



Introduction
The oldest-old persons
The demographic and social structures of most industrialised and developing countries are changing rapidly as the lifespans of their population increase. The remarkable increase in average lifespan expectancy confirms the positive impact of a variety of factors that slow down biological ageing, including improved nutrition, medical treatment, sanitation and safety (Berk, Reference Berk2004). In Croatia, between 1961 and 2011 the coefficient of ageing increased from 7.4 to 17.7 – that is, the share of older persons more than doubled (Peračković and Pokos, Reference Peračković and Pokos2015).
The oldest-old persons, advanced-agers or ‘centenarians’ in the present study are defined as those aged 80 years and older (Smith and Ryan, Reference Smith, Ryan, Schaie and Willis2016: 304). This age group is usually characterised by more women than men, relatively high levels of comorbidity, dementia, higher dependency and institutionalisation, as well as reduced social interaction and increased consumption of medical services (Felten and Hall, Reference Felten and Hall2001; Smith and Ryan, Reference Smith, Ryan, Schaie and Willis2016). This is also the most heterogeneous age group (Blood and Bamford, Reference Blood and Bamford2010) with the greatest variability in physical (Lowsky et al., Reference Lowsky, Olshansky, Bhattacharya and Goldman2013) and mental health (Scheetz et al., Reference Scheetz, Martin and Poon2012; Wu et al., Reference Wu, Schimmele and Chappell2012). The biography of older persons reflects the gains and losses experienced during their lifetime. The oldest-old persons have usually had diverse and multiple stressful experiences, such as the loss of a spouse and most of their contemporaries, sometimes even the death of children, loss of economic resources or moving to long-term care facilities. In contrast, these oldest-old adults can also look back at many event-related accomplishments and achievements: work success and starting a family, residential moves that brought them more comfort and historical changes (Martin et al., Reference Martin, Da Rosa, Poon, Poon and Cohen-Mansfield2011). Advanced-agers have been exposed to more events and particular challenges in development, but have also had more time to develop effective coping methods (Hayman et al., Reference Hayman, Kerse and Consedine2017).
Wartime experiences
Ageing is framed by historical time and shaped by unique social and cultural conditions (Settersten, Reference Settersten2006). Historical time may result in either cohort or period effects. The effects of a cohort refer to the influence of historical time specific to a group of people born at a particular time. The effects of the period include variations in time periods that affect all populations in society regardless of age and cohort (war, famine, economic crisis) (Victor et al., Reference Victor, Westerhof, Bond, Bond, Peace, Dittmann-Kohli and Westerhof2007). Wartime experiences are ‘hidden variables’ underlying current scientific knowledge about ageing (Settersten, Reference Settersten2006). Older persons who grew up during the Second World War (WWII) underwent multiple traumatic experiences (Strauss et al., Reference Strauss, Dapp, Anders, von Renteln-Kruse and Schmidt2011). War experience, exposure to extreme stress and trauma can affect health and longevity in later life (Schnurr et al., Reference Schnurr, Spiro, Aldwin and Stukel1998; Korinek et al., Reference Korinek, Teerawichitchainan, Zimmer, Brindle, Nguyen, Nguyen and Tran2019). They can lead to a reduction in the quality of life (QoL) (Matanov et al., Reference Matanov, Giacco, Bogic, Ajdukovic, Franciskovic, Galeazzi, Kucukalic, Lecic-Tosevski, Morina, Popovski, Schützwohl and Priebe2013), and the effects of war-related events can last for many years (Freitag et al., Reference Freitag, Braehler, Schmidt and Glaesmer2013). Krause (Reference Krause2004) has provided evidence that greater lifelong trauma is associated with lower levels of life satisfaction (LS). Many studies have shown the negative effects of violence on the lives and health of survivors of 20th-century wars. Only a smaller number of these studies focused on the health and ageing of individuals with wartime experiences (Korinek et al., Reference Korinek, Teerawichitchainan, Zimmer, Brindle, Nguyen, Nguyen and Tran2019). Most research has been based on cohorts of individuals whose lives were marked by WWII, the Vietnam War, the Korean War or, for the earliest studies, the First World War (WWI) (Settersten, Reference Settersten2006). The war survivors are usually grouped into three larger categories: (a) military veterans, (b) concentration camp survivors and prisoners of war, and (c) civilians. Military service affects the ageing process and provides a context for studying optimal versus impaired ageing. It is associated with physical, psychological and social functioning in late life (Settersten, Reference Settersten2006; Spiro et al., Reference Spiro, Schnurr and Aldwin1997, Reference Spiro, Settersten and Aldwin2016).
Holocaust victims in general, and those who survived concentration camps in particular, were the subject of numerous and prolonged stressogenic events. Holocaust survivors represent an exceptional group of people, having been able to counteract enormous physical and psychological hardship and cope with the complicated situation following the war when they suffered grief for family members, but often living to a relatively old age (Konečná et al., Reference Konečná, Lyčka, Nohelová, Petráková, Fňašková, Koriťáková, Polanská Sováková, Brabencová, Preiss, Rektor, Fajkus and Fojtová2019). Old and old-old Holocaust survivors are a select group with a unique biopsychosocial constitution (Shanan, Reference Shanan1989) and provide a paradigm for the special challenges of the long-term effects of extreme trauma (Shmotkin et al., Reference Shmotkin, Shrira, Palgi, Poon and Cohen-Mansfield2011). There are various mechanisms by which old-old Holocaust survivors remain resilient or even show better functioning than their peers (Shmotkin, Reference Shmotkin, Jacoby and Keinan2003).
Only a few studies have been conducted so far on the long-term impact of war on civilians (Bramsen and van der Ploeg, 1999; Waugh et al., Reference Waugh, Robbins, Davies and Feigenbaum2007). Some of the most common war experiences are migration and forced displacement of civilians caused by armed conflicts. Forced displacement in WWII significantly predicts current LS, anxiety symptoms, resilience and protective coping strategies (Steel et al., Reference Steel, Silove, Phan and Bauman2002; Kuwert et al., Reference Kuwert, Spitzer, Träder, Freyberger and Ermann2007, 2009; Freitag et al., Reference Freitag, Braehler, Schmidt and Glaesmer2013).
Quality of life and life satisfaction in older persons
QoL is ‘the individual's perception of his/her position in life within his/her cultural context and value systems, related to his or her objectives, expectations, standards and social relationships’ (World Health Organization, 1998: 551–558). It is a multi-dimensional concept used to capture the quality of the emotional, physical, material and social wellbeing of an individual and a society (Carr and Moorman, Reference Carr, Moorman, Settersten and Angel2011). QoL is both objective and subjective, each axis being the aggregate of seven domains: material wellbeing, health, productivity, intimacy, safety, community and emotional wellbeing. Objective domains comprise culturally relevant measures of objective wellbeing. Subjective domains include domain satisfaction weighted by the importance to the individual (Cummins, Reference Cummins1997).
