



Introduction
Depression is a common mental disorder in older adults. It is well known that depression increases mortality risk and can have a negative impact on the physical and psychological functioning of older adults (Beekman et al., Reference Beekman, Penninx, Deeg, De Beurs, Geerlings and Van Tilburg2010). Among people aged 60 and above, prevalence rates of mental disorders have been found to be about 15 per cent (World Health Organization, 2017). In China, the pooled detection rate of depression among community-dwelling older adults was 22.7 per cent from 2000 to 2012 (Zhang et al., Reference Zhang, Xu, Nie, Zhang and Wu2012). More study of risk indicators for depression could help to develop policies and interventions that might reduce the risk of depression in older adults in China.
Social participation and depression
Social participation is defined as socially oriented sharing of individual resources (Bukov et al., Reference Bukov, Maas and Lampert2002), and has been found to be an important factor for risk of depression (Lin et al., Reference Lin, Ye and Ensel1999; Cattan et al., Reference Cattan, White, Bond and Learmouth2005; Perese and Wolf, Reference Perese and Wolf2005), especially among older adults for whom social isolation is linked to decline in physical functions and loss of social roles (Lee et al., Reference Lee, Min, Gallagher and Kirkwood2005). However, findings concerning the effect of social participation on risk of depression have not been consistent.
A large body of research has found that social participation is beneficial in preventing depression among older adults and could reduce their symptoms of depression (Lin et al., Reference Lin, Ye and Ensel1999; Cattan et al., Reference Cattan, White, Bond and Learmouth2005; Perese and Wolf, Reference Perese and Wolf2005). How older adults’ social participation benefits their health has been considered from two points of view: on the one hand, older adults might access information or receive social support from their social participation, which could prevent depression (Kawachi and Berkman, Reference Kawachi and Berkman2001; Umberson and Montez, Reference Umberson and Montez2010). Umberson and Montez (Reference Umberson and Montez2010) found that social support derived from social participation could alleviate stress and prevent mental health problems that come from stress. Li et al. (Reference Li, Jiang, Li and Zhang2017) conducted a direct test of this and confirmed the mediating effect of social support from social participation. On the other hand, social participation might produce positive psychological states, which could then have a strong impact on depressive symptoms (Takagi et al., Reference Takagi, Kondo and Kawachi2013; Tomioka et al., Reference Tomioka, Kurumatani and Hosoi2015). In a long-term survey of older adults in Japan, Tomioka et al. (Reference Tomioka, Kurumatani and Hosoi2015) found that social participation could produce positive psychological states including better self-esteem, a sense of belonging and a purpose in life for participants. These positive psychological states have a protective effect on depression (Tomioka et al., Reference Tomioka, Kurumatani and Hosoi2015).
However, a few studies have pointed out that social participation is not all beneficial for older adults’ mental health because it may induce mental stress (Murayama et al., Reference Murayama, Nofuji, Matsuo, Nishi, Taniguchi, Fujiwara and Shinkai2015; Tomioka et al., Reference Tomioka, Kurumatani and Hosoi2017). Social participation may be an additional burden in an already stressful daily life, resulting in a negative association between social participation and mental health (Takagi et al., Reference Takagi, Kondo and Kawachi2013; Tomioka et al., Reference Tomioka, Kurumatani and Hosoi2017). Further, different cultural backgrounds also could explain variation in the influence of social participation. Because of the national antipathy to self-assertion, and the societal value of harmony among people, more Japanese cannot refuse the social participation recommended by acquaintances and participate unwillingly in social groups in greater numbers than Europeans and Americans (Tomioka et al., Reference Tomioka, Kurumatani and Hosoi2017). These inconsistent results suggest that the impact of social participation on older adults’ depression may change as their state of mind changes.
