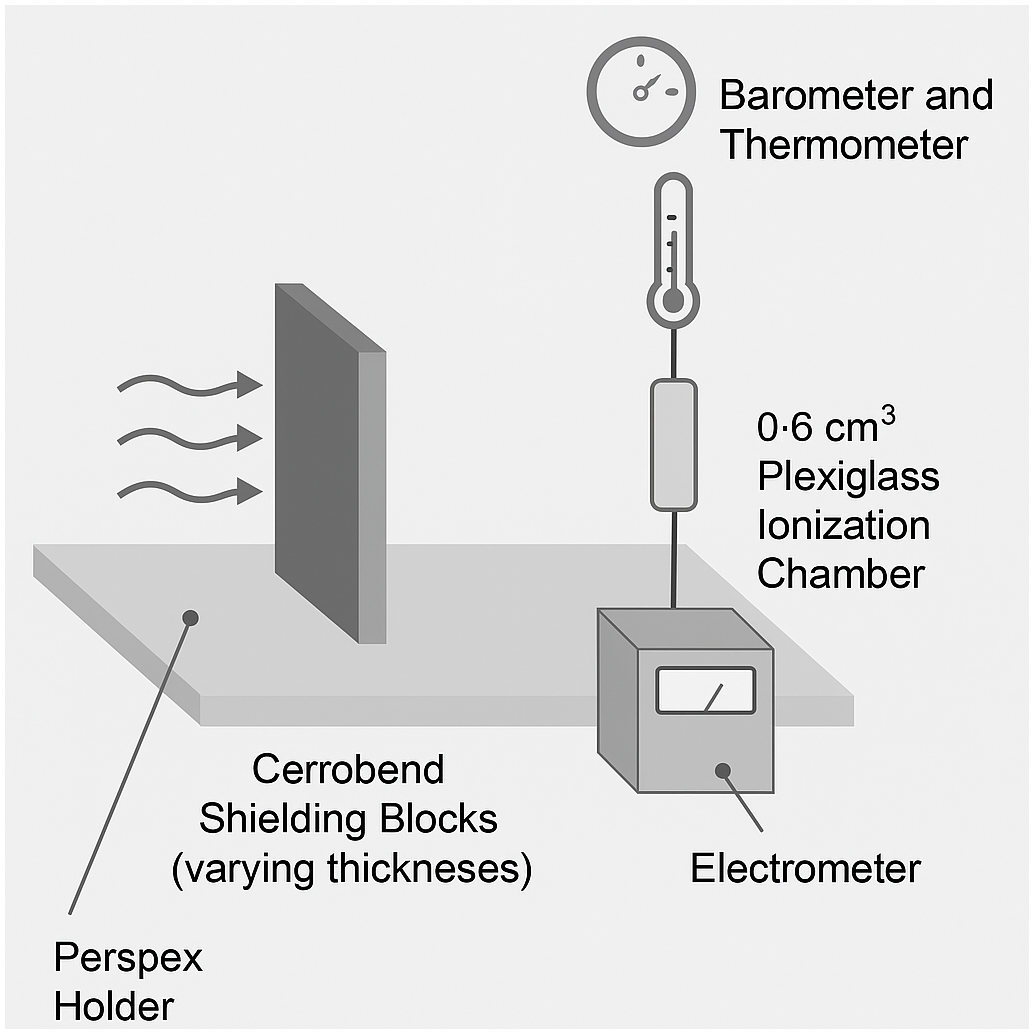
Figure 1. Schematic diagram of the experimental setup showing the Cerrobend shielding blocks, ionization chamber, electrometer, and supporting Perspex stand.
Variables
-
The intensity transmitted through the Cerrobend shielding blocks was determined as follows:
 $${I_t} = {I_o}{e^{ - \mu t}}$$
$${I_t} = {I_o}{e^{ - \mu t}}$$
-
where,
-
It = intensity transmitted through an attenuator of thickness (t)
-
Io = intensity with no attenuator present (constant)
-
µ = linear attenuation coefficient
-
t = thickness of the attenuator
-
• Percentage transmission (X) of radiation through each block thickness was calculated using the formula: X = (It/I0) × 100%.
