

1 Historical Prelude: Kuru and the Fore People of Papua New Guinea
What I am about to tell you is a medical story that is more compelling than any story you could possibly imagine. It will leave an indelible impression on you, as it did when I first encountered it. This is not only because it is based entirely on actual events but also because it reveals a fascinating scientific journey that has unfolded over several decades. It will leave you mesmerised at the depth and complexity of medical discovery but also at our rather tenuous understanding of some of the diseases that afflict us. There are important lessons about logic, reasoning, and communication along the way – lessons that have heightened salience following the COVID-19 pandemic. But they are couched within a narrative that unfolds on multiple levels. We begin that narrative some 70 years ago, with the Fore people of Papua New Guinea:
Dark night in the mountains and no drums beating … In pity and mourning but also in eagerness the dead woman’s female relatives carried her cold, naked body down to her sweet-potato garden bordered with flowers. They would not abandon her to rot in the ground. Sixty or more women with their babies and small children gathered wood and lit cooking fires … The dead woman’s daughter and the wife of her adopted son took up knives of split bamboo … They began to cut the body for the feast … the dead woman’s daughters ringed her wrists and ankles, sawed through the tough cartilage, disjointed the bones and passed the wrinkled dark hands and splayed feet to her brother’s wife and the wife of her sister’s son. Slitting the skin of the arms and legs, the daughters stripped out muscle, distributing it in dripping chunks to kin and friends among the eager crowd of women. They opened the woman’s chest and slack belly … Out came the heavy purple liver, the small green sac of the gallbladder cut carefully away from the underside … Out came the dark red heart … and looping coils of intestines … One of the daughters … cut around the neck, severed the larynx and esophagus, sawed through the cartilage connecting the vertebrae, disjointed the spine and lifted the head aside. The other daughter skinned back the scalp skilfully, took up a stone ax, cracked the skull and scooped the soft pink mass of brain into a bamboo cooking tube … Even the feces would be eaten, mixed with edible ferns and cooked in banana leaves.
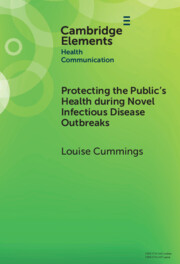
This account of cannibalism is based on the field notes of anthropologists who lived and worked among the Fore people of Papua New Guinea in the early 1950s. The Fore was a linguistic and cultural group of some 35,000 people who lived in 160 villages in the mountainous interior of the country. Fore men and women lived separately. The men of the tribe believed that contact with women made them weak (see Figure 1). They also resented the fecundity of women. Men ate the best parts of the pig, small game, possums, and lizards. Women consumed beans, sweet potatoes, and sugar cane. Their largely vegetarian diet was supplemented with roasted, hand-sized spiders and fat grubs. The practice among Fore women of consuming dead kin – known as endocannibalism – was their revenge against men for eating the best parts of pigs (Reference RhodesRhodes, 1997, pp. 23, 27). Fore women were selective in the dead bodies that they would consume. They would not eat the flesh of those who had leprosy, dysentery, or suspected yaws (Reference LindenbaumLindenbaum, 2008, p. 3717). At the time of witnessing this ritual, anthropologists could not have predicted the devastating impact that it would eventually have on this remote group of people.

Figure 1 Fore warriors in New Guinea, 1957.
The consumption of dead kin by Fore women and children is now widely believed to be responsible for the emergence of a fatal neurological disease called ‘kuru’. The disease takes its name from a Fore word meaning ‘to be afraid’ or ‘to shiver’ and is a description of the symptoms experienced by those who suffered the ravages of kuru. Some 2,500 people died of kuru between 1957 and 1977. Most deaths occurred in adult Fore women. So many Fore women succumbed to kuru that in 1962 a sample of 125 males in the village of Wanitabe revealed that 63 men had no living wives and 10 had never married (Reference LindenbaumLindenbaum, 2008, p. 3718). The marked disparity in the prevalence of the disease between men and women led Fore women to believe that the men of their tribe were practicing sorcery against them. Shirley Lindenbaum, an Australian anthropologist who lived among the South Fore between 1961 and 1963, recorded the fears of a Fore woman of Kamila, which were expressed during a public gathering on 4 December 1962:
Why are you men killing off all the women, stealing our feces from the latrines to perform sorcery? We women give birth to you men. Try to find one man who is pregnant now and show him to us. Or go and search the old burial grounds and bring us the skull or bones of one man we women have killed. You won’t be able to find any. You men are trying to wipe us out.
Lindenbaum and her then husband Robert Glasse had been asked by Henry Bennett of the University of Adelaide to study kinship relations among the Fore. Bennett believed that a genetic explanation of kuru could be given. Lindenbaum and Glasse began their anthropological study of kuru in July 1961 (Reference LindenbaumLindenbaum, 2015). It became apparent to them that a genetic cause of kuru could not be supported by the kinship relations they were observing among the Fore. Writing in 2008, Lindenbaum reflected on her and Glasse’s research in the following terms:
Our genealogical research indicated that the Fore definition of relatedness included people said to possess ‘one blood’, many of whom had acquired the status of close kinship by social means. In a number of ways our research had begun to indicate that a simple hereditary explanation for kuru seemed hard to justify.
Anthropologists were not alone in trying to understand this bizarre disease in the Fore people. An American paediatrician and virologist, Carleton Gajdusek, and an Estonian-born physician, Vincent Zigas, were beginning to undertake systematic scientific studies of kuru. Gajdusek had heard about kuru while visiting Australia. Zigas was the district’s medical officer and had first learned of kuru in 1956 (see Figure 2). They started their fieldwork in March 1957 (see Figure 3). Gajdusek and Zigas established a Kuru Research Centre at the Okapa Patrol Post with the assistance of patrol officer Jack Baker (see Figure 4). Gajdusek’s work on kuru was to earn him the 1976 Nobel Prize in Medicine and guaranteed him a position of prominence in our understanding of prion diseases.

Figure 2 Vincent Zigas (left) working with patrol officer Jack Baker (centre) and Carleton Gajdusek (right) in Okapa, New Guinea, Reference Gajdusek and Zigas1957.

Figure 3 Carleton Gajdusek working with Fore people, Reference Gajdusek and Zigas1957.

Figure 4 Carleton Gajdusek and Jack Baker outside Baker’s house in Okapa, Reference Gajdusek and Zigas1957.
Gajdusek and Zigas conducted extensive investigations that examined genetic, infectious, endocrine, and nutritional factors as possible causes of the disease. The neurological degeneration that attended the disease was also vividly captured for the first time in a large collection of photographs taken by Gajdusek. Kuru is so advanced in the women in Figure 5 that they each require the use of one or two sticks for support. The pregnant woman on the right of the picture delivered a healthy infant four months before her death. The young boy in Figure 6 has advanced kuru. He is pictured in the middle of a myoclonic body jerk and he has a marked strabismus or squint. Three of the women with kuru in Figure 7 show upper limb postures to prevent postural tremors. Several of these women are seen smiling. Unmotivated laughter is one of the characteristics of kuru.

Figure 5 Kuru victims at the Kuru Research Centre, New Guinea, Reference Gajdusek and Zigas1957.

Figure 6 A boy from the Fore tribe, New Guinea, with advanced kuru, Reference Gajdusek and Zigas1957.

Figure 7 Five women with kuru, Reference Gajdusek and Zigas1957.
2 The Discovery of a New Infectious Agent and a New TSE
Gajdusek’s early articles on kuru reveal that he believed the disease to be genetic in nature. In his first published article on the disease in 1957, Gajdusek wrote that ‘clinical observations, along with further epidemiologic study, suggest a possible genetic etiology or, at least, hereditary predisposition for this unusual condition’ (Reference Gajdusek and ZigasGajdusek and Zigas, 1957, p. 974). In a 1965 paper, he remarked that ‘in view of the absolute ethnic limitation of the disease overriding all boundaries of custom and environment, some genetic mechanism must form the basis for it’ (Reference Alpers and GajdusekAlpers and Gajdusek, 1965, p. 852). It was only later that Gajdusek began to characterise kuru in terms of an infectious disease caused by an unconventional virus. In his Nobel Lecture on 13 December 1976, he stated that:
Kuru has led us … to a more exciting frontier in microbiology than only the demonstration of a new mechanism of pathogenesis of infectious disease, namely the recognition of a new group of viruses possessing unconventional physical and chemical properties and biological behaviour far different from those of any other group of micro-organisms. However, these viruses still demonstrate sufficiently classical behaviour of other infectious microbial agents for us to retain, perhaps with misgivings, the title of ‘viruses’.
The agent that Gajdusek took to be a virus we now know to be an infectious protein called a ‘prion’ (see Figure 8). Prions are unconventional agents in several respects. Scientists have so far failed to locate any nucleic acid within prion proteins. This is significant in that nucleic acid is the basis of cell replication and information transfer in all other pathogens known to man. Also, these proteins display ‘extraordinary resistance’ to various physical and chemical challenges. Storage in 10 per cent or 12 per cent formalin for periods ranging from 6–28 months is known not to inactivate this infectious agent (Reference PattisonPattison, 1965). These proteins can survive unusually high doses of ionising radiation (Reference Gibbs, Gajdusek and LatarjetGibbs et al., 1978). They are also resistant to heat and are incompletely inactivated at 100°C (Reference Gajdusek, Lecture and LindstenGajdusek, 1976). Many deadly viruses, including Ebola virus, human immunodeficiency virus (HIV), and SARS-CoV-2, are inactivated at temperatures below 100°C. The remarkable robustness of prions to physical and chemical challenges raises special considerations around the sterilisation of instruments used in neurosurgical procedures, an issue that was exposed with the first cases of iatrogenic transmission of another prion disease, Creutzfeldt–Jakob disease, through the use of neurosurgical electrodes (Reference Gibbs, Asher, Kobrine, Amyx, Sulima and GajdusekGibbs et al., 1994).

Figure 8 Prion protein. Four nerve cells in a mouse illustrate how infectious prion protein moves within cells along neurites, the wire-like connections that nerve cells use for communicating with adjacent cells.
While Gajdusek’s investigations of kuru had failed to describe the infectious agent responsible for this disease – it was the electron microscopy work of Patricia Merz that first led to the identification of prion rods or strands in cells in 1981 – Gajdusek’s early studies of kuru victims were to have a number of beneficial consequences. Gajdusek and Zigas obtained complete post-mortem examinations on 25 of more than 300 cases of kuru investigated during their first year of field study (Reference Zigas and GajdusekZigas and Gajdusek, 1959). The tissue changes that occurred in the brains of kuru victims were particularly well characterised and included the presence of dark plaques (now known to be bundles of prion protein), loss of nerve cells, and the proliferation of star-shaped cells called astroglia. These features were to grab the attention of an American veterinary neuropathologist, William J. Hadlow, during a visit in July 1959 to an exhibit on kuru held at the Wellcome Medical Museum in London (see Figure 9). Hadlow was struck by photomicrographs of the tissue changes that occurred in the brains of kuru victims. These changes were like those he had witnessed in his work on scrapie, a brain disease of sheep, at the Agricultural Research Council Field Station at Compton in Berkshire. So close was the similarity that Hadlow felt compelled to write to the editor of The Lancet to express his thoughts:
There are certain striking similarities in the histopathology of the central nervous system in each disease. In scrapie, a characteristic finding is the presence of single or multiple ‘soap-bubble’ vacuoles in the cytoplasm of affected nerve cells, and similar changes have been observed in kuru. Certain non-specific neuronal degenerative changes are common to both, also intense astrocytic activity with minimal myelin degeneration … An important discovery has been that scrapie can be transmitted to previously uninfected stock by the intracerebral or subcutaneous inoculation of brain homogenates from affected sheep … The author suggests that experiments should be made to transmit kuru from man to a laboratory primate.
Hadlow also sent Gajdusek a copy of the letter, in which he urged him to attempt experimental induction of kuru in a laboratory primate. In 1936, scrapie had been transmitted for the first time through the experimental inoculation of healthy animals using brain and spinal cord material from diseased sheep (Reference Cuillé and ChelleCuillé and Chelle, 1936). If experimental induction of kuru in a primate proved to be possible, this was evidence of the transmissible nature of kuru and of a link between this human disease and animal disease. In the event, Gajdusek achieved the transmission of kuru to three chimpanzees in 1965, some 18–21 months after having been inoculated intracerebrally with brain suspension from different kuru patients (Reference Gajdusek, Gibbs and AlpersGajdusek et al., 1966).

Figure 9 Dr William J. Hadlow (1921–2015), veterinary pathologist at the National Institutes of Health Rocky Mountain Laboratory between 1952 and 1987; photo taken in 1954. The author wishes to acknowledge NIH History Office.
The demonstration of kuru’s transmissibility to primates firmly established this disease as one of the transmissible spongiform encephalopathies or TSEs. Scrapie was by far the best known of the TSEs by the time Gajdusek was undertaking his primate experiments. The disease takes its name from the scraping action that is performed by an affected sheep, which leads to the deterioration of the fleece (see Figure 10). The UK had substantial expertise in scrapie in the form of three research institutions located in Edinburgh and Berkshire. It was known, for example, that scrapie could transmit to unaffected animals under natural conditions. Both sheep and goats can succumb to the disease after sharing the same pen as infected animals (Reference Brotherston, Renwick, Stamp, Zlotnik and PattisonBrotherston et al., 1968). Even land that is free of scrapie-infected sheep, in some cases for several years, can harbour the scrapie agent and infect a new flock. Maternal transmission of the scrapie agent to offspring is also possible (Reference Dickinson, Stamp and RenwickDickinson et al., 1974).