Attitudes towards ageing and depression
Attitudes towards ageing are formed through older adults’ experiences during the ageing process and their evaluation of this process. Such experiences can be divided into two classes: negative experiences (psychosocial loss) and positive experiences (psychosocial growth). Negative experience refers to the experience of losing physical, psychological and other capabilities during ageing (Neupert and Bellingtier, Reference Neupert and Bellingtier2017). Positive experiences refer to the positive feelings about old age, such as better health status and increased wisdom brought by ageing (Laidlaw et al., Reference Laidlaw, Power and Schmidt2007). There is a large body of evidence affirming the effects of attitudes towards ageing on older adults’ mental health (Baltes and Baltes, Reference Baltes, Baltes, Baltes and Baltes1990; Levy et al., Reference Levy, Ashman and Dror1999; Yang et al., Reference Yang, Browning and Thomas2013; Faudzi et al., Reference Faudzi, Armitage, Bryant and Brown2020; Chen et al., Reference Chen, Guo and Perez2021). People who had negative attitudes towards ageing were more likely to believe that depression is an inevitable and normal part of getting older, and such beliefs may prevent older adults from engaging with treatment for depression (Chachamovich et al., Reference Chachamovich, Fleck, Laidlaw and Power2008; Quinn et al., Reference Quinn, Laidlaw and Murray2010; Laidlaw, Reference Laidlaw2010; Liu et al., Reference Liu, Xi, Hall, Fu, Zhang, Guo and Feng2020).
On the other hand, social participation could increase older adults’ chances of interacting with other people, and older adults’ attitudes towards ageing could be constructed through the lens of how they interact with other people, sometimes interpreted as ‘You are as young or old as others make you feel’ (Karp and Yoels, Reference Karp and Yoels1982). Indeed, attitudes towards ageing are inextricably linked with social participation. A study of the relationship between social participation and attitude towards ageing of retired teachers found that active participation is beneficial for older adults’ attitudes towards ageing, even among widows and older adults with poor health (Su, Reference Su2011). This is consistent with the results of Cusack (Reference Cusack2006), who compared attitudes of Canadian and Japanese older adults towards ageing and their participation in learning. Social participation was shown to contribute to a positive attitude towards ageing. Self-confident and active older adults hold more positive attitudes towards ageing, and are role models of healthy and successful ageing (Cusack, Reference Cusack2006).
However, how social participation and attitudes towards ageing impact depression (separately or jointly) in China is not clear. Chinese society is strongly shaped by traditional Confucian culture, whose values are different from those of modern Western culture where values of freedom and personal rights are central. Chinese culture is a collective reference that elevates the consciousness and moral principle of respecting older adults. Hess (Reference Hess, Birren and Schaie2006) found that attitudes and assessments by other people could affect older adults’ attitudes towards ageing. This implies that older adults’ attitudes towards ageing may differ between Chinese society and Western societies, namely older Chinese adults may be more likely to accept their elderly status than in Western societies, where youth is given more cultural value. Meanwhile, everyone lives in a network of interwoven relationships that are closely related to trust in China. Social participation may give older adults more chance to build their circles of friends, integrate into community and improve their mental health, rather than create mental stress. In addition, for Chinese older adults, ‘a near neighbour is better than a distant relative’, they may place more value on relationships with neighbours than Western older adults do. Community participation, which could promote such neighbourhood relationships, may have a positive influence on Chinese older adults’ mental health. Therefore, investigation of the effects of social participation and attitudes towards ageing on depression might contribute to promoting positive ageing and developing health intervention strategies.
To the best of our knowledge, there have been no studies on the relationship between social participation, attitudes towards ageing and depression in China. Only Liu et al. (Reference Liu, Xi, Hall, Fu, Zhang, Guo and Feng2020) found that positive ageing attitudes and available social support were associated with reduced depressive risks, and social support moderated the association between attitudes towards ageing and depressive symptoms (Liu et al., Reference Liu, Xi, Hall, Fu, Zhang, Guo and Feng2020). Social support could reflect one aspect of benefits that older people receive from social participation; however, it cannot represent all aspects of social participation that might affect older adults’ attitudes towards ageing. The main goals of this study are as follows: (a) to examine the association between social participation and older adults’ depression; (b) to examine the association between attitude towards ageing and older adults’ depression; (c) to examine the moderated relationships between social participation and attitude towards ageing on older adults’ depression. In order to avoid issues of reverse causation between social participation, attitude towards ageing and depression, we examine the associations between baseline social participation and attitudes towards ageing and depression in both the baseline and follow-up waves.
Data and methods
Data
This study used two waves of a national representative survey of older adults aged 60 and older from the 2014–2016 China Longitudinal Ageing Social Survey (CLASS). CLASS aimed to collect social and economic data on the Chinese ageing population at both individual and community levels and was conducted by the National Survey Research Center at Renmin University of China. This survey used a stratified multi-stage sampling design. Counties, county-level cities and districts (the county-level areas) were selected as the primary sampling units, and village/residential communities were selected as the secondary sampling units. Data came from 462 communities within 28 provinces, municipalities and autonomous regions; 11,511 older adults completed the survey and provided valid information, of whom 6,908 respondents produced sufficient information in the 2014 baseline survey (they provided completed information on depression and all independent variables); 3,477 follow-up cases in the 2016 survey were used in this study. Descriptive characteristics for baseline variables are reported in Table 1.
