



Introduction
Sexual satisfaction (SS) is important for overall well-being. It has been strongly linked to various individual and interpersonal benefits, including mental and physical health (e.g., Carlsson-Lalloo et al., Reference Carlsson-Lalloo, Berg, Rusner, Svedhem and Mellgren2022), quality of life (e.g., Chao et al., Reference Chao, Lin, Ma, Lai, Ku, Kuo and Chao2011), subjective well-being/happiness (e.g., Buczak-Stec et al., Reference Buczak-Stec, König and Hajek2019; Chernyavska et al., Reference Chernyavska, Yermakova, Kokorina, Kolot and Kremenchutska2022) and relationship satisfaction (e.g., Herzberg et al., Reference Herzberg, Wildfang and Quittschalle2022). Recognized for its positive impact on sexual health and well-being, SS serves as a valuable indicator of an individual’s health status and subjective sense of well-being. It not only refers to the absence of sexual issues but also (and more importantly) reflects the extent to which an individual can derive pleasure and fulfillment from healthy sexual experiences. In this study, we define SS as the subjective overall experience derived from an individual’s assessment of how effectively their desires, needs, and expectations—both solitary and with a partner—are met through sexual activity. This covers a range of multifaceted experiences, including pleasure, joy, well-being, and happiness across physical, emotional, and cognitive dimensions (Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2022).
Given that SS is a potential consequence of sexual behaviors (SBs), understanding the predictors of SBs has attracted considerable research interest. The reciprocal influence between knowledge, beliefs, attitudes, and behaviors has been widely investigated. For instance, some meta-analyses have examined the causal relationships between attitudes and behavior, particularly how positive attitudes can lead to healthier SBs (e.g., Albarracín et al., Reference Albarracín, Gillette, Earl, Glasman, Durantini and Ho2005; Glasman & Albarracín, Reference Glasman and Albarracín2006; Sheeran et al., Reference Sheeran, Maki, Montanaro, Avishai-Yitshak, Bryan, Klein and Rothman2016). Additionally, some have explored the relationship between knowledge, beliefs, and behavior, highlighting the role of informed beliefs in shaping SBs (e.g., Albarracín et al., Reference Albarracín, Gillette, Earl, Glasman, Durantini and Ho2005; Sheeran et al., Reference Sheeran, Abraham and Orbell1999). Furthermore, research has shown the impact of knowledge and beliefs on behavior and attitudes toward such behavior (e.g., Glasman & Albarracín, Reference Glasman and Albarracín2006), and emphasized the importance of enhanced knowledge for facilitating behavioral change (e.g., Fonner et al., Reference Fonner, Armstrong, Kennedy and Sweat2014). Regarding sexual health and self-efficacy, individuals’ judgments about their confidence in their ability to execute a behavior and accomplish the desired consequences (Bandura, Reference Bandura1977) have emerged as strong predictors of behavioral outcomes, including those aiming at health improvement (Leman et al., Reference Leman, Mora and Gandes2021; Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno, García-Pérez, Liñán-González and Godoy-Izquierdo2024). Self-perceptions of efficacy have been shown to determine the enactment of SBs, and their correlation with social-cognitive variables such as knowledge, beliefs, and attitudes has been consistently demonstrated (e.g., Mahat et al., Reference Mahat, Scoloveno and Ayres2014; Montanaro & Bryan, Reference Montanaro and Bryan2014). Sexual self-efficacy (SSE), defined as confidence in one’s ability to make decisions and take actions regarding sexuality—especially when faced with barriers and obstacles (Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2023)—plays an important role in an individual’s control over their sexual lives (Assarzadeh et al., Reference Assarzadeh, Khalesi and Jafarzadeh-Kenarsari2019).
Therefore, previous research has established a relationship between knowledge, beliefs, attitudes, and SSE and the role of these factors in SBs. However, to the best of our knowledge, studies have yet to explore these variables concerning not only preventive but also health-promoting SBs or their association with SS from a positive perspective, especially among women.
This study aims to investigate whether distinct configurations of psychosocial predictors—namely, knowledge, beliefs, attitudes on sexuality, and SSE—are differentially associated with SBs and SS as outcome variables. Our goal is to identify profiles of women exhibiting similar cognitive–motivational and sexual health patterns. Additionally, we aim to explore the characteristics of these configurations concerning sociodemographic, sexuality-related, and other psychosocial factors. This relationship is important because sociodemographic factors such as age, gender, educational level, socioeconomic status, and religiosity can significantly influence individual expressions and experiences of sexuality (Giménez-García et al., Reference Giménez-García, Castro-Calvo and Gil-Llario2020; Sánchez-Fuentes et al., Reference Sánchez-Fuentes, Santos-Iglesias and Sierra2014). By examining how the identified profiles correlate with these variables, we can gain insights into factors that may shape women’s SBs and SS. While research is contradictory regarding levels of SS among women (Giménez-García et al., Reference Giménez-García, Castro-Calvo and Gil-Llario2020; Sánchez-Fuentes et al., Reference Sánchez-Fuentes, Santos-Iglesias and Sierra2014), there is a trend to growing research on gender and sexuality beyond sexual functioning (e.g., sexual health, pleasure), particularly among women. In addition, research such as the present one is beyond the traditional, gendered classification of masculine sexuality and SS as being more dependent or focused on the rewarding and pleasurable physical dimensions of sexual activity, and feminine ones more centered on relational and emotional aspects. To our knowledge, no prior study has conducted such a profile analysis, so our hypotheses are not based on previous evidence. However, some studies have used this analytical procedure to predict other behavioral outcomes, such as the use of oral contraception (e.g., Dempsey et al., Reference Dempsey, Johnson and Westhoff2011) or changes in sexual risk behaviors such as unprotected intercourse (e.g., Kalichman et al., Reference Kalichman, Cain, Knetch and Hill2005). Other studies have used SBs to cluster individuals and determine attitudes toward condom use and SSE in relation to both consenting to condom use and refusing unsafe sex within these clusters (e.g., Gomes & Nunes, Reference Gomes and Nunes2015). Given this evidence, we expected to find distinct configurations, including at least one group with a schema reflecting an appropriate cognitive–motivational foundation for behavior, another group with a poor or dysfunctional background, and an intermediate group differing from the other two profiles. Moreover, we expected these profiles to exhibit varying relationships with SBs and SS as external criteria, i.e., sexual health outcomes. Specifically, we anticipated that the first profile would demonstrate higher levels on both outcomes. In contrast, the second profile would exhibit the lowest levels on both outcomes, and the third one would display intermediate levels. As others have pointed out previously (e.g., Sánchez-Fuentes et al., Reference Sánchez-Fuentes, Santos-Iglesias and Sierra2014), there is a reduced number of theoretical explanatory models on SS, and studies such as the present one, through the combination of several variables, may offer insights about the complexity of SS among young and adult women, contributing to its understanding and future theoretical and applied research as well as clinical practice.