(A) A sheep with scrapie. An intense itching sensation (pruritus) is one of the symptoms of the disease. This causes the animal to engage in rubbing, scraping, or chewing behaviour, with resulting deterioration of the fleece. © Crown copyright 2011. Published with the permission of the Controller of Her Majesty’s Stationery Office. The views expressed are those of the author and do not necessarily reflect those of Her Majesty’s Stationery Office or the Veterinary Laboratories Agency or any other government department. Lesions in the grey matter of the brain of a sheep with scrapie:

(B) typical spongiform change in neurons (haematoxylin and eosin stain);

(C) spongiform change and astrocytic hypertrophy and hyperplasia (glial fibrillar acid protein stain). Magnification ×500
Figure 10 Sheep and brain section.
Scrapie could also be experimentally transmitted to a range of species, including goats, mice, rats, and hamsters (Reference Zlotnik and RennieZlotnik and Rennie, 1965). Direct inoculation of infected material into the brain was always the most efficient means of transmission. The lymphatic tissues and intestines are first to show infectivity at around 10–14 months of age. The scrapie agent is found in the central nervous system for the first time at around 25 months of age (Reference Hadlow, Kennedy and RaceHadlow et al., 1982). Genes are known to regulate the pathogenesis of the disease by extending or shortening the incubation period. Tissue changes in the brain of diseased sheep are similar to those observed in kuru and include the presence of prion plaques and the appearance of small holes or vacuoles. The exact pattern of brain changes is influenced by the type of scrapie agent used in inoculation. Most animals are between 2–4 years of age when they display signs of the disease (Reference Chatelain, Baron, Baille, Bourdonnais, Delasnerie-Laupretre and CathalaChatelain et al., 1986). Like kuru, the condition is invariably fatal.
For completeness, something should be said about two other animal TSEs, both of which were known to scientists when BSE first emerged in British cattle in November 1986. These diseases are transmissible mink encephalopathy and chronic wasting disease in deer and elk. In the summer of 1963, transmissible mink encephalopathy devastated ranched mink in three outbreaks in Wisconsin, Idaho, and Ontario, Canada. The disease is always fatal once symptoms appear. Outbreaks affect adult breeder animals (over 1 year old). In this type of stock, morbidity may be 100 per cent (Reference BarlowBarlow, 1972). The clinical signs of the disease include locomotor disturbances and excitability. Over a few weeks, this progresses to ataxia which is characterised by stiff, jerky movements. There are increasing periods of somnolence, and affected mink may grasp an object for extended time periods (see Figure 11). During outbreaks, many diseased mink have been found dead, suspended from the walls of their wire cages. Histopathological examination reveals widespread spongy transformation in the cortical and subcortical grey matter accompanied by astrogliosis. Neurons in the cerebrum, cerebellum, and brainstem undergo degenerative changes. There is cytoplasmic vacuolation of neurons but in a different distribution to that observed in scrapie (Reference BarlowBarlow, 1972).

(A) Mink affected with encephalopathy may appear somnolent and grasp an object for extended time periods. (Photograph taken from Virus Infections of Carnivores, M. J. Appel (ed.), Elsevier Science Publishers B.V., 1987. The permission of Elsevier to reproduce this photograph is gratefully acknowledged.)

(B) A haematoxylin and eosin stain (also referred to as H&E) section of the thalamus of mink at the stage of clinical disease with TME. The diseased mink was experimentally inoculated with TME by the oral route. Like spongiform encephalopathies in other species, there is extensive vacuolation.
Figure 11 Mink and brain section.
Chronic wasting disease is known to affect Rocky Mountain elk, mule deer, and black-tailed deer. Many affected animals have been held in captivity in wildlife facilities in Colorado and Wyoming. In elk, the duration of illness is 1–6 months, and in mule deer it is 2 weeks–8 months (Reference Williams and YoungWilliams and Young, 1980; Reference Williams and YoungWilliams and Young, 1982). Elk have been known to develop this disease after coming into sporadic fence-line contact with clinically affected deer or being kept in pens that housed such deer. Behavioural changes are observed in affected animals and include nervousness or hyperexcitability, alterations in personality, and changes of behaviour towards handlers. Progressive weight loss leads to emaciation (see Figure 12). The course of the disease is usually interrupted by complications (e.g. pneumonia) or euthanasia. Histopathological examination reveals lesions in the grey matter of the central nervous system. Lesions are bilaterally symmetrical. There is spongiform change, vacuolisation in neurons, and astrocytic hyperplasia and hypertrophy (Reference WilliamsWilliams, 2005).

Figure 12 Elk and deer infected with chronic wasting disease.
There is extensive wasting of the neck, flank, and hindquarters of these animals. The vast majority of infected cervids never reach the symptomatic stage of CWD. Infected animals usually succumb to predation, vehicle collisions, or other diseases long before they show outward symptoms of CWD.
When BSE emerged in British cattle in 1986, kuru was one of three TSEs known to affect humans. The other two were Creutzfeldt–Jakob disease (CJD) and Gerstmann–Sträussler–Scheinker syndrome. Creutzfeldt–Jakob disease was by far the best known. In 1986, three forms of CJD were recognised: sporadic, iatrogenic, and familial CJD. Sporadic CJD occurs in approximately 1–1.5 people per 1 million population per year (Centers for Disease Control and Prevention, 2022). Males and females are affected with roughly equal frequency, and onset typically occurs in the sixth and seventh decades of life. Iatrogenic CJD is related to medical intervention. Cases of iatrogenic CJD have arisen following the use of contaminated electrodes during neurosurgery, the use of dura mater grafts and corneal transplants, and the treatment of growth hormone deficiency with pituitary-derived growth hormone. A familial form of CJD also occurs. This is an inherited form in which there is a pathogenic mutation in the prion protein gene PRNP. Familial CJD is less common than sporadic CJD. Approximately 15 per cent of human prion diseases are inherited (Reference Clift, Guthrie, Klee, Boczek, Cousin, Blackburn and AtwalClift et al., 2016).
A fourth type of CJD, variant CJD, was first identified in 1996 by the National CJD Surveillance Unit in Edinburgh (now known as the National CJD Research & Surveillance Unit). As of July 2021, there have been 178 deaths in the UK related to variant CJD (Reference Ritchie, Peden and BarriaRitchie et al., 2021) (see Figure 13). Its sufferers are typically younger than in other types of CJD. Among the 178 cases of variant CJD in the UK, the median age at onset was 26 years (range 12–74 years) and the median age at death was 28 years (compared with 67 and 68 years as the respective medians for sporadic CJD) (Reference Brandel, Knight, Pocchiari and MansonBrandel and Knight, 2018). Variant CJD is the only form of CJD to be linked to an animal TSE, namely BSE in cattle. Histopathological findings on post-mortem examination include neuronal loss, intracytoplasmic vacuolation, spongiosis, and astrocytosis (see Figure 14).

Figure 13 Memorial plaque.
A plaque in memory of vCJD victims, close to St Thomas’ Hospital, near the River Thames walkway opposite the Houses of Parliament in London.

(A): The most common subtypes (MM1 and MV1) of sporadic CJD. (1) low power micrograph in routine H&E stain of the neocortex (NCtx) with underlying white matter (WM). These two parts make up the gyri or winding pattern of the cerebral hemispheres. Note the delicate speckled aspect in the lower layers of the neocortex; these are tiny vacuoles that are indicated by arrows in the enlargement in (2). The darker triangular or rhombic shapes in (2) are the neurons. (3) shows the delicate granular prion protein (PrP) deposits made visible with an antibody to PrP. This pattern of PrP is deposited on nerve cell synapses; hence, this is called a synaptic pattern. (Reproduced with kind permission of Dr Gerard H. Jansen, Neuropathologist for the Eastern Ontario Regional Laboratory Association at The Ottawa Hospital, Canada, and Canadian Reference Neuropathologist to the CJD surveillance.)

(B) vCJD. (4) low power micrograph showing neocortex and WM (stained blue). Arrow indicates a florid plaque, with detail of same plaque in (5) and PrP stain in (6). Panels (5) and (6) are rotated at 90 degrees to (4). The florid plaque is named after the plaque centre which has a radiant aspect and looks like a flower heart, and the vacuoles surrounding it which are then the petals of the flower.
Figure 14 Sporadic and variant CJD brain sections.
Gerstmann–Sträussler–Scheinker (GSS) syndrome was the third human TSE known to scientists when BSE emerged in British cattle. It is another inherited prion disease that is caused by mutations in the PrP gene PRNP. In the medical literature, GSS has been described in several Italian families. In one family with a four-generation pedigree, GSS was identified in 11 patients (Reference De Michele, Pocchiari, Petraroli, Manfredi, Caneve, Coppola, Casali, Saccà, Piccardo, Salvatore, Berardelli, Orio, Barbieri, Ghetti and FillaDe Michele et al., 2003). The mean age at onset in these patients was 41.4 years. This is an earlier age of onset than in CJD. Gerstmann–Sträussler–Scheinker syndrome differs from CJD in several other respects. It is known to progress more slowly than CJD. The mean disease duration to death in 4 of the 11 patients studied by De Michele et al. was 5.5 years. This compares to a mean survival of 4–8 months in sporadic CJD (Reference Sitammagari and MasoodSitammagari and Masood, 2022). The age at death is typically lower in GSS than in CJD. Amyloid plaques, which are found in the brain tissue of 10–15 per cent of sporadic CJD patients, are a consistent finding in GSS subjects (Reference LiberskiLiberski, 2004). Spongiform change is less severe in GSS than in CJD (see Figure 15).

(A) low power micrograph of temporal neocortex showing multicentric plaques (red dots) even at this power (H&E stain).

(B) shows multiple cores, referred to as multicentric plaques, in detail.

(C) is a low power image stained for PrP. The very high plaque load is visible in brown and shows that all the cores of the multicentric plaques and their immediate vicinity of the neocortex are filled with PrP.