LS is a subjective evaluation of QoL in general (Fagerström et al., Reference Fagerström, Borg, Balducci, Burholt, Wenger, Ferring, Weber, Holst and Hallberg2007). It refers to life as a whole and reflects a retrospective view of life (Mannel and Dupuis, Reference Mannel, Dupuis and Birren1996; Bowling, Reference Bowling1997). It is therefore an important concept in research on older persons, because it gives a complete overview of the adjustment and adaptive coping ability of the individual (Hamarat et al., Reference Hamarat, Thompson, Steele, Matheny and Simons2002). In gerontology, LS is a concept often used to assess subjective wellbeing (Pinquart and Sörensen, Reference Pinquart and Sörensen2000; Silverman et al., Reference Silverman, Hecht, McMillin and Chang2008), and it is an important factor in successful ageing (Tate et al., Reference Tate, Lah and Cuddy2003; Daatland, Reference Daatland and Johnson2005; Berg et al., Reference Berg, Hassing, McClearn and Johansson2006). LS is used worldwide in research including older adults (Hillerås et al., Reference Hillerås, Jorm, Herlitz and Winblad2001; Borg et al., Reference Borg, Hallberg and Blomqvist2006, Enkvist et al., Reference Enkvist, Ekström and Elmståhl2012; Cho et al., Reference Cho, Martin and Poon2015). Among the variables related to LS in the oldest-old persons, health perception (Borg et al., Reference Borg, Hallberg and Blomqvist2006; Inal et al., Reference Inal, Subasi, Ay and Hayran2007; Chen and Short, Reference Chen and Short2008; Tigani et al., Reference Tigani, Artemiadis, Alexopoulos, Chrousos and Darviri2012), social support (Tsuji and Khan, Reference Tsuji and Khan2016; Chen et al., Reference Chen, Guo and Perez2019), perceived control (Berg et al., Reference Berg, Hassing, McClearn and Johansson2006; Andrew and Meeks, Reference Andrew and Meeks2016) and functional ability (Inal et al., Reference Inal, Subasi, Ay and Hayran2007; Enkvist et al., Reference Enkvist, Ekström and Elmståhl2012) emerged as important aspects of wellbeing. The results of the studies conducted to determine LS among the oldest-old persons suggest an ambiguous picture (Berg, Reference Berg2008). Some studies indicate stability (Diener et al., Reference Diener, Suh, Lucas and Smith1999) or even an increase in satisfaction (Mercier et al., Reference Mercier, Peladeau and Tempier1998; Gana et al., Reference Gana, Bailly, Saada, Joulain and Alaphilippe2013), whereas other studies suggest a decrease in satisfaction (Mroczek and Spiro, Reference Mroczek and Spiro2005; Enkvist et al., Reference Enkvist, Ekström and Elmståhl2012). Inconsistent research findings therefore prevent firm conclusions about LS in the oldest-old age segment.
Concerning gender, some researchers have argued that wellbeing models do not apply to older men and women in the same way (Pinquart and Sörensen, Reference Pinquart and Sörensen2000; Stevens and Westerhof, Reference Stevens and Westerhof2006; Gaymu and Springer, Reference Gaymu and Springer2010; Horstmann et al., Reference Horstmann, Haak, Tomsone, Iwarsson and Gräsbeck2012; Oshio, Reference Oshio2012; Meggiolaro and Ongaro, Reference Meggiolaro and Ongaro2015), because differences in socialisation may lead to gender differences in goals and values and, thus, in sources of LS. Some studies found no differences in LS between older women and men (Bourque et al., Reference Bourque, Pushkar, Bonneville and Béland2005; Tomás et al., Reference Tomás, Sancho, Gutiérrez and Galiana2014), while other studies have found differences, especially in self-perceived health (Murtagh and Hubert, Reference Murtagh and Hubert2004; Berg et al., Reference Berg, Hassing, McClearn and Johansson2006; Škarić-Jurić et al., Reference Škarić-Jurić, Smolej Narančić and Smolić2020).
Aim
In this paper, we investigated whether a life-long impact of the war experiences of the 345 oldest-old institutionalised persons (born in the period 1906–1928) could be detected. Participants in the study experienced war during their lives, some of them even several war events: WWI (1914–1918), WWII (1941–1945) and the Croatian Homeland War (1991–1995). The study participants who reported one or more wars were treated as those exposed to war (‘war-exposed’ group) in the analysis, while those who did not have a direct war experience were treated as non-exposed to war (‘not-exposed’ group).
This paper sought to explore the differences between persons with and without war experiences in their life-history, current QoL and attitudes, as well as in their socio-demographic characteristics. Additionally, the differences among different kinds of war experience were evaluated along with gender-related peculiarities. We expected to find some differences between the ‘war-exposed’ and ‘not-exposed’ groups in terms of their life-history as well as in their socio-demographic characteristics. However, we did not expect to find any differences in their current QoL and attitudes, because the members of both groups are all retirement home residents and are all advanced-agers – that is, those who have successfully overcome all life's challenges.
Participants and methods
Study and participants
The performed analyses are part of the interdisciplinary project ‘HEalth, CUltural, and Biological determinants of longevity: Anthropological perspective on survival in very old age – HECUBA’. This project aims to investigate comprehensively the impact of numerous biological and health-related features – as well as different socio-economic and psychological traits, life-history and cultural factors (attitudes, behaviour, habits) – on long-lived individuals.
The data were collected within the course of the previous project ‘Complex traits variation and health in children, adults and centenarians’. A field study was carried out from 2007 to 2009, and the participants were recruited from 13 retirement homes in Zagreb (all 11 retirement homes in the City of Zagreb, and two private homes located in Zagreb County). Residents 85 years old and older were provided with information on the research procedure and were invited to participate voluntarily. All participants signed informed consent. Fifteen retirement home residents who were under the age of 85 applied to participate in the study. Altogether, 345 very old persons participated in this study, 258 women (74.8%) and 87 men (25.2%) (age range = 79–101 years, mean age = 88.33 (standard deviation = 3.52) years). The gender asymmetry of the sample appropriately represents the population structure for this age group. There were two-thirds more women than men who participated in the research, which is in accordance with census data for Zagreb City, where the proportion of women is 71 per cent in the population group aged 80+ years (Croatian Bureau of Statistics, 2001).