Methods
Participants
An initial sample (N = 1,877) was recruited voluntarily through non-probabilistic sampling. Eleven cases were excluded based on methodological criteria (e.g., determined by researchers’ tests). Additionally, 512 individuals did not respond to the main measures, and 274 were eliminated for not meeting the inclusion criteria, i.e., self-identified female gender, aged between 18 and 50 years, residing in Spain for at least 1 year (either Spanish or foreign nationality) and being able to read and write in Spanish. The decision to recruit women within the 18–50 age range was based on their exposure to significant social, political, and cultural developments following the establishment of democracy in Spain. Moreover, this age range was expected to exclude menopausal and postmenopausal status based on previous findings in Spain (Dam et al., Reference Dam, Van der Schouw, Onland-Moret, Groenwold, Peters, Burgess and Butterworth2019; Larroy et al., Reference Larroy, Marin Martin and López-Picado2020), which can be key factors influencing female sexuality. Exclusion criteria also included suffering from any severe physical or mental disease. Finally, four outlier cases identified during preliminary analyses (below) were removed from the database.
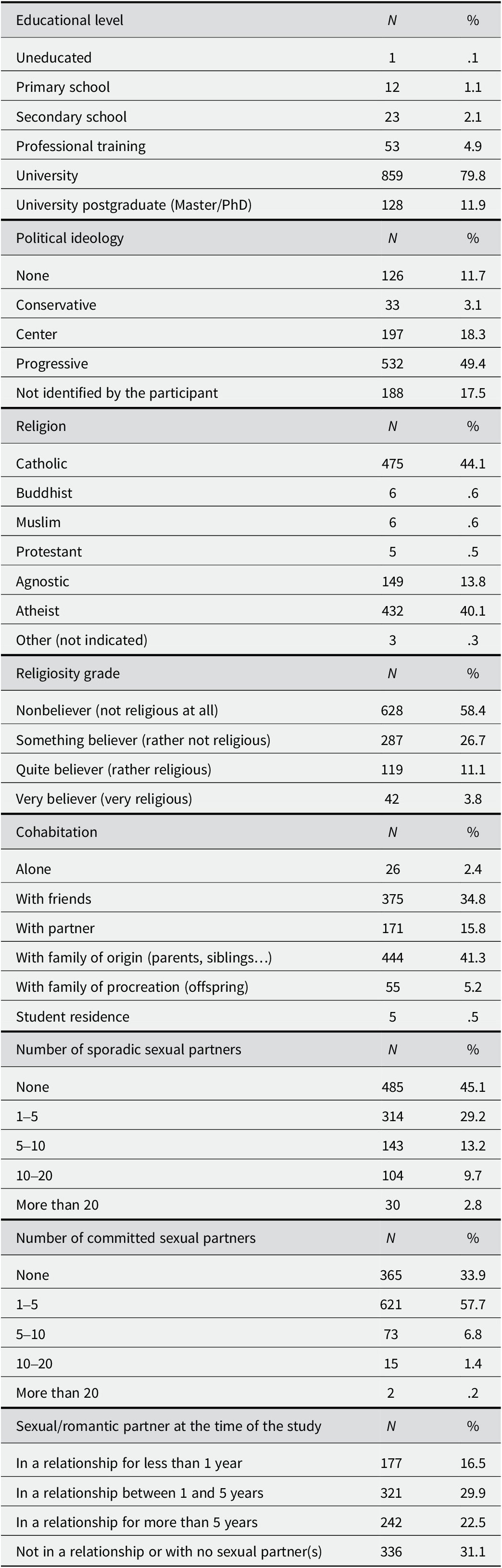
The final study sample comprised 1,076 women aged 18–50 years (M = 24.47; SD = 6.11). Among them, 1,046 (97.2%) were Spanish citizens born and raised in Spain, while 30 participants (2.8%) were of European, Latin American, or Asian origin, with the majority having lived in Spain for a significant portion of their lives (98.6%). Cultural influences from foreign participants were therefore expected to be minimal. Regarding sexual orientation, 80.4% identified themselves as heterosexual, 13.1% as bisexual, 3.2% as lesbian, and 3.3% had not fully defined their sexual orientation. Additionally, 68.9% reported having a sexual partner(s) at the time of the study. Further details about participants’ characteristics, including educational level, religiosity, and sexual and intimate relationship experiences, are presented in Table 1.
Table 1. Sociodemographic and personal data (N = 1,076)
Measures
Based on a previously used semi-structured interview and the findings obtained (Ogallar-Blanco et al., Reference Ogallar Blanco, Godoy Izquierdo, Vázquez Pérez and Godoy García2017) as well as various published measurement tools that were reviewed and considered incomplete for our purposes, the following measures were used.
(A) Sexual knowledge: This was assessed using 20 true/false/unknown items regarding sexuality, reproduction, and sexually transmitted diseases (STDs). The average was calculated to obtain a total score, with higher values indicating greater knowledge. Similar tools have been employed in previous studies (e.g., Sümer, Reference Sümer2015). To establish reliability, we chose not to use the typical internal consistency coefficients, as the items do not assess a single trait or show homogeneity of scores. Instead, we employed Guilford and Fruchter’s formula (Reference Guilford and Fruchter1978, p. 431), yielding a reliability coefficient of .88.
(B) Sexual beliefs: We evaluated beliefs concerning women’s sexual roles, contraceptive methods, and SBs using a 25-item instrument with responses given on a 4-point Likert-type scale (0 = strongly disagree to 3 = strongly agree). The average score was obtained to indicate a total score, with higher values indicating more accurate and less biased beliefs. Katz-Wise and Hyde (Reference Katz-Wise and Hyde2015) have employed similar ad hoc measures. The internal consistency of this measure was Cronbach alpha = .67. Notably, removing any item did not improve the reliability beyond .68. This moderate reliability could indicate the broad diversity of topics included, which are not necessarily intercorrelated.
(C) Sexual attitudes: We evaluated attitudes toward sexuality, contraceptive methods, masturbation, intercourse, oral and anal sex, and sexual orientation using 81 items with a 4-point Likert-type response scale (0 = strongly disagree to 3 = strongly agree). The average was calculated to obtain a total score, with higher scores indicating more positive attitudes toward sexuality. Other studies (e.g., Katz-Wise & Hyde, Reference Katz-Wise and Hyde2015; Wright & Bae, Reference Wright and Bae2015) have used similar measures. The internal consistency was Cronbach Alpha = .86.
(D) Sexual self-efficacy: This was measured using the original Spanish version of the Sexual Self-Efficacy Questionnaire (SSEQ) (Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2023). This is a bidimensional measure, with 10 items measuring the SSE for health promotion actions and 10 items assessing SSE for preventive actions. All 20 items used a Likert-type response scale from 0 = not at all confident to 4 = very confident. Average scores were calculated, with higher values indicating greater SSE. The Cronbach alpha values were .88, .84, and .90 for the subscales SSE for promotion, SSE for prevention, and total SSE, respectively, indicating strong internal consistency. Previous studies have also reported adequate psychometric characteristics for this measure (Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2023).
