

Why does COVID‐19 kill more in some places than in others?
Pasteur stated that ‘science knows no country because it is the light that illuminates the world’ (cited in Morse, Reference Morse1996, p. xvii). Yet, if there is something that the COVID‐19 pandemic is elucidating, it is that the science light seems to shine brighter in some regions and countries than in others. Expert recommendations to control the spread of the virus – from social distancing or staying at home, to adopting novel treatments – have been endorsed to a far larger extent by some governments than others and followed more by some societies than others.
We argue that these differences across otherwise similar territories (countries or subnational regions) are the result of low trust and political polarization and, in turn, have had an impact on contagion and, especially, COVID‐19 related deaths. Societies strongly divided and confronted along partisan lines have been less capable, first, to garner the wide cross‐party agreements necessary to take tough policies against a pandemic and to clearly communicate them to the population; and, second, to implement those policies effectively, for government supporters and non‐supporters may opt for opposite courses of action. Political polarization is, among other factors, behind the refusal of many Republicans in the United States to wear a facemask (Gallup, 2020), or the ‘patriotic duty’ of Conservatives to visit pubs in Britain (Jones, Reference Jones2020), and the bullfighting arena in Spain (Minder, Reference Minder2020a).
The impact of divisive politics on the social and political response to COVID‐19 has received notable media coverage, but limited scholarly attention to date. Most of the COVID‐19 research has focused on epidemiological factors. Yet, given the unequal spread of the disease across territories and the different responses by national, regional and local governments, there are reasons to presume that political, societal and psychological factors also play a notable role. As long as we lack the ultimate means to eradicate COVID, the key variable to contain the spread of the pandemic is human behaviour (Van Bavel et al., Reference Van Bavel, Baicker, Boggio, Capraro, Cichocka, Cikara, Crockett, Crum, Douglas, Druckman, Drury, Dube, Ellemers, Finkel, Fowler, Gelfand, Han, Haslam, Jetten and Willer2020), as it determines factors such as the vaccination drive and the respect of basic social distancing norms. In order to understand the devastation of epidemics we need to put them in a large ecological context, considering the social variables that may foster or hinder their spread (Morse, Reference Morse1996). Disease thrives in ‘undercurrents of opportunity’ made available through social and political decisions, or lack thereof (Krause, Reference Krause and Morse1996). This paper presents a pioneering systematic study of these undercurrents of opportunity in the case of COVID‐19, and, in particular, of how political polarization may affect the lethality of the pandemic.
The paper builds on previous literature indicating that both social trust and institutional trust are protective factors against epidemics. As it has been noted regarding the COVID‐19 pandemic, how people have been able to stay at home, to keep physical distance from each other or to refrain from going to a bar or restaurant has depended on the trust citizens have both for other people – that is, social trust – and for their government – that is, institutional trust (Oksanen et al., Reference Oksanen, Kaakinen, Latikka, Savolainen, Savela and Koivula2020). Our paper makes four contributions to this literature.
First, we do not focus only on levels of trust, but also on variation – or polarization – of trust among citizens. We argue that in societies where there is a wide gap in institutional trust between those who support the government and those who support the opposition, it will be more difficult to implement measures and recommendations against COVID‐19. At the extreme, half of the voters could decide to wear a facemask and keep social distancing, and the other half could decide not only not to take preventive actions, but even to sabotage them, organizing protests and willingly violating the rules.
Second, we posit that both polarization and populist anti‐expert feelings lead to suboptimal policy making and implementation in the combat against the virus. If, in a society, there is a widespread scepticism of the recommendations by experts and of international cooperation such as the European Union's (EU) initiatives, it is difficult to gather support for crucial anti‐pandemic measures. Using several original measures of elite level polarization and ideology, we test whether the average government partisan positioning and level of polarization along three ideological dimensions – left‐right, GAL‐TAN, and European integration – explains our outcome variable.
Third, while research has largely concentrated on government outputs (e.g., anti‐contagion measures) against the pandemic, we look at outcomes: excess mortality during the first wave of the pandemic. Many scholars have explored the factors leading to different government responses to the pandemic: the strictness of the preventive measures, such as school and workplace closures, restrictions on mobility, cancellation of public events or public information campaigns (Cheibub et al., Reference Cheibub, Hong and Przeworski2020; Hsiang et al., Reference Hsiang, Allen, Annan‐Phan, Bell, Bolliger, Chong, Druckenmiller, Huang, Hultgren, Krasovich, Lau, Lee, Rolf, Tseng and Wu2020; Sebhatu et al., Reference Sebhatu, Wennberg, Arora‐Jonsson and Lindberg2020). Several works have also examined aggregate indicators of anti‐pandemic policies, such as the Oxford COVID‐19 Government Response Tracker (OxCGRT) (Cepaluni et al., Reference Cepaluni, Dorsch and Branyiczki2021). Comparatively less research in political science has focused on health outcomes, such as official accounts of deaths due to COVID‐19 or the daily data on confirmed cases of COVID‐19 (Cronert, Reference Cronert2020). Yet, since we are interested in the ability of regions to manage the COVID outbreak, measures like confirmed cases and confirmed deaths present problems since the World Health Organization notes, no reported cases represent a prevailing problem in this pandemic (WHO, 2020). A low account in both confirmed cases and confirmed deaths could be hiding either health authorities’ incompetence or even opportunistic underreporting. Confirmed cases, especially in the early stages of the pandemic, were also affected by huge variations in the capacity to test. Consequently, we consider that a more realistic measure of the devastation caused by a pandemic is to compare the excess mortality in a given territory relative to the previous 5 years. For, from a moral point of view, it is irrelevant whether a death – that could have been avoided – was directly due to COVID‐19 or, indirectly, because the patient did not get proper care for his/her cancer or heart attack. Consequently, our outcome variable of interest is excess deaths during the first 27 weeks of 2020 compared with the previous 5 years. Having said that, we also perform robustness checks with data on average weekly COVID‐19 cases for the period of analysis.
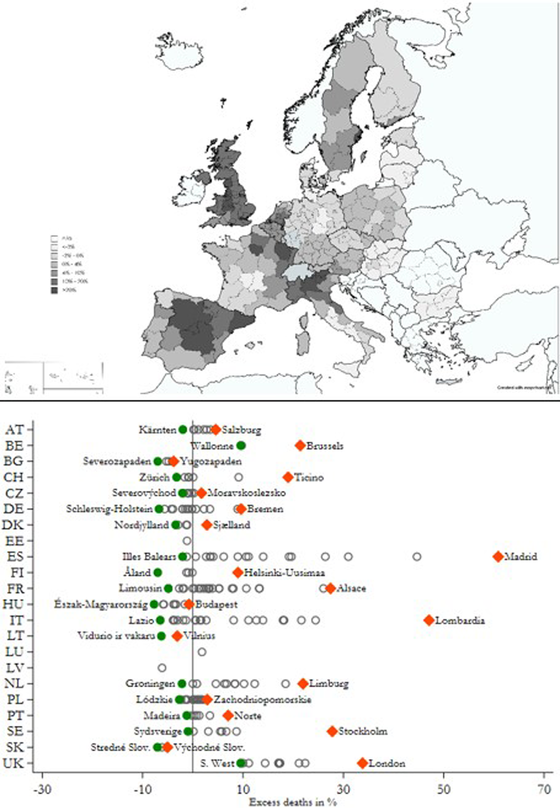
Fourth, while several studies have explored the influence of political factors on policy responses, public adherence to government regulations and COVID‐related deaths, such studies focus on national‐level variation, overlooking significant within‐country differences. For instance, democracies have generally reacted slower than autocracies. This is particularly the case with the most solidly democratic nations, such as the Nordic countries, the United States or the United Kingdom (Cheibub et al., Reference Cheibub, Hong and Przeworski2020). Authoritarian systems have imposed more stringent lockdowns (Frey et al., Reference Frey, Chen and Presidente2020). A study of 111 countries found that those with more obedient and collectivist cultural traits experienced larger declines in geographic mobility relative to their more individualistic counterparts (Frey et al., Reference Frey, Chen and Presidente2020). Moreover, most studies on institutional trust focus on cross‐national differences (Marien & Werner, Reference Marien and Werner2019; Van der Meer & Hakhverdian, Reference Van der Meer and Hakhverdian2017). That is particularly the case for studies on the impact of institutional trust on the (cross‐national) divergent reactions to COVID‐19 (Oksanen et al., Reference Oksanen, Kaakinen, Latikka, Savolainen, Savela and Koivula2020). This research rightly notes that institutional trust is typically highest in Nordic countries (Finland, Denmark, Iceland, Norway and Sweden). Yet, as recent studies with EU regions remark, the subnational differences in institutional trust between, for instance, northern and southern regions in nations like Italy or Spain outweigh cross‐national differences (Charron & Rothstein, Reference Charron, Rothstein, Bernitz, Mårtensson, Oxelheim and Persson2018). And, when it comes to the COVID‐19 pandemic, the regional divergence within the borders of the same country in excess deaths during the first 6 months of 2020 (in comparison to the 2015–2019 average) are remarkable, as can be seen in Figure 1. Many country capitals, as well as rich and highly dense regions, suffered significantly more during the first wave of the coronavirus pandemic.