In the framework of this field research, extensive face-to-face interviews performed by trained interviewers, as well as various biometrical measurements, were carried out, while blood samples were taken for haematological, biochemical and genetic analyses. The study protocol was approved by the Ethics Committee of the Institute for Anthropological Research in Zagreb, Croatia.
Definition of war exposure and the structure of the ‘war-exposed’ group
The HECUBA study participants are 345 persons aged 80+ born in the period from 1906 to 1928. The principal target variable of the present study is the direct exposure to war events (mostly to WWII), so the two resulting and contrasted sub-samples are: the ‘war-exposed’ and the ‘not-exposed’. The ‘war-exposed’ group has been selected by their life-history responses, which include: (a) ‘Military’ – active military service (soldiers) or the wounded in the war (soldiers and civilians); (b) ‘Detention’ – imprisonment in concentration camps or prisons; (c) ‘Migration’ – (forced) migration due to the war; and (d) ‘Death in the family’ – war-related death of close family members (parent, sibling, spouse or child).
The structure of the war exposure categories in the ‘war-exposed’ group (112 persons, 139 war exposure events) is presented in Table 1 and Figure 1. One-third of the participants (112, 32.5%) met the described war exposure criteria, 28.6 per cent of all men and 31.0 per cent of all women. The targeted group of participants had one or more war experiences: 14 participants (10.1%) were soldiers or were wounded in war (11 men and three women); 14 participants (10.1%) were in concentration camps or prisons, including those who were imprisoned after WWII for political reasons (six men and eight women); 54 participants (38.8%) migrated or were forcibly displaced at some point in their lives due to the war (21 men and 33 women); and most participants (57, 41.0%; seven men and 50 women) experienced the death of one or more close family members. Out of these, the largest number lost a brother or sister in the wars (38 participants), followed by parents (18 participants) and eight participants lost a spouse in the war. Only one participant had a child killed in the war. Within this group, nine participants experienced two deaths in the family, while one participant lost three close family members in the wars. For some participants, multiple war trauma spans over two wars. Here we present one painful testimony:
My three brothers were killed in 1945, and one sister was killed in 1991 in Vukovar … During the war, in 1945, they made me dig my own grave, and in 1991, I was a refugee from Vukovar in Zagreb. Most of my family moved out to Australia in 1991, during the war, so I don't see them very often. (H39, female, 87)
Table 1. The structure of the ‘war-exposed’ group (112 individuals, 139 war exposure events) of the sample of very old persons

Notes: The difference between men and women in the structure of war exposure events is tested by a χ2-test. Twenty-seven participants experienced two or more war-related events: four individuals who were engaged in military activities or wounded also migrated due to war; two participants who were involved in military actions or wounded have also been in a detention camp; two participants who were in detention camps or prisons also migrated due to war. Nineteen individuals with a death in the family during the war also experienced other war-related events: 14 migrated and one was involved in military activities or wounded. Four participants experienced as many as three war-related events: out of four individuals engaged in military actions and experienced death in the family during the war, two were also in detention camps and two had to migrate due to war.

Figure 1. The structure of the war exposure events by gender in the sample of oldest old persons.
Note: Error bars represent 95 per cent confidence intervals.
A χ2-test showed a significant difference between men and women in the structure of war exposure events (p < 0.001). More men than women were actively involved in war events (fought or were wounded in action as soldiers, were captured and detained in a camp, and/or migrated due to war) and were politically active in the pre-war and post-war periods (political prisoners). Women were more likely to report ‘more passive’ forms of war-related experience, such as death within the family and migration.
Questionnaire
The Questionnaire for the Oldest-Old Persons used in the survey was adjusted to the specific population of oldest-old persons and adapted to the needs of this research. This questionnaire consists of six semi-structured sections. The section on socio-demographic characteristics consisted of general questions, multiple choice and open-ended questions on the participant's age, gender, marital status, education, migration history, employment history, income, and number of children, grandchildren and great-grandchildren. The section on functional ability was used for measuring activities of daily living (personal care, walking, basic domestic chores); it included a set of scales for assessing psychosocial and functional capacity: activities of daily living and the standardised Mini-Mental State Examination test, which evaluates general cognitive functioning and measures eventual cognitive impairment. The health questions addressed medical history, health status and health-related behaviour; it included the Mini-Nutritional Assessment and self-rated health scales.
The section on QoL and LS included questions assessing the quality of past and current life, LS and related aspects. The first set of questions concerned satisfaction with the quality of respondents' past life (six-point scale from 1 = extremely dissatisfied to 6 = extremely satisfied) and satisfaction with the job (responses included a three-step assessment: satisfied, mostly satisfied and dissatisfied). Also included in this set was a question about the best role in their life (parent, spouse, employee, friend, grandfather/grandmother, other roles). In the question ‘What was your favourite role in life?’, participants could choose between one or more options, and choose whether it was being a parent, spouse, worker, friend, grandparent or, in an open-ended question, add a role that was not offered in closed questions. The last question in this set was: ‘When were you most satisfied in your life?’ Respondents could respond by selecting between five offered life periods: childhood, 20–40 years, 40–65 years, 65–85 years and 85+ years. They were asked to explain their choice in an open-ended question.
The next set of questions was about QoL after retirement from work. Participants were asked to rate their satisfaction regarding life in retirement: ‘Overall, how would you say the quality of retired life compares with life when you were working?’ Possible responses were: better, about the same and worse. They were also asked about working after retirement and about new activities they started after retirement. Participants were asked about their physical activity after retirement. Responses included: less physically active, same level of activity or more physically active.
Two sets of questions assessed financial independence. In the first question, participants were asked to identify and describe in what period of their life they had the largest level of financial independence: 20–40 years, 40–65 years, 65–85 years and 85+ years. The second question was about the period of life when they lived in a poor economic/financial situation; participants could choose between the following offered periods and were asked to explain their choice: in childhood, during schooling, when starting a family and looking for a job, after the war (WWI, WWII, the Homeland War). In the end, in an open-ended question, they could add a period that was not offered in the closed questions. The last set about their past life included questions about stressful life events (death of a close family member, divorce, stress at work, retirement, WWI, WWII, the Homeland War, departure of loved ones from home, loss of a pet).