(E) Sexual behaviors: Participants provided self-reports on the usual frequency of engaging in 25 solitary SBs (e.g., masturbation, fantasy) and activities with a partner(s) (e.g., kissing, practicing intercourse) using a Likert-type scale (0 = I have never done it, 3 = I do it very frequently). Additional items assessed behaviors related to sexuality, such as communication (0 = No, never to 4 = Always), initiative-taking within the relationship (0 = Always my partner to 4 = Always me), and the use of fantasies (0 = Never to 3 = Always). Finally, participants reported on the use of contraceptive methods (0 = Never to 5 = Always). Given the asymmetry in the response scale, the scores for all items and subdomains were summed to obtain an SB summation variable, with higher scores indicating a higher frequency of the assessed SBs. All items were taken from expert judgments and professional and research sources (e.g., Brown, Reference Brown and Gellman2020; Levay & Valente, Reference Levay and Valente2006). Given the nature of this self-report, no psychometric analyses were conducted. Other studies have used similar frequency-based measurement tools (e.g., Carrobles et al., Reference Carrobles, Gámez-Guadix and Almendros2011; Katz & Schneider, Reference Katz and Schneider2015).
(F) Sexual satisfaction: We employed the original Spanish version of the Sexual Satisfaction Comprehensive Index (SSCI) (Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2022) consisting of 4 face-valid items assessing both actual and desired SS during individual-solitary and partnered activities. Responses were provided on a Likert-type scale (0 = Not satisfactory/Not interested, 3 = Very satisfactory). Including desired SS allows us to ascertain the variance between participants’ current satisfaction levels and their desired levels. An average score was calculated to determine overall SS, with higher scores denoting greater levels of SS. This metric reflects the satisfaction derived from sexual experiences and the extent of deviation from desired levels. Higher levels of SS are indicated when actual satisfaction is high and the discrepancy between actual and desired satisfaction is low. Conversely, lower levels of SS are suggested when there is a high discrepancy, or both satisfaction and discrepancy are low, thus penalizing current satisfaction and providing a more realistic assessment of SS. Previous studies have reported adequate psychometric characteristics for this measure (Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2022), and the Cronbach alpha value for this sample was .93.
In addition, other data from the participants were collected regarding their sociodemographic and health characteristics (e.g., self-reported time since last menstruation, following clinical standards on reproductive condition; Harlow et al., Reference Harlow, Gass, Hall, Lobo, Maki and Rebar2012) and sexual experience (see Table 1).
Procedure
The assessment protocol was made available online through Limesurvey® by Limesurvey GmbH, Germany. It was also publicized through various channels, including online platforms (such as social networks of psychology and sexology professionals) and traditional media (such as direct requests for participants to share or participate), to recruit a nationwide sample.
On the first page of the online protocol, participants were provided with information regarding the confidentiality of their responses, the exclusive use of their data for scientific purposes, their rights, and details about the study. Access to the survey was granted only after participants provided informed consent. No feedback or compensation was offered for participation.
Following data collection, the database was downloaded and thoroughly checked for accuracy. Ethical approval for the study was obtained from the Ethics Committee on Human Research of the University of Granada, with registration number CEFM-44521-0511.
Study Design and Data Analyses
This is a descriptive, correlational study with a cross-sectional design. Preliminary and exploratory data analyses were conducted to identify and rectify potential errors in data entry, missing data, or outliers. No univariate outliers were detected, but four multivariate outliers (identified through Mahalanobis distance test) were observed and subsequently removed from the database (N = 1,076). Following this, assumptions of normality and homoscedasticity were verified, and descriptive statistics and Pearson’s correlation analyses were conducted. To determine distinct profiles based on participants’ knowledge, beliefs, attitudes regarding sexuality, and SSE, a multivariate nonhierarchical k-means cluster analysis was performed, employing the Euclidean distance as a measure of similarity (Jain et al., Reference Jain, Murty and Flynn1999). We utilized this analysis to maximize within-group homogeneity and promote clear separation among configurations or clusters while minimizing between-group homogeneity. Prior to the analysis, raw scores were transformed into standardized scores (Z). We followed the criteria published by Clatworthy et al. (Reference Clatworthy, Buick, Hankins, Weinman and Horne2005) for using and reporting cluster analyses in Health Psychology. To determine the appropriate number of clusters, we calculated the pseudo-F index (PSF) (Calinski & Harabasz, Reference Calinski and Harabasz1974), which is considered the most efficient statistic for determining the goodness of fit of the cluster solution (Milligan & Cooper, Reference Milligan and Cooper1985). The optimal solution was determined by identifying the number of clusters with the greatest PSF. Moreover, we used Goodman–Kruskal’s λ index (where values closer to 0 indicate better variable performance in configuring the clusters). We also considered the percentage of cases correctly classified, with higher percentages indicating better clustering accuracy. Additionally, we adopted the suggestion by Clatworthy et al. (Reference Clatworthy, Hankins, Buick, Weinman and Horne2007) to consider three groups, as this number of clusters is commonly observed in Health Psychology research. Nevertheless, we explored alternative solutions, such as two- or four-cluster models. We based our final decision on the values of the above-mentioned indexes, the accuracy of the classification, as well as the solution with more meaningful compositions. This examination of multiple criteria reinforces the robustness of the selected cluster solution.
Further, a discriminant analysis was conducted using all variables involved in the cluster analysis to identify the most influential variables for achieving optimal clustering. Additionally, an initial univariate ANOVA was performed to investigate differences among the clusters for all variables, aiding in selecting the most relevant variables for creating the profiles. After establishing configurations (clusters), ANOVAs and pairwise t-tests were conducted to explore differences between profiles.
Next, we conducted univariate one-way ANOVAs and multiple pairwise comparisons to explore differences among the multidimensional profiles in relation to two outcomes: SBs and SS. Both indicators were used as criterion variables to cross-validate the identified cluster solution (i.e., external validation; Clatworthy et al., Reference Clatworthy, Buick, Hankins, Weinman and Horne2005) and as outcome variables to explore the expected differences in sexual health as a consequence of the different psychosocial configurations.
The criterion for establishing high, moderate (average), or low values for each subscale was ±0.5 standard deviations (SD) of the Z scores. Therefore, scores within ±0.5 SD of the standardized mean indicated moderate differences from the z-mean. Scores higher than ±0.5 SD indicated large differences, while scores below ±0.5 SD were considered to indicate small differences (Dezutter et al., Reference Dezutter, Waterman, Schwartz, Luyckx, Beyers, Meca and Hardy2014). Since the clusters were defined using Z scores for the entire sample, each cluster’s standardized mean reflects the extent to which that cluster deviates from the mean score of the total sample, standardized to zero, and from the means of the other clusters. The distance between the clusters’ means (and between each cluster mean and the total sample mean) can be interpreted as an index of effect size in standard deviation units. Similar to Cohen’s d (Reference Cohen1988), a difference of .2 SD represents a small effect size, .5 SD represents a moderate effect size, and .8 SD represents a large effect size.