Figure 1. Excess deaths in percentage across European regions. Note: Total deaths by region in 2020 between weeks 1 and 27 (until beginning of July) in comparison with Average deaths by region (2015–2019) between weeks 1 and 27. Above map shows darker shades = higher excess deaths. Below scatter‐plot shows excess mortality in all sample regions with diamonds (circles) representing the region with the highest (lowest) level of excess deaths in a given country. Hollow, grey circles summarize all other regions. Overseas French regions not included [Colour figure can be viewed at wileyonlinelibrary.com]
Figure 1 shows the importance of the subnational level variation across European countries. For example, in decentralized Belgium, the share of excess deaths during this time in the Brussels region was 21.4 per cent, whereas in Wallonia it was limited to 9.5 per cent. In the more centralized Netherlands, excess deaths in Limburg exceeded 22 per cent, while Groningen had just over 2.2 per cent fewer deaths. In even more extreme cases, we find remarkable differences between the Italian regions of Lombardy (over 47 per cent change in deaths), whereas Molise witnessed close to a 4 per cent decline. Similarly in Spain, excess mortality in Madrid increased by nearly 61 per cent, compared with a 2 per cent decline in the Balearic Islands, or 0.6 per cent increase in Andalucía. These within‐country differences are at times far more meaningful than the country‐level average differences: the most extreme comparison between Spain (19.4 per cent) and Latvia (−6.1 per cent) is far smaller than the within‐country gaps in Italy, Spain or France, and nearly equivalent to those in smaller, centralized countries, such as Sweden or the Netherlands. Moreover, due to the nature of the crisis itself, subnational governments (regional or local) are highly relevant, as they are responsible for many services directly affected by COVID‐19, such as health care and social services, which renders them at the ‘frontline of crisis management’ (OECD, 2020, p. 4). These factors motivate our choice of level of analysis.
In sum, this paper aims to contribute to the literature by examining the effects of trust and polarization on excess mortality due to COVID‐19 for European regions. We test four hypotheses. Two regard social division or the existence of an ‘uncooperative society’. We expect higher excess mortality in those regions with lower overall levels of social trust (H1) and lower mass polarization (measured by the difference in institutional trust between government and nongovernment supporters) (H2). Two hypotheses refer to political division or the existence of an ‘uncooperative politics’. We predict higher excess mortality in those regions with more political division (measured by the ideological polarization among the political parties in a region, and party fragmentation) (H3), and more populism (measured by a higher average score of the political parties in the region in the GAL‐TAN and anti‐European integration scale) (H4).
Our next section develops the theoretical arguments, and the subsequent ones explain the data and methods, and presents the empirical results.
Theory: Trust, polarization and pandemics
Governments around the world have responded to COVID‐19 in different ways (Hale & Webster, Reference Hale and Webster2020; Moon, Reference Moon2020) because they face conflicting considerations (Cheibub et al., Reference Cheibub, Hong and Przeworski2020). Our central message is that, in dealing with the pandemic, some governments, national and regional (which are particularly involved in health care policies in many European countries), have been constrained by socio‐political divisions. When taking and implementing the inherently high‐risk decisions on how to fight the virus, governments have pondered whether they have enjoyed sufficient support of opposition forces and the trust of their populations. Likewise, when deciding whether to follow governments’ rules and recommendations, citizens have been affected by the level of polarization.
Why have some regions and countries performed better than others in the fight against COVID‐19? The pandemic has forced governments all over the world to intervene in the health, social and business life of their citizens on a scale not seen since WWII (Cepaluni et al., Reference Cepaluni, Dorsch and Branyiczki2021). The general goal was to flatten the epidemiological curve and avoid the collapse of health care systems (Anderson et al., Reference Anderson, Heesterbeek, Klinkenberg and Hollingsworth2020). To start with, the virus hit first (and hardest) some territories and not others. Although Alpine ski resorts, notably in Austria, seem to have played an important part in the rapid diffusion of the pandemic, northern Italy is generally regarded as ground zero of COVID‐19 in Europe (Florida et al., Reference Florida, Rodríguez‐Pose and Storper2021). The havoc it wreaked in cities like Bergamo and Milan sent a strong warning to the rest of Europe, but it could not prevent its expansion to other hotspots, such as Madrid, London, Paris, Brussels or Stockholm. The higher initial exposure to the virus of some regions and countries may account for a good deal of excess deaths due to COVID. Yet we argue that other sources of variation stem from socio‐political divisions elucidated below.
Social trust
To understand those differences, existing research has highlighted the importance of both social trust (also known as generalized or interpersonal trust) and institutional trust. We have known for long that trust is a cornerstone of healthcare, from an effective doctor‐patient relationship to an efficient use of health services and adoption of pro‐healthy behaviour (Rowe & Calnan, Reference Rowe and Calnan2006). Additionally, trust is regarded as essential for an effective response to disasters (Norris et al., Reference Norris, Stevens, Pfefferbaum, Wyche and Pfefferbaum2008).
In principle, the relationship between social trust and containment is complex: high‐social‐trust areas are economically more vibrant, and thus the virus could have spread there more quickly. Yet in high‐social‐trust areas, citizens are more willing to contribute to the common good, and more conscious of the social consequences of their individual behaviour (Ostrom, Reference Ostrom, Serageldin and Dasgupta1999; Putnam, Reference Putnam1993). In essence, when enacting orders and recommendations against a pandemic, governments must rely on the social responsibility of their citizens (Bartscher et al., Reference Bartscher, Sebastian, Sebastian, Michaela and Nils2021). Good behaviour by each individual citizen is dramatically required for the success of a strategy against the virus (Bargain & Aminjonov, Reference Bargain and Aminjonov2020). If social trust is high, governments can rely on first‐best solutions that have low enforcement costs – such as recommending social distancing and hand washing, and asking citizens not to visit the elderly, and limit their travel – but those, as a downside, have a large risk of defection (Harring et al., Reference Harring, Jagers and Löfgren2021). Indeed, individuals with high levels of interpersonal trust exhibit higher support for the government's responses to the pandemic in a study of eight Western democracies (Jørgensen et al., Reference Jørgensen, Bor, Lindholt and Petersen2021). Yet, if people do not follow the recommendations not to socialize or to keep physical distance, as happened in Italy and Spain during the first week of the pandemic, then these governments need to take very tough measures, such as curfews (Oksanen et al., Reference Oksanen, Kaakinen, Latikka, Savolainen, Savela and Koivula2020). If citizens do not trust each other, governments cannot take an optimal response – recommendations that allow citizens some freedom to implement them to their personal circumstances – and will have to resort to a suboptimal hard monitoring and enforcement of regulations, like curfews enforced by the police or even the armed forces.