Table 1. Descriptive information for the sample in 2014
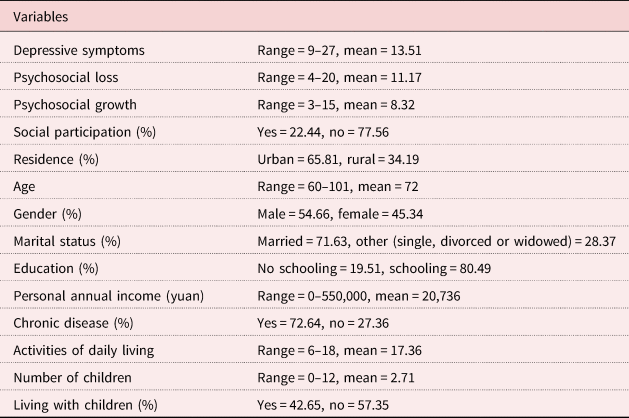
Note: N = 6,908.
Dependent variable
Depression was quantified using the nine-item Center for Epidemiologic Studies Depression Scale (CES-D). This is a standardised scale used to identify clinically depressed people in community samples (Radloff, Reference Radloff1977). The scale contains nine items. For example, the respondents were asked: ‘Did you feel good about yourself’, ‘Did you think your life is going well’ and ‘Did you feel useless’. Respondents replied ‘no’, ‘sometimes’ or ‘often’ to these questions, and the scores for these responses were 1, 2 and 3, respectively. A summary score was created by converting the positive values, with higher scores indicating more depression. Cronbach's alpha for the scale was 0.76. The level of depression was assessed in both 2014 and 2016.
Independent variables
Social participation
The local community is the main venue for older adults in China to acquire social resources and participate in social activities (Sun, Reference Sun2007). The social participation we used in this study was community social participation, and it was measured with the question: ‘Did you participate in any volunteer work at local communities in past three months?’ Volunteer works in local communities included seven items: local community security patrols, help for older adults in daily living and shopping, chatting with others as a psychological consulting service, dispute resolution, environmental sanitation or protection activity, volunteering technical services, and taking care of children from other households. If older adults participated in any of these activities, they were assigned the score 1; they were assigned 0 if they did not participate in any community social activities. This was measured in 2014.
The attitudes towards ageing
Our measure of attitudes towards ageing is a short version of an Attitudes to Ageing Questionnaire (AAQ), developed by Laidlaw et al. (Reference Laidlaw, Power and Schmidt2007). The AAQ, which consists of a three-factor model (psychological growth, psychosocial loss and physical change), has been widely used to capture the cross-cultural perception of the process of ageing. The short version of the AAQ in CLASS consists of only two dimensions: psychosocial loss and psychosocial growth (Chen et al., Reference Chen, Guo and Perez2021). Psychosocial loss was measured with four items: ‘I think I am getting old’, ‘In my opinion, getting old is a process of losing’, ‘I found it harder to make new friends after getting old’ and ‘Because of my age, I feel that I am being excluded’. These reflect negative attitudes towards ageing. Psychosocial growth was assessed with three items, including ‘The older the person is, the stronger the ability to cope with life’, ‘Wisdom grows with age’ and ‘There are many pleasant things about getting old’. These reflect positive attitudes towards ageing. A five-point Likert scale was used to score these items, and a summary score was created by converting the reverse values, with higher score indicating more positive attitudes towards ageing. Cronbach's alpha for the scale was 0.66. Cronbach's alpha of two sub-scales of psychosocial loss and psychosocial growth were 0.69 and 0.60, respectively. Both dimensions were assessed from 2014 data only.
Confounders
We controlled for demographic-economic variables, including gender, age, residence (urban or rural residents), educational attainment (schooling or no schooling), marital status (married or others (divorced, widowed, single)), total amount of earnings in the last 12 months (logarithm form), health status (chronic disease and activities of daily living (ADL)),Footnote 1 number of children and living arrangement (lived with children or did not live with children). These confounders are commonly used in studies on the relationship between social participation and attitudes towards ageing and depression (i.e. Tomioka et al., Reference Tomioka, Kurumatani and Hosoi2017; Liu et al., Reference Liu, Xi, Hall, Fu, Zhang, Guo and Feng2020). All of these confounders were measured in 2014.