Finally, ANOVAs and independent samples Student’s t-tests were conducted to explore differences between the clusters in terms of sociodemographic variables.
It is important to note that cluster analysis techniques are particularly sensitive to outliers and multicollinearity. Before transforming the data into Z scores, as previously mentioned, univariate and multivariate tests confirmed the absence of outliers. Additionally, no evidence of multicollinearity was found (all variables had a variance inflation factor (VIF) < 10 and a tolerance index >0.1; the condition index, a robust test of multicollinearity, was very low for all variables). Consequently, none of the variables were excluded from the cluster analysis.
Data analyses were conducted using SPSS 22.0. The significance level was set at p < .05.
Results
The mean values (raw scores) obtained for knowledge and beliefs were moderate, with slightly higher scores for positive attitudes. For all three variables, the low standard deviation indicated high homogeneity among the participants (see Table 2). The mean SSE scores regarding preventive and health promotion actions were considerably high, with standard deviations also reflecting homogeneity among participants. In contrast, the mean score for SBs was moderately low, with a notable low variability between subjects indicated by the standard deviation. Finally, SS had a high mean score and a low standard deviation. Pearson’s correlation analyses (see Table 2) revealed correlations between knowledge, beliefs, attitudes, and SSE for preventive and health promotion actions. SBs showed correlations with all psychosocial variables. SS correlated with all variables, although only marginally with knowledge (for all, p < .05).
Table 2. Participants (raw) scores and bivariate zero-order correlations for all variables
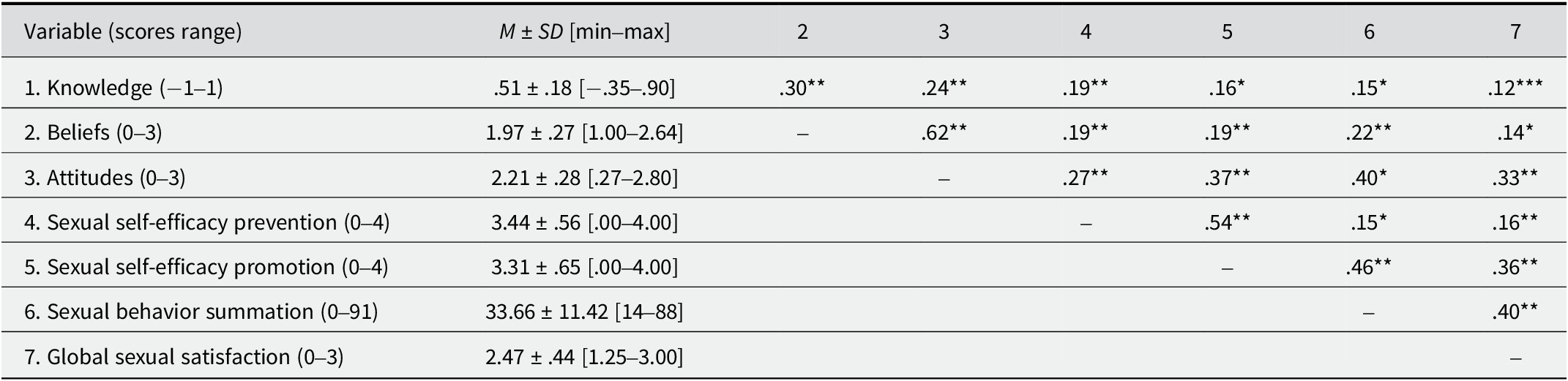
** p < .01, * p < .05, *** p < .10
To explore configurations of psychosocial predictors of SBs, including knowledge, beliefs, attitudes regarding sexuality, and SSE, a k-means cluster analysis was conducted using these cognitive–motivational indicators as variables to configure the profiles. Given the absence of previously published empirical evidence, we tentatively explored solutions with two, three, and four clusters. We chose the three-cluster solution for several reasons: it exhibited a higher percentage of correctly grouped participants in each cluster, it provided the most informative outcome with the fewest clusters (enhancing parsimony), it did not assign a small number of atypical cases to a cluster (improving replicability), and it offered a more straightforward and meaningful conceptual interpretation. Additionally, this three-cluster solution was supported by optimal values for the PSF and λ indices and the percentage of cases correctly classified. A preliminary ANOVA confirmed significant differences between the clusters for all configuring variables (p < .001). Thus, all variables were retained for subsequent analyses.
Furthermore, a discriminant analysis confirmed the fit of the solution provided by the cluster analysis. It revealed significant between-group differences and demonstrated high discriminative power, with minimal variance in the discriminant scores unexplained by the differences between profiles. The Wilks’ lambda indices of canonical discriminant functions for the global model were .168 (χ 2 = 383.032, p < .001) and .499 (χ 2 = 149.114, p < .001), indicating substantial discrimination between groups. The full discriminant function explained 100% of the variability among groups, with 66.1% and 33.9% explained by each function. Using the three-cluster solution, 95.9% of cases were correctly classified.
Thus, three clusters were identified, each characterized by a different configuration of the cognitive–motivational predictors included in the study (Figure 1). Based on these profiles, we labeled the configurations as follows: high cognitive–motivational resources and high SSE (Cluster I), low cognitive–motivational resources and moderate SSE (Cluster II), and low cognitive–motivational resources and low SSE (Cluster III).
