



Introduction
According to the World Health Organization (WHO, 2020), Alzheimer's disease and related dementias (ADRD)Footnote 1 currently affect around 52 million people globally with nearly 10 million new cases every year. This number is expected to increase to 75 million by 2030 and to 132 million by 2050 (WHO, 2017). With increasing longevity, ADRD is becoming a global epidemic that should not be overlooked (Alzheimer's Disease International, 2013; WHO, 2015). The Middle East and North Africa (MENA) region is no exception: estimates of 2.3 million incidences are expected to rise to 4.4 million by 2030 (World Innovation Summit for Health, 2016). Not only will this pose a heavy burden on health-care systems but will also require informal support systems to alleviate most of the burden. Informal support refers to unpaid, ongoing care provided by family, relatives, friends or neighbours as opposed to formal (paid) support services provided by trained professionals (Bond, Reference Bond1992; Frederik, Reference Frederik2017). The focus of this paper specifically pertains to family care-givers who deliver primary and long-term care within the private home realm and whose voices are less heard in the ADRD literature emerging from the MENA region. This role begins when ageing family members require intensive assistance with the onset of debilitating chronic conditions or diseases (including ADRD). Studies have indicated the lack of preparedness of family members for the challenges specific to ADRD care-giving, an experience described as ‘unplanned and unexpected’ (Aneshensel, Reference Aneshensel, Pearlin, Mullan, Zarit and Witlatch1995).Footnote 2 Within Arab communities, while this role is regarded as an extension of familial duty towards older family members (El-Islam, Reference El-Islam2008; Hamdan, Reference Hamdan2009), it does not make them any more prepared for it. As a result, family care-givers’ experiences within the context of Arab-Muslim sociocultural norms tend to be an implicit expectation which partially explains why it remains insufficiently researched.
In this paper, we present the key findings of a qualitative studyFootnote 3 conducted in Qatar,Footnote 4 a country that has striven to improve its dementia care policies and support infrastructure over the last decade. Taking a much-needed shift from the prevailing biomedicalisation of ADRD studies (Lyman, Reference Lyman1989), it contributes an underresearched perspective on dementia care as it seeks to explore how sociocultural influences affect family care-givers’ choices and attitudes towards their older loved ones living with ADRD. It aims to shed light on some of the ways that sociocultural and religious beliefs and practices tend to be appropriated as ‘influencers’ on care practices, with the view that understanding family care-givers’ experiences, and close attention to the inevitable intersectionality with the sociocultural and religious beliefs and practices, could lead to more effective and culturally appropriate interventions for persons affected by ADRD. Furthermore, sociocultural insights emerging from care-giving practices and attitudes inform Qatar's health and social care provision sectorFootnote 5 as well as other communities that share similar cultural and religious belief systems in the region and beyond.
The care-giving experience
Studies have shown that most care-giving occurs in the informal sector, highlighting the significant role of families in long-term care-giving for older persons (see Bond, Reference Bond1992; Walker et al., Reference Walker, Pratt and Eddy1995; Aranda and Knight, Reference Aranda and Knight1997; Gaugler and Teaster, Reference Gaugler and Teaster2006). In the Arab region, informal care for older persons mostly occurs in the home and is performed by family members, privately hired nurses or domestic staff (Hamdan, Reference Hamdan2009; Abdelmoneium and Alharahsheh, Reference Abdelmoneium and Alharahsheh2016; Abdelmoneium et al., Reference Abdelmoneium, Rankin and Corman2017). Family members assist with activities of daily living, management of care-giving in response to their loved one's needs, administering medication and health-care professionals’ advice, overseeing nutrition and feeding support, accompaniment to medical appointments, attention to their loved ones’ overall wellbeing, and supporting with other comorbidities (e.g. diabetes, high blood pressure). As much of the literature in Arab Islamic as well as other contexts has shown, some cultural beliefs attach stigma to mental and cognitive illness which, in turn, affects societal attitudes and help-seeking practices (Al-Subaie and Alhamad, Reference Al-Subaie and Alhamad2000; Gearing et al., Reference Gearing, MacKenzie, Ibrahim, Brewer, Batayneh and Schwalbe2015; Kevahyan et al., Reference Kevahyan, Hammad, Alharahsheh, Haque, Gilstrap and Ghuloom2020). A closer look at the ways that the sociocultural context of dementia care-giving influences attitudes and practices is needed in the MENA region, as compared to biomedical and prevalence lenses applied to dementia research (Lyman, Reference Lyman1989; Harding and Palfrey, Reference Harding and Palfrey1997; Down, Reference Down2000; Hammad et al., Reference Hammad, Kane, Daher-Nashif and Al-Wattary2019; Kane et al., Reference Kane, Hammad, Islam, Clark, Al-Wattary and Daher-Nashif2021).