Participants were asked to rate their present LS on a six-point scale (from 1 = dissatisfied, 2 = somewhat satisfied, 3 = moderately satisfied, 4 = mostly satisfied, 5 = satisfied to 6 = completely satisfied) with regard to the question: ‘How satisfied are you with the quality of your present life?’ They were also asked: ‘What do you consider to be your current most significant problem?’ Responses included: poor health, loneliness, financial state, or feeling of uselessness. Two questions on meaning in life and life change were asked in the following order: ‘Would you say that the meaning of your life is/was: family, work, leisure-time activities, or other?’ The open question was: ‘If you had the chance, what would you change in your life?’ The last two questions in the QoL questionnaire were about longevity. They first had to choose the reason for their longevity from the offered answers and then explain their choice. The second question was: ‘What psychological characteristic would you list as the primary driver of your longevity?’
Self-rated health was measured by two linearly added items. Participants rated their general health on a five-point response scale (from 1 = poor to 5 = excellent) and compared their subjective health to that of their age peers on a four-point response scale (from 1 = worse to 4 = better). Participants also self-rated their mobility and independence on a five-point response scale (from 1 = poor to 5 = excellent). The question on social support evaluated relationship satisfaction with family, children, grandchildren and friends on a two-point scale (1 = bad relation or no contacts, 2 = good relation). Social participation evaluated the participation in different social (social, cultural, religious) and leisure activities and hobbies (mental, social, physical).
Statistical analysis
Group differences were tested using Fisher's exact test and Pearson's χ2-test for qualitative variables and by Student's t-test for the quantitative ones, with statistical significance set at p < 0.05 in all cases. Statistical analyses were performed using the SPSS software package 17.0.
Results
Demographic and socio-economic characteristics
Demographic and socio-economic characteristics in the total sample and the ‘war-exposed’ group are presented in Table 2 for quantitative and in Table 3 for qualitative variables. The following features were considered: age cohort (year of birth, age at the time of WWI and WWII, age at interview); longevity (age at death); region of birth; current living situation (duration of stay in the retirement home); family data (current marital status, age at first marriage, number of children, grandchildren and great-grandchildren); education (duration of elementary and secondary school, as well as the total years of both, graduated from college or university); employment and retirement history (age of first employment, age at retirement, number of employment years, duration of separate life from family because of job); wealth/monthly income (pension category); current health and functional ability status (self-rated health, mobility and independence); and LS (job satisfaction, satisfaction with overall life and with present life).
Table 2. Demographic and socio-economic quantitative characteristics in the total sample (N = 345) and in the ‘war-exposed’ group (N = 112; 32.5%)

Significance level: * p < 0.05 (Student's t-test).
Table 3. Demographic and socio-economic qualitative characteristics in the total sample (N = 345) and in the ‘war-exposed’ group (N = 112; 32.5%)

Significance level: *p < 0.05 (χ2-test).
The eldest person was born in 1906 and the youngest in 1928. The mean age at interview was 88.3 years. The mean age at death was 92.6 years. At the follow-up (30 June 2018), 311 (90%) participants were deceased, and the oldest person died at 106.7 years of age. Most participants in the study (53.7%) were born in the city of Zagreb and nearby regions (north-west and central Croatia), while some were born in Adriatic Croatia (21.5%) and East Croatia (9%). Fifty-three participants (15.8%) were born abroad, most coming from other former Yugoslav states (46, 13.7%). As many as 268 (77.7%) respondents had already been born when WWI began, 40 participants (11.6%) were born during that war, while 37 participants (10.7%) were born after WWI. At the beginning of WWII, 64 participants (18.6%) were minors, while 281 (81.4%) were 18+ years old. The third war that took place in Croatia was the Croatian Homeland War (1991–1995), and 197 participants (57.1%) were in advanced old age (70 years) at that time. Within our sample, 308 participants (89.3%) had survived all three wars.
According to the Student's t-test (Table 2), the differences between the two groups were significant for three variables: the ‘war-exposed’ persons had a larger number of grandchildren and great-grandchildren (2.4 versus 2.0 and 1.5 versus 1.1, respectively). On the other hand, the ‘not-exposed’ group had a higher number of elementary school years (4.4 versus 4.2).
A χ2-test showed significant differences in four qualitative socio-demographic characteristics (Table 3). Within this 1906–1928 birth cohort, a bigger percentage of ‘war-exposed’ persons survived until their 95th birthday compared to the ‘not-exposed’ group. The two groups also differed in region of birth, where the ‘war-exposed’ group in higher percentages consisted of persons born in coastal (Adriatic) parts compared to other regions of Croatia. The remaining two differences appeared in terms of the number of offspring: the ‘war-exposed’ group more frequently had three or more grandchildren and great-grandchildren.
The impact of war exposure on life-history, quality of life and current attitudes
The significant differences in life-history, quality of current life and attitude characteristics of the ‘war-exposed’ group in comparison to the rest of the sample of the institutionalised 1906–1928 birth cohort are presented in Table 4. In comparison to the ‘not-exposed’ persons, the change in place of residence due to the war was significantly a more frequent answer in the total ‘war-exposed’ group and in both genders, while the change of the place of residence due to political reasons was a more frequent answer in the total ‘war-exposed’ group and in men. The change in place of residence because of employment was a less frequently confirmed option in ‘war-exposed’ than in ‘not-exposed’ women.
Table 4. ‘War-exposed’ group differences from the rest of the sample of oldest old persons in life-history (LH), current quality of life (QoL) and attitudes (Atd) characteristics

Notes: The differences between ‘war-exposed’ and ‘not-exposed’ groups are tested by a χ2-test. ns: not significant (p > 0.050).
In comparison with the ‘not-exposed’, ‘war-exposed’ persons more frequently confirmed that in leisure time they talked with friends or neighbours, and the significance of this difference was attained for the total sample and for both genders. The ‘war-exposed’ women more frequently than the ‘not-exposed’ women confirmed that they were intellectually active (reading, writing, following actualities and new insights). The answer that they regularly played chess or used the internet was more frequently answered among ‘war-exposed’ persons, and significance (marginal) was reached only at the level of the total sample. Only the ‘war-exposed’ men significantly less often responded that they lived with their partner (marital or not).
‘War-exposed’ persons more frequently consider the age 20–40 as the most satisfying period of their life, and that relation was significant in women and at the total sample level. The same groups more rarely answer that a poor economic situation occurred during their education period. ‘War-exposed’ persons more frequently chose the option that being a parent was the favourite role in their life than the ‘not-exposed’; however, this relation was not significant within gender groups.
‘War-exposed’ women more frequently consider that the major problem of old persons is poor health. On the other hand, that the major problem of old persons is loneliness is less frequently considered in the ‘war-exposed’ women group, and this difference was also significant at the total sample level. ‘War-exposed’ women (also significant at the total sample level) consider the greatest stress in their life was something that was not directly asked in the questionnaire (open part of the question). They named various sources of stress, such the death of a close family member and their children's problems (financial situation, unemployment, health problems).