-
• The thickness required for 5% maximum transmission (t5%) was calculated using the formula: [t5% = ln (0.05)/−μ]
Experimental procedure
The experimental procedure was designed to evaluate the attenuation properties of Cerrobend shielding blocks at varying thicknesses. The study was conducted in a controlled environment ensuring that radiation safety protocols were rigorously adhered to. The experiment began with the preparation and calibration of the ionization chamber and electrometer. The ionization chamber was prewarmed before each series of measurements to eliminate residual charges from prior exposures. This step ensured that the chamber’s readings were unaffected by stray charges, providing accurate and reliable baseline measurements. Calibration checks were performed to ensure the accuracy of the equipment, and all instruments were stabilized in the experimental environment for at least 15 min prior to using them.
Cerrobend shielding blocks of five different thicknesses (1 cm, 2 cm, 3 cm, 4 cm, and 5 cm) were prepared and mounted on Perspex trays. A fixed radiation field size of 10 cm × 10 cm was set and maintained throughout all measurements to ensure consistency. To establish a baseline measurement, the intensity of the radiation (I0) was first measured without any shielding block in place. The ionization chamber with a buildup cap was positioned at a distance of 1 m from the radiation source, while the source-to-tray distance was maintained at 0·05 m as depicted in Figure 2. The buildup cap ensured that accurate readings were taken by accounting for the required radiation dose for detector equilibrium in low-energy regions, improving measurement accuracy. This configuration minimized scatter before the radiation reached the shielding block and reduced interference from scattered radiation when measuring transmitted intensity. The measurements were conducted for each thickness of Cerrobend shielding block in turn. After placing a shielding block on the Perspex tray, the radiation source was activated for a standardized exposure time of 60 s. The transmitted intensity (It) was recorded by the ionization chamber, and five independent readings were taken for each block to ensure consistency and reproducibility.
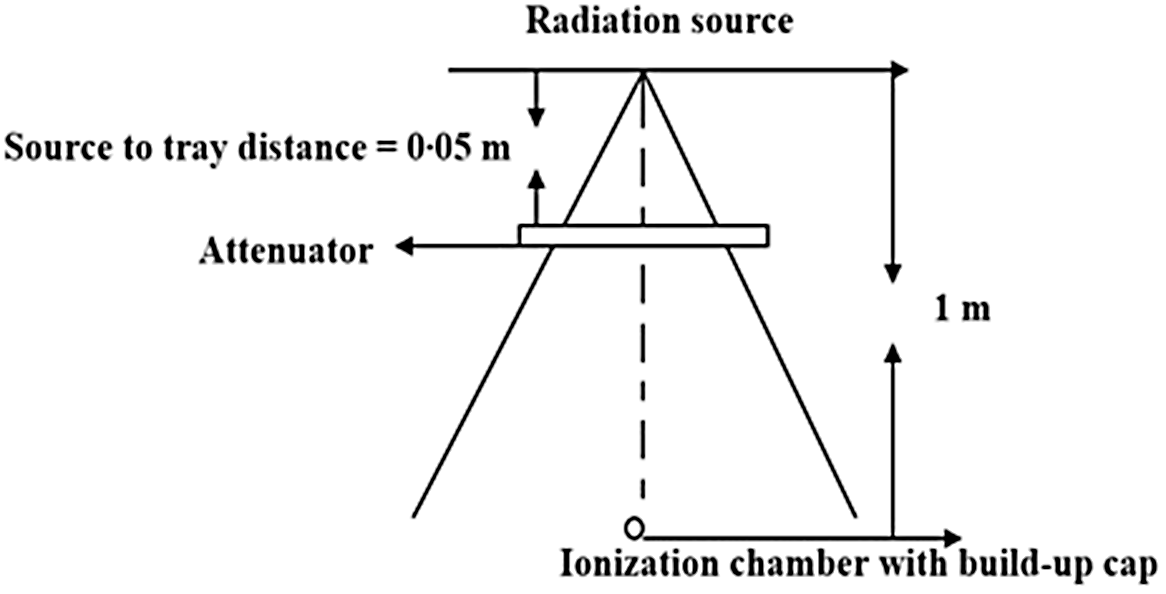
Figure 2. Set-up for measuring the intensity of radiation passing through Cerrobend blocks. The short distance from the source to the tray (0·05 m) was to ensure that radiation was not scattered before reaching the tray whereas the wide distance between the source of radiation and the ionization chamber (1 m) was to ensure that the readings would not be influenced by scattered radiation.