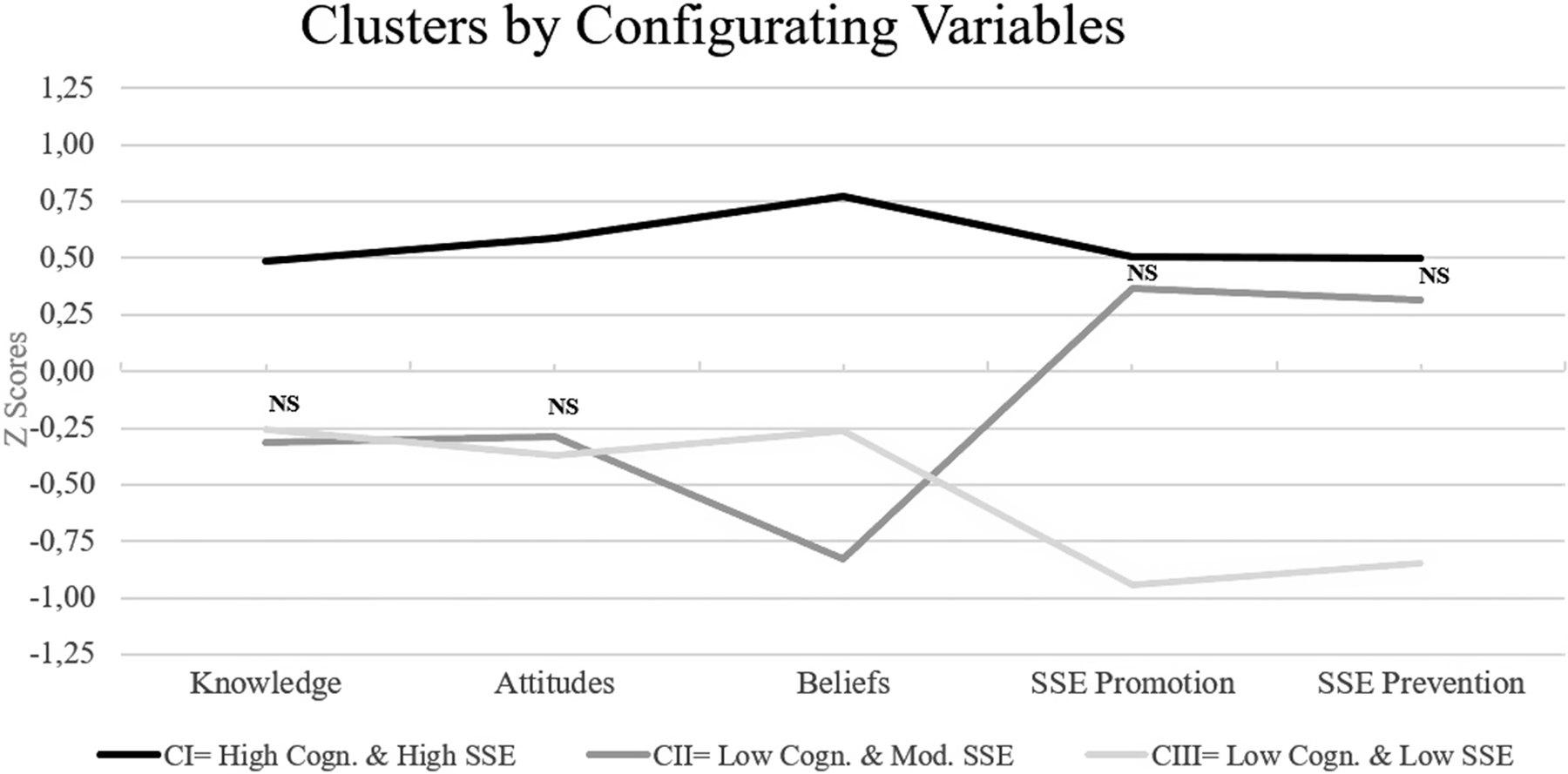
Figure 1. Graphical representation (centroids for Z scores) of the profiles identified in the cluster analysis.
Note. Cluster I is composed mainly of women with high levels of cognitive–motivational resources and high sexual self-efficacy; Cluster II consists primarily of women with low levels of cognitive–motivational resources and moderate sexual self-efficacy; and Cluster III includes women with low levels of cognitive–motivational resources and low sexual self-efficacy. All the comparisons were significant (p < .01), except for those labeled as NS, indicating nonsignificant differences.
Cluster I (43.2%) comprised participants whose knowledge, beliefs, and attitudes regarding sexuality and their SSE were .5–.75 SD above the mean. Based on this, and comparing the average raw values obtained by this cluster across different variables with P25 and P75 values for the complete sample, these participants have comparatively higher cognitive, attitudinal, and motivational competencies for maintaining a healthy and satisfactory sexuality, and they feel more confident in doing so. Thus, Cluster I demonstrates a high potential for experiencing healthy and satisfactory sexuality.
Cluster II (33.6%) comprised participants with poor knowledge, beliefs, and attitudes (approx. −.25 to −.75 SD below the mean). However, their SSE scores were above average (up to .37 [promotion] and .32 [prevention] SD above the mean). Comparisons of the raw data with percentiles for the whole sample indicated low levels for all variables. Consequently, these women could be considered at moderate risk for unhealthy or unsatisfactory sexuality despite their positive SSE.
Cluster III (23.2%) included participants with poor knowledge, beliefs, and positive attitudes regarding sexuality (around −.25 SD below the mean) along with the lowest level of SSE, −1 SD below the mean. Comparing the raw data with percentiles for the whole sample revealed low levels for all variables. Given their (standardized) substantially diminished cognitive–motivational resources, this configuration can be considered at high risk for experiencing unhealthy or unsatisfactory sexuality.
The clusters were then compared regarding the variables involved in the configuration (i.e., knowledge, beliefs, attitudes, and SSE) using univariate ANOVAs and a posteriori pairwise comparisons. ANOVAs revealed significant differences between the clusters for all the variables involved in the configuration (Table 3). Bonferroni’s or Games-Howell’s pairwise comparisons, using Levene’s F value for testing homoscedasticity, indicated significant differences between the three clusters for each of the variables (p < .001), except for knowledge and attitudes between Clusters II and III (p > .05) and for SSE for preventive and health promotion actions between Clusters I and II (p > .05) (see also Figure 1).
Table 3. Clusters centroids (Z scores) and comparisons for clustering variables
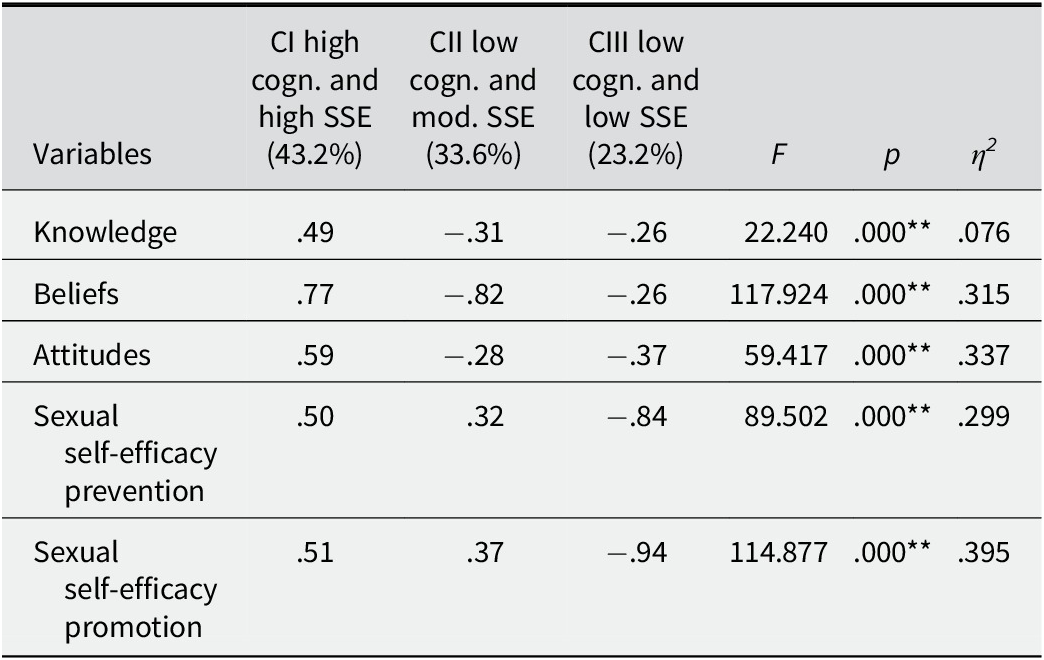
** p < .01
The clusters were also compared based on other sociodemographic and sexuality-related variables. There were no significant differences due to age (F = .166, p = .846), education level (F = 1, 523, p = .220), political ideology (F = 2, 215, p = .112), number of stable sexual partners (F = 1, 529, p = .219), number of sporadic sexual partners (F = 1, 858, p = .159), or stability of the current relationship with sexual or intimate partner(s) (F = 2, 702, p = .069). However, the analysis revealed significant differences between the clusters regarding religiosity (F = 5, 650, p = .004), regardless of the system of religious beliefs or practices. Cluster I showed a significantly lower religiosity level than Cluster II (p = .039) and Cluster III (p = .008).