(D) This is shown in detail in.
Figure 15 GSS brain sections.
One of the subtypes of genetic human prion diseases.
3 The Emergence of a New Brain Disease in Cattle
With the exception of variant CJD, these human and animal TSEs were to form the knowledge base that scientists used in their assessments of the health risks posed by BSE. When pathologists at the Central Veterinary Laboratory in Weybridge, Surrey first diagnosed a novel spongiform encephalopathy in cattle from two different herds at the end of 1986, little could they have known of the animal and human health crises that lay ahead. By March 1996, when the then Secretary of State for Health, Stephen Dorrell, announced to the British Parliament that BSE was the most likely cause of several cases of variant CJD in young people, some 160,000 cattle affected by BSE had been slaughtered. A further 30,000 animals suspected of BSE, but not confirmed to have the disease, had also been slaughtered. As of 13 June 2022, 178 people have died of variant CJD in the UK. Readers may consider this a relatively minor loss of life compared to the large death toll exacted by the COVID-19 pandemic. But they should also consider that the true magnitude of variant CJD may still lie ahead of us. A study of 32,441 archived appendix samples in UK hospitals has revealed that 1 in every 2,000 people is currently incubating this disease (Reference Gill, Spencer, Richard-Loendt, Kelly, Dabaghian, Boyes, Linehan, Simmons, Webb, Bellerby, Andrews, Hilton, Ironside, Beck, Poulter, Mead and BrandnerGill et al., 2013). In the absence of a reliable test for variant CJD, the National Health Service in the UK has had to place many thousands of blood donors ‘at risk’ for public health purposes. Currently, people who have received a blood transfusion in the UK since 1980 are not permitted to donate blood and other tissues. People who are potentially at risk from CJD are not permitted to donate blood, tissue, or organs, including eggs and sperm for fertility treatments. A further precaution is the removal of white blood cells, which may carry the greatest risk of transmitting CJD, from all blood used for transfusions.
In addition to the sizeable human and animal health costs of the BSE epidemic, there has been a considerable economic cost to the UK. In April 2000, the British government estimated that by the end of the 2001/2002 financial year, the total net cost of the BSE crisis to the British Exchequer would be £3.7 billion. Exports of British beef would take much longer to recover, with exports to the US only resuming on 30 September 2020. My own work in this area has attempted to address this question: to what extent could these adverse consequences have been mitigated by an analysis of the reasoning employed by scientists who were charged with undertaking risk assessments of BSE? To tackle this question, I must first say something about the committees and individuals who were involved in BSE risk assessments.
Making assessments of the human health risks posed by BSE was by any standard a formidable task. Bovine tissues were used, directly and indirectly, in the production of a vast array of food products, cosmetics, medicines, and materials used in surgical procedures (see Box 1). Apart from the consumption of red meat, the root gland of the bovine tongue was used to produce pregastric lipase, an enzyme employed in cheese production. The thymus gland was consumed as the delicacy ris de veau on the European Continent. Bovine fat was used in the production of toothpaste, chewing gum, and topically applied medicines. Bovine eyeballs were dissected in British schools. The trachea or windpipe was used to produce pharmaceuticals that treated arthritis. The pituitary gland and adrenal glands were used to produce growth hormones and steroids, respectively. Bovine hearts were used in the production of pericardium patches and valves, both used in heart surgery. Surgical catgut was used in a range of surgical procedures, including neurosurgery. The quantities of bovine intestines that were required to produce it were vast: every year, 25 million metres of bovine intestines from 550,000 cattle, which was 13 per cent of the cattle kill from 18 abattoirs throughout the UK, were used to manufacture it (BSE Inquiry Report, 2000c, Volume 7, p. 151). Bovine uteruses were used in the production of anti-ageing creams, and bovine testicles were used to produce pharmaceuticals that treated cartilage and joint problems. In short, no part of a cow was discarded. With such reliance on bovine tissues, it was clear to all that if BSE were to be transmissible to humans, then there would be multiple routes by means of which transmission could occur. Even the nation’s vegetarians would not be safe from this particular health risk.
Box 1 Uses of bovine tissues at the start of the BSE epidemic
Root gland of tongue – pregastric lipase (cheese production)
Thymus – delicacy on European Continent
Fat – toothpaste, chewing gum, topically applied medicines
Eyeballs – dissected in schools
Trachea – drugs to treat arthritis
Pituitary gland – growth hormones
Adrenal glands – steroids
Heart – pericardium patches, valves
Intestines – surgical catgut
Uterus – anti-ageing creams
Testicles – drugs to treat cartilage and joint problems
To address the many aspects of the BSE problem, a number of expert scientific committees and groups were established by successive British governments. The first of these groups, the Southwood Working Party, was established under Margaret Thatcher’s government on the recommendation of the Chief Medical Officer, Sir Donald Acheson. Its terms of reference were broad: ‘to advise on the implications of Bovine Spongiform Encephalopathy and matters relating thereto’ (BSE Inquiry Report, 2000b, Volume 4, p. 2). The Working Party consisted of experts in human and animal health. Its members were Sir Richard Southwood, Chairman of the Working Party, and a professor of zoology at Oxford University; Anthony Epstein, a professor of virology who conducted research in the Nuffield Department of Clinical Medicine at Oxford; Sir John Walton, a clinical neurologist who was the Warden of Green College, Oxford; and William Martin, a veterinarian with direct knowledge of scrapie who had held the Directorship of the Moredun Research Institute in Edinburgh.
Sir Richard was in no doubt about the seriousness of the task he had been set and the uncertainties that he and his colleagues faced in executing it. In a letter dated 9 August 1988 to a colleague, Dr Poole of the Radcliffe Infirmary in Oxford, Sir Richard wrote ‘[m]y colleagues and I have made various recommendations based, I have to admit, largely on guesswork and drawing parallels from the existing knowledge of scrapie and CJD’ (BSE Inquiry Report, 2000a, Volume 1, p. 55). The Southwood Report was submitted to the government on 9 February 1989. The report concluded that it was most unlikely that BSE would have any implications for human health. However, the general conclusions section of the report ended with this warning: ‘if our assessment of these likelihoods is incorrect, the implications would be extremely serious’.
Several other scientific advisory committees were established with the express purpose of addressing the BSE problem. On the recommendation of the Southwood Working Party, the Tyrrell Committee was formed to advise on research priorities in relation to BSE. This small committee had a fixed membership of just five members, with expertise in areas such as virology, clinical neurology, and TSEs. The Spongiform Encephalopathy Advisory Committee (SEAC) was established in April 1990 ‘[t]o advise the Ministry of Agriculture, Fisheries and Food and the Department of Health on matters relating to spongiform encephalopathies’ (BSE Inquiry Report, 2000d, Volume 11, p. 40). The SEAC had a much larger membership than the Tyrrell Committee. Its membership also varied as scientists with different fields of expertise were recruited to the committee to address specific issues. The SEAC was dissolved on 30 March 2011, with its functions passed to the Advisory Committee on Dangerous Pathogens.
Other, pre-existing government scientific committees were also called upon to consider the BSE issue. Established under Section 4 of The Medicines Act 1968, these so-called Section 4 Committees were heavily involved in assessing the risks posed by BSE for human and animal medicinal and surgical products. These four committees were the Veterinary Products Committee, the Committee on Dental and Surgical Materials, the Committee on the Review of Medicines, and the Committee on Safety of Medicines. Contrary to the widespread public perception of government indifference to the BSE problem, the existence of these various committees demonstrates that this animal and human health issue was at the very heart of government scientific work for many years.
The first cases of BSE appeared in British cattle in November 1986. Affected animals initially displayed altered social behaviour, preferring to stand apart from the herd. They then developed severe locomotor problems. Disturbing images began to appear in the print and broadcast media of cows with their hind legs collapsing beneath them (see Figure 16). Early neuropathological studies confirmed the spongiform appearance of the brain that was typical of the transmissible spongiform encephalopathies. But the origin of this new bovine disease was unclear.

(A) has laid itself down inside its indoor pen, showing signs of lethargy and stupor. The cow in

(B) has isolated itself in a wet area of the pen. Behavioural changes in temperament, including nervousness or aggression, abnormal posture, incoordination and difficulty in rising, decreased milk production, and/or loss of weight, despite continued appetite, are followed by death. (Content Provider: US Department of Agriculture – Animal and Plant Health Inspection Service, APHIS; Photo Credit: Dr Art Davis; Photos taken in 2003; Public Health Image Library:). (Bottom) Section of the lower part of the brainstem (medulla) of a bovine with BSE.

(C) shows H&E-stained section at lower power with a nerve nucleus (aggregate of neurons) with spongiosis circled by arrows.

(D) shows vacuoles/spongiform change indicated by asterisks.