Between each measurement, the equipment was reset, and the ionization chamber was briefly prewarmed to maintain stable conditions. Environmental conditions, including temperature and pressure, were closely monitored throughout the experiment. A digital thermometer and barometer were used to measure these parameters, and a constant temperature of 25 °C and pressure of 100·95 kPa were maintained to prevent fluctuations that could influence the readings. Corrections for minor variations in environmental conditions were applied to standardize the data. The careful design and execution of the experimental procedure ensured the collection of accurate and reliable data, forming a solid foundation for the study’s conclusions.
Data collection and analysis
The data for each thickness of shielding block, including baseline intensity (I0) and transmitted intensity (It), were meticulously recorded in an Excel workbook immediately after each measurement. To ensure accuracy, the average intensity values for each block thickness were calculated by averaging the five repeated readings per block. This approach minimized random errors and provided a robust dataset for further analysis. This dataset was used to determine the percentage transmission, linear attenuation coefficient, and optimal thickness for achieving a 5% transmission level. To determine the effectiveness of each shielding block, the percentage transmission (X) of radiation through each block thickness was calculated (X = It/I0 × 100). The resulting values quantified the degree of attenuation provided by each thickness, forming the basis for subsequent calculations and interpretations. The linear attenuation coefficient (μ), a key parameter in assessing shielding efficacy, was determined by plotting the natural logarithm of the transmitted intensity against the corresponding block thickness. Linear regression analysis was performed to fit the data and determine the slope of the line, which corresponds to the negative value of the linear attenuation coefficient. The strength of this linear relationship was validated by calculating the coefficient of determination (R2), with values close to 1·0 confirming the high linearity of the attenuation data. The thickness of Cerrobend required for 5% radiation transmission (t5%) was then calculated, providing a theoretical estimate of the optimal block thickness to achieve the desired attenuation level. To ensure consistency and reliability, standard deviations were calculated for the repeated readings of each block thickness, allowing an assessment of measurement variability. Additionally, statistical tests, such as t-tests, were conducted to compare the experimental results with theoretical predictions, further validating the findings. All calculated values, including percentage transmission, linear attenuation coefficient and optimal thickness for 5% transmission, were organized into comprehensive tables for clarity.
Quality control
To ensure the reliability and validity of the study’s findings, robust quality control measures were implemented at every stage of the experiment. These quality control measures collectively minimized errors, enhanced reproducibility and ensured that the results accurately represented the attenuation characteristics of Cerrobend shielding blocks under controlled conditions. The ionization chamber and electrometer were calibrated according to international standards, specifically IAEA TRS-398, before the data collection process began. Calibration was performed at a secondary standard dosimetry laboratory to ensure the accuracy of dose measurements. Additionally, routine cross-checks were conducted using a reference dosimeter to confirm the consistency of the readings.
Prewarming the ionization chamber ensured the elimination of any residual charges that could influence subsequent readings. The chamber was allowed to stabilize under experimental conditions for a minimum of 15 min to ensure accurate measurements. Environmental parameters such as temperature and pressure were continuously monitored to ensure environmental stability. The electrometer was regularly verified against a standard test voltage to confirm its operational accuracy prior to the study. Additionally, the alignment of the radiation source and shielding blocks was checked routinely to prevent misalignment that could alter the beam path and distort the results. Manual cross-verification of results was carried out to confirm the accuracy of the findings. For independent validation, preliminary results were compared with theoretical calculations and existing literature to validate the findings. Furthermore, an independent physicist reviewed the experimental setup and measurement procedure to ensure that the methodology was sound and that the results were reliable. A detailed logbook was maintained throughout the experiment, documenting each step of the process, including equipment setup, calibration and measurement readings. After completing the measurements, an internal audit was conducted to verify adherence to the experimental protocol, ensuring that all quality control measures were followed meticulously.