High levels of social trust may explain Sweden's ‘light approach’ to the fight against coronavirus and the fact that, at some stages of the pandemic, it achieved very similar results to some other European countries despite not undergoing a lockdown (Born et al., Reference Born, Dietrich and Müller2020). In turn, the corona crisis led to higher levels of social (and institutional) trust, as shown in a panel study of Swedish citizens from the initial phase to the acute phase in the spring of 2020 (Esaiasson et al., Reference Esaiasson, Sohlberg, Ghersetti and Johansson2021). In contrast, low social trust may be behind some of the hardest policy measures against COVID‐19 in European regions with a poor record in terms of controlling the pandemic. As Spain's chief epidemiologist Fernando Simón openly admitted when justifying the closure of children parks in the region of Madrid, a measure that attracted extensive criticism by experts in mental health and education, low trust in citizens’ behaviour was the main reason behind it: we need to close parks because ‘we do not have enough police officers as to put one in each corner of each park’ (El Español).
Other factors closely linked with social trust – such as social capital or levels of civil duty – have also been found to activate pro‐public health behaviour during this pandemic. Using mobile phone and survey data for US individuals, Barrios and Hochberg (Reference Barrios and Hochberg2020) show that voluntary social distancing during the early phases of COVID‐19 was higher where individuals exhibited a higher sense of civic duty. Additionally, social distancing prevailed in US counties with high civic capital, even after US states started to re‐open. A within‐country study of Austria, Germany, Italy, the Netherlands, Sweden, Switzerland and the United Kingdom showed that one standard deviation increase in social capital led to between 12 per cent and 32 per cent fewer COVID‐19 cases per capita (Bartscher et al., Reference Bartscher, Sebastian, Sebastian, Michaela and Nils2021). And, focusing on Italy, areas with high social capital exhibit both lower excess mortality and lower mobility (Bartscher et al., Reference Bartscher, Sebastian, Sebastian, Michaela and Nils2021). Likewise, there seems to be a strong association between social capital and the early reduction of mobility across US counties (Borgonovi & Andrieu, Reference Borgonovi and Andrieu2020).
Institutional trust
In order to comply effectively with government recommendations, citizens must trust that the recommendations they receive from the public authorities are correct and in their best interest (Harring et al., Reference Harring, Jagers and Löfgren2021). Evidence from previous pandemics points out in that direction. In 2014–16 Liberia and Congo citizens who distrusted their governments took fewer precautions against Ebola and were also less compliant with Ebola control policies (Blair et al., Reference Blair, Morse and Tsai2017).
Similarly, a lack of trust in government may lead to bad health outcomes. For instance, the historic low levels of trust in government in 1990s‐Britain were linked to the increasing hesitancy towards the measles‐mumps‐rubella (MMR) vaccine in large sectors of society (Larson & Heymann, Reference Larson and Heymann2010). Equally, the outbreak of measles in 2015 in Orange County has been associated to parents’ low trust in American public health agencies (Salmon et al., Reference Salmon, Glanz and Omer2015).
Regarding COVID‐19, influential observers noted early on that the major dividing line in the effectiveness of the crisis response was not the one between autocracies and democracies, but the one between high and low trust in government (Fukuyama, Reference Fukuyama2020). Moreover, institutional trust has been associated with lower COVID‐19 mortality in early studies. Countries, such as France, Spain or Italy, with lower levels of institutional trust than other European peers experienced higher deaths rates in the first weeks of the pandemic (Oksanen et al., Reference Oksanen, Kaakinen, Latikka, Savolainen, Savela and Koivula2020).
Institutional trust may also be conducive to a higher adoption of health and prosocial behaviours. Citizens are more prone to act in favour of the collective if they perceive that governments are well organized, that they disseminate clear messages and knowledge on COVID‐19 and that government interventions are fair (Han et al., Reference Han, Zheng, Cristea, Agostini, Belanger, Gutzkow, Kreienkamp, Collaboration and Leander2020). With regards to European regions, it has been found that those with higher institutional trust experienced a sharper decrease in mobility, related to non‐necessary activities, than low‐trust‐in‐government regions (Bargain & Aminjonov, Reference Bargain and Aminjonov2020). Nevertheless, other studies have concluded that institutional trust is of relatively little importance for predicting whether people follow government recommendations or take health precautions, such as using facemasks, social distancing or handwashing (Clark et al., Reference Clark, Davila, Regis and Kraus2020). Also, it was found that trust needs to be paired with high state capacity for producing desired outcomes (Christensen & Laegrid, Reference Christensen and Lægreid2020).
Polarization and populism
Our concept of polarization is in line with the notion of ‘partisan polarization’, whereby attitudes of elites and citizens are clustered around their partisan affiliations (Drukrman et al., Reference Druckman, Peterson and Slothuus2013). Partisan polarization can take two broad forms. The first, ‘ideological polarization’, refers to partisan voters or elites holding more extreme positions on policy issues. The second, ‘affective polarization’ (Iyengar et al., Reference Iyengar, Lelkes, Levendusky, Malhotra and Westwood2019), captures the idea that partisans distrust (or even dislike) those from opposing parties. In our framework, we apply the former type of polarization to the elite level (party positions in parliament), while the latter refers to mass polarization. We argue that both ideological (or elite) polarization as well as affective (or mass) polarization matter for understanding the results in the fight against the pandemic. If a large part of the population – those who vote for opposition parties – do not trust their institutions, the implementation of effective policies against the pandemic becomes difficult. If the fight against COVID‐19 is filtered thorough ideological lenses, supporters of a given party may find a duty in not following recommendations and health precautions suggested by institutions perceived as dominated by an opposing party. Given that face‐to‐face contact has been significantly reduced during the pandemic, the polarizing effects from self‐selected social media or partisan ‘echo chambers’ may enhance the effects of partisan polarization (Tucker et al., Reference Tucker, Guess, Barberá, Vaccari, Siegel, Sanovich, Stukal and Nyhan2018).
On the issue of mass‐level polarization, a noteworthy example is the Republicans in the United States. To start with, social distancing policies were taken more slowly in those states with Republic governors and more Trump supporters (Adolph et al., Reference Adolph, Amano, Bang‐Jensen, Fullman and Wilkerson2020). At county level, the effect of restriction orders has been stronger in Democratic‐leaning counties (Engle et al., Reference Engle, Stromme and Zhou2020). And, at individual level, it has been shown, tracking data from smartphones, that Republicans practice less social distancing (Barrios & Hochberg, Reference Barrios and Hochberg2020).
The situation may not be much different in Europe. In April 2020, Italy's opposition leader Matteo Salvini, together with 74 MPs, occupied the Italian parliament in protest at the ongoing lockdown in Italy (Roberts, Reference Roberts2020). In October that year, supporters of Spain's far‐right VOX organized protests against government restrictions (Rodriguez‐Guillermo, Reference Rodriguez‐Guillermo2020), and in several Italian cities, including Turin, Rome and Palermo, right‐wing demonstrations ended up with violent clashes with the police, including the throwing of petrol bombs at officers (BBC, 2020a).
Yet what motivates protests is not necessarily a right‐wing ideology, but the ideological distance with the institution that imposes (or is perceived as imposing) the anti‐COVID measures. For instance, in May 2020, right‐wing voters of upscale districts in Madrid demonstrated against the left‐wing national government for allegedly curtailing their freedoms with the anti‐COVID measures imposed in Spain (Viejo & Ramos, Reference Viejo and Ramos2020). While, in September, it was the turn of left‐wing supporters in poorer districts of Madrid to organize protests against the partial lockdowns decided by the conservative local and regional governments, for allegedly being ‘racist’ and ‘classist’ (Jones, Reference Jones2020).
This political polarization of a society is associated (as cause and/or effect) with polarization of the political elite (Hetherington, Reference Hetherington2001). We argue that the exacerbated ideological differences among political parties lead to worse outcomes in the fight against the pandemic through three mechanisms: first, it is more difficult for governments to build policy consensus with opposition parties; second, government parties give priority to core constituencies’ (e.g. business owners) demands over public health concerns and third, because with polarization, policies become more populistic and less based on experts’ criteria (see Drukrman et al., Reference Druckman, Peterson and Slothuus2013).