A growing body of literature has argued that culture and ethnicity can play a significant role in care-giving practices (Aranda and Knight, Reference Aranda and Knight1997; English et al., Reference English, de Voursney, Enomoto, Talley, Fricchione and Druss2014). Since dementia care-giving in the Arab-Muslim region involves the formal and informal, the institutional and sociocultural systems, we adopt the socio-ecological model of Bronfenbrenner (Reference Bronfenbrenner2004) as the main framework of this study. Despite the original focus of Bronfenbrenner's socio-ecological model on child and human development, many researchers have found his model an appropriate framework for scrutinising people's behaviours in relation to their physical and social situations in a variety of health-care settings and care-giving practices, including dementia care. For example, Moniz-Cook and Vernooij-Dassen (Reference Moniz-Cook and Vernooij-Dassen2006) claim that the ecological model allows a shift from the tendency to frame the tasks of dementia care in terms of a medical management model, to care-giving that is concerned with the wellbeing and overall quality of life of the older persons with ADRD and their families. It considers the immediate and wider influences on care-giving practices of family care-givers with attention to the intersections between Bronfenbrenner's model of five systems: the Microsystem (the direct context of the individual home and family); the Mesosystem (the close community and neighbourhood); the Exosystem (the larger social system such as school, workplace, policies and mass media); the Macrosystem (larger cultural context, such as attitudes, social ideologies and religion); and the Chronosystem (elements of time such as the physiological changes that occur with the ageing). Similar studies explored individuals’ interactions through these layers or systems to understand better formal and informal care support services and the associated challenges (Bowlby and McKie, Reference Bowlby and McKie2019), socio-structural influences on context-based experiences in what Bosco et al. (Reference Bosco, Schneider, Coleston-Shields and Orrell2019) referred to as the ‘caring ecology’, and how care-givers’ resilience can be facilitated or hindered through a consideration of the individual, community and societal resources accessible to them (Windle and Bennett, Reference Windle, Bennett and Ungar2011).
In the context of Arab societies, a closer examination of care-giving practices through the Bronfenbrenner model can be hugely enriching, given the central role of the family as main conduit of protection, companionship and socialisation for individuals (Abdul-Haq, Reference Abdul-Haq, Nasir and Abdul-Haq2008). The family functions in most Arab societies as the primary support mechanism to older individuals requiring consistent care, a commitment rooted in traditional collective values and expectations towards kin (Abdul-Haq, Reference Abdul-Haq, Nasir and Abdul-Haq2008). Despite shifts over the past decade towards nuclear family household structures, the extended family in Qatar continues to play a powerful role as a ‘community safety network’ that maintains family cohesion and offers support at many levels (Al-Ghanim, Reference Al-Ghanim2012: 329). Intergenerational families tend to live together communally or in close proximity and individuals are expected to actively engage with and support each other, especially ageing family members. The inherent hierarchical structure of authority and kinship relations within this traditional extended family structure influences how decision-making is made about important issues such as decisions surrounding care of older family members, typically made by the eldest male kin member. Thus, resorting to professional care or opting to institutionalise a family member with dementia is often regarded as a dereliction of one's familial duty and subject to censure by the broader community in the form of stigma and shame (Liu et al., Reference Liu