Ethical considerations
Ethical approval for this study was obtained from the institutional review board, ensuring that the research adhered to established ethical standards and guidelines. While the study did not involve human subjects, ethical considerations were observed to uphold safety and integrity in the use of radiation. All procedures were conducted in compliance with international radiation safety standards, including the International Atomic Energy Agency (IAEA) guidelines, to minimize potential risks to researchers and the environment. Radiation exposure during the study was limited to controlled laboratory settings, and proper protective measures, such as lead shielding and personal dosimeters, were utilized to safeguard researchers from unnecessary exposure. Experimental materials and waste were handled and disposed of according to institutional and national radiation safety regulations.
Results
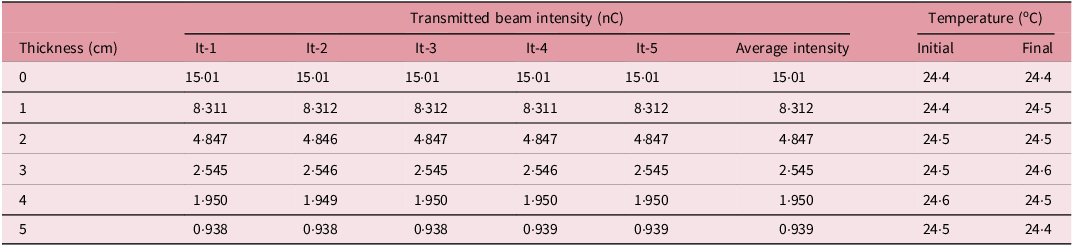
Table 1 provides detailed measurements of transmitted beam intensities through Cerrobend blocks of varying thicknesses, highlighting the attenuation characteristics of the material. Measurements (It-1 through It-5) showed remarkable consistency across all trials, indicating high precision in the experimental setup. The transmitted intensity decreased as the thickness of the Cerrobend blocks increased, with the average transmitted intensity dropping from 15·01 nC at 0 cm thickness to 0·939 nC at 5 cm thickness. This trend illustrates the exponential attenuation of the beam as it passes through increasing material thickness. Temperature variations were minimal, ranging between 24·4 °C and 24·6 °C, ensuring that temperature fluctuations have a negligible impact on the transmitted intensity measurements. This dataset is indicative of the material’s capability to attenuate radiation effectively and supports further quantitative analysis, such as calculating attenuation coefficients or modelling the exponential attenuation behaviour.
Table 1. Measured transmitted intensities through various thicknesses of Cerrobend blocks
nC: nanoCoulombs.
The graph in Figure 3 shows a linear relationship between the natural logarithm of transmitted intensity (y-axis) and the thickness (cm) of Cerrobend (x-axis). The data points closely align with the regression line, represented by the equation y = −0·5386x + 2·6705, where the slope (−0·5386) indicates the rate of decrease in the natural logarithm of transmitted intensity per unit increase in thickness. The positive intercept (2·6705) represents the value of the natural log of transmitted intensity when the thickness is zero. The coefficient of determination (R2 = 0·992) suggests that 99·2% of the variation in the natural logarithm of transmitted intensity is explained by the thickness of the Cerrobend shielding block, demonstrating a very strong linear correlation between these variables. The negative slope confirms that as the thickness increases, the transmitted intensity decreases exponentially, consistent with the behaviour of radiation attenuation.