Finally, the clusters were compared regarding the outcome variables SBs and SS using ANOVAs and subsequent pairwise comparisons. ANOVAs revealed significant differences between the clusters for both outcomes (see Table 4 and Figure 2). Bonferroni’s or Games-Howell’s pairwise comparisons, based on Levene’s F value, indicated significant differences between the three clusters for each variable (p < .01), except for SS between Clusters I and II (p = .253).
Table 4. Clusters centroids (Z scores) and comparisons for outcome variables
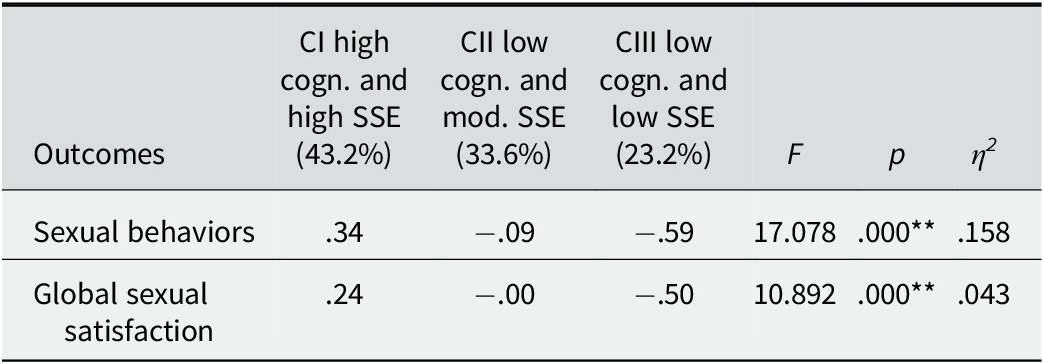
** p < .01

Figure 2. Outcomes (centroids for Z scores) for the profiles identified in the cluster analysis.
Note. All the differences are significant (**p < .01) except for those labeled as NS, indicating non-significant differences.
Discussion
Adopting a person-oriented, idiographic approach and focusing on women’s sexuality, which has often been neglected, misinterpreted, or mistreated (Bass, Reference Bass2016; Gavey, Reference Gavey2012), this study revealed different configurations of cognitive–motivational predictors of SBs among women during both youth and adulthood. These factors are differentially related to sexual health outcomes, including their SBs and SS.
Our participants showed adequate knowledge levels as a group, albeit slightly below the desired standard. Moreover, their beliefs regarding sexuality were slightly biased, but they also showed flexible and healthy attitudes toward the issue. In contrast, their SSE was notably high, although they reported engaging in less frequent and varied SBs without significant between-participant variability. Nevertheless, they reported relatively good levels of SS. All study variables showed the expected positive correlations, except for knowledge and SS, which showed a weaker association. This discrepancy may be attributed to the moderate knowledge levels observed in the sample, highlighting the importance of interventions aimed at enhancing cognitive competencies for healthier and more satisfying sexual experiences (e.g., Mahat et al., Reference Mahat, Scoloveno and Ayres2014; Montanaro & Bryan, Reference Montanaro and Bryan2014). Notably, this study found that sexual actions and well-being were more strongly linked to SSE in promoting health rather than preventing negative outcomes. While existing research has predominantly focused on self-efficacy expectations for behaviors aimed at averting or managing various risks (such as using condoms to prevent STDs or unwanted pregnancy) (see Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2023 for a review), this study highlights the importance of considering the relationships between self-efficacy, behavior, and positive outcomes. Neglecting these relationships limits the focus of sexuality research to undesirable actions and consequences, overlooking the broader spectrum of human behavior that includes pleasure, joy, and well-being.
Our primary objective was to identify individual patterns of cognitive and motivational predictors of SBs and SS. When distinct individuals exhibit specific profiles of these factors associated with different outcomes, it becomes less meaningful to analyze variables in isolation and for the entire sample, as this approach would obscure the true impact of these factors. These profiles and their prevalence can offer more informative and easily understandable insights than average descriptive values. Moreover, if various configurations are linked differently to SBs and SS, pinpointing individuals with these profiles could aid in designing interventions to promote sexual health. Utilizing cluster analysis techniques allowed us to establish such profiles. To our knowledge, no prior study has examined individual configurations of psychosocial predictors of SBs and SS at a multivariate level. Therefore, this study presents a particularly noteworthy contribution to the field.
The cluster analysis identified three distinct clusters characterized by varying combinations of cognitive and motivational competencies concerning sexuality (Figure 1). Approximately half of the women were categorized into a high-potential cluster. This group exhibited a moderate level of knowledge regarding sexuality, including STDs prevention, contraception, and a range of SBs that extend beyond preventive actions to include behaviors pursued primarily for enjoyment and pleasure. Additionally, they displayed healthier and more adaptable attitudes toward female (and male) sexuality, embracing diverse sexual orientations, masturbation, and other potentially pleasurable activities. They also showed a greater acceptance and normalization of contraceptive methods and held fewer biased beliefs regarding women’s sexual roles or the purposes of certain SBs, such as sexual fantasies. Participants in this cluster expressed confidence in performing not only preventive behaviors, such as correct condom usage, but also actions aimed at enhancing the pleasure and satisfaction derived from their sexual activities, such as communicating their desires to their partner(s). This configuration is consistent with results reported in other research (e.g., Kim et al., Reference Kim, Muise and Impett2018) and with Fishbein and Ajzen’s Theory of Planned Behavior (Reference Fishbein and Ajzen2010), which posits that attitudes toward certain attitudinal objects (in this case, healthy and satisfying sexuality) are shaped by complex cognitive processes involving knowledge and beliefs. Furthermore, the high level of SSE observed in this cluster, particularly in the context of engaging in preventive and health promotion actions, is consistent with Bandura’s self-efficacy theory (Reference Bandura1977, Reference Bandura1990, Reference Bandura1997). According to this theory, women who possess accurate information regarding sexuality-related issues (and have thus developed unbiased and flexible beliefs and attitudes) are more likely to hold stronger SSE beliefs. These enhanced SSE beliefs may increase the likelihood of successfully developing healthier SBs, thereby reinforcing SSE beliefs further through enactive mastery experience, as suggested by similar findings in the literature (e.g., Byno et al., Reference Byno, Mullis and Mullis2009).