First, if political parties are ideologically distant from each other, governments will lack the support of opposition parties to take the necessary measures. To make extraordinary policies, governments need to build extraordinary consensus with other relevant political actors. Governments have to avoid taking erratic decisions once panic strikes following the onset of a pandemic and build consensus around expertise‐based solutions that may yield better long‐term results, even if they impose short‐term concerns. Building consensus is easier when, to start with, there is low polarization among the political elite. If opposition forces and the mass media that support them are ideologically very distant from the government, agreement about the adequate response to a crisis is unlikely.
To take costly measures – like wide‐scale testing and tracing measures – governments require the support of large parliamentary majorities that are improbable in highly polarized and fragmented party systems. One of the reasons for Spain's poor performance against the pandemic after the summer of 2020 is that, after having had Europe's strictest lockdown in the spring, the minority coalition in government headed by the social democratic Partido Socialista Obrero Español (PSOE) did not get parliamentary support to renew the state of emergency that allowed it to continue implementing tough measures (The Economist). The conservative PP and the Catalan and Basque nationalists refused to back the PSOE in a highly tense political climate amidst accusations of lying and hiding the real number of deaths due to COVID‐19. Rebuffed, the Spanish national government handed control of the pandemic to the regions. As indicated by The Economist, ‘Spain's poisonous politics have worsened the pandemic and the economy’ (ibid., p. 23).
Second, in highly polarized settings, governments may give priority to core constituencies’ short‐sighted interests over long‐term social benefits. To start with, governments fear reputational costs for both underreacting and overreacting. During the early stages of COVID‐19 many governments were accused of overlooking the threat. The opposite happened during the 2008 swine‐flu epidemic, when governments were blamed for overreacting. For instance, the French government spent 1.5 billion euros on swine‐flu vaccines and, since swine‐flu never reached a pandemic stage, the Minister of Health was accused of misspending (Cheibub et al., Reference Cheibub, Hong and Przeworski2020). In all crises governments face unavoidable trade‐offs, and, during pandemics, governments are forced to weigh in whether the health benefits of draconian anti‐contagion policies are worth their social and economic costs, such as sharp increases in unemployment and the worsening of educational outcomes (Hsiang et al., Reference Hsiang, Allen, Annan‐Phan, Bell, Bolliger, Chong, Druckenmiller, Huang, Hultgren, Krasovich, Lau, Lee, Rolf, Tseng and Wu2020).
In relatively low‐polarized party systems, governments may need to signal to their citizens that the high‐risk decisions they take serve public interests and not special interests (Cairney, Reference Cairney2016). Yet in highly polarized ones, parties in government may prefer to secure the support of their core constituencies, knowing that their actions will not get the legitimacy from a hostile rest of society. For example, the conservative Madrid regional government decided to reopen the interior of bars and restaurants against scientific advice, ‘given the importance of bars and restaurants to the Spanish economy’ (Dombey et al., Reference Dombey, Chaffin and Burn‐Murdoch2020, p. 1). For the president of the region, the tough measures recommended by experts would amount to ‘the death to our community’ (ibid.). As a result of these pro‐business policies, the Madrid hospitality association declared itself ‘very satisfied’ (ibid.). Quite the opposite, the Partnership for New York City, which collects the views of business, severely criticized Governor Cuomo and Mayor de Blasio for having ‘erred in the direction of favouring the health over the economic side of the crisis’ (ibid.), for they ignored business pressures and kept the restrictions on indoor dining. The result is that two large metropolises, Madrid and New York, which suffered almost an identically devastating first wave of COVID‐19 in the spring, entered the autumn with almost opposite patterns: the worst regional data in the early stages of the second wave in Europe (Madrid), and a relatively controlled situation (New York).
Likewise, in highly polarized settings, governments may be unable to take short‐term unpopular policy decisions, even if they are more effective in the long run. For instance, the Spanish government preferred not to cancel the massive demonstrations on 8th March across the country to commemorate International Women's Day, despite the existence of reports warning on the health dangers. As a matter of fact, three Spanish ministers leading the women's rally in Madrid – as well as the PM's wife – later tested positive for coronavirus (Minder, Reference Minder2020b). Yet banning the demonstrations would have infuriated core left‐leaning supporters of the coalition parties: as one of the popular banners in the protest stated, the demonstration was more important than stopping the pandemic for ‘machismo kills more than coronavirus’.
In third place, highly polarized settings are a fertile soil for populist policies instead of sound expert‐based ones. An active participation of experts is needed to resist short‐sighted political pressures during a pandemic. If civil servants are autonomous from their political superiors, they can speak truth to power, expressing their views based on their professional criteria, instead of trying to please their political bosses (Dahlström & Lapuente, Reference Dahlström and Lapuente2017). Expert autonomy and independence lead to decisions more guided by long‐term considerations rather than short‐sighted political pressures (Cronert, Reference Cronert2020). This is, for instance, what happened during the 2009 H1N1 influenza outbreak in California, where local health department officials prioritized proportionality considerations over short‐term panic reactions (Kayman et al., Reference Kayman, Salter, Mittal, Scott, Santos, Tran and Ma2015). Countries like South Korea or Denmark, contained the spread of COVID‐19 through an adaptive approach, thanks to the preparedness, professionalism and technological capacity of those experts.
The canonical example of political interference with experts would be the United States under President Trump. Trump tried to politicize neutral, scientific‐based bureaucratic agencies fighting against the pandemic. At the FDA, officials were ‘forced’ to authorize unproven coronavirus treatments that the then president championed but that scientists advised against, such as the malaria drug hydroxychloroquine or convalescent plasma (Interlandi, Reference Interlandi2020). At the CDC, political appointments by the Trump administration prevented scientists from publishing clear guidelines on what Americans should do against the virus. As a result, ‘decisions across the country about school openings and closings, testing and mask‐wearing have been muddy and confused, too often determined by political calculus instead of evidence’ (ibid.). Likewise, the conservative Madrid regional government, in its effort to minimize the importance of the pandemic, dismissed or forced the resignation of a dozen high‐ranking officials in health care, including the general director of public health, the manager of primary care and the one responsible for the Madrid hospitals, who were mostly in favour of tougher measures (Caballero, Reference Caballero2020).
A key question is how to measure the anti‐expert or anti‐elitist populism prevailing in a society. Following the literature on populist attitudes in Europe, we consider that anti‐EU feelings are a good proxy, because populist politicians across the continent have traditionally deemed the EU as an elitist‐expert project, far away from the problems of the common people, and a threat to national sovereignty (De Vries & Edwards, Reference De Vries and Edwards2009; Hooghe et al., Reference Hooghe, Marks and Wilson2002), and the waves of populism and Euroscepticism tend to break together in Europe (Pirro et al., Reference Pirro, Taggart and Van Kessel2018). In addition, the anti‐EU discourse of populist parties have been increasing in the aftermath of the 2008 financial crisis (Dijkstra et al., Reference Dijkstra, Poelman and Rodríguez‐Pose2020; Pirro & Van Kessel, Reference Pirro and Van Kessel2017).
Hypotheses
From the above discussion, we derive four hypotheses to be tested. First, in relation to the existence of social division or an ‘uncooperative society’:
Hypothesis 1 On social and institutional trust: The lower the level of social and/or institutional trust, the higher the excess mortality in the region.
Hypothesis 2 On mass polarization: The bigger the chasm in trust between government and nongovernment supporters in a region, the higher the excess mortality in the region.
In relation to the existence of political division or ‘uncooperative politics’:
Hypothesis 3 On elite polarization: The higher the degree of ideological polarization among the political parties in a region, the higher the excess mortality in the region.
Hypothesis 4 On populism: The higher the level of populism/anti‐experts politics in a region, the higher the excess mortality in the region.