Compared to the ‘not-exposed’, ‘war-exposed’ women were less likely to declare that they found the meaning of life in their job. ‘War-exposed’ men consider their job to cause the greatest stress in their life, and this relation was significant at the total ‘war-exposed’ group level as well. ‘War-exposed’ women (and this relation was significant also at the total sample level) more frequently think that the most influential psychological initiator of longevity was religion and spirituality. On the other hand, ‘war-exposed’ men think that the most crucial cause of longevity is friends.
Effects of kind of war exposure on life-history, quality of life and current attitudes
Despite numerous similarities, several characteristics related to specific life-history traits, QoL peculiarities, and some attitudes and reflections distinguish the ‘war-exposed’ group according to their kind of war experience. The significant differences within the ‘war-exposed’ group are presented in Table 5.
Table 5. The structure of differences within the ‘war-exposed’ group in life-history (LH), current quality of life (QoL) and attitudes (Atd) characteristics

Notes: 1 See textual explanation for the difference at the level of the total sample and within particular gender groups. The differences among different ‘war-exposed’ experience groups are tested by a χ2-test. ns: not significant (p > 0.050).
Military group
There are three highly significant (p < 0.01) answers that distinguish the ‘war-exposed’ persons by type of war exposure where the Military strongly differed from other groups: they more rarely have good relations with children and also more rarely used to have a pet. On the other hand, all three women belonging to this group declared that there was a poor economic situation in the period when they formed their families. The other two, to a lesser degree, significant variables (p = 0.01–0.05) point to this group: they more frequently started a new activity after retirement. They find that right now (in their eighties), they enjoy the highest level of financial independence.
Detention group
The prominent characteristic of this group is that they are financially the best off among the ‘war-exposed’ groups: all members of this group have at least moderate pensions and many of them belong to the higher pension categories. This group's members are prominent in their frequent claims that they changed the place of residence due to political reasons. This group more rarely claims that the greatest psychological initiator of longevity is self-discipline and health maintenance (p = 0.01–0.05).
Migration group
This group more frequently claims that they changed their place of residence due to war and more rarely that they did so due to political reasons. They more frequently used to have a pet, and they also more frequently think that the greatest psychological initiator of longevity is self-discipline and health maintenance.
Death in family group
Members of this group more frequently declare that they have a good relationship with their children, while they more rarely declare a moderate or higher pension. The women in this group were the only ‘war-exposed’ group in which there were participants who do not receive any pension at all. Because women make up the vast majority of this group, there is no relation in the importance for this group significant for the male gender. The only relation that is significant for the total sample level and not for women (indicating a degree of importance for both genders) is the more rarely confirmed statement that they started a new activity after retirement.
Discussion
Previous research in Croatia explored the effect of war on older persons in the period of immediate banishment during the Croatian War of Independence (Despot Lučanin, Reference Despot Lučanin, Krizmanić, Fučkar, Havelka, Barath and Kolesarić1991, Reference Despot Lučanin and Ajduković1993; Ajduković, Reference Ajduković1993; Havelka et al., Reference Havelka, Despot Lučanin and Lučanin1995) and the effect of war and war-inflicted losses on the QoL of older people in the post-war period (Babić-Banaszak et al., Reference Babić-Banaszak, Kovačić, Kovačević, Vuletić, Mujkić and Ebling2002; Poredoš and Ivanec, Reference Poredoš and Ivanec2004). However, so far there has been no research which shows a long-term effect of war and war-related experiences on ageing, longevity and the QoL of very old persons in Croatia.
Our sample did not include older persons living in their own homes, so the obtained results cannot be generalised to all Croatian age peers. Several studies have found differences in terms of age, education, level of mobility and cognitive functions between older adults living in retirement homes and those living in their own homes (Sertel et al., Reference Sertel, Simsek, Yümin, Öztürk and Yümin2011; Del Duca et al., Reference Del Duca, Silva, Thumé, Santos and Hallal2012; Onder et al., Reference Onder, Carpenter, Finne-Soveri, Gindin, Frijters, Henrard, Thorsten, Topinkova, Tosato, Liperoti, Landi and Bernabei2012; Vitorino et al., Reference Vitorino, Paskulin and Vianna2013). Living arrangements play an important role in determining QoL. There are only a few studies that compare QoL among retirement home residents and older community-dwelling persons in Croatia (Brajković, Reference Brajković2010; Rusac et al., Reference Rusac, Vahtar, Vrban, Despot Lučanin, Radica and Spajić-Vrkaš2016; Despot Lučanin et al., Reference Despot Lučanin, Lučanin, Koščec Bjelajac, Delale, Štambuk and Tokić2020). The first one showed that participants who live in a retirement home and had children showed higher LS than those who lived in their own households (Brajković, Reference Brajković2010). The next one revealed that there is no significant difference in LS level nor in self-perceived health between older persons with regards to their living arrangements (Despot Lučanin et al., Reference Despot Lučanin, Lučanin, Koščec Bjelajac, Delale, Štambuk and Tokić2020); older adults also attach more importance to those domains of functioning such as health or social participation that would ensure higher LS in their specific living conditions – an institution or one's own home.
The present study suggests that the ‘war-exposed’ 1906–1928 birth cohort scarcely shows any peculiarities concerning the explored general traits (family and financial status, education and work history, self-rated health, functional ability status and LS). However, several gender-specific differences distinguished the ‘war-exposed’ group as well as the specific groups based on type of war experience. These are related to specific life-history traits, peculiarities of QoL, and some attitudes and reflections.
Socio-demographic features
Among socio-demographic characteristics, the ‘war-exposed’ displayed the following three differences to the ‘not-exposed’ group. A smaller number of elementary school years in persons with war experience is a consequence of changes in duration of elementary school during the 20th century. In 1874, the Croatian Parliament issued the first Croatian Education Act, which regulated a compulsory five-year education. In 1946, seven-year education became compulsory, and this was increased to eight years in 1958, covering all children aged between 7 and 15 (Franković, Reference Franković1958). If war exposure disturbed the regular elementary school attendance of our participants, it had no effect on their total educational attainment, which is visible in the absence of differences between the ‘war-exposed’ and the ‘not-exposed’ groups in terms of the total number of years of elementary and secondary schooling as well as in the proportion of persons with college or university education.