Method
Ordinary least squares (OLS) regression was used to analyse the relationship between social participation, attitudes towards ageing and depression. Adjusting for potential confounders, Model 1 analysed the association between social participation and depression; Model 2 analysed the association between the attitudes towards ageing and depression; and Model 3 further analysed the association between social participation, attitudes towards ageing and depression. Models 4 and 5 explored the interaction between social participation and psychosocial loss on depression and the interaction between social participation and psychosocial growth on depression, respectively. For the 2016 follow-up sample, we applied the same scoring and analysis to examine the associations between baseline social participation, attitudes towards ageing and depression (presence of depressive symptoms in 2014 was controlled in these models).
Results
Descriptive findings
Table 1 shows the characteristics of the sample. Among 6,908 older adults, the average age was 72 years old, and 66 per cent were urban dwellers. More than 50 per cent were male. Nearly 70 per cent of respondents were married and 20 per cent were illiterate. The mean personal annual income in the past 12 months was 20,736 yuan. More than 77 per cent of the respondents had at least one chronic disease, and the mean ADL score was 17.86. On average, they had three children, and more than 40 per cent lived with at least one of their children. Older adults who took part in social participation accounted for 22.44 per cent. The average scores for psychosocial loss and psychosocial growth were 11.17 and 8.32, respectively, with ranges from 4 to 20 and 3 to 15, respectively. The mean depression score was 13.51 with a range of 9–27.
OLS results for the associations between social participation, attitudes towards ageing and depression at baseline (2014)
Associations between social participation, attitudes towards ageing and depression are presented in Table 2, controlling for potential confounders. The regression estimates in Model 1 show that respondents who engaged in social participation reported a lower level of depression, compared with older adults who did not engage in social participation. Model 2 shows that both psychosocial loss and psychosocial growth are negatively associated with depression. When attitudes towards ageing and social participation are further controlled in Model 3, the results show that both attitudes towards ageing (‘psychosocial loss’ and ‘psychosocial growth’) and social participation are still significantly associated with depression. Results from Model 4 and Model 5 show no evidence that social participation moderated the relationship between attitudes towards ageing and depression. Because nearly 40 per cent of respondents were lost to follow-up in 2016 (which may cause bias in our estimates), we also re-ran Model 3 by restricting the sample to those being followed in 2016; the results for these 3,477 respondents remain significant and show similar patterns to those from the 6,908 respondents in 2014 (last column in Table 2).
Table 2. Ordinary least squares models for community participation, ageing attitudes and depressive symptoms in 2014
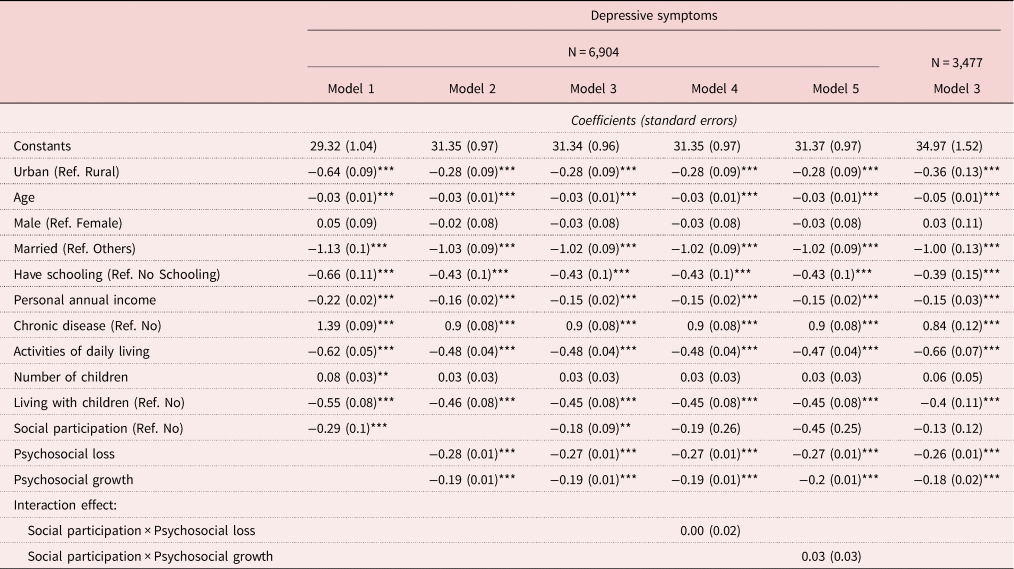
Note: Ref.: reference category.