Sample, data and design
Our sample includes up to 165 regions in 20 European countries.Footnote 1 The regions in question are largely at the NUTS 2 level, with the exception of Germany, Belgium and the United Kingdom, which are taken at the NUTS 1 level.Footnote 2 The selection of cases was determined largely by data availability on key variables and on our aim to present a valid comparison of cases from a common region that was affected by the pandemic at approximately the same time. The analysis therefore relies on a comparative, observational cross‐sectional research design, as randomization of trust and polarization are not feasible. While this feature renders estimating valid causal effects challenging, our estimation is not subject to critiques of ‘reverse causality’ common in cross‐sectional research, as the COVID‐19 pandemic in this case is exogenous from our mostly temporally prior regional‐level, explanatory characteristics. This implies that given our analysis accounts for possible confounding factors, our findings can be quite elucidating, yet should be still treated with caution.
Our outcome of interest is the relative performance of regions in response to COVID‐19. Recent empirical studies have relied on a host of various COVID‐19 outcome measures to evaluate government performance across countries. These include, inter alia, government response strategies (Yan et al., Reference Yan, Zhang, Wu, Zhu and Chen2020), citizen compliance with government guidelines (Becher et al., Reference Becher, Stegmueller, Brouard and Kerrouche2020; Cheibub et al., Reference Cheibub, Hong and Przeworski2020), economic outcomes (Ashraf, Reference Ashraf2020), or the spread of overall cases (Gilbert et al., Reference Gilbert, Pullano, Pinotti, Valdano, Poletto, Boëlle, D'Ortenzio, Yazdanpanah, Eholie, Altmann, Gutierrez, Kraemer and Colizza2020), hospitalizations and case‐fatality rates (Huber & Langen, Reference Huber and Langen2020; Oksanen et al., Reference Oksanen, Kaakinen, Latikka, Savolainen, Savela and Koivula2020; OECD, 2020). While such studies have provided keen insights into governments’ performance in handling COVID‐19, our outcome of focus is total death in (European) regions in 2020 between weeks 1 and 27 (until the beginning of July) in comparison with the average deaths by region for the same weeks during 2015–2019.Footnote 3 Our primary measure is the percentage increase (or decrease) in 2020 deaths during this time relative to the previous five years (‘excess deaths’).
The main argument in employing this measure is two‐fold. One, we are most concerned with how trust and polarization explain outcomes resulting from the COVID‐19, as opposed to government measures taken or compliance with guidelines. Two, as many governments (national or regional) employ different testing regimes and differ in terms of counting COVID‐19 deaths (BBC, 2020b), we argue that our measure of excess deaths allows for the most valid, cross‐regional comparison across numerous countries simultaneously.Footnote 4 The assumption of the measure is therefore that excess deaths in this period during 2020 compared to the same period in the previous 5 years can be attributed, directly or indirectly, to COVID‐19. As we are unaware of any other systematically confounding events, such as alternative diseases or conflicts, which are germane to certain regions or countries, we do not have any valid reason to question this assumption. As demonstrated in Figure 1, the measure provides remarkable variation within and across countries. The sample mean is a 5.1 per cent increase in deaths, with a high of 60.1 (Madrid, Spain) and a low of −7.7, in the Central and Western Lithuania region.
Concerning our main explanatory variables, we proxy institutional and social trust with data from the European Quality of Government Index survey (‘EQI’, Charron et al., Reference Charron, Lapuente and Annoni2019, Reference Charron, Lapuente and Bauhr2021). We take from the latest round of the data in lieu of the 2017 round because of the reported ‘rally effects’ noted in several recent empirical studies due to the onset of COVID‐19 (see, for example, Bol et al., Reference Bol, Giani, Blais and Loewen2021; Schraff, Reference Schraff2021) Data are taken from this source due to the unique sampling design that targets the regional level and provides between 500–600 individual respondents per region. This far exceeds the regional sample size which alternative sources, such as the European Social Survey (ESS) or World Values Survey (WVS) could provide at the subnational level. The questions are scaled from 1–10, with higher scores indicating greater degrees of trust in one's country parliament (institutional trust) and other people in their area (social trust). We aggregate the individual responses using post‐stratification weights for age, gender and education by region to account for over/under representation of people with certain characteristics. Further details on question formulation and summary statistics and pairwise correlations for all variables are found in the Supporting Information Appendix 1.
Second, as polarization is a contested concept and its operationalization is without a universally accepted measure (DiMaggio et al., Reference DiMaggio, Evans and Bryson1996), we construct and rely on several proxies in this analysis. Our first set of measures intends to capture our concept of mass (or ‘affective’) polarization to test H2, which is mainly focused on partisan polarization among the citizenry. In this vein, we build on a number of studies that measure the ‘winner‐loser’ gap in democratic countries by taking the difference in trust or democratic satisfaction between supporters of the sitting government versus supporters of opposition parties (for example Anderson & Tverdova, Reference Anderson and Tverdova2001; Bauhr & Charron, Reference Bauhr and Charron2018; Curini et al., Reference Curini, Jou and Memoli2012). Where this gap is low, we argue that there is a general consensus about the performance of national institutions (whether of high or low quality), whereas when this gap is large, there are clearer partisan divisions and less mass‐consensus in society. Using a question on the EQI survey about respondents’ partisan support, we then take the mean difference between government and non‐government supporters by region, to proxy for mass polarization. Specifically, we capture mass polarization (P) in region ‘j’ via the mean of political trust among supporters of the sitting government party (or parties) in relation to voters of opposition parties:
 $$\begin{equation*}M{P_j} = {\overline {Gov.\,supporter\,trust} _j} - {\overline {non\_Gov.\,supporter\,trust} _j}\end{equation*}$$
$$\begin{equation*}M{P_j} = {\overline {Gov.\,supporter\,trust} _j} - {\overline {non\_Gov.\,supporter\,trust} _j}\end{equation*}$$ To test H3 and H4, we proxy for elite (or ‘attitudinal’) polarization with several measures, relying on polarization of political parties in regional parliaments. We construct three measures. The first two rely on ideological partisan polarization, while the third is non‐ideological. First, following several studies of parliamentary polarization on the left‐right dimension (e.g. Dalton, Reference Dalton2008), we take the standard deviation of parties on a given ideological dimension, where elite polarization (EP) is a function of the number of parties (N), their party position ((
 ${p_i}$) compared with the mean party position in the regional parliament (
${p_i}$) compared with the mean party position in the regional parliament (
 $\bar p)( {\bar p} )\sum ( {{v_i} * {p_i}} )$and their relative vote share (v).
$\bar p)( {\bar p} )\sum ( {{v_i} * {p_i}} )$and their relative vote share (v).
 $$\begin{equation*}{\rm{EP\;}} = \sqrt {\mathop \sum \limits_{i = 1} N{v_i}{{\left( {{p_i} - \bar p} \right)}^2}} \end{equation*}$$
$$\begin{equation*}{\rm{EP\;}} = \sqrt {\mathop \sum \limits_{i = 1} N{v_i}{{\left( {{p_i} - \bar p} \right)}^2}} \end{equation*}$$ This measure thus captures the average distance of parties from the ‘ideological centre’ (
 $\bar p)$, yet not necessarily the relevant ideologically based conflict in a party system. It tends to rate two‐party systems more polarized than multiparty systems with a large range of ideological representation, while making skewed multiparty systems seem less polarized due to the weighted centre of gravity (see Evans, Reference Evans2002). As an alternative, we calculate the maximum ideological distance between parties (see Mair, Reference Mair and Laver2001). This more pragmatic measure captures the full ideological range of party systems in a given regional parliament:
$\bar p)$, yet not necessarily the relevant ideologically based conflict in a party system. It tends to rate two‐party systems more polarized than multiparty systems with a large range of ideological representation, while making skewed multiparty systems seem less polarized due to the weighted centre of gravity (see Evans, Reference Evans2002). As an alternative, we calculate the maximum ideological distance between parties (see Mair, Reference Mair and Laver2001). This more pragmatic measure captures the full ideological range of party systems in a given regional parliament:
 $$\begin{equation*}{\rm{EP}} = \max \left( p \right) - {\rm{min}}\left( p \right)\end{equation*}$$
$$\begin{equation*}{\rm{EP}} = \max \left( p \right) - {\rm{min}}\left( p \right)\end{equation*}$$There are clear issues with this measure as well, as small, irrelevant parties can alter the results quite drastically. It does not capture any distributional dynamics within the min‐max range. However, if both measures produce similar results, this provides stronger evidence for our claims.