A greater number (three or more) of grandchildren (in the total sample) and great-grandchildren (in the total sample and in men) in the ‘war-exposed’ group is the most intriguing unexpected demographic finding from the present study. It is interesting to note that the two groups did not significantly differ in terms of the number of children and that a significant difference occurred only in the number of more distant descendants. Another issue should be emphasised: the proportion of persons who did not have any offspring at all (in each of the three categories: children, grandchildren, great-grandchildren) was approximately the same in both groups. This relation is presented in Figure 2, where it is visible that there is no difference between the two groups in the proportion of participants who did not have more distant offspring at all. The only difference appears in the number of distant offspring in persons who did have grandchildren/great-grandchildren. One possible explanation for this observed difference in the number of progeny could be cultural, arising from the fact that a higher proportion of ‘war-exposed’ persons were born in coastal (Adriatic) Croatia.
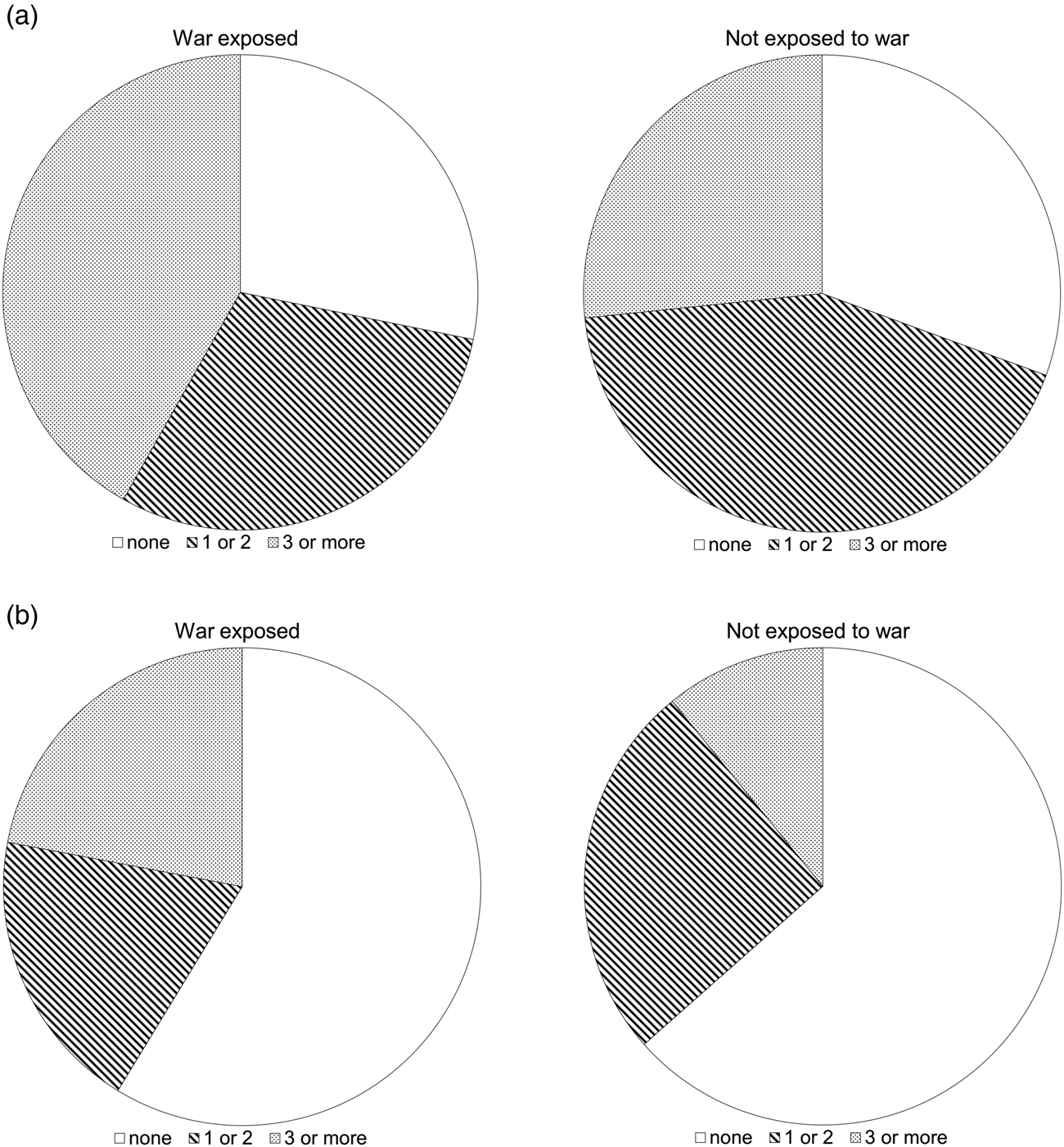
Figure 2. (a) The number of grandchildren in ‘war-exposed’ and in ‘not-exposed’ groups of very old persons. The number of grandchildren is divided into three groups: none, one or two, and three or more. The relation tested by a χ2-test is significant at the total sample level (p = 0.013) but not in men (p = 0.217) and women (p = 0.054). (b) The number of great-grandchildren in ‘war-exposed’ and in ‘not-exposed’ groups of very old persons. The number of great-grandchildren is divided into three groups: none, one or two, and three or more. The relation tested by a χ2-test is significant at the total sample level (p = 0.014) as well as in men (p = 0.026) but not in women (p = 0.117).