(E) shows the same stained for (light brown) prion protein deposits.
Figure 16 BSE cows and brain sections.
The top photographs show cows with BSE. The cow in
Against this uncertainty, an early hypothesis took hold: scrapie in sheep had somehow transmitted to cattle and this new disease in cattle was effectively bovine scrapie. This set in motion a series of analogical comparisons that informed assessments of the risk that this disease in cattle posed for human health (Reference CummingsCummings, 2015a). Viewing a collapse in consumer confidence in the safety of British beef, government ministers were keen to allay public anxiety by repeatedly producing a statement that the public inquiry into BSE chaired by Lord Phillips later labelled the ‘mantra’ of the BSE crisis: there is no evidence that consuming beef transmits BSE to humans. These analogical and ‘no evidence’ arguments were to become the mainstay of the British government’s response to the BSE problem, an approach that was also echoed by many health officials and industry representatives (Reference CummingsCummings, 2005). But to observers with knowledge of logic and reasoning, it was the beginning of a form of public health communication that posed considerable risks. If the logical underpinnings of this early response to the emergence of BSE were weak, the consequences for public health would be very serious indeed – a point that, as we saw earlier, was subsequently acknowledged by Sir Richard Southwood.
4 Assessing and Communicating the Human Health Risks Posed by BSE
We must now take a logical detour. In examining the risk assessments made by the UK government’s scientific committees, I have argued that we need to begin by treating seriously a group of arguments called the informal fallacies. These arguments have been disparaged as weak or shoddy forms of reasoning by many generations of philosophers and logicians. Labelled by Woods (1992) as ‘the gang of eighteen’, the group includes some well-known names such as false analogy and begging the question, as well as less familiar arguments like post hoc, ergo propter hoc (after this, therefore because of this) (see Box 2). For most traditional philosophers and logicians, these arguments are little more than the deceptive tactics first employed by ancient sophists. Informal logicians have challenged this view by contending that these arguments only appear to be fallacious when we operate with deductive ideals of validity and soundness. When viewed within the actual epistemic contexts in which they are used, these arguments have hitherto unrecognised attributes that can be shown to serve reasoners very well.
Box 2 The Gang of Eighteen (Reference Woods, van Eemeren, Grootendorst, Blair and WillardWoods, 1992)
|
|
For some time, I have argued that the uncertainty that confronts scientists when an infectious disease like BSE first emerges is one context in which the informal fallacies can demonstrate their true worth (Reference CummingsCummings, 2009, Reference Cummings2011, Reference Cummings2020a). I have made this argument in relation to several informal fallacies on the standard list, including argument from ignorance (Reference CummingsCummings, 2002, Reference Cummings2015b), analogical argument (Reference CummingsCummings, 2004, Reference Cummings2014a), argument from authority (Reference CummingsCummings, 2014b), fear appeal (Reference CummingsCummings, 2012), and begging the question (Reference CummingsCummings, 2000). The emergence of a novel infectious disease creates tension between the need to understand the disease and prevent its onward transmission at a point in time when our epistemic resources for doing so are severely constrained. I have argued that the informal fallacies can ease this tension by bridging gaps in our knowledge. This allows inquiry to proceed and, importantly, protective health measures to be taken until such time as a knowledge base can be developed and substantial evidence can be accrued. In this epistemic context, the informal fallacies are the best way of managing the uncertainty that confronts us.
But we are not done. An informal fallacy that can bridge gaps in our knowledge and facilitate decision-making and other actions in a context of uncertainty has all the hallmarks of a cognitive heuristic. A cognitive heuristic is a mental shortcut or quick ‘rule of thumb’ that takes us through short, intuitive steps to solutions to problems. In doing so, it allows us to reduce complex problems to simpler judgemental operations (Reference Tversky and KahnemanTversky and Kahneman, 1974, Reference Tversky, Kahneman and Shafir2004). One such judgement is that if X is not known to be true, then X must be false. Under certain epistemic conditions – to be outlined later in the Element – this lack-of-knowledge reasoning is valid or rationally warranted. Heuristics challenge the widely held assumption that more information results in better or more accurate decision-making (Reference Marsh, Todd, Gigerenzer, Leighton and SternbergMarsh et al., 2004). In fact, simple heuristics have been shown to perform comparably to, and in some cases better than, more complex decision mechanisms (Reference GigerenzerGigerenzer, 2008; Reference Gigerenzer and BrightonGigerenzer and Brighton, 2009). A simple heuristic that detects markers of expertise can, in the right circumstances, provide rational warrant for the truth of an expert’s claims. It allows reasoners to bypass a more extensive deliberation of the evidence which may not be possible if evidence is lacking (such as in 1986 when BSE emerged) or if the available evidence exceeds a person’s knowledge and expertise (the situation that confronts the public). Under these conditions, I have argued that the informal fallacies are a productive source of cognitive heuristics (Reference CummingsCummings, 2014c).
So, informal fallacies have an important role to play during reasoning in contexts of uncertainty. But how exactly can we apply these arguments to the BSE problem? Several informal fallacies were used extensively by scientists during the BSE affair. Two prominent arguments were analogical argument and the argument from ignorance. All analogical reasoning involves drawing a similarity between two objects or situations, A and B. It is argued that if A has a certain property or feature, then B will also have that same property or feature. An analogical argument is rationally warranted when there are particularly strong grounds for claiming that A and B are related. The argument loses its rational force as these grounds become weaker.
Analogical arguments are used extensively in public health reasoning (Reference CummingsCummings, 2004, Reference Cummings2014a). Before HIV had been identified as the cause of early cases of acquired immune deficiency syndrome (AIDS), the Centers for Disease Control and Prevention (CDC) in the US issued public health advice that drew on an analogy between the causal agent in AIDS and another, blood-borne virus – namely, hepatitis B. The CDC had extensive experience of hepatitis B by the time the first cases of AIDS emerged and used its knowledge of the epidemiology of this disease to frame health messages about AIDS to specific populations (e.g., intravenous drug users and homosexual males). Analogical reasoning also shaped early actions in the management of severe acute respiratory syndrome (SARS) when it emerged in 2003. Aileen Plant, a medical epidemiologist who led the World Health Organization’s SARS team in Vietnam, stated in 2008:
[W]e considered that the SARS organism was most likely a virus and spread predominantly via the respiratory route. Hence we acted as though that was true, meaning that infection control, patient management, patient isolation and so on were all treated as though the (assumed) virus causing SARS was similar to other viruses.
During the BSE crisis, an analogy between BSE and scrapie was used extensively by scientists who were charged with making risk assessments about this new bovine disease. In relation to the question of BSE’s transmissibility to humans, the argument took the following form:
MAJOR PREMISE: BSE is similar to scrapie in sheep.
MINOR PREMISE: Scrapie has not transmitted to humans.
CONCLUSION: Therefore, BSE will not transmit to humans.
Analogical reasoning based on scrapie was also the basis of the decision to exclude calf tissues such as the thymus from the human Specified Bovine Offal ban. This was a measure introduced in November 1989 with the purpose of removing infective bovine tissues from the human food chain. In this case, the argument unfolded as follows (LRS stands for lymphoreticular system):
MAJOR PREMISE: BSE is similar to scrapie in sheep.
MINOR PREMISE: In scrapie, the thymus is lower risk than other LRS tissues.
CONCLUSION: In BSE, the thymus will be lower risk than other LRS tissues.
Both these analogical arguments contain strongly warranted minor premises. In the first argument, there were strong grounds for claiming that scrapie had not transmitted to humans. When BSE first emerged in British cattle, scrapie had been endemic in the sheep population of the UK for some 250 years. Extensive epidemiological studies conducted in the UK and elsewhere had failed to find any evidence of a link between eating sheep meat and the development of CJD in humans (Reference Brown, Cathala, Raubertas, Gajdusek and CastaigneBrown et al., 1987). In the second analogical argument, scientists also had strong grounds for the claim that the thymus gland in sheep contained less scrapie agent than other tissues in the lymphoreticular system and, therefore, posed less risk than those tissues. The pathogenesis of scrapie had been extensively studied over many years (Reference CummingsCummings, 2010). Scientists knew the order in which sheep tissues became infected with scrapie agent and the level of infectivity in specific ovine tissues.
The difficulty for scientists using these arguments lay not in the rational warrant of the minor premises – these premises were well supported – but in the decidedly weak rational standing of the major premise in each case. Certainly, early epidemiological, histopathological and molecular evidence suggested that BSE and scrapie were similar diseases. The distribution of early BSE cases was consistent with scrapie transmitting to cattle through their consumption of scrapie-infected sheep tissues in commercial feed (Reference Wilesmith, Wells, Cranwell and RyanWilesmith et al., 1988). Early investigations of the brains of BSE cattle at the Central Veterinary Laboratory had revealed the same pattern of vacuolation and cell abnormalities that were known to occur in scrapie (Reference Wells, Scott, Johnson, Gunning, Hancock, Jeffrey, Dawson and BradleyWells et al., 1987). Molecular studies of brain tissue from diseased cows had revealed a bovine homologue of the prion proteins found in scrapie-infected sheep brains (Reference Hope, Reekie, Hunter, Multhaup, Beyreuther, White, Scott, Stack, Dawson and WellsHope et al., 1988). Notwithstanding the convergence of these three strands of evidence, the only decisive way to establish if BSE and scrapie were related diseases was to conduct strain-typing studies. The techniques that made these studies possible were not available to scientists when BSE first emerged. In their absence, the major premises of these analogical arguments were somewhat tentative and any conclusions based on these premises were weakly warranted at best. However, this is not the end of the story.
When strain-typing studies were eventually performed, they revealed that BSE was distinct not only from scrapie but also from all other naturally occurring TSEs. Yet, even in the absence of the very studies that would have provided definitive evidence of the nature of the relationship of BSE to scrapie, these weakly warranted analogical arguments were performing an important heuristic function in the reasoning of scientists. One such function was the licensing of public health actions, such as the introduction of the human Specified Bovine Offal (SBO) ban, in advance of evidence emerging from experimental studies. The SBO ban was a key measure to protect public health. In the public inquiry into BSE, Lord Phillips and his team remarked of this ban:
The introduction of this vital precautionary measure was commendable. However, this ban was presented to the public in terms that underplayed its importance as a public health measure.
Given the lengthy incubation periods of TSEs (running to several decades in some cases), experimental results could not be achieved within the sort of timeframe that would be required to avoid health risks to humans from BSE, should such risks exist. The relatively speedy manner with which this ban was introduced was at all possible because of analogical reasoning based on scrapie. Moreover, the extent of this ban – knowing which bovine tissues to include in the ban – was directly predicated upon what was known about the pathogenesis of scrapie. Scientists had extensive knowledge of the infectivity of different ovine tissues with the progression of scrapie disease. They used this knowledge to exclude tissues from calves under six months old from the SBO ban, for example.
As well as warranting the introduction of public health measures, the scrapie analogy also enabled scientists to institute a BSE research programme within a relatively short timeframe. By December 1988, the Central Veterinary Laboratory at Weybridge in Surrey already had an extensive research programme into BSE underway. Five experiments were in progress, addressing questions in the areas of epidemiology, clinico-pathological studies, transmission, molecular biology, and molecular genetics. In all five areas, research was based upon similar investigations that had been conducted into scrapie. The first species chosen to undergo experimental inoculation with BSE-infected material – marmosets, mink, goats, mice, sheep, and hamsters – had already been shown to be susceptible to scrapie. Establishing the parameters of this transmission research would have been a much more costly process, in terms of both time and resources, had a well-developed research framework relating to scrapie not already existed. Experimental inoculation studies, for example, took considerable time to produce results. The research programme that would eventually establish the host range of scrapie commenced in 1965 and took until February 1988 to demonstrate transmission of scrapie to marmosets.
A second informal fallacy that played a significant role during the BSE affair was the argument from ignorance. This single-premise argument typically took the following form:
PREMISE: There is no evidence that BSE is transmissible to humans.
CONCLUSION: Therefore, BSE is not transmissible to humans.
In any argument from ignorance, a reasoner argues from a lack of knowledge or evidence that X is true to the conclusion that X is false (similarly, from a lack of knowledge or evidence that X is false to the conclusion that X is true). This argument is more or less strongly warranted based on the satisfaction of two conditions. The first condition concerns the knowledge base in a certain area or domain. If this base is complete or closed, in the sense that it contains all the information that is relevant to a particular issue, it is said to exhibit epistemic closure. The second condition concerns the extent to which the knowledge base is examined or searched. A knowledge base that is exhaustively searched satisfies the search condition. If a knowledge base satisfies both conditions – that is, it displays epistemic closure and is exhaustively searched – the resulting argument from ignorance is strongly warranted. Ignorance arguments that fall short of full epistemic closure and are only partially searched are less strongly warranted.
An example of a strongly warranted argument from ignorance was employed by Brown and his co-investigators in 1987. These investigators conducted a fifteen-year investigation of CJD in France and a review of world literature on the epidemiology of scrapie and CJD. They arrived at the conclusion that scrapie was not transmissible to humans using the following argument from ignorance:
PREMISE: There is no evidence that scrapie is transmissible to humans.
CONCLUSION: Therefore, scrapie is not transmissible to humans.
This argument satisfied the epistemic closure and search conditions. There was epistemic closure of the knowledge base on the epidemiology of scrapie and CJD by 1987: a large number of studies conducted across several countries had examined whether a link existed between scrapie in sheep and CJD in humans. Brown and his colleagues had also completed an exhaustive search of this knowledge base. This was undertaken as part of their review of the world literature on the epidemiology of scrapie and CJD. With both conditions satisfied, the conclusion of the foregoing argument from ignorance was derived by means of modus tollens, a deductively valid inference of the form If P then Q; Not-Q; Therefore Not-P:
MAJOR PREMISE: If it were true that scrapie is transmissible to humans, then we would know that scrapie is transmissible to humans.
MINOR PREMISE: But we do not know that scrapie is transmissible to humans.
CONCLUSION: Therefore, it is not true that scrapie is transmissible to humans.
For scientists, this conclusion was something very much worth knowing. Or, at least, it would have been if its implications had been fully considered. The knowledge that scrapie had not transmitted to humans despite their ingestion over many years of meat from sheep populations in which scrapie was endemic should have raised concern about the bovine scrapie hypothesis of BSE. It was initially hypothesised that each case of BSE was an index case caused by the ingestion of scrapie-infected feed. Mr John Wilesmith of the Central Veterinary Laboratory’s Epidemiology Department concluded:
The form of the epidemic was typical of an extended common source in which all affected animals were index cases … The findings were consistent with exposure of cattle to a scrapie like agent, via cattle feedstuffs containing ruminant-derived protein.
For this to be the case, the oral route would need to be a particularly efficient route for transmission of the scrapie agent to other species. However, the lack of scrapie transmissibility to humans via the oral route over many years clearly indicated that this was not the case. The conclusion of the foregoing argument from ignorance provided scientists with an early sign that the bovine scrapie hypothesis was mistaken and should be rejected. The failure to consider the full logical implications of this argument was to prove a costly error in the public health response to BSE.
In the aforenoted case, an argument from ignorance resulted in a conclusion that could have been used in subsequent reasoning about the origins of the BSE agent had a more thoroughgoing analysis of its logical implications been undertaken. The conclusion of this argument provides support for the minor premise in the following modus tollens inference:
MAJOR PREMISE: If each BSE case is caused by the transmission of scrapie to cattle, then the oral route must be efficient at transmitting the scrapie agent to other species.
MINOR PREMISE: The oral route is not efficient at transmitting scrapie to humans.
CONCLUSION: Therefore, each BSE case is not caused by the transmission of scrapie to cattle.
As well as providing propositions that could be used in other reasoning about BSE, the argument from ignorance served another heuristic function during the BSE crisis. Consider the following ignorance argument, repeated from earlier:
PREMISE: There is no evidence that BSE is transmissible to humans.
CONCLUSION: Therefore, BSE is not transmissible to humans.
This argument did not satisfy the epistemic closure and search conditions that must be fulfilled for an argument from ignorance to be rationally warranted. The long incubation period of TSEs meant that even if BSE were transmissible to humans, it would take many years for this to become apparent to investigators. In the early years of the BSE epidemic, this knowledge base was not closed. Yet, there was still a certain heuristic value for investigators in using the foregoing argument. By presenting the question of BSE’s transmissibility to humans as disconfirmed, rather than unconfirmed, which it actually was, investigators could remove this question from further consideration in inquiry. This was a beneficial move for investigators in the following respect. Ethical considerations prevented scientists from performing the experiments on humans that could directly answer this question. The lengthy incubation period of TSEs meant that even if BSE were transmissible to humans, it would probably be many years before natural transmission to humans would reveal this to be the case. Given that an answer to the question of BSE’s transmissibility to humans was unlikely to be forthcoming in either the short or the longer term, there was little to be gained for scientists in continuing to address this question. By excluding it from further consideration in inquiry, investigators could direct their cognitive and technical resources to other questions for which there was a reasonable prospect of obtaining answers.
The informal fallacies served several heuristic functions during the UK’s BSE crisis. Analogical arguments allowed scientists to devise public health measures such as the human SBO ban and to develop a programme of BSE research; arguments from ignorance generated propositions that could be used in reasoning about the origins of BSE and to set aside questions that could not be directly addressed. Similar rational gains were also achieved through arguing in a circle (begging the question) and arguing from authority (Reference CummingsCummings, 2010). Through warranting public health actions (the introduction of the human SBO ban) and facilitating judgements and decision-making, these arguments emerged as a valuable cognitive resource in the management of the uncertainty that surrounded this new brain disease in cattle. But these arguments are not unique to the BSE problem. To the extent that they are rational adaptations of our cognitive resources to the uncertainty that confronts us, they should be found in other domains when actions and decisions must be taken in the absence of knowledge. In the next section, I argue that this is in fact the case.
5 Getting Closer to the Fallacies
The BSE problem has still to run its full course. The unsettling finding that 1 in 2,000 people in the UK population are currently incubating variant CJD suggests that this disease could have a destructive legacy that far exceeds the 178 deaths recorded to date. The uncertainty that surrounded BSE when it first emerged continues, albeit in a different form. Although we now know many things about BSE that we did not know in 1986 – it does transmit to humans, and it was not caused by the ingestion of scrapie-infected material in meat and bone meal fed to cattle – there is still much that we do not know, not least of which will be the health outcome for those currently incubating variant CJD. But what the BSE affair has shown us is that human beings can be cognitively resourceful when they are confronted with uncertainty. They draw connections between events and take quick, intuitive steps to bridge gaps in their knowledge. They find ways of turning an absence of knowledge into a positive resource for making decisions and taking courses of action. In short, they engage in leaps, find shortcuts, and fall back on simple rules of thumb that allow them to move forward in their thinking when the only other course of action is to do nothing – a choice that is not neutral but can pose substantial risks.
When navigating uncertainty, the informal fallacies are a rich rational resource that has been bestowed on us by evolutionary pressures. Our survival demands rapid assessment of threats and risks in our environment and a type of cognition that can undertake these assessments. If I see a car moving at speed towards me, I do not take time to perform a detailed calculation of its velocity based on distance travelled in a certain time. Rather, I leap quickly out of its way. And if I leap in time, I am able to avoid death or serious injury and can reflect on the quick thinking that saved my life. Similarly, if I see a man discharging a firearm in the direction of a crowd of people, I do not approach him to establish the make of the gun and the type of ammunition he is using so that I can calculate how many bullets his firearm can discharge in ten seconds. Instead, on the basis of a couple of cues – I see a black object in the man’s hands and I hear the sound of gunfire – I hastily leave the scene and retreat to a safe place. The lesson in both scenarios is clear. Fast, intuitive decisions in these contexts can ensure our survival; lengthy, systematic ones might result in us ending up dead. The cognitive mechanisms that make these life-saving decisions possible did not arise by chance. They are as much a part of our evolutionary design as are our eyes that allow us to see the world around us and our lungs that allow us to extract oxygen from the air that we breathe.
To understand the role that informal fallacies play in our reasoning, we need to think of them as a type of cognitive adaptation to the uncertainty that confronts us in our daily lives. We seldom have full possession of knowledge relating to a problem or issue; even if we did, most lay people would not have the expertise required to comprehend it and make use of it in their reasoning and decision-making. We have to find a way of circumventing gaps in our knowledge and making decisions and judgements efficiently. This is where the informal fallacies come into action. They permit quick, intuitive judgements to be made based on salient features of the problem domain in which they are employed. In the case of the argument from ignorance, these features might be that there is epistemic closure of a knowledge base and that there has been a search conducted of the base. For the argument from authority, salient features or markers of an individual’s expertise might involve qualifications, institutional affiliation, and independence of a range of commercial and political interests. Through their sensitivity to these markers, informal fallacies allow us to come to a judgement by means of quick inferential steps. In the case of an argument from authority, this might be that if person P satisfies markers x, y, and z, then what person P asserts must be true. In effect, the informal fallacies are the same type of cognition that allows us to detect certain cues in our environment (e.g., the sound of a gunshot) and to use these cues to take prompt courses of action (e.g., retreat from danger).
But we are not done. For as well as functioning as a cognitive shortcut or heuristic in reasoning, the informal fallacies can also participate in slower, more deliberative processes of reasoning. We saw this in Section 4 when we considered a deductively valid form of the argument from ignorance. In this case, scientists had the strongest possible grounds for claiming that the knowledge base on the transmission of scrapie to humans was closed: scrapie had been endemic in the UK’s sheep population for some 250 years and had not transmitted to humans. Scientists also had the strongest possible grounds for claiming that the knowledge base had been exhaustively searched: Brown and his colleagues had conduced a wide-ranging review of the world literature on the epidemiology of scrapie and CJD in humans. In this context, an extensive process of evidence gathering and deliberation had taken place and had failed to find any evidence that scrapie had transmitted to humans. On this basis, it could be definitively concluded that scrapie had not transmitted to humans. This conclusion was not arrived at through the quick inferential steps of heuristic reasoning; rather, it was reached through the slower, deliberative processes of systematic reasoning. Where heuristic reasoning was satisfied with the rapid identification of markers like epistemic closure and search, systematic reasoning undertook a detailed examination of every study and finding relating to the epidemiology of scrapie and CJD. No stone was left unturned.
Prior to his death in early 2020, Douglas Walton worked extensively on the informal fallacies. He was part of the Woods–Walton approach to the fallacies that characterised non-fallacious variants of most of the major informal fallacies. In his later work, Walton aligned these arguments with the work on heuristics that was undertaken by cognitive scientists (Reference Gigerenzer and ToddGigerenzer et al., 1999). But he retained his strong identity as an argumentation theorist and his emphasis on argumentation schemes as a framework in which to analyse the fallacies:
Heuristics are clearly related in some way both to defeasible argumentation schemes and to fallacies, as we can see by comparing them. For example, the heuristic ‘If it’s an expert opinion, defer to it’ is clearly related to the argumentation scheme for expert opinion.
According to Reference WaltonWalton (2010), most of the informal fallacies are associated with an argumentation scheme and a corresponding parascheme. The argumentation scheme is part of a newer (in evolutionary terms) cognitive system that operates in a controlled, conscious, and slow manner. This scheme asks critical questions of arguments – questions that are likely to expose logical weaknesses, if such weaknesses exist. The parascheme is a shorter version of the argumentation scheme. It is part of an older cognitive system that uses fast and frugal heuristics to achieve solutions to problems. Some of these heuristics involve jumping to conclusions. Although this is a cognitive strategy that works well enough on some occasions, it can result in errors on other occasions.
Walton demonstrates this view of the fallacies as heuristics in relation to the argument from expert opinion. The parascheme of this argument omits assumptions, exceptions, and one ordinary premise that are integral to the corresponding argumentation scheme. By neglecting these aspects, which confer a slow, deliberative character on reasoning, an arguer can employ a fast heuristic to the effect ‘if it’s an expert opinion, defer to it’ (2010, p. 170). This heuristic is depicted in Figure 17.