Significance levels: ** p < 0.05, *** p < 0.01.
OLS results for associations between baseline social participation, and attitudes towards ageing and depression at the follow-up wave (2016) among those who were in two waves of CLASS
In order to avoid potential reverse causation between social participation, attitudes towards ageing and depression, we further used depression in 2016 as the dependent variable to examine the associations between baseline social participation, attitudes towards ageing and depression. Depression in 2014 was used as a confounder. Similarly to the models with 6,908 respondents in Table 2, the associations between baseline social participation, attitudes towards ageing and depression in the follow-up sample of 3,477 respondents (who were in both 2014 and 2016) remain significant and show similar patterns (Table 3). Respondents who engaged in baseline social participation reported a lower level of depression in 2016 compared with those who did not engage in social participation (Model 1). Both baseline psychosocial loss and psychosocial growth are negatively associated with depression in 2016 (Model 2). Model 3 includes baseline social participation, psychosocial loss and psychosocial growth; the results show that both attitudes towards ageing (‘psychosocial loss' and ‘psychosocial growth’) are negatively associated with depression, and respondents who engaged in social participation reported a lower level of depression, compared with those who did not. Again, there is no evidence that social participation moderated the relationship between attitudes towards ageing and depression (Models 4 and 5).
Table 3. Ordinary least squares models for baseline community participation, ageing attitudes and depressive symptoms in 2016
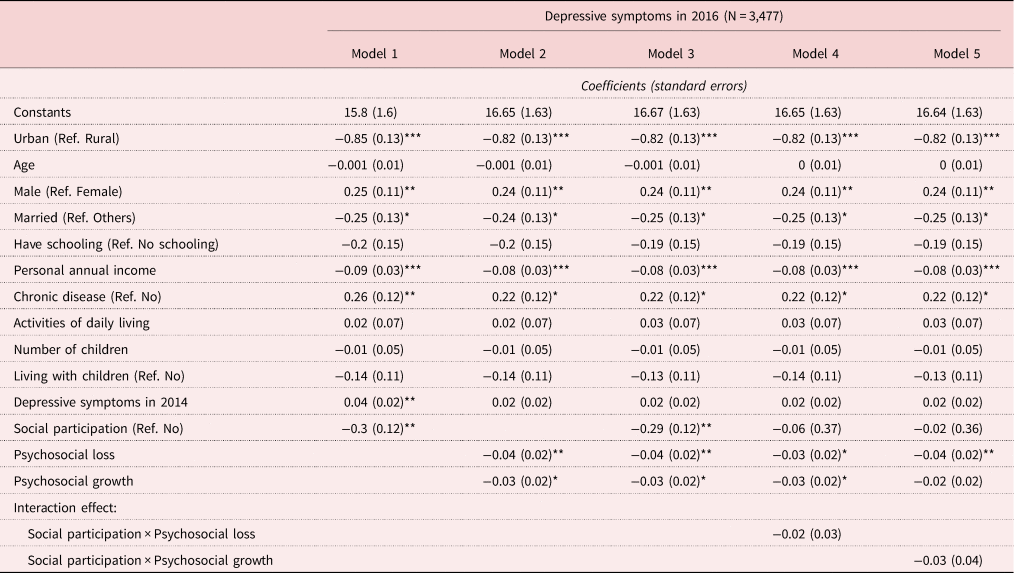
Note: Ref.: reference category.
Significance levels: * p < 0.10, ** p < 0.05, *** p < 0.01.