Finally, although there was no difference in average duration of life, the group of participants with war experience showed a higher percentage of persons with extreme longevity (95+ years of life). Their war-related experiences and traumas did not prevent them from living to a very old age, which could be attributed to resilience. That our ‘war-exposed’ group managed to live up to 80+ years, and moreover – in comparison to the ‘not-exposed’ group – that a higher proportion of them reached extreme longevity (95+ years), points to resilience as their prominent common characteristic. This can be further illustrated by their testimonies, which presented war trauma not directly captured by our criteria and its true gravity. In their words:
During the war, in the period of the Independent State of Croatia (NDH; 1941–1945), I was in prison and in the camp, I wanted to bribe the guards not to torture me, but I didn't have any money, my folks gave away a pig. (H138, female, 88)
My father was killed in the Jasenovac camp. (H138, female, 88)
My first husband died in 1941, I was married for just four years. (H342, female, 87)
My brother died as an infant, another brother was forcefully mobilised and got killed in Germany, it is not known whether the third brother is still alive. Father died grieving at the age of 64. (H193, female, 88)
My 36-year-old brother died of pneumonia because there was no penicillin, my sister got killed when she was 35 and the other sister was in the camp. (H198, female, 96)
Resilience is the ability to achieve, retain or regain a level of physical or emotional health after a devastating illness or loss (Felten and Hall, Reference Felten and Hall2001). Zautra (Reference Zautra2009) identified two key aspects to resilience: recovery and sustainability. Recovery is the ability to regain functioning after a stressful event or trauma, and sustainability is the ability to endure and persist throughout life's challenges. There is growing evidence that prior exposure to stressful events contributes to resilience during later events (Jennings et al., Reference Jennings, Aldwin, Levenson, Spiro and Mroczek2006). Resilience is either stable or increases with age (Cherry et al., Reference Cherry, Silva, Galea and Cherry2009; Zeng and Shen, Reference Zeng and Shen2010). Developmental and socio-historical context affects the exposure to and the experience, measurement and impact of adversity and resilience. An appropriate conceptualisation of late-life resilience should emphasise subjectivity and life experience concerning the challenges, resources and adaptive outcomes that typically occur for these individuals (Hayman et al., Reference Hayman, Kerse and Consedine2017). Advanced age provides a relevant context for resilience research. The key characteristics of high resilience among older adults include mental, social and physical factors. It has been significantly associated with positive outcomes, including successful ageing, lower depression and greater longevity (MacLeod et al., Reference MacLeod, Musich, Hawkins, Alsgaard and Wicker2016). Most investigators agree that many older persons who endured trauma in early life demonstrate resilience (Schnurr et al., Reference Schnurr, Spiro, Vielhauer, Findler and Hamblen2002). Data suggest that WWII veterans who experienced the greatest adversity during the war showed the most significant improvement in resilience in later life (Elder and Clipp, Reference Elder and Clipp1989). Shmotkin et al. (Reference Shmotkin, Shrira, Palgi, Poon and Cohen-Mansfield2011) have discussed three major modes of surviving into old-old age with lingering trauma: (a) dementia-moulded survival, which raises the question as to whether cognitive impairment sensitises traumatic memories or blunts them; (b) embattled survival, which involves either a chronic confrontation with the past trauma or else its reactivation in the adverse conditions of late life; and (c) robust survival, which maintains the capacity to stay well in the face of age-related challenge as well as past trauma.
The gender-specific impact of war exposure
The present study shows that, despite vast similarities, there are gender-specific elements related to several life-history traits, QoL peculiarities, and current attitudes and reflections that distinguish the group of persons with direct war experience. Given that three-quarters of the HECUBA sample were women, this sex ratio affected some of the obtained results relating to typical developmental, normative events in a woman's life.
Characteristics that are significant (primary) at the total sample level indicate the similarity of men and women in each particular relation. There are two traits that strongly (p < 0.01) distinguish the ‘war-exposed’ versus ‘not-exposed’ groups at the total sample level. Compared to the rest of the sample of very old retirement home residents, the ‘war-exposed’ men and women most strongly (p < 0.001) differed by their more frequent positive answer to the question whether they had changed their place of residence due to war. The second characteristic is that the ‘war-exposed’ men and women more frequently talk with friends or neighbours in their leisure time.
With a lesser degree of significance (p = 0.01–0.05), the total sample shows other relations that are not visible in gender-separated analyses. ‘War-exposed’ persons more frequently played chess or used the internet, and they claimed that being a parent was the favourite role in their life. These findings point to intellectual activities and openness to novelty as an important coping strategy that could have an impact on the successful ageing of these oldest-old persons who, regardless of their war exposure, survived into their eighties. The latter finding points to possible prioritisation of family relations among ‘war-exposed’ persons, which could be the foundation for their larger number of offspring.
There are several differences between men with and without war experience in the sample of very old residents in retirement homes. There are two most significant differences characterising the ‘war-exposed’ men (p = 0.001) but not women: the first is that they more frequently disclosed that they had changed residence for political reasons. The second difference was in their more frequently expressed opinion that one of the most important causes of longevity was friends. With lesser significance (p = 0.01–0.05), the ‘war-exposed’ men are also characterised by the fact that they more frequently declare that currently they are not living with their partner (marital or not). They more frequently consider that the biggest stress in their life came from their work. It seems that, in men, this closer relation with peers is preferred to marital relations. Some research confirmed that comradeship with peers (especially for older men and veterans) was understood as a necessity for wartime survival, imparting lifetime social values that have remained a core aspect of their sense of self in older age (Sixsmith et al., Reference Sixsmith, Sixsmith, Callender and Corr2014).
The most significant differences (p < 0.01) in ‘war-exposed’ women (which were not significant in men) were found in their answers to three questions. They less frequently considered that they had experienced a poor economic situation during their education period. On the other hand, they more frequently chose the period between 20 and 40 years as the most satisfying period of their life. They also considered the greatest stress in their life to be more frequently something that was not directly asked in the questionnaire (open part of the question), naming various sources of stress such as the death of close family members or their children's problems (e.g. financial situation, unemployment, health problems). Several questions with a lower level of significance (p = 0.01–0.05) also characterised ‘war-exposed’ women: they more rarely found the meaning of life in their job, although currently they were more frequently intellectually active (reading, writing, following actualities and new insights). Women with war experience more frequently considered that the primary problem of older adults was poor health, and more rarely that it was loneliness. They more frequently considered religion and spirituality to be the greatest psychological initiators of longevity. This finding is similar to other studies that have found that spiritual life or belief was described as a major strategy for a resilient nature (Reis and Menezes, Reference Reis and Menezes2017; Holston and Callen, Reference Holston and Callen2021).
The gender-specific impact of the kind of war exposure
The kind of war involvement was significantly different for men and women, so it is no wonder that the significance pattern in the two genders mostly seems mutually exclusive. However, two answers were highly significant (p < 0.01) at the total ‘war-exposed’ group level, indicating a certain degree of concordance in the two genders. The first is that the Detention group more frequently and the Death in the family group more rarely have moderate or higher pensions (€260–1,300), and this relation was also significant in women (although to a lesser degree). Among the 17 different groups of receivers of the privileged pension in the Republic of Croatia are the National Liberation War participants, members of the Croatian Home Guard Army 1941–1945, former political prisoners, members of the former Yugoslav National Army, members of the Croatian Army, Croatian Homeland War veterans and members of the Croatian Defence Council. The amount of their pension differs significantly from the amount of regular pensions, and it is significantly higher. According to data from the Croatian Pension Insurance Agency, the average pension for June 2009 was 2,166 Croatian kunas (approximately €290) and the average military pension amounted to 3,525 Croatian kunas (approximately €470) (Bađun, Reference Bađun2009). It is obvious that the Death in the family and Migration groups of persons who experienced war-related damages are not recognised and awarded by Croatian pension regulations, and women constitute the vast majority in those groups.
The same two groups of ‘war-exposed’ persons of both gender (i.e. Death in the family and Migration) shared the second common characteristic: they more frequently declared that they used to have a pet. With a lower degree of statistical significance, there emerged a third characteristic with the two genders' concordance: the more frequent answer in both the Military and the Migration group is that after retirement they started a new activity.