Figure 17 Heuristic of argument from expert opinion, taken from Reference WaltonWalton (2010, p. 170).
Whatever framework is ultimately best for capturing fallacies-as-heuristics, it is in some respects less important than the achievements and principles that underpin this view of the fallacies. We can summarise these achievements as follows. Informal fallacies are no longer treated as bad, weak, or shoddy forms of reasoning. Rather, they embody an important type of rationality that serves us well when we must make decisions and take courses of action in contexts of uncertainty. Historically castigated, the fallacies have been successfully rehabilitated – not that they deserved their lowly status in logic in the first place. But while there are still uses of these arguments that are fallacious, we are no longer inclined to think of the fallacies as logical aberrations, pure and simple. We now have a more nuanced appreciation of the logical merits and deficiencies of these arguments that is premised on how they are used in particular contexts.
There is another important achievement to consider. To permit their characterisation as heuristics, the fallacies must be viewed as part of cognition. This cognitive reorientation has connected the fallacies with actual reasoners who make judgements and decisions within various physical limitations and cognitive constraints. One physical limitation above all others – time – may prohibit extended deliberation of an issue, as this can incur costly delays in the implementation of health measures. Actual reasoners also encounter limits on memory, attention, and a range of other cognitive skills. When we talk about a complete knowledge base in a particular domain, as we have done in relation to the argument from ignorance, we are not talking about the knowledge of an ideal reasoner who is not constrained by attention and memory. Instead, we are talking about knowledge that is acquired by reasoners with human cognitive capacities – the type of cognitive capacities that can be exceeded by demands and that can give rise to error.
These noteworthy achievements that underpin the view of fallacies-as-heuristics sit alongside significant principles. The first principle is that when we talk about fallacies-as-heuristics, we are describing a general rational capacity. Although we have examined this capacity in the specific context of expert reasoning in public health, it should in principle be applicable to complex and mundane judgements in all manner of areas. It could be applied, for example, to the types of financial decisions that are made by investors as they navigate the uncertainty of the stock markets. But it may also apply to the judgements that we each make when we are contemplating our ability to repay a mortgage against a backdrop of uncertain employment and unpredictable interest rates. Complex problems generate uncertainties for expert reasoners regardless of the discipline or field under consideration. The same is true for lay reasoners who must address uncertainties when they confront more mundane problems in their daily lives. Both types of uncertainty can be managed by means of heuristic reasoning based on the fallacies.
We can illustrate this point by returning to the BSE problem. When Brown and his colleagues used an argument from ignorance to conclude their investigation of scrapie’s transmissibility to humans, they did so from the perspective of expert reasoners. These scientists examined the epidemiological literature on scrapie and CJD. This literature could only be surveyed and its implications assessed by reasoners with expertise in the epidemiology of TSEs. In this context, the argument from ignorance concluded an extensive process of deliberation by a group of scientific experts:
PREMISE: There is no evidence that scrapie is transmissible to humans.
CONCLUSION: Therefore, scrapie is not transmissible to humans.
Now, imagine that it is 1986 and I am a British consumer who is trying to decide whether it is safe to continue eating beef and beef products. I may have little acquaintance with the BSE problem apart from media coverage on the television. Also, I have not undertaken any research into the potential human health implications of this new brain disease in cattle. Under these circumstances, I may be inclined to accept an argument that is repeatedly put forward by government ministers and health officials. That argument is another argument from ignorance. It unfolds as follows:
PREMISE: There is no evidence that eating beef transmits BSE to humans.
CONCLUSION: Therefore, eating beef does not transmit BSE to humans.
The same type of argument that concluded a process of deliberation by scientific experts is used this time by a lay person to assess personal health risks from the continued consumption of beef. Of course, the rational standing of these arguments differs. We saw earlier that scientists used a rationally warranted argument from ignorance when they concluded that scrapie was not transmissible to humans. The consumer’s use of the same argument is not rationally warranted, however. It does not satisfy the epistemic closure condition on the use of the argument from ignorance; closure of the BSE knowledge base could not be reasonably claimed in so short a time after the emergence of BSE. Setting aside the rational standing of these arguments, the key point remains: the informal fallacy can be used in both expert and mundane reasoning because it involves the exercise of a general rational capacity that is not limited to a particular domain.
The second principle is that the view of fallacies-as-heuristics does not imply a thesis about the infallibility of human reasoning. By challenging the idea that the informal fallacies are inherently fallacious, I am not thereby claiming that there is no such thing as fallacious reasoning. When the British consumer of beef accepts the conclusion of the foregoing argument from ignorance, he has committed an error of reasoning. He has not subjected this argument to proper scrutiny – an intended outcome, no doubt, of those who somewhat glibly proposed it. If he had done so, he would have recognised that the epistemic closure and search conditions on the rationally warranted use of this argument had not been satisfied. We must not correct the excessive swing of the pendulum in the direction of the view that informal fallacies are inherently fallacious by causing it to swing excessively in the direction of the claim that human reasoning is inherently infallible. There is a middle ground in which reasoners can exercise their rational judgement to the best extent possible by using fallacies-as-heuristics. Occasionally, these heuristics lead us into error, as they did for the British consumer. But they guide us well enough for most deliberations for us to want to retain them as part of our rational toolkit.
6 New Challenges: The COVID-19 Pandemic
The COVID-19 pandemic has been a worldwide health emergency like no other. While there was always the realisation that such an event could happen, for most people it was treated as only a theoretical possibility. In early 2020, the global scientific community was abruptly woken from its pandemic slumber. The SARS outbreak of 2003 was an early warning shot of what could happen if a novel coronavirus were to jump from an animal species to humans and then undergo respiratory transmission from person to person. But some seventeen years later, the SARS experience was a distant memory for all but the most committed observers.
So, how did the scientific community respond to the most serious global health threat in more than 100 years? While the biomedical response was impressive, particularly the development of effective vaccines within a year of the emergence of SARS-CoV-2 (see Figure 18), the public health response was altogether more fragmented. Attempts to reduce transmission of the virus in the period leading up to, and beyond, the administration of the first vaccines were disorganised and largely ineffective. Poor public compliance with restrictions was fuelled by strong commercial voices in aviation, hospitality, and tourism that wanted a quick return to normal. Against the clamour, scientists were often disparaged, with many even receiving threats for providing expert advice to governments and expressing their views on COVID-19 in the media. With the exception of frontline medical workers, it appeared that there were few other parties who acted with beneficence during the pandemic.