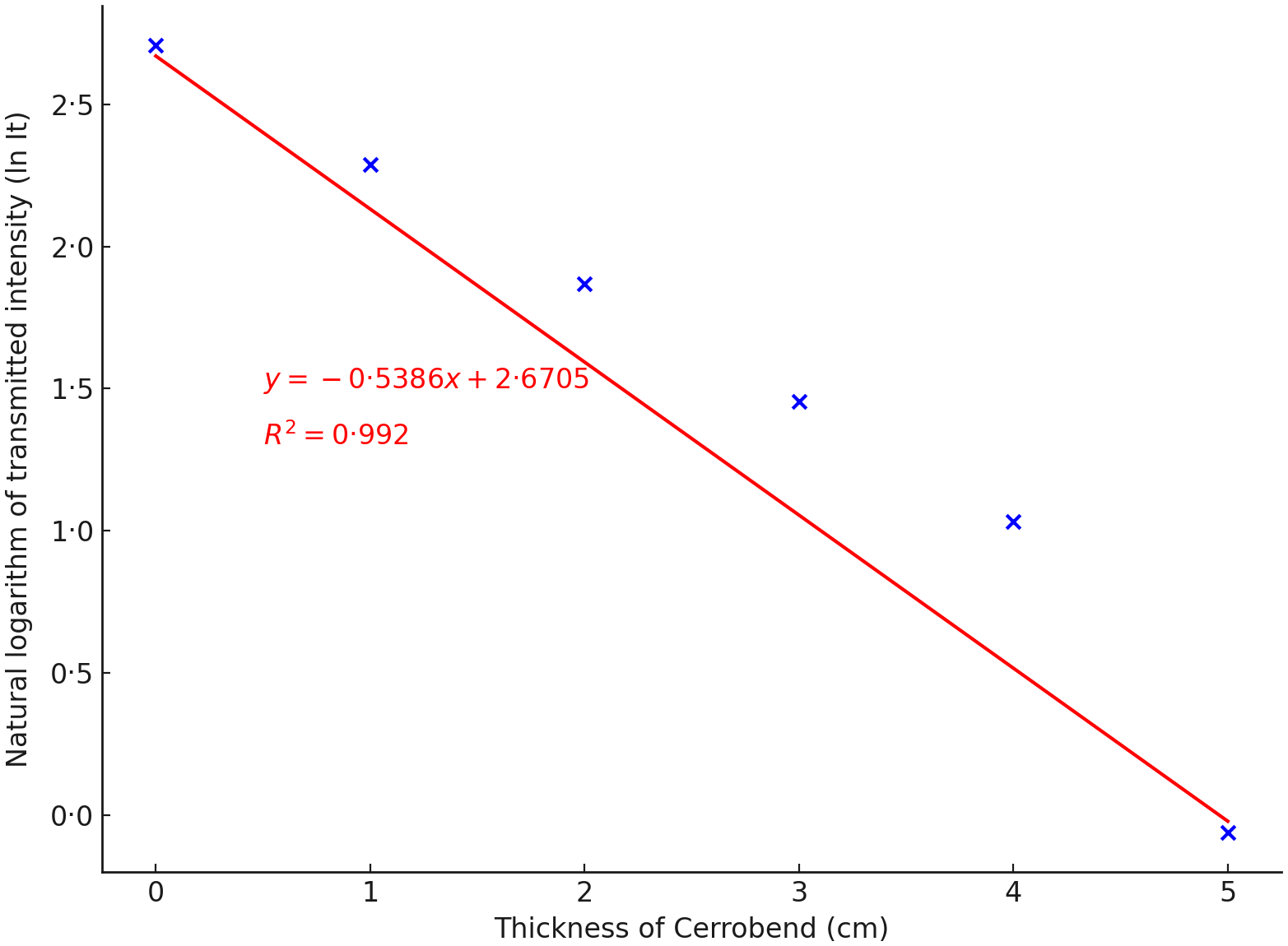
Figure 3. Attenuation curve. Relationship between the natural logarithm of transmitted intensity and thickness of Cerrobend shielding blocks. The negative slope of the regression line indicates exponential attenuation.
Figure 4 presents the percentage transmission of radiation through Cerrobend blocks of varying thicknesses (ranging from 0 cm to 5 cm). As the thickness of the Cerrobend block increases, the percentage transmission decreases sharply, demonstrating the material’s effectiveness in attenuating radiation. At 0 cm (no shielding), transmission is near 100%, but by 5 cm thickness, transmission drops to approximately 8·02%. This graph highlights that even relatively modest increases in thickness significantly enhance shielding, particularly at lower thickness levels.