Differences were also found in the sub-sample of men with war experience concerning the type of war experience. According to the kind of war exposure, the most significant (p < 0.01) difference in men was that the change of place of residence due to political reasons was more frequently present in the Detention group and more rarely in the Migration group. At a lower degree of significance (p = 0.01–0.05), men differed in terms of the profile of their war exposure in response to two questions: the Military group more frequently claimed that the life period when they had the greatest level of financial independence was right then (i.e. at age 85 years up to the present), and the Migration group more frequently regarded self-discipline and health maintenance as the greatest psychological initiators of longevity.
Four questions strongly (p < 0.001) distinguished the ‘war-exposed’ women by the kind of war exposure. The change in place of residence due to war was more frequently confirmed in the Migration group and more rarely in the Military and Death in the family groups. Here, it should be noted that among women, not one of the three Military persons chose this answer. Next, among women, the Military group more frequently and the Migration group more rarely declared that a poor economic situation occurred in their family-forming period. The Detention group among women more frequently reported higher pensions (€520–1,300). Finally, a good relationship with children was more frequently declared in the Death in the family (all of them) and Migration groups, and less frequently in the Military and Detention groups.
The structure of war exposure events showed an important difference between men and women. As expected, men were more frequently engaged in military actions or wounded. However, the observed gender difference in the number of deceased close family members in the course of the war cannot reflect real differences. There is probably a gender difference in willingness to report a death in the family during the interview (open part of various questions).
From war experience to successful coping strategies
The answers obtained from ‘war-exposed’ persons according to their kind of war experience form distinct patterns that could be described as follows.
Military group
Their answers indicate that emotional relations (e.g. cultivating good family relations or having a pet) and attachment to their professional career are not among their highest priorities. On the other hand, they present themselves as persons who are content with their current life. We could not judge the causality of this relation, namely we could not test whether the initial personal characteristics were a basis for their military involvement, or if this kind of war experience formed those persons' future unique characteristics. We could only point out that the group of persons with military experience could be characterised as ‘tough’ (colloquially) or ‘resilient’ (scientifically).
Detention group
The pattern of answers points to politics as the most influential factor in the life of persons with detention war experience. They are strongly determined by their particular war experience: positively (with higher income) and negatively (they had to change their place of residence due to politics). Even their attitude towards their longevity – which they do not see as a part of their individual accomplishment and a consequence of their personal investment – could also be regarded as related to some external (political) factors crucial for their longevity.
Migration group
The obtained answers point to the group who experienced migration due to war as persons who think that their actions could impact the quality (e.g. having a pet) and duration of their lives (e.g. active engagement in health maintenance).
Death in the family group
This group has two sources of (maybe interrelated) stress: the premature loss of a close family member and poverty. The lack of interest in new activities (e.g. after retirement) and cultivating good relations with children both seem like an appropriate reaction to those stressors. It could also be regarded that the prevailing gender roles of female participants are a direct consequence of their war-related experience.
Each of the four kinds of war exposure group showed very specific characteristics that could merely be a reflection of their very different gender structure. However, it is also possible that the different life-history, QoL and attitude characteristics distinguishing the four kinds of war exposure might also be regarded as a potential consequence of a particular war experience per se. Research has shown that social activities, social networks, social support and social relationships are important for maintaining cognitive functioning and physical health in old age (Holt-Lunstad et al., Reference Holt-Lunstad, Smith and Layton2010; Kelly et al., Reference Kelly, Duff, Kelly, McHugh Power, Brennan, Lawlor and Loughrey2017). Gender roles and distinct psychological characteristics, but also specific war experiences and their consequences, all modelled the features of different coping strategies that proved to be successful in our sample of the oldest-old persons.
Conclusion
This paper explored the differences between persons with and without war experience in their life-history, QoL and attitudes, as well as in their socio-demographic characteristics. The differences among different kinds of war experience were also evaluated, along with gender-related peculiarities. As expected, we found some differences between the ‘war-exposed’ and ‘not-exposed’ groups in terms of their life-history as well as in their socio-demographic characteristics. However, some unexpected results emerged, such as the higher number of distant offspring in the ‘war-exposed’ persons. Socio-economic situations strongly differed by gender and according to the kind of war exposure, amplifying the differences within the ‘war-exposed’ group in terms of wars' life-long impact on their lives.
Unexpectedly, we found patterns of experience according to the kind of war exposure that stretched through various aspects of the previous and current life-history features, QoL and attitudes. We could not claim that those differences are the direct consequences of the war exposure events per se nor that they are related to the primary personality characteristic that pushed specific war experiences. We only present our findings, which suggest that those differences existed decades after the war. Therefore, we could claim that the war experiences were not the same for everybody, and that they had lasting consequences on the lifecourse of persons who directly faced war-related events.
The gravity of the war experience of persons in this sample are illustrated by their comments given in the open part of the questionnaire, which also pointed to their high resilience capacity as a common feature among persons who survived direct exposure to at least two wars and yet survived to exceptionally old age. It is therefore important to add that those impacts are visible even on advanced-agers – that is, persons who have overcome all life's challenges due to their different but obviously successful coping strategies.
Strengths and limitations of the study
The advantage of this research rests in the fact that it includes a sample of institutionalised individuals of very old age (80+ years). This produces two sorts of strengths: one is that study participants provide a truly life-long perspective that could shed light on the lasting consequences of war experience. The second is that the study includes participants who are all living in a very homogeneous and safe environment that enables us to see effects that are not covered by a variety of distractions caused by the diversities in current life circumstances that could have an immediate impact on self-perceived LS and attitudes. Of importance for future study is the fact that the HECUBA project, being interdisciplinary, could link these results to the outcomes of genetic and biomedical research, which could contribute to a comprehensive understanding of the phenomenon of human ageing and longevity. The limitations of the research are the rather small sample size, particularly for some kinds of war exposure, and the larger number of female respondents in the sample, which affects the results because they represent the attitudes and experience predominantly from a female perspective.
Acknowledgements
We would like to thank all our study participants for their commitment and willingness to join the study, and the administration, medical teams and employees of the retirement homes.
Financial support
This work was supported by the Croatian Science Foundation (IP-01-2018-2497 granted to T. Škarić-Jurić); and the old cohort sample was collected within the project supported by the Croatian Ministry of Science, Education and Sports (grant number 196-1962766-2747).
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
Ethical approval was obtained by the Ethics Committee of the Institute for Anthropological Research, Zagreb, Croatia.








 Open access
Open access