In constructing both ideological, partisan polarization measures, the overwhelming majority of studies rely on a measure on the left‐right scale, usually via expert opinion data or party manifestos. Given that the economic left‐right spectrum plays a lesser role in Central/Eastern European polities (Bértoa, Reference Bértoa2014), we construct separate polarization measures based on three different possible ideological dimensions provided by the Chapel Hill expert survey data from 2019 (Bakker et al., Reference Bakker, Hooghe, Jolly, Marks, Polk, Rovny, Steenbergen and Vachudova2020). First, the standard economic left‐right cleavage, which captures preferences for state‐led distributive and regulatory policies versus a more market‐centred approach. Second, to proxy for alternative dimensions of relevant polarization as well as H4 regarding anti‐elite, populist politics, we take the so‐called ‘GAL‐TAN’ dimension which captures social conflicts around issues such as religion, marriage and national identity that range from libertarian to traditional/authoritarian/nationalistic (TAN). The TAN parties have been documented as being anti‐elite, anti‐expert populist parties (Polk et al., Reference Polk, Rovny, Bakker, Edwards, Hooghe, Jolly, Koedam, Kostelka, Marks, Schumacher, Steenbergen, Vachudova and Zilovic2017). Third, we also add pro‐ versus anti‐European integration stances, as this is a key dimension of competition in many countries, which can as GAL‐TAN, signal division over international cooperation and trust in technocratic and expert policy making versus a more nativist, populist set of preferences (Dijkstra et al., Reference Dijkstra, Poelman and Rodríguez‐Pose2020). We generate both the standard deviation and min‐max distance polarization measures for each of these three dimensions.
In addition to the ideological polarization measures, we construct a standard measure of party‐system fractionalization via 1‐the Herfindahl index (Powell, Reference Powell1982; Wang, Reference Wang2014). The measure captures the amount of party competition in a given parliament (similar to measures of firm competition in a market), where
 $v_i^2$ is the squared seat‐share of party ‘i’, which is summed and then subtracted from 1 so that higher values equal more fractionalization (or less concentration). The measure ranges between ‘0’ and ‘1’ where ‘0’ indicates that a single party controls all seats in parliament and ‘1’ equals perfectly equal dispersion of seats among different parties.
$v_i^2$ is the squared seat‐share of party ‘i’, which is summed and then subtracted from 1 so that higher values equal more fractionalization (or less concentration). The measure ranges between ‘0’ and ‘1’ where ‘0’ indicates that a single party controls all seats in parliament and ‘1’ equals perfectly equal dispersion of seats among different parties.
 $$\begin{equation*}P = 1 - \mathop \sum \limits_{i = 1}^N v_i^2\end{equation*}$$
$$\begin{equation*}P = 1 - \mathop \sum \limits_{i = 1}^N v_i^2\end{equation*}$$Finally, we include several control variables that have been considered to influence variations in the incidence of the pandemic. First is age. The mortality of older citizens from COVID‐19 is far greater than that of younger ones. We control for age, by including the average life expectancy, measured in years (from Eurostat). Next, it has been argued that the virus spreads more easily in more densely populated areas, thus increasing the risk for more deaths. We account for this with several factors. One, regional population density per square kilometre (logged, from Eurostat), which proxies for relative proximity to others and opportunities for human interaction. Additionally, we include controls for infrastructure quality (road accessibility) and average temperatures. The former proxies for the ease in which people can travel in and out of the area, while the latter has been found to be connected with the spread of COVID‐19 (Wang et al., Reference Wang, Tang, Feng and Wang2020).
Third, many studies point to the benefit of institutional capacity in handling the pandemic (Christensen & Laegrid, Reference Christensen and Lægreid2020; Hartley & Jarvis, Reference Hartley and Jarvis2020; Rodríguez‐Pose & Burlina, Reference Rodríguez‐Pose and Burlina2021). We account for a region's institutional capacity with the European Quality of Government Index (EQI, Charron et al., Reference Charron, Dijkstra and Lapuente2014), which measures the degree of perceived and experienced corruption, as well as the quality and level of impartiality of public services across EU regions. Additionally, specifically to the health sector, we proxy the capacity of subnational health care services via hospital beds per capita (100,000 inhabitants). Fourth, we include a measure of overall economic capacity via its GDP per capita (measured in purchasing power parity (PPP, logged)), from Eurostat. Finally, the mean values of a parliament's left‐right, GAL‐TAN and pro/anti‐European integration positions in several models are also considered. Summary statistics and further information about all the variables are included in Appendix, section 1, while more on the sample is found in Appendix 2. A correlation matrix of all variables is found in appendix Table A5.
Estimation
As our dependent variable is continuous, we use linear regression to estimate our models. Several diagnostic tests reveal several issues of concern that could violate the assumptions of Ordinary Least Squares (OLS) and thus affect our estimates. First, several of our explanatory variables show high levels of multicollinearity, thus we approach our estimation using several step‐wise models, avoiding the inclusion of too many explanatory variables that co‐vary significantly. Additionally, we report the variance inflation index (VIF) for each model. Second, we find strong heteroscedasticity (Brasch‐Pagen test, p < 0.001). Third, even though many countries in Europe and elsewhere have taken a regionally focused approach in response to COVID‐19, allowing much regional policy flexibility based on regional disparities in cases, the regional observations are not independent, but nested in countries. For example, an empty hierarchical model reveals that 73 per cent of the variation is in fact at the regional level, yet a significant percentage (27 per cent, p = 0.000) lies at the country level. To address the issue of nested observations – regions within countries – there are several approaches commonly used in the literature, such as country‐level clustering, country‐fixed effects or hierarchical models that estimate random country‐level intercepts (Bryan & Jenkins, Reference Bryan and Jenkins2016). In our case, clustered standard errors will not suitably address the structural differences in the dependent variable across countries, while country‐level fixed effects provide less flexibility with respect to degrees of freedom. We rely on advice from recent research, which demonstrates that even with a somewhat limited second level of observations (as in our case, 19), the estimates for first level covariates (regions in our case) are valid (see Elff et al., Reference Elff, Heisig, Schaeffer and Shikano2021). We therefore elect to account for the country‐level context via hierarchical estimation with country‐level random intercepts to account for structural variation in the dependent variable across countries and robust, country‐clustered standard errors.
Empirical results
We begin with a test of H1 and H2 – anticipating that higher levels of institutional and social trust will yield lower excess deaths on average, while greater mass polarization on these measures between supporters and non‐supporters of the government will result in higher rates of excess mortality due to COVID‐19. Model 1 tests the baseline effects of our control variables, which we find are generally in line with our a priori expectations. We find that excess mortality during the first wave of COVID‐19 at a regional level in Europe is connected, as expected, to ageing, the capacity of the health care system and various factors that render regions more susceptible to the spread of the virus in general, such as population density, road accessibility and climate at a regional level, yet seems unrelated to the size of the economy and the regional quality of government, all things being equal. The random effects parameter σ (country) reveals that even with the control variables in the mode, there is significant unexplained country‐level variance; the standard deviation of country level variance is roughly 4.1 per cent excess deaths. Finally, a VIF score of 3.66 indicates that multicollinearity does not represent a problem (James et al., Reference James, Daniela, Trevor and Robert2013).