Figure 18 SARS-CoV-2.
Scanning electron microscope image shows SARS-CoV-2 (round blue objects) emerging from the surface of cells cultured in the lab. The virus shown was isolated from a patient in the US.
Against this background, scientists and the public did their best to navigate their way through this new health threat. There were many logical lapses in the process (Reference CummingsCummings, 2020b, Reference Cummings2021). But rational voices did emerge, and many sound decisions and actions were taken. The informal fallacies were at the centre of the early response to the emergence of SARS-CoV-2. Arguments from ignorance and analogical arguments were used extensively to frame early public health advice from both the World Health Organization (WHO) and the Centres for Disease Control and Prevention (CDC) in the US (Reference CummingsCummings, 2020b, Reference Cummings2021). Many other expert scientific bodies provided advice to national governments on how to address this infectious disease.
In the UK, one such body was the Scientific Advisory Group for Emergencies (SAGE). The first meeting of SAGE to discuss ‘Wuhan coronavirus’ (WN-CoV) was conducted on 22 January 2020. The minutes of the meeting reveal the pervasive uncertainty that existed at the time about this new virus and its human health impact (SAGE, 2020a). A summary of the ‘current understanding’ of WN-CoV in the minutes was noteworthy for the expressions of uncertainty that were used (see Box 3). Viral dynamics, including the sustainability of transmission and the incubation period, were unknown and unclear. There was no evidence about infectivity prior to the onset of symptoms or when symptoms were severe. Information on genetic strain was insufficient. The mortality rate could not be reliably quantified. Other aspects of the virus and its behaviour only appeared to be so or were probably or likely to be the case.
Box 3 A summary of what was known about ‘Wuhan coronavirus’ in SAGE minutes of 22 January 2020
There is evidence of person-to-person transmission. It is unknown whether transmission is sustainable.
The incubation period is unclear – but appears to be within 5 to 10 days; 14 days after contact is a sensible outer limit to use.
It is highly probable that the reproductive number is currently above 1.
It is currently estimated that the mortality rate for WN-CoV is lower than for SARS, but it is too early to reliably quantify that rate.
There is insufficient information currently on the genetic strain to comment on WN-CoV’s origin.
There is no evidence yet on whether individuals are infectious prior to showing symptoms.
There is no evidence that individuals are more infectious when symptoms are more severe, but that is likely.
There appears to be very little genetic diversity in WN-CoV based on sequences available so far.
It is reasonable to argue – based on lessons from MERS and SARS, and consistent with exported cases of WN-CoV – that individuals returning from Wuhan are no longer at risk if they show no symptoms after 14 days.
Against this backdrop of uncertainty, some tentative steps were taken. As shown in Box 3, analogies based on SARS and Middle East respiratory syndrome (MERS) were pressed into action to guide assessments of risk. At SAGE’s second meeting on Wuhan coronavirus on 28 January 2020, caution was raised about drawing an analogy between WN-CoV and SARS and MERS – there were differences in the transmission dynamics of these diseases. But even as this analogy receded slightly, another was coming to the fore. SAGE agreed that it was to base infection control measures on those that were already in place for pandemic influenza:
SAGE urges caution in comparing WN-CoV with SARS and MERS: the transmission dynamics are different … It was agreed that Pandemic Influenza infection control guidance should be used as a base case and adapted.
Modelling of the coronavirus outbreak in the UK was also to be based on pandemic influenza: ‘SAGE also agreed that the UK reasonable worst-case scenario should be based on pandemic influenza planning.’ Alongside analogical templates for how the new virus might behave and how the disease outbreak might develop in the UK, SAGE scientists also made use of the argument from ignorance. The minutes of the thirteenth SAGE meeting held on 5 March 2020 contained the following statement: ‘There are currently no scientific grounds to move away from containment efforts in the UK’ (SAGE, 2020c). That SAGE intended this statement to serve as the premise in an argument from ignorance is evident from this later remark in the same minutes: ‘SAGE concluded that the UK remains in the containment phase of the epidemic’. The argument from ignorance that SAGE employed can be set out as follows:
PREMISE: There are no scientific grounds for the UK to move away from containment efforts.
CONCLUSION: The UK should not move away from containment efforts.
This is a variant of the argument from ignorance that asserts there are no scientific grounds for a claim or proposition as opposed to no evidence or no knowledge (Reference CummingsCummings, 2002, Reference Cummings2010, Reference Cummings2015a). Like these other forms, this variant is only rationally warranted to the extent that it satisfies the epistemic closure and search conditions. In terms of epistemic closure, there was a problem even at this early stage of the pandemic in the knowledge base on this new coronavirus. When this argument from ignorance was used by SAGE, there were grounds for moving away from containment efforts in the UK. As the SAGE minutes recorded, patients with severe COVID disease that was not connected to travel or contacts were already being treated in intensive care units in UK hospitals. This indicated that the virus was transmitting in the community and that containment efforts, such as early detection of positive cases with tracing and isolation of contacts, had already failed to limit its spread:
UK surveillance of intensive care units has identified Covid-19 cases. Not all of these have had overseas travel or contacts, suggesting community transmission is underway in the UK.
So, the knowledge base included evidence that containment had not succeeded in limiting the transmission of the virus and that the pandemic response needed to move to the delay phase – a phase in which efforts were made to slow down the rate of virus transmission. Not only was the coronavirus knowledge base not closed, but it contained evidence that indicated that the pandemic response should move beyond containment efforts. The first condition on the rationally warranted use of the argument from ignorance – epistemic closure – was not satisfied.
We move next to the search condition. Did SAGE scientists at the start of the COVID-19 pandemic conduct an exhaustive search of the knowledge base on novel coronavirus? The short answer is ‘yes’. The knowledge base on novel coronavirus was not well developed at the outset of the pandemic – it could not have been otherwise. But such knowledge and information as did exist was well examined. SAGE scientists considered information on the developing situation in Wuhan, as these comments in the minutes of the first SAGE meeting on 22 January 2020 indicated:
‘It was reported that diagnostic testing capability in Wuhan is overwhelmed.’
‘WHO has received some environmental sampling from Wuhan: information on the zoonotic reservoir may be forthcoming shortly.’
SAGE scientists also had access to clinical information through the National Health Service, including the number of COVID-related hospital admissions throughout the UK, ICU bed occupancy, and demographic information on seriously ill and deceased patients. Although some information was not particularly well developed at the start of the pandemic, when information was available it was fully searched and examined. The second condition on the rationally warranted use of the argument from ignorance – the search condition – was satisfied. But in the absence of epistemic closure, the overall conclusion of the argument from ignorance – the UK should not move away from containment efforts – was not strongly warranted.
So, it emerges that arguments from analogy and ignorance played an important role in the early deliberations of SAGE scientists, with some of these uses more rationally justified than others. These arguments were to continue to play a vital role in SAGE risk assessments during the pandemic. At its seventy-fourth meeting held on 22 December 2020, SAGE discussed the emergence in parts of England of a new variant of SARS-CoV-2: the so-called Alpha variant (B.1.1.7). Of concern was the higher rate of transmissibility of this new variant, as well as its potential to cause more severe clinical disease. In their assessment of these possibilities, SAGE scientists compared the Alpha variant to a new variant that had recently emerged in South Africa. The South African variant provided an analogical template for the reasoning of these scientists:
A variant in South Africa has some similar and some different mutations. It is spreading rapidly and has mutations that raise theoretical concerns in terms of immune recognition.
Arguments from ignorance also continued to be employed by SAGE scientists. At the eighty-fourth SAGE meeting conducted on 25 March 2021, an argument from ignorance was used to reject the hypothesis that women are at higher risk of testing positive for COVID-19 than men:
Analysis of Office for National Statistics (ONS) Community Infection Survey (CIS) data shows no evidence to support the hypothesis that women are at higher risk of testing positive for COVID-19 than men. More men than women have died from COVID-19 in the UK, and the difference in mortality was particularly pronounced in the early stages of the pandemic (before April 2020).
When reconstructed, this argument from ignorance takes the following form:
PREMISE: There is no evidence that women are at higher risk of testing positive for COVID-19 than men.
CONCLUSION: Women are not at higher risk of testing positive for COVID-19 than men.
The CIS data from the ONS was particularly comprehensive. From October 2020 onwards, the ONS conducted 179,000 nose and throat swabs every fortnight across the UK (Office for National Statistics, 2022). A further 150,000 blood tests were also conducted every month. Based on such wide-ranging data, it can be argued that there was full closure and an exhaustive search of the knowledge base on COVID-19 infections (i.e., the epistemic closure and search conditions on the rationally warranted use of the argument from ignorance were satisfied). But even as this argument was rationally warranted, it is important to observe a logical lapse on the part of the SAGE scientists who used it. For, in attempting to support a conclusion about the risk of testing positive for COVID-19, these scientists used grounds that described the risk of dying from COVID-19. This was an illicit shift in the grounds that were needed to support a conclusion about the risk of women testing positive for SARS-CoV-2. Knowing that more men died of COVID-19 tells us nothing about the rate at which women tested positive, as disproportionately more men could die of the virus even as more women tested positive for it. Although the SAGE scientists’ use of an argument from ignorance was logically sound based on the CIS data, they had illicitly shifted the grounds of their argument from testing positive for the SARS-CoV-2 virus to dying of COVID-19.
Thus far, we have examined the judgements of SAGE experts and have found that some of these judgements were sound while others appeared to be of dubious logical standing. But, of course, the COVID-19 pandemic did not only present experts with a challenge in scientific reasoning. If hospitals were not to be overwhelmed, the public needed to comply with measures to reduce the transmission of the virus. SAGE scientists agreed that public compliance and trust would be vital in mounting an effective response to SARS-CoV-2. Minutes of the second meeting of SAGE held on 28 January 2020 emphasised the need for input from behavioural science:
SAGE agreed on the importance of behavioural science informing policy – and on the importance of public trust in Her Majesty’s Government approach.
But SAGE scientists were also of the view that public compliance would not be readily achieved. At the thirteenth SAGE meeting conducted on 5 March 2020, public compliance was directly addressed. Scientists assumed compliance would be low and undertook their modelling on this basis:
The modelling undertaken assumed considerably less than total public compliance for these measures (e.g., 50% compliance for household quarantine).
A clear, consistent strategy was required to communicate the risks to the British public. In the early months of the pandemic in the UK, this took the form of daily, televised broadcasts from Downing Street. These press briefings were led by Boris Johnson (until he tested positive for the virus on 27 March 2020) and other prominent members of the Cabinet. At each broadcast, government ministers were accompanied by prominent medical and scientific experts, including Professor Chris Whitty, the Chief Medical Officer (CMO) for England and the UK government’s Chief Medical Adviser, and Sir Patrick Vallance, the UK government’s Chief Scientific Adviser. Standing behind lecterns with yellow and red warnings that stated STAY HOME≫PROTECT THE NHS≫SAVE LIVES, these individuals were the face of the government’s communication strategy during the first national lockdown that came into force on 23 March 2020. But while this was the most visible display of UK government communication about coronavirus, and an important source of information for millions of people up and down the country, the public turned to many other health agencies and media outlets for guidance on the pandemic. A question of some interest is whether they used the same heuristic strategies as experts as they considered this guidance and assessed the risks of novel coronavirus.
In the rest of this section, I will argue that the public drew heavily on fallacies-as-heuristics as they evaluated information about COVID-19 during the pandemic. In support of this claim, let us consider some of the key actors in the transmission of information to the public. It became apparent during the first national lockdown that one government health official towered above all others in his ability to talk to the public and gain their compliance with the measures that were needed to control COVID-19. That individual was Professor Jonanthan Van-Tam (now Professor Sir Jonathan Van-Tam) (see Figure 19). Van-Tam was Deputy Chief Medical Officer during the pandemic, a position junior to Chris Whitty. But he quickly surpassed his medical colleagues in terms of public trust on all manner of COVID issues, including the easing of restrictions and the need for vaccination.Footnote 1 To understand why this was the case, we need to consider not only how Professor Van-Tam was perceived by the public, but also how he communicated with the public.

Figure 19 Professor Jonathan Van-Tam, Deputy Chief Medical Officer, at a COVID-19 press conference held at No 10 Downing Street.
Trust in experts is a type of cognitive heuristic par excellence. We look to and rely upon experts when we lack knowledge in a domain; we defer to the judgement of experts when we have an issue or problem that we cannot address on account of our ignorance. Experience teaches us that not everyone who claims to be an expert is an expert, and so we must become adept at identifying genuine experts and setting aside individuals whose expertise is illusory. What are the cues or markers that we use to help us make this identification? We can make a start on this question by looking to the empirical literature on trust (Reference CummingsCummings, 2014b). When investigators have examined the factors that lead us to trust experts and agencies on a range of issues – food and drug safety, new technologies, smoking risks, to name a few – they generally identify attributes that relate to an expert’s competence and integrity (e.g., Reference Liu, Bouman, Perlaviciute and StegLiu et al., 2020; Reference Ranney, Jarman, Baker, Vu, Noar and GoldsteinRanney et al., 2018). Competence involves factors such as knowledge, technical skills, and a track record of accuracy. Integrity includes openness, honesty, objectivity, and fairness. These components of trust vary in significance depending on who is making the assessment of trust and the nature of the issue under consideration. I may be more inclined to trust family members and friends than health officials when deciding if I should have a COVID-19 vaccination. Evidence from studies suggests that, for many people, this is in fact the case (Reference Purvis, Hallgren, Moore, Willis, Hall, Gurel-Headley and McElfishPurvis et al., 2021; Reference Tan, Straughan and CheongTan et al., 2022). In this instance, integrity supersedes competence in my assessment of trust.
If we adopt competence and integrity as markers of expertise, we can begin to understand why Jonathan Van-Tam forged ahead of his colleagues in terms of public trust. There was no reason to judge Professor Van-Tam’s competence as significantly superior to that of his other public health colleagues in terms of academic and medical qualification. It is doubtful that the public made any assessment of the qualifications and experience of any of the government’s top COVID-19 advisers. But if it had, it would have found a team of highly accomplished individuals, each with considerable qualification for the roles they were performing. However, if we construe competence more broadly to include communication skills with the public, this is where Professor Van-Tam begins to pull ahead of his colleagues. For it was his communication skills, and specifically his use of heuristics such as analogies, that set him apart from his colleagues. Consider the following train and football analogies that Professor Van-Tam used at press briefings held at Downing Street in late 2020 and early 2021. This was a time when the UK experienced a large second wave of COVID-19 infections and deaths. The first COVID-19 vaccines had shown promising efficacy results and were shortly to be approved for use:
9 November 2020: Train analogy
This to me is like a train journey where you’re standing on the station. It’s wet, it’s windy, it’s horrible. And two miles down the tracks, two lights appear and it’s the train. And it’s a long way off. We’re at that point at the moment. That’s the efficacy result.
2 December 2020: Train analogy
The train has now slowed down safely. It has stopped in the station and the doors have opened. That was the authorization by the MHRA [Medicines and Healthcare products Regulatory Agency]. What we need now is for people to get on that train and travel safely to their destinations.
26 February 2021: Football analogy
It’s a bit like being three nil up in a game and thinking well we can’t possibly lose now. But how many times have you seen the other side take it four three? Do not wreck this now. It is too early to relax.
Professor Van-Tam used the train analogy to explain the development and authorisation of the vaccines to the public. By November 2020, COVID vaccines were showing promising efficacy results. Vaccines were found to produce a good immune response to SARS-CoV-2, indicating for the first time that vaccination could be used in the control of this deadly viral pandemic. But there was still some distance to travel in terms of getting the vaccines approved by the MHRA, the regulatory body for vaccines and other healthcare products in the UK. Professor Van-Tam did not want the public to interpret promising early efficacy results as a sign that SARS-CoV-2 was no longer a serious threat to health, and so he signalled this by describing how we could now see the lights on the train but that the train was still ‘a long way off’. He used the train analogy again at a press briefing on 2 December 2020. By this stage, COVID vaccines had started to be authorised by the MHRA. He compared this authorisation to the doors on the train opening. But he was also at pains to convey that if people did not come forward for vaccination in large numbers – if they did not ‘get on that train’ – then it would not be possible to bring COVID-19 under control. Only then could we expect to lead our lives safely again or ‘travel safely to [our] destinations’. In February 2021, Professor Van-Tam used a football analogy to warn that it was too early to ease COVID-19 restrictions. Doing so early, he claimed, would be tantamount to players thinking they had already secured victory in a football match only to lose in the final minutes of a game.
Through his use of vivid and transparent analogies, Professor Van-Tam had shown himself to be an effective communicator of vaccine information and COVID-19 guidance to the public. His carefully crafted ‘analogical’ communication strategy set him apart from his public health colleagues and elevated him in terms of public trust. Here was a government health official who could talk plainly to people about COVID-19 and explain the risks and benefits in terms that they understood. Through his use of analogies, Professor Van-Tam encouraged the public to process vaccine information and COVID guidance by means of heuristics. This was exactly what people needed at this stage of the pandemic. By late 2020, the public had been exposed to months of information, much of it contradictory, on everything from mask wearing to social distancing. They needed simple heuristics to navigate this quagmire of claims and counterclaims. Professor Van-Tam’s use of analogies served this purpose very well. It made dual use of heuristic reasoning in communication with the public, for not only was the public using heuristic reasoning by appealing to the Deputy CMO’s expertise (see Figure 17), but Professor Van-Tam also used heuristics when he employed analogies to talk about vaccines and restrictions. This heuristic-based public communication strategy is represented in diagram form in Figure 20.