The remaining participants were unequally distributed among the high-risk cluster (23.2%) and moderate-risk cluster (33.6%). The high-risk cluster includes women with low levels of knowledge and biased, less flexible, and unhealthy beliefs and attitudes. Their confidence in engaging in healthier and more pleasurable behaviors is notably low. Again, the Theory of Planned Behavior could explain this configuration. Additionally, their poor sexual self-confidence (SSE) seems plausible, as the less accurate the knowledge and the more biased and negative the beliefs and attitudes, the less likely the execution of successful behaviors and the development of SSE. The lower SSE observed in this cluster could be attributed to the lack of enactive mastery experience, recognized as the most influential source of self-efficacy (Bandura, Reference Bandura1997). This absence of firsthand successful experiences in SBs may contribute to the lower SSE observed, findings that are consistent with those of Gomes and Nunes (Reference Gomes and Nunes2015), who identified a cluster characterized by riskier SBs, weaker SSE, and more biased attitudes toward condom use. Although their study focused solely on preventive behaviors and used them as clustering variables rather than outcomes, the association between biased attitudes, weaker SSE beliefs, and less healthy behaviors aligns with our findings.
Participants in the moderate-risk cluster showed similar levels of knowledge and attitudes compared to the high-risk cluster but demonstrated the poorest beliefs. Interestingly, they also displayed high SSE levels, similar to the high-potential cluster. However, this level of SSE may be illusory, as it lacks a solid cognitive–motivational foundation for the development of perceived SSE and the performance of successful healthy and pleasurable SBs that could enhance it. Several potential explanations could account for this discrepancy. First, knowledge may act as a safety-like factor, wherein the absence of information about STDs or methods for preventing undesired pregnancy might lead to risky behaviors without immediate consequences, fostering a false perception of SSE. In other words, due to a lack of knowledge, participants might believe that their ability to engage in preventive SBs is adequate, even though this is not the case. Additionally, the choice of behaviors congruent with participants’ beliefs and attitudes, the effects of misleading negative beliefs on behavior (given that this cluster holds less flexible and healthy beliefs), or the influence of non-fact-based vicarious experience and persuasion may also contribute to this phenomenon (e.g., Byno et al., Reference Byno, Mullis and Mullis2009; Hu et al., Reference Hu, Cheng, Lu, Zhu and Chen2016; Zlomuzica et al., Reference Zlomuzica, Preusser, Scheider and Margraf2015). These alternatives should be more deeply explored in the future as sources of personal SSE when inappropriate knowledge coexists with negative beliefs and attitudes.
Another plausible explanation of this configuration could originate in the differences in religiosity between clusters, given that no other differences were found when considering sociodemographic, personal, and sexual factors, contrary to previous proposals (Sánchez-Fuentes et al., Reference Sánchez-Fuentes, Santos-Iglesias and Sierra2014). Specifically, religious beliefs might influence SSE through an indirect mechanism, namely, SBs. For instance, research has indicated that religious beliefs are associated with higher rates of sexual abstinence, fewer sexual partners, engaging in fewer sexual activities, and a lower frequency of sexual intercourse (e.g., Lefkowitz et al., Reference Lefkowitz, Gillen, Shearer and Boone2004), less sexual permissiveness (e.g., de Mamani et al., Reference de Mamani, Mejia, Gurak and Sapp2012), and delayed sexual activity (e.g., Hauser & Obeng, Reference Hauser and Obeng2015). Religious beliefs about the appropriateness of certain SBs could instill confidence and a sense of success in participants belonging to the moderate-risk cluster. Consequently, despite lacking an adequate cognitive–motivational basis, their SSE could be enhanced. Another conceivable explanation for this effect might stem from spirituality being linked to greater self-control (e.g., Desmond & Kraus, Reference Desmond and Kraus2012) (which fosters internalization of behavioral standards, self-monitoring, and desire to control or alter one’s behavior), optimism (e.g., Consiglio, Reference Consiglio2012), and self-esteem (e.g., de Mamani et al., Reference de Mamani, Mejia, Gurak and Sapp2012). Thus, religious beliefs could potentially serve as a mediating or even moderating factor in the relationship between knowledge, beliefs, and attitudes and SSE. Future research should test these hypotheses, given that religiosity has been robustly related to sexuality (Giménez-García et al., Reference Giménez-García, Castro-Calvo and Gil-Llario2020). This connection is more evident for women, with religiosity acting both as a system of sociocultural values shaping and regulating identities, learnings, and practices, and a structural politics of control (Muniz et al., Reference Muniz, da Costa, Fernandes, Castiglione, Rodrigues and Tanaka2024; Schnabel et al., Reference Schnabel, Abdelhadi, Ally Zaslavsky, Ho and Torres‐Beltran2022).
Comparisons among the three different clusters across the outcome variables of SBs and SS confirmed our expectations. Specifically, only the high-potential cluster showed favorable levels in both indicators. Women with higher cognitive–motivational competencies and stronger SSE engaged in more frequent and varied health-promoting and preventive SBs, consequently reporting higher levels of SS. This outcome was expected, given that SSE has previously been associated with the performance of preventive SBs (e.g., Boafo et al., Reference Boafo, Dagbanu and Asante2014; Katz & Schneider, Reference Katz and Schneider2015) and, although not extensively researched, it is also expected to correlate with health-promoting SBs (see also Ogallar-Blanco et al., Reference Ogallar-Blanco, Lara-Moreno and Godoy-Izquierdo2023). Moreover, the frequency and variety of SBs have been linked to better levels of SS (e.g., Barrientos & Páez, Reference Barrientos and Páez2006; Fisher et al., Reference Fisher, Donahue, Long, Heiman, Rosen and Sand2015; Ogallar-Blanco et al., Reference Ogallar Blanco, Godoy Izquierdo, Vázquez Pérez and Godoy García2017).
As expected, the high-risk cluster showed less frequent and varied SBs and reported the poorest levels of SS. Both outcomes were expected given the lower level of cognitive–motivational resources and SSE in participants belonging to this cluster. These findings are consistent with those of other studies (e.g., Espada et al., Reference Espada, Morales, Guillén-Riquelme, Ballester and Orgilés2016; Mahat et al., Reference Mahat, Scoloveno and Ayres2014; Montanaro & Bryan, Reference Montanaro and Bryan2014).