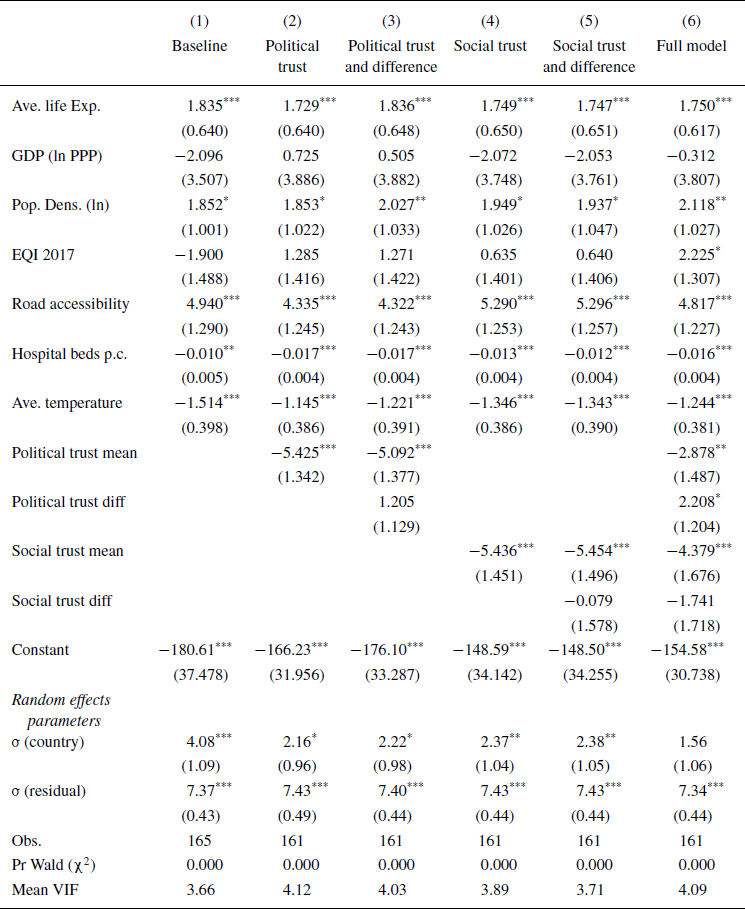
In models 2–6, we test H1 and H2. Beginning with institutional trust in model 2, we observe corroborating evidence for H1: higher levels of institutional/political trust are associated with lower mortality. All things being equal, a one‐unit increase in social trust results in 5.4 per cent fewer excess deaths in the first six months of 2020 compared with the same months in the previous 5 years. Regarding H2 (the bigger the chasm in trust between government and nongovernment supporters in a region, the higher the excess mortality), model 3 shows that although political trust polarization is in the expected direction, it is not a significant predictor in rates of mortality. In terms of social trust, model 4 displays that the results are quite similar to those with political trust (model 2), whereby a one unit increase in social trust is associated with 5.4 per cent fewer excess deaths across the regions in our sample, all things being equal. Yet model 5 shows that the anticipated effects of social trust polarization among the population are not significantly associated with greater excess deaths. Model 6 reports the effects of the trust variables together, where the negative effects of both dimension of trust remain significant predictors of the dependent variable, indicating a strong support for H1 even after controlling for most other factors that have been highlighted by the COVID‐19 literature as drivers of excess mortality: lower levels of both social and political trust are associated with higher mortality rates. Further, we find that when controlling for the effects of social trust, the polarization of institutional trust becomes significant at the 90 per cent level of confidence (p = 0.06). Model 6 thus also presents some support, even if weak, for H2: the higher the difference in (political) trust between government and nongovernment supporters in a region, the higher the excess mortality in the region. Finally, in this model, we also observe that the trust variables together account for enough of the country‐level variation to render the random effects parameter insignificant.
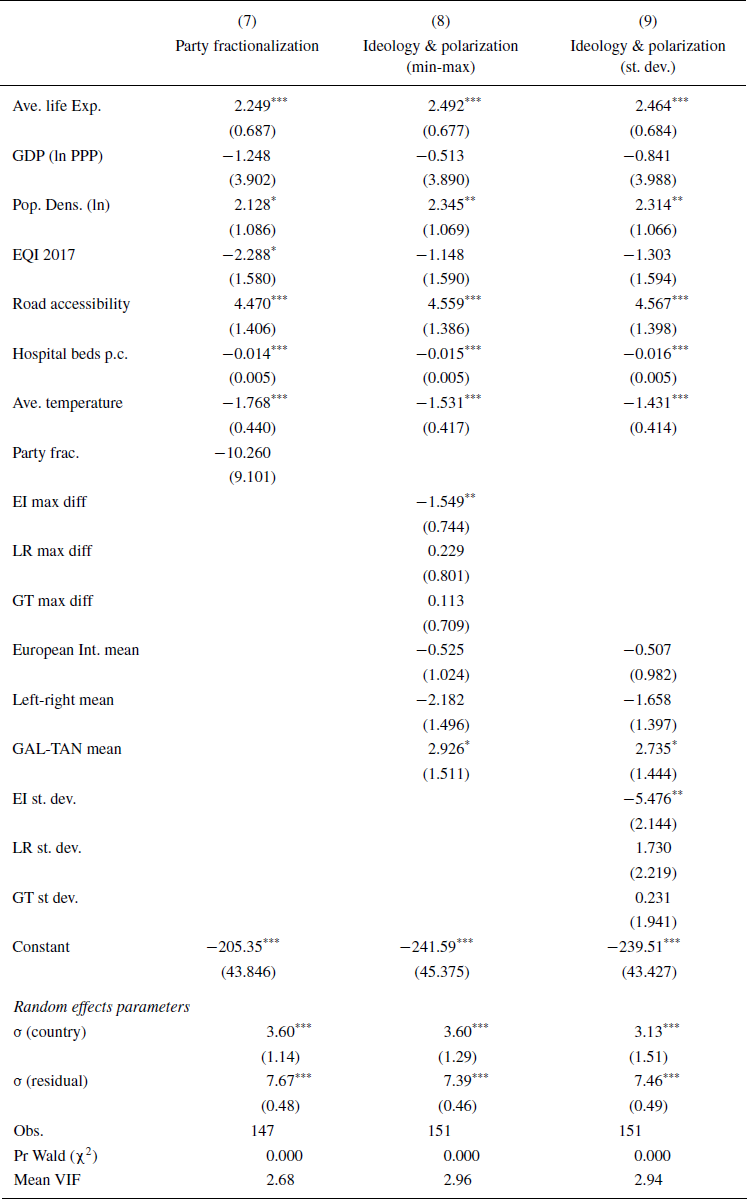
Models 7–9 in Table 2 report the results for H3 (on elite polarization) and H4 (on elite populism). As noted in the previous section, we present several different proxy measures of elite polarization. The first measure is the non‐ideological measure of party fractionalization, which captures the concentration of political power in a given parliament. Model 7 shows no evidence that fractionalization is related with mortality due to COVID‐19. That is, the polarization in terms of having an extraordinarily fragmented parliament does not seem to be associated with higher mortality during the pandemic.
In models 8 and 9, we present three different proxies of ideological polarization: polarization in the dimension European Integration, in the Left‐Right, and in the GAL‐TAN. As the dimensions are related, we include all three simultaneously to estimate the effect of each holding constant the other dimensions and to avoid omitted variable bias. Model 9 reports the measure of min‐max difference on the three ideological dimensions, whereas model 10 reveals the results of average standard deviation difference from the parliament's mean position. We test these under control for the mean position of each ideological dimension. The results do not corroborate H3, except for the European Integration dimension. Neither the polarization on the left‐right or the GAL‐TAN dimensions explains systematic variation in excess mortalities. However, polarization on the European integration dimension does in fact explain mortality, thus providing some support for H3. It is thus interesting that the only ideological dimension in which the polarization of political parties in the parliament is related to higher mortality is the one of the two noted by the literature (and our theory) as a proxy for expert versus populist tensions: the attitudes towards the EU. All things being equal, a one standard deviation increase on the min‐max and standard deviation measures are associated with −2.6 per cent to −3 per cent change, or roughly 6,500 and 7,500 deaths respectively in a region with a mean population of 2.35 million (see Table A10 for predictions).
Moving to H4 (i.e., the higher the level of populism/anti‐experts politics in a region, the higher the excess mortality in the region), we see some support. The mean of TAN (Traditional, Authoritarian, Nationalistic) attitudes among politicians is significant. Ceteris paribus, regions with a higher ‘tan’‐leaning parliament, experience higher rates of excess deaths on average.
The findings are similar irrespective of the methods of operationalizing polarization. Both the min‐max (model 8) and the standard deviation (model 9) indicate that some proxies for polarization and populism (among the political elite) are associated with higher excess deaths on average.