Figure 4. Percentage transmission of radiation through Cerrobend blocks of varying thicknesses.
Table 2 summarizes the data for the Pearson’s product moment correlation coefficient, showing the relationship between the natural logarithm of transmitted intensity (Y) and thickness (X) in centimetres. As X increases, Y generally decreases, with the values of Y declining from 2·7087 at X = 0 to –0·0629 at X = 5, before rising sharply to 7·9438 at X = 15.
Table 2. Pearson’s product moment correlation coefficient for the graph of the natural log of transmitted intensity against thickness (centimeters)
X = thickness (cm), Y = (log-transmitted intensity), X² = the squared value of X, Y² = the squared value of Y, and XY = the product of X and Y.
The required thickness for a maximum transmission of 5% was determined to be 6 cm whereas the percentage transmission of a 5 cm thickness Cerrobend block (routinely used at NRONMC) was calculated to be 8·02%.
Discussion
The study evaluated the attenuation efficacy of Cerrobend shielding blocks used in EBRT at a leading radiotherapy centre in sub-Saharan Africa. The findings provide crucial insights into optimizing radiation protection practices in resource-constrained settings, where access to advanced shielding technologies. Specifically, the results provide evidence-based guidance for selecting optimal shielding-block thicknesses in resource-constrained environments. The results highlight the exponential attenuation of radiation intensity as the thickness of Cerrobend increases, with average transmitted intensity decreasing from 15·01 nC at 0 cm to 0·939 nC at 5 cm thickness. This attenuation pattern is consistent with the Beer–Lambert law, which describes the exponential reduction of beam intensity with increasing material thickness. Reference Attix15 The study’s regression analysis (y = −0·5386x + 2·6705) demonstrates a strong linear correlation (R2 = 0·992) between the natural logarithm of transmitted intensity and Cerrobend thickness, underscoring the reliability and reproducibility of the observed attenuation behaviour.
The results align with findings from previous studies, which emphasize the high attenuation efficiency of Cerrobend shielding blocks in minimizing radiation exposure. Podgorsak (2005) observed similar trends in attenuation, reporting the suitability of Cerrobend for shaping radiation beams and protecting critical structures. Reference Podgorsak16 Chung et al. (2023) investigated the attenuation properties of low melting point alloys and confirmed that Cerrobend exhibits superior attenuation efficiency, particularly at photon energies typical of radiotherapy, due to its high density and homogeneity. Reference Chung, Kim and Lee17 Their study reported an attenuation coefficient comparable to that calculated from this study’s regression line slope (−0·5386 cm−1), reinforcing the reliability of the present results.
The study’s calculated percentage transmission for a 5 cm block (8.%) corroborates earlier results from another study that demonstrated photon transmission rates of 5–8% through Cerrobend blocks, depending on beam energy and block density. Reference Varian and Stanford18 Notably, the study determined that a thickness of 6 cm is required to achieve the recommended 95% attenuation standard, consistent with guidance from Khan (2014), who emphasized the importance of meeting this threshold to optimize radiation protection. Reference Khan and Gibbons12 Further corroborating the significance of Cerrobend, Moghadam et al. (2022) evaluated various shielding materials and reaffirmed that Cerrobend remains a cost-effective and effective alternative to pure lead, particularly in clinical settings where precision and customizability are crucial. Reference Moghadam, Aghamiri and Koosha19
The study findings have significant implications for radiation protection in EBRT, particularly in low-resource settings where cobalt-60 teletherapy is prevalent. The observed consistency of transmitted intensity measurements (It-1 through It-5) and the minimal temperature fluctuations (24·4 °C to 24·6 °C) reflect the robustness of Cerrobend blocks under varying clinical conditions. Establishing a standard thickness of 6 cm for achieving 95% attenuation provides evidence-based guidance for improving shielding practices. This recommendation is particularly relevant considering the study’s finding that the routinely used 5 cm blocks at the facility allow 8% transmission, exceeding the 5% safety threshold. Revisiting and revising standard practices to adopt thicker blocks where necessary would enhance both patient and staff safety by minimizing potential radiation exposure.