Figure 20 Communication between the public and the UK’s Deputy Chief Medical Officer
7 Implications
The fallacies have been on a remarkable journey. They set out from a position of relative obscurity in the history of logic. A renewed interest in them since the publication in 1970 of Charles Hamblin’s book Fallacies has resulted in more sophisticated analyses of these arguments. The Woods–Walton approach to the fallacies succeeded in characterising non-fallacious variants of most of the major informal fallacies. More recently, a cognitive reorientation of the fallacies has seen them function as heuristics that bridge gaps in our knowledge and facilitate reasoning under uncertainty in other ways. For scholars of reasoning, this journey has been a worthwhile intellectual exploration in its own right. But for health communication scholars, knowledge of the further implications of this work is required. In this final section, I describe three such implications.
Let us return to Professor Van-Tam for our first implication. In the preceding section, we described how he used analogies to good effect in his communication with the public about COVID-19. While this seemed to be an intuitive course of action on his part – if Professor Van-Tam’s use of analogies was a well-rehearsed strategy, it certainly did not appear that way to the public – it was consistent with the finding that the public can be encouraged to process health messages using either systematic or heuristic techniques. For his part, the Deputy CMO was encouraging the public to undertake heuristic processing of his messages on vaccines and COVID restrictions through his reliance on analogies. Reference JohnsonJohnson (2005) states that:
[A] heuristic-systematic model (HSM) separates systematic from heuristic information processing. The systematic approach … is deliberative, attends to detail, weighs alternative views, and assesses argument quality in judging the validity of persuasive messages. The heuristic approach is alert to cues (e.g., trusted groups’ evaluation of the information) and simple decision rules (if encoded in memory, accessible to recall, and deemed reliable) justifying quick intuitive judgment.
The HSM has been investigated in many health contexts, including processing of conflicting information on e-cigarettes (Reference Katz, Erkkinen, Lindgren and HatsukamiKatz et al., 2018), educational messages about progesterone as a risk factor for breast cancer (Reference Hitt, Perrault, Smith, Keating, Nazione, Silk and RussellHitt et al., 2016), and treatment decision-making about prostate cancer (Reference Steginga and OcchipintiSteginga and Occhipinti, 2004). While these studies can establish the types of messages that undergo heuristic or systematic processing, and the audiences that are most likely to undertake this processing, they seldom deliver the conceptual innovations that are required to significantly advance our understanding of heuristic processing. Empirical studies cannot establish the conditions under which it is rational to argue from ignorance, or to use an analogy or a circle in argument, or to reason that because Y follows X that X is the cause of Y (the post hoc ergo propter hoc fallacy). Yet, these conceptual analyses must take place before empirical studies can test heuristic processing of health messages in different audiences. On this view, the informal fallacies are a necessary conceptual driver of the models of heuristic and systematic processing that are examined in empirical studies, not a supplement to these models. If empirical models of message processing are divorced from these conceptual discussions, it is difficult to see how they can achieve their full explanatory potential.
To explore this idea a little further, consider a scenario in which Professor Van-Tam had used a different analogy to talk to the public about COVID vaccines. Let us imagine that instead of comparing vaccine development and authorisation to the arrival and boarding of a train, he had compared it to a trek up a high mountain. On this alternative analogy, the vaccine developers might be compared to the trekkers. The efficacy studies might be equivalent to reaching first base camp and the authorisation by the MHRA might be characterised as reaching the summit of the mountain. Such an analogy would be every bit as vivid as the train analogy and, therefore, would be as likely to undergo heuristic processing as the train analogy. Even in the absence of personally undertaking such a mountain trek, members of the public can easily imagine what it would be like for climbers to achieve each of these milestones on their journey.
However, despite its comparable imageability, a mountain trek analogy would not be rationally warranted in this context. This is because vaccine development, authorisation, and uptake are dissimilar from an arduous mountain trek in a significant way. While a mountain trek analogy might adequately characterise the efforts of vaccine developers, with each key stage of their work (e.g., efficacy results) corresponding to a milestone in the trekkers’ journey (e.g., reaching first base camp), this analogy does not capture public participation in vaccine uptake, a feature that Professor Van-Tam was at pains to emphasise in his messaging. Without the public coming forward for vaccination, the entire vaccine endeavour could not be successful.
It is on the issue of public participation in vaccine uptake that the train analogy is rationally warranted, and the mountain trek analogy is unwarranted. The train analogy captured this vital aspect of Professor Van-Tam’s message – people needed to board the train and travel safely to their destinations – in a way that the mountain trek analogy failed to do so. Clearly, both analogies were highly imageable and were equally likely to induce heuristic processing on the part of the public. But a vital component of Professor Van-Tam’s message – public participation in vaccine uptake – would have been lost in the mountain trek analogy. Identifying this weakness required scrutiny of the rational merits of the respective analogies. This necessitated a prior conceptual appraisal of these analogies that no amount of empirical literature on messages and audiences could achieve. This is what it means to talk about the fallacies being a driver of empirical models of heuristic and systematic processing, and not a supplement to these models. By foregrounding the fallacies, we uncover the rational processes that should drive the design of health messages; by leaving the fallacies in the background, we end up with health messages that might persuade or convince an audience without knowing how or why.
To examine the second implication of this work on fallacies for health communication, we need to consider some of the reasons why health messages to the public often fail to achieve their desired result. Clearly, the public may fail to act on health messages if they lack the knowledge that is needed to understand these messages. The view that the public has a knowledge deficit is supported by studies that show there are low levels of health literacy among the public (Reference Cajita, Cajita and HanCajita et al., 2016; Reference Levy and JankeLevy and Janke, 2016), with poor literacy associated with a range of negative health outcomes (Reference Berkman, Sheridan, Donahue, Halpern and CrottyBerkman et al., 2011). The argument goes that we can address this knowledge deficit by providing the public with more knowledge about the illnesses and health risks that it faces. This is the rationale for health education work that aims to equip people with the knowledge they need to make sound decisions about their health. But if we take seriously what has been said about the informal fallacies in this discussion, then maybe what is required is not more knowledge but better ways of reasoning using the knowledge that is at our disposal. This is because we – the public and experts alike – will always have knowledge deficits, no matter what problem or issue confronts us, but also because there comes a point where further knowledge will not help us arrive at a solution. People can and do make sound decisions about their health based on relatively little knowledge if they manage the knowledge they have in smart ways. This is what heuristics, and the informal fallacies, have taught us.
Let us examine this second implication further. The public has a rational choice to make when it is exposed to messages about risks to its health. It can decide to acquire more knowledge about these risks. This can take many forms, such as listening to health experts on TV as they share their knowledge with the viewing public. It may involve conducting research on the internet, reading books and journal articles, and taking advice from local health professionals. By the end of these efforts, the public will have more knowledge upon which to base its assessments of health risks. The acquisition of more knowledge goes hand in hand with systematic reasoning, as people examine this knowledge in detail and assess its significance for the health behaviours they practice. But the public may also decide that it lacks the cognitive and technical resources that are needed to acquire more knowledge and may opt instead to think in smarter ways about the knowledge that it already possesses. This may involve creating logical analogies based on what is currently known, working out how to draw conclusions from an absence of knowledge, and learning when it is warranted to derive causation between two events based on their temporal order (the post hoc fallacy). The public may be quite adept at assessing health risks using these logical strategies even if not every health decision it takes is shown ultimately to be correct. It will almost certainly have expended less cognitive resources than if it had pursued a systematic approach to message processing.
So, what is the upshot of these deliberations? The upshot is that we should train people in skills of logical analysis rather than give them more knowledge if we want to improve their ability to respond effectively to health messages. Providing training in skills of logical analysis sounds very much like the content of a critical thinking course and, to a certain extent, this is what it does involve. But its focus should be narrower than the content of a traditional critical thinking course. Specifically, it would be a valuable educational effort to encourage people to reflect, among other things, on the conditions under which lack-of-knowledge reasoning is warranted, it is warranted to draw analogies between scenarios, and it is warranted to appeal to the opinion of experts when reasoning about a health issue. These are typical components of a much broader course in critical thinking – components that sadly in many cases still appear under the title of ‘errors of reasoning’. However, they are the components that are most likely to achieve a step change in how people process health messages. Knowledge is, of course, still important; the emphasis on critical thinking is not a rejection of knowledge and should not be taken as such. But knowledge in the absence of the mental shortcuts or heuristics that propel reasoning forward in contexts of uncertainty is not the valuable epistemic resource that we assume it to be.
There is a third implication of this discussion on fallacies for health communication scholars. This implication relates to the expert bodies that make assessments of health risks for onward communication to the public. It cannot have escaped readers’ attention that the scientific experts who sit on these bodies are prone to logical error. We saw this in Section 6 when SAGE scientists shifted grounds in their reasoning and argued from a premise about testing positive for SARS-CoV-2 to a conclusion about dying from COVID-19. Logical errors also arose during the BSE crisis, such as when SEAC scientists failed to question the dominant bovine scrapie analogy when BSE was detected in species that were not within the host range of scrapie (Reference CummingsCummings, 2010). These logical lapses are not unusual in themselves – we all make them. But what is remarkable is how often they pass undetected and unchallenged by scientists and end up firmly established in the wider discourse about a disease and the risks that it presents to human health.
I want to propose the following remedy to this problem: experts in argumentation and reasoning should sit on expert scientific bodies alongside the epidemiologists, virologists, statisticians, and behavioural scientists that we have come to accept as regular members of these bodies. It cannot be acceptable that these logical errors are detected for the first time when public inquiries are established to comprehensively examine issues like BSE and COVID-19, or by academics who uncover them as part of an analysis of public health reasoning undertaken retrospectively. Uncovering these errors long after they have been made and when their consequences cannot be reversed is not conducive to establishing public trust in the work of expert committees. But detecting them as they arise can be achieved if an expert in reasoning and argumentation is embedded in these committees alongside experts in a range of other disciplines. This will allow rigorous logical oversight of the deliberations of these committees to occur, with prompt identification and correction of logical errors and other shortcomings should they arise. If this can be part of the legacy of the COVID-19 pandemic, we might succeed in mounting more effective responses to the pandemics and other health crises that will inevitably afflict us in the future.
Glossary
- Astrocytic hyperplasia and hypertrophy:
Astrocytic hyperplasia and hypertrophy is a reaction of astrocytes to central nervous system (CNS) injury. Hyperplasia (cell proliferation) and hypertrophy (cell enlargement) are a chronic response to injury. Astrocytes may also undergo cellular swelling. This is an acute response to injury.
- Astroglia:
Another term for astrocytes. Astroglia are one of three types of glial cells in the CNS. They maintain homeostasis of the brain by providing metabolic and other support to neurons.
- Astrogliosis:
A process that is designed to minimise and repair damage following an injury to the CNS. There are three types of glial cells in the CNS: astrocytes, oligodendrocytes, and microglial cells. Astrogliosis involves molecular, cellular, and functional alterations in reactive astrocytes.
- Ataxia:
This involves a lack of coordination of muscles in the body which presents as abnormalities in gait, speech changes, and abnormal eye movements. Ataxia is a clinical finding in many diseases (e.g., strokes, neurodegenerative diseases) and mostly involves dysfunction of the cerebellum.
- Brainstem:
The human brainstem is the most caudal part of the brain. It is structurally continuous with the spinal cord and consists of the midbrain, pons, and medulla oblongata. The brainstem contains cranial nerve nuclei and other nuclei. It can be damaged by neurodegenerative diseases (e.g., prion diseases) and other events (e.g., cerebrovascular accidents).
- Bovine spongiform encephalopathy (BSE):
A progressive neurological disorder in cattle that emerged in the UK in 1986. The disease is one of the transmissible spongiform encephalopathies (TSEs), a group of human and animal prion diseases. Affected cattle initially display altered social behaviour and eventually progress to severe locomotor problems.
- Cerebellum:
In humans, the cerebellum is located at the back of the brain beneath the occipital and temporal lobes of the cerebral cortex. The cerebellum does not initiate motor commands. It modifies the motor commands of the descending pathways to make movements more adaptive and accurate.
- Cerebral hemisphere:
see cerebrum
- Cerebrum:
This is the largest part of the brain in humans. It consists of two cerebral hemispheres that are connected by a bundle of nerve fibres called the corpus callosum. Each hemisphere contains a cavity called the lateral ventricle and five lobes: the frontal, parietal, occipital and temporal lobes and insula.
- Creutzfeldt–Jakob disease (CJD):
A human prion disease characterised by spongiform change in the brain, neuronal loss, and proliferation of astrocytes (specialised glial cells that contiguously line the entire CNS). The disease has sporadic, familial, and iatrogenic forms, and, more recently, a variant form that is related to BSE in cattle. All forms of CJD are fatal.
- Central nervous system:
The brain and spinal cord.
- Chronic wasting disease:
A prion disease of deer, elk, reindeer, sika deer, and moose. The condition has been found in the United States, Canada, Norway, and South Korea. Symptoms include drastic weight loss, stumbling, listlessness, and other neurological features. Like all transmissible spongiform encephalopathies, chronic wasting disease is relentlessly progressive to death.
- Cytoplasm:
A thick solution that is mostly composed of water, salts, and proteins. The cytoplasm includes all the material inside the cellular membrane and outside the nuclear membrane.
- Dura mater:
One of three membranes, known as the meninges, that envelope the brain and spinal cord. The dura mater is the toughest of the three membranes and is the outermost membrane. Beneath it is the arachnoid. The pia mater is the membrane closest to the brain and spinal cord. Cerebrospinal fluid (CSF) is found in the ventricles of the brain and the space between the pia mater and the arachnoid. The meninges and CSF protect the CNS.
- Epidemiology:
The study of the prevalence and incidence of a disease or disorder. Prevalence describes the total number of cases of a disease or disorder that exist in a population. Incidence captures the number of newly diagnosed cases of a disease or disorder within a specified time period, typically a year.
- Gerstmann–Sträussler–Scheinker syndrome (GSS):
A slowly progressive neurodegenerative disease that has an autosomal dominant mode of inheritance. It is a rare disease with a prevalence of only 1–10 per 100 million. GSS has been found in a small number of families worldwide. The clinical features are progressive ataxia, dementia, and encephalopathy. In brain cells there are multicentric prion protein plaques.
- Grey matter:
The CNS is made up of grey matter and white matter. The grey matter makes up the outer most layer of the brain. It gets its grey tone from a high concentration of neuronal cell bodies.
- Gyrus: (plural:
gyri) Convolutions that appear on the surface of the cerebral hemispheres. The groove that lies between two gyri is known as a sulcus.
- Histopathology:
The study of changes in animal or plant tissue that is associated with disease or disorder.
- Iatrogenic transmission:
The transmission of an infectious disease from person to person through a medical intervention. CJD has undergone iatrogenic transmission through neurosurgery, corneal transplants, blood transfusions, and use of pituitary gland-derived growth hormones.
- Index case:
The index case is the first recorded case of a disease in an infectious disease outbreak. Finding the index case can help scientists establish the cause of an outbreak.
- Locomotor disturbances:
Any disturbance of the ability to undertake directional movement from one location to another location.
- Lymphoreticular system:
The tissues and organs which produce and store cells that fight infection, and the network of vessels that carry lymph. This includes bone marrow, the spleen, the thymus, and lymph nodes. There is an additional primary lymphoid tissue in the gut of ruminants and humans called the ileal Peyer’s patch.
- Medulla:
see brainstem.
- Myelin degeneration:
The myelin sheath is the insulating fatty substance that envelopes the axons of neurons and permits the propagation of electrical impulses along the length of axons. Many conditions may cause degeneration of the myelin sheath. In multiple sclerosis, the immune system attacks the myelin sheath, leading to its deterioration in a process called demyelination.
- Myoclonus:
Myoclonus is a sudden, rapid, brief, involuntary jerking of a muscle or group of muscles. These shock-like movements may be caused by sudden muscle contractions (positive myoclonus) or sudden losses of muscle tone (negative myoclonus). Many different neurological disorders can cause myoclonus (e.g., multiple sclerosis and Parkinson’s disease). It is, therefore, considered a symptom of neurological disorder rather than a specific diagnosis.
- Neocortex:
As its name implies, the neocortex is the newest addition to the brain in terms of evolution. It is the seat of cognitive abilities and is the part of the brain that makes humans uniquely different from other non-human mammals. The neocortex of humans is a thin, extended, convoluted sheet of tissue with a thickness of 3–4 millimetres.
- Neuron:
A type of cell that is specialised for the transmission of electrical impulses around the body. Neurons or nerve cells consist of an axonal appendage and major dendrites.
- Nucleic acid:
Nucleic acids are the main information-carrying molecules in cells where they direct protein synthesis. There are two main classes of nucleic acids. The genetic material of free-living organisms and most viruses contains deoxyribonucleic acid (DNA). The other class of nucleic acids is ribonucleic acid (RNA). It is found in certain viruses and in all living cells, where it is involved in protein synthesis.
- Pathogenesis:
Literally, how a disease (pathos) begins (genesis) or develops. Diseases may arise from entry of pathogens into the body that secrete toxins, from dysregulation of the immune system, and from processes related to ageing, among other factors.
- Scrapie:
A transmissible spongiform encephalopathy that is found in sheep. The term ‘scrapie’ derives from the scraping action that is repeatedly undertaken by diseased sheep.
- Somnolence:
A state of drowsiness or sleepiness that is a late feature of transmissible mink encephalopathy. Affected mink become less aware of their surroundings and spend much of the time in deep somnolence from which they are not easily aroused.
- Synapse:
Also called the neuronal junction, the synapse is the site of transmission of electric nerve impulses between two nerve cells (neurons) or between a neuron and a gland or muscle cell.
- Thalamus:
In humans, the thalamus consists of two egg-like masses that lie on either side of the third ventricle. It transmits sensory information to the cerebral cortex, and has motor, arousal, and mood functions.
- Thymus:
In cattle, the thymus consists of two parts. One part is located in the cervical region in the neck adjacent to the trachea; the other part is in the thorax region. Along with the spleen and superficial and deep lymph nodes, the thymus is an important organ in the immune system of cattle.
- Transmissible mink encephalopathy (TME):
A transmissible spongiform encephalopathy that occurs in farmed mink. The disease was first identified in 1947 in Wisconsin. It follows an invariably progressive course when symptoms appear. Early symptoms include changes in habits and cleanliness and difficulty eating and swallowing. Affected animals become hyperexcitable, arch their tails over their backs and eventually lose locomotor coordination.
- Transmissible spongiform encephalopathy (TSE):
A group of invariably fatal brain diseases in humans and animals. They are caused by an unusual infectious agent known as prions. Prions cause normal proteins in brain cells to change their form and aggregate in clumps in cells. As their name suggests, TSEs can transmit within species and across species, such as occurred when BSE in cattle transmitted to humans. The most common human TSE is Creutzfeldt–Jakob disease. This can transmit between people through neurosurgery, blood transfusions, and corneal transplants (iatrogenic transmission).
- Vacuolation:
A neuropathological process in human and animal prion diseases that gives rise to the typical spongiform appearance of the brain in transmissible spongiform encephalopathies.
- White matter:
White matter is found in the deeper tissues of the brain. It contains nerve fibres (axons), which are extensions of nerve cells (neurons). Many of these nerve fibres are surrounded by a myelin sheath that gives the white matter its colour.
- Yaws:
A chronic bacterial infectious disease that affects skin, bone, and cartilage. Humans are believed to be the only reservoir and transmission is from person to person. Yaws can be cured with a single oral dose of the antibiotic azithromycin.
Acknowledgement
The author thanks the National Library of Medicine in the USA for making available images from its D. Carleton Gajdusek collection.
Louise Cummings
The Hong Kong Polytechnic University
Louise Cummings is Professor in the Department of English and Communication at The Hong Kong Polytechnic University. She conducts research in health communication and clinical linguistics and is the author and editor of over 20 books in these areas. Prof. Cummings is a member of the Royal College of Speech and Language Therapists and the Health & Care Professions Council in the UK.
About the Series
This series brings together a wide range of disciplines that converge on the study of communication in health settings. Each Element examines a key topic in health communication and is carefully crafted by experts in their respective disciplines. The series is relevant to students, researchers, and practitioners in humanities, medical and health professions, and social scientific disciplines.
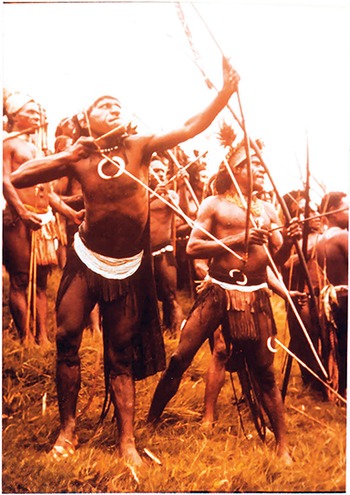