Discussion
Using two waves of data from a nationally representative sample, we examined the relationships between social participation, attitudes towards ageing and depression in China. Our findings show that older adults who engaged in baseline social participation reported lower depression scores in both 2014 and 2016 than those who did not engage in social participation, which contribute an important perspective on active ageing during China's social and demographic transition. In other words, social participation is beneficial for older adults’ mental health. In addition, upon including attitudes towards ageing into the statistical model, the direct influence of social participation on depression remains significant. The positive effect of social participation may be attributed to the Chinese culture of ‘a near neighbour is better than a distant relative’, which is deeply rooted in Chinese older adults. Social participation could improve the harmonious and friendly neighbourhood relationships in the community, which might have a positive impact on their mental health (Umberson and Montez, Reference Umberson and Montez2010). Social participation also strengthens the social network, which could contribute to the mental health of older adults. On the other hand, the function of family support has gradually been weakened in modern society, but for the Chinese older adults who are deeply influenced by traditional culture, home-based support is still the most suitable alternative. For those older adults who lack family support, the resources they obtain from community participation may compensate for the lack of family support and improve their mental health. Another possible explanation for the positive effect of social participation is that the social connections that are made via social participation may reduce negative emotions such as loneliness, and improve their psychological welfare (Musick and Wilson, Reference Musick and Wilson2003).
Our results also suggest that attitudes towards ageing, including both psychosocial loss and psychosocial growth, are associated with depression in older adults. According to the results of Levy (Reference Levy2009), who found that only when older adults assimilate from the surrounding culture do they form a self-definition that influences their health, personal attitudes towards ageing are shaped by the general attitudes of the surrounding population. The social environment is an important external factor that can influence the attitudes towards ageing of older adults. People's negative evaluation of old age will affect older adults’ communication, and hence their negative emotion (Hess, Reference Hess, Birren and Schaie2006). Therefore, it is also important to remove labels that discriminate against the aged and establish a cultural atmosphere that respects old people.
Active social participation can have a positive influence on people's attitudes towards ageing and prevent depression. However, analysis of the interactions between social participation and attitudes towards ageing provided no evidence that social participation moderate the relationship between attitudes towards ageing and depression. A possible explanation is that the attitude towards ageing is stable throughout one's life (Sun & Ji, Reference Sun and Ji2016); the time interval of CLASS was only two years, which may be not be long enough for social participation to accelerate or decelerate the effect of attitudes towards ageing on depression.
There are a few limitations in this study. First, although we used the two waves of CLASS to avoid the reverse causation for this study, we can only use the baseline attitudes towards ageing because CLASS did not collect information on attitudes towards ageing in the second wave (2016). We are therefore not able to estimate how changes in attitude towards ageing might affect depression. Second, a large fraction of respondents could not be followed up, which may cause bias in our estimates. However, in comparing the results among those who were interviewed in 2014 (6,908 respondents) and who were interviewed in both 2014 and 2016 (3,477 respondents), the results were similar. Therefore, we believe that our results are robust. Third, social participation in our study mainly focused on volunteer work. Other social participations such as daily leisure activities that could influence depression among older adults could be examined in future research. CLASS does not have such information. Even with these limitations, however, CLASS has information on attitudes towards ageing that other sources of Chinese data like the China Health and Retirement Longitudinal Study (CHARLS) or the Chinese Longitudinal Healthy Longevity Survey (CLHLS) do not have.
Our study provides a useful target for intervention to be incorporated into health promotion activities. Encouraging social participation among older adults has an important inhibitory effect on their potential to suffer from depression. In addition, this study extends the knowledge gained from previous studies by examining the unique contribution of attitude towards ageing. It has been pointed out that many factors contribute to successful ageing, including physical health (Depp and Jeste, Reference Depp and Jeste2006; Britton et al., Reference Britton, Shipley, Singhmanoux and Marmot2010) and genetic predisposition (Lee et al., Reference Lee, Min, Gallagher and Kirkwood2005). Some of these factors may not be easily modifiable, while others, most notably psychological and attitudinal factors, may be more amenable to intervention. Therefore, encouraging older adults to correctly understand the process of ageing and their own value is important for their mental health. Since psychosocial growth is related to older adults’ depression, making use of the influence of social environment on psychosocial growth, changing the stereotyped concept of society for older adults and encouraging them to participate in social activities should also have positive effects on the health of older adults and development of an inclusive society.
Acknowledgements
Data analysed in this study were collected by the research project ‘China Longitudinal Aging Social Survey (CLASS)’, sponsored by Renmin University of China. The CLASS research project was conducted by Institute of Gerontology and National Survey Research Center of Renmin University. The authors acknowledge the assistance in providing the data from the institutes and individuals aforementioned. The views expressed in this paper are the authors’ own. We would like to acknowledge of Marcus W. Feldman of Stanford University for his suggestions and editing of this article.
Financial support
This work was supported by a Major Project of the National Social Science Foundation of China (21ZDA103).
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
This study is exempt from ethics approval as it is an analysis of secondary data.