Additionally, Moghadam et al. (2022) found similar exponential attenuation behaviour, with percentage transmissions dropping sharply as thickness increased, akin to the drop from 100% to 8·02% observed in this study for a 5 cm block. Reference Moghadam, Aghamiri and Koosha19 In the broader context of radiation protection, this study reinforces the principle of justification and optimization outlined by IAEA. 20,21 Justification requires that the benefits of radiotherapy outweigh potential radiation risks, while optimization ensures that exposure is as low as reasonably achievable (ALARA) while meeting clinical objectives. The use of Cerrobend blocks exemplifies this balance by allowing precise shaping of the therapeutic beam while shielding critical organs and minimizing scattered radiation. However, the finding that the current standard practice at the study centre does not fully meet the 5% maximum transmission threshold highlights an opportunity for improvement. As part of quality assurance programmes, there should be regular testing and quality control of shielding blocks to confirm their attenuation performance, particularly in limited-resource settings where variability in material properties may occur. Also, Zamanian et al. (2021) explored radiation attenuation for therapeutic X-ray applications and demonstrated that a 6-cm Cerrobend shield could reduce transmission to below 5%, validating this study’s projection that 6 cm is required for maximum shielding efficacy under the 5% transmission threshold. Reference Zamanian, Ghorbani and Aslani22
The study holds particular significance in the context of clinical radiation safety and dosimetry, as it empirically determines the attenuation curve of Cerrobend and identifies a critical shielding threshold of 6 cm for achieving less than 5% transmission. This provides actionable guidelines for medical physicists engaged in treatment planning and radiation protection. The minimal influence of temperature variations further affirms the robustness and repeatability of the experimental setup. Importantly, the study raises critical questions about material variability and quality control in the production of Cerrobend blocks—differences in alloy composition or manufacturing processes could affect attenuation efficiency and result in inconsistent shielding performance. Future investigations should explore these factors to ensure reliability and also extend to evaluating Cerrobend’s attenuation characteristics under different beam modalities, such as electrons or protons, which are increasingly relevant in modern radiotherapy. Additionally, the study encourages the exploration of cost-effective alternatives to Cerrobend, such as tungsten or other high-density materials, which may offer comparable or superior attenuation in cobalt-60 teletherapy. Finally, the comprehensive transmission data and regression analysis presented here provide a solid foundation for future modelling and Monte Carlo simulations of radiation transport, supporting the development of optimized shielding strategies for diverse clinical applications.
Limitations
The study was limited to Cerrobend’s performance in a laboratory setting, and the results may not fully reflect its behaviour in clinical environments with varying geometries and patient-specific factors. Therefore, future studies should explore Cerrobend’s effectiveness in clinical settings, taking into account factors such as patient anatomy and treatment plans. Another limitation is the absence of direct comparisons with other shielding materials, which could provide a more comprehensive understanding of Cerrobend’s relative effectiveness. While environmental factors such as temperature and pressure were controlled during the study, real-world variations in environmental conditions could impact Cerrobend’s attenuation properties. Further studies should investigate how fluctuations in environmental parameters may influence the material’s performance in different settings.
Conclusion
This study underscores the critical role of Cerrobend shielding blocks in radiation protection during EBRT. By quantifying the attenuation characteristics of Cerrobend and establishing a standard thickness for optimal shielding, the findings contribute to evidence-based improvements in radiotherapy practices. However, the observed discrepancy between current practices and recommended standards highlights the need for enhanced quality assurance and updated clinical guidelines to ensure optimal patient and staff safety. These results serve as a foundation for further research and policy development aimed at advancing radiation protection in sub-Saharan Africa and other similar limited-resource settings. Future studies on shielding for cobalt-60 teletherapy should include additional thicknesses beyond 5 cm, assessing the effects of material variability and exploring the attenuation properties of Cerrobend for other radiation modalities such as electron or proton beams.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Financial support
This study did not receive any specific funding support from funding agencies in the public, commercial or not-for-profit sectors.
Competing interests
The authors declare no competing interest.







 Open access
Open access