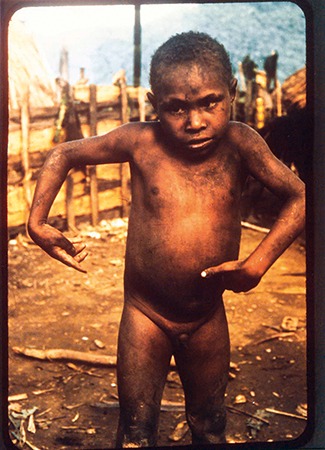

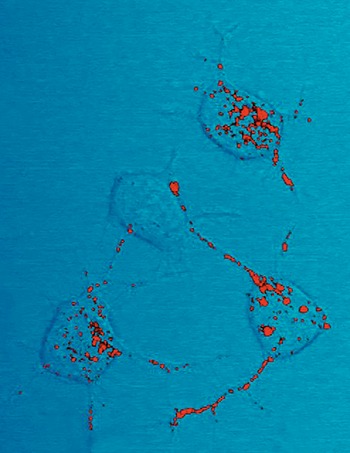





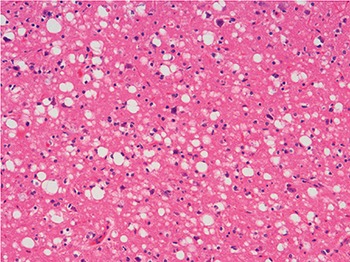
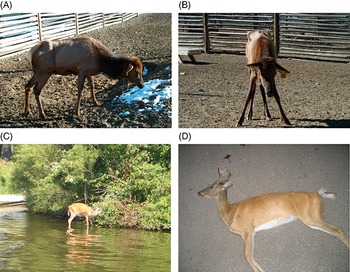

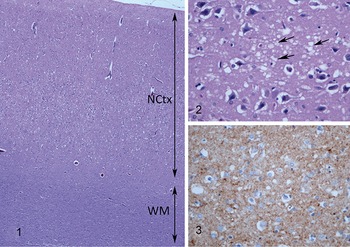
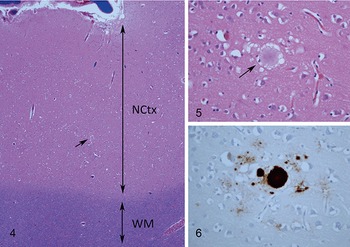






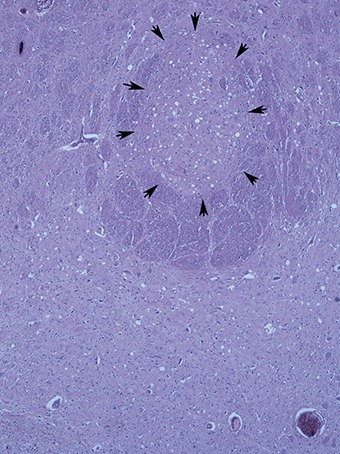



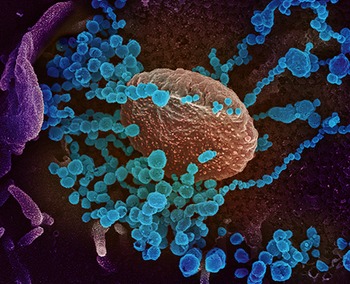



 Open access
Open access