Overall, the models show support for two of the four hypotheses (H1 and H4), some support for one hypothesis (H3), and weak support for another (H2). Yet, in addition to our control variables, we further test the robustness of our findings. First, our model presumes a constant degree of polarization, yet this factor might be affected by the electoral cycle. Next, we account for the fact that several regions in our data are non‐land contiguous islands, which could have the dual effect of more social cohesion together with better protection against the spread of the virus. We find the results in our main models to be unaffected (see Appendix 3). Additionally, higher death rates and trust/polarization levels can be affected by other confounding factors, such as regional income inequalities. We re‐run our analyses with a proxy for income inequality (% of regional population at risk of poverty, from Eurostat). The models are unaffected by this factor. We re‐run all models that corroborate our hypotheses from Tables 1 and 2 and include controls for regional inequality, island status, along with a binary variable for whether a region has an election in 2020. We find the results to be stable (see Table A8).
Table 1. Test of H1 and H2

Note: marginal effects coefficients from linear hierarchical regression with random country intercepts. Country clustered, robust standard errors in parentheses. The dependent variable is excess mortality (in %) in the first six months of 2020, relative to the previous five years. Number of countries included models with trust variables is 17. ‘VIF’ is the mean variance inflation factor for all right‐hand side variables in each respective model. *** p < 0.01, ** p < 0.05, * p < 0.1.
Table 2. Test of H3 and H4

Note: marginal effects coefficients from linear hierarchical regression with random country intercepts. Country clustered, robust standard errors in parentheses. The dependent variable is excess mortality (in %) in the first six months of 2020, relative to the previous five years Number of countries included models is 18. ‘VIF’ is the mean variance inflation factor for all right‐hand side variables in each respective model. *** p < 0.01, **p < 0.05, *p < 0.1.
We further check whether the results are sensitive to the sample employed. In particular for the effects of elite polarization for H3 and H4, we include country level data in the main tables for those cases that do not have a regionally elected parliament at the level of the unit included in our sample. As a robustness check, we re‐run Table 2 with a subsample of only those regions with elected parliaments at the relevant NUTS level to our sample (see Table A7). The results remain consistent with the main findings.
Finally, we test two alternatives to the main dependent variable. One, we use data on average weekly Covid‐19 cases for a similar time period to our excess deaths variable (average cases per 100k inhabitants, weeks 13–27 in 2020).Footnote 5 Although the sample is more restricted due to data limitations, we find that for H1 and H2, the results are in fact more pronounced when applying cases, as the dependent variable is cases compared with excess deaths (see Table A5). When looking at H3 and H4, we find that the results of elite polarization and ideology are less pronounced. Yet, when accounting for cases as a variable on the right‐hand side of the model, the effects found in tests of H3 and H4 are more or less equivalent with the main results (Table A6). Two, as the variable exhibits a right skew (see Figure A1), we re‐run the results with a logged dependent variable (Table A9), where we find the results mostly indistinguishable. We interpret this finding as the effects of ideology and elite polarization on deaths, holding constant the volume of Covid‐19 cases in a region.
Conclusions
Since the beginning of March 2020, the COVID‐19 pandemic has taken over the lives of European citizens. With its high death toll and its social and economic disruption – as a consequence of lengthy lockdowns, closure of public and work spaces, travel restrictions and the re‐establishment of border checks, among others – COVID‐19 has gone from being considered as just ‘another flu’ to the biggest threat to hit Europe since the end of the second World War. But the incidence of the pandemic has been geographically very uneven, both across and within countries. Whereas some parts of Europe have been ravaged by it, others came out of the first wave of the pandemic relatively unscathed. This article has examined the reasons behind these substantial differences in incidence at the regional level in Europe by analysing how variations in social and institutional trust, and social and political polarization, may have contributed to explain variations in COVID‐19‐related excess mortality during the first wave of the pandemic.
The results of the analysis conducted for 165 regions in Europe show that, in addition to well‐known drivers, such as age and density, accessibility, the preparation of the health system or climate, variation in (social and institutional) trust explains the uneven geography of the pandemic. Regions characterized by a low social and institutional trust witnessed a higher excess mortality during the first wave. We also find some support for the idea that the bigger the chasm in trust between government and non‐government supporters in a region, the higher the excess mortality in the region – yet not in all models and only regarding political (or institutional) trust, not social trust. When the divide in political trust between supporters and opponents of incumbent governments within societies is high, we observe consistently higher COVID‐19‐related excess mortality. The results highlight that social division – or what we refer to as an ‘uncooperative society’ – is highly correlated with excess mortality, controlling for the main prevailing confounders.
Likewise, we also find support for the relationship between political division – or what we refer to as ‘uncooperative politics’ – and higher mortality. Although we find limited evidence of elite polarization driving excess deaths, partisan differences on one particular ideological dimension emerge as a strong predictor of higher levels of excess deaths: the attitudes towards the EU. This is precisely the dimension that we, following the literature, use as a proxy for (anti)populism. The reason for this may be that regions with a sharper divide between Eurosceptics (i.e. anti‐expert populists) and EU‐supports (i.e. pro‐expert policies) among politicians have more problems to gather consensus around (what mostly are expert‐based) anti‐pandemic measures. Likewise, we also find support for H4: in those regions where the political elite is less supportive of European integration (i.e., more anti‐expert populist), the excess deaths have been significantly higher. Similarly, regions with a higher ‘tan’‐leaning parliament (i.e., more traditional, authoritarian and nationalistic) present higher rates of excess deaths on average, providing further evidence that the prevalence of populism (among the political elite) has negative effects for handling a pandemic.
Hence, our findings indicate that lower social or institutional trust, as well as greater social and political polarization, may have ended up costing lives during the first wave of COVID‐19 in Europe. In other words, having an uncooperative society and an uncooperative politics is detrimental for handling a pandemic. Our results concur with what previous studies have noted: in order to build societal resilience against collective threats, we need a degree of societal and institutional trust (Oksanen et al., Reference Oksanen, Kaakinen, Latikka, Savolainen, Savela and Koivula2020; Norris et al., Reference Norris, Stevens, Pfefferbaum, Wyche and Pfefferbaum2008). Likewise, the results are also compatible with existing research that analizes the relationship in reverse – that is, how (government's responses to) pandemics may foster social and institutional trust (Esaiasson et al., Reference Esaiasson, Sohlberg, Ghersetti and Johansson2021). And this is an intriguing debate in the theory of democracy: will the pandemics reinforce support for democratic institutions – consolidating a virtuous cycle of social and institutional trust – or debilitate democratic support – following the experimental evidence showing how a virus outbreak increases citizens’ willingness to give up individual freedom and demand for a strong leader (e.g., Amat et al., Reference Amat, Arenas, Falcó‐Gimeno and Muñoz2020)?
Having said that, a concluding implication from the analysis we present here is that, if (social and institutional) trust fail, especially in already polarized or polarising societies, the defences against a pandemic or other threats may become weakened, making many attempts to combat it futile. If Pasteur said that science is the light that illuminates the world, we can say polarization is the darkness that shadows it. Generating trust and overcoming polarization are thus essential if we are going to succeed in fighting the COVID‐19 pandemic and in confronting other collective challenges further down the line.
Online Appendix
Additional supporting information may be found in the Online Appendix section at the end of the article:
Appendix 1: further details about the variables
Table A1: Description and source of variables
Table A2: Summary Statistics
Table A3: Correlation Matrix of Variables
Appendix 2: Description of the Sample
Table A4: Full Sample of regions
Appendix 3: checks for robustness
Table A5: Replicating Table 1 with Covid‐19 Cases per capita
Table A6: Robustness check of Table 2: Controlling for Covid‐19 Case Rates
Table A7: Testing H3 and H4 with Sub‐sample of regions with elected parliaments
Table A8: Replicating main findings with inclusion of additional regional controls
Table A9: Replicating main findings with logged dependent variable
Table A10: predicted changes in excess deaths resulting from changes in significant variables.
Figure A1: Histogram of dependent variable, excess deaths (%)
Supplementary information



 Open access
Open access