The moderate-risk cluster demonstrated healthier and more satisfactory sexual SBs than the high-risk cluster. However, these behaviors were still significantly lower in frequency and variety compared to the high-potential cluster. These findings emphasize how the cognitive and motivational schema characterized by higher knowledge, less biased beliefs, and flexible and healthier attitudes, along with stronger SSE beliefs, represents the most effective configuration for engaging in more satisfying and health-promoting SBs. It is noteworthy that, despite their cognitive–motivational resources appearing inadequate as a whole, participants in the moderate-risk cluster felt confident in engaging in sexuality-related behaviors. The key question is whether this confidence stems from their knowledge, beliefs, and attitudes, or, conversely, as the findings suggest, they felt confident in executing other (potentially risky) behaviors due to their presumably insufficient knowledge and inappropriate beliefs and attitudes. This crucial issue warrants further exploration in future research.
Additionally, the moderate-risk cluster demonstrated better levels of SS than the high-risk cluster, but their SS was (non-significantly) lower than that of the high-potential cluster. Since SSE concerns the perception of control over performance (Bandura, Reference Bandura1997), it is likely that, for this moderate-risk cluster, the sense of control experienced by participants may contribute to their levels of SS by simply reducing stress or fear of potential negative consequences. Alternatively, as discussed earlier, their unawareness of the actual nature of the behaviors they presumably do (or do not) execute and their consequences (or lack of positive consequences) might also influence their SS. Of course, given their moderate level of knowledge, it is also plausible that some of the knowledge they have acquired facilitates this level of SS, particularly when combined with their lower level of proper beliefs.
Despite the contributions of this study, several limitations should be acknowledged and appropriately addressed in future research. First, future studies should aim to increase both the number and heterogeneity of participants to enhance the generalizability of the results. This study focused solely on women during emerging or middle adulthood in Spain; therefore, the findings may not apply to other demographics or cultural contexts. Additionally, results may differ among individuals of different gender identities and sexual orientations; and hence, research with broader populations is warranted to test the robustness of these clusters. It is also important to consider the potential implications of self-selection bias, as our reliance on voluntary online recruitment may lead to a sample that could differ from the general population, since our participants might exhibit greater openness or interest in these topics. Future research may benefit from employing diverse recruitment strategies to achieve a more representative sample of attitudes, expressions, and experiences. Furthermore, this study was limited by the use of certain non-validated measures. While assessment tools were chosen to provide a broader perspective on the variables of interest, including items related to promotion issues and SS in various types of relationships, it is important to acknowledge this limitation. However, it is worth noting that all measures demonstrated adequate psychometric properties, including reliability and construct validity, based on available literature and prior research (e.g., Brown, Reference Brown and Gellman2020; Katz-Wise & Hyde, Reference Katz-Wise and Hyde2015; Wright & Bae, Reference Wright and Bae2015).
Given the multifaceted nature of sexuality, future research should also consider including additional psychosocial factors when establishing multidimensional profiles. These could include motivations for engaging in sexual relationships, intimate relationship status, experiences of sexual violence, or the influence of social media or new trends in sexuality (e.g., pornography consumption). Investigating additional predictors, such as partner dynamics (e.g., communication) and systemic factors (e.g., access to sexual health resources), could also provide deeper insight into SBs and SS. Finally, this study adopted a descriptive, cross-sectional, and correlational design, which limits the ability to draw causal conclusions. Therefore, future research must replicate and expand upon these findings using different research designs and analytical techniques. As a priority to enhance the understanding of how individuals navigate their sexual health, future studies should consider incorporating longitudinal designs to explore how cluster membership evolves over time and whether appropriate interventions can shift individuals from high-risk to high-potential profiles.
Practical Implications for Sexual Health Interventions
Traditionally, research on sexuality has primarily focused on identifying determinants of risky SBs to plan interventions aimed at preventing negative outcomes. However, our findings suggest that this approach overlooks a crucial aspect of the human sexual experience—the importance of enhancing pleasure, joy, and overall well-being. Therefore, it is vital to incorporate this complementary perspective into research and interventions. To achieve this, adopting an idiographic approach is essential. This approach enables the analysis of various configurations of cognitive and motivational variables closely related to both SBs and SS, shedding light on the unique contribution of each to inform the design of sexual health-promoting actions. The results of this study highlight the importance of implementing a nuanced strategy in interventions related to sexual health, taking intraindividual cognitive and motivational profiles into account. Targeted sexual health programs should be designed and implemented with the identified predictors of SBs and SS in mind by policymakers and practitioners. By concentrating on these influencing factors, interventions can be adapted to fulfill particular requirements, consequently augmenting their efficacy.
By examining configurations of psychosocial predictors of SBs and their relationship with both SBs and SS, we can effectively guide the focus of sexual health-promoting interventions. Establishing the predictors of SBs aids in identifying individuals at heightened risk for unhealthy and unsatisfactory sexual experiences, thereby facilitating the development of appropriate intervention initiatives. For instance, tailored educational programs for each cluster could enhance the effectiveness of these interventions. For the high-potential cluster, reinforcing healthy behaviors through advanced communication techniques or satisfaction-enhancing strategies may lead to better health outcomes and increased satisfaction. In contrast, for the moderate-risk cluster, developing interventions to correct biased beliefs and improve foundational knowledge while leveraging existing SSE to encourage safer and healthier practices would be essential. Finally, the high-risk cluster would benefit from an integral sexual health education intervention addressing knowledge, beliefs, attitudes, behaviors, and SS for enhancing the expression and experience of a healthy and pleasurable sexuality.
Conclusions
In this study, we identified three distinct intraindividual profiles that could be clearly differentiated, highlighting how cognitive and motivational competencies regarding sexuality shape specific schemata. These schemata, in turn, are differentially associated with SBs and SS among both young and middle-aged adult women. Furthermore, based on these general patterns, we have confirmed that SSE is a fundamental factor influencing both SBs and SS. Furthermore, it is critical to combine conventional risk prevention measures with strategies that enhance sexual pleasure and general well-being. In order to improve sexual health outcomes, idiographic approaches that assess unique combinations of sexual health determinants can result in more effective and individualized interventions.
Data availability statement
Data related to this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors are grateful to Your English Lab for language editing. The authors are also grateful to the participants in the present study.
Author contribution
All authors contributed to the investigation, material preparation, data collection, and curation, resources, validation, visualization and writing – review and editing. Conceptualization, design, formal analysis, and writing – original draft, were performed by Adelaida I. Ogallar-Blanco and Débora Godoy-Izquierdo. All authors have read and agreed to the published version of the article.
Funding statement
This research was supported by the financial assistance provided to the “Psicología de la Salud/Medicina Conductual” Research Group (CTS-0267) by Consejería de Innovación, Ciencia y Empresa, Junta de Andalucía (Spain), which included support for language editing. The authors declare that no additional financial support was received for the research, authorship, and/or publication of this article from other sponsors.
Competing interests
The authors declare that there are no commercial or financial relationships that could be construed as a potential conflict of interest.







 Open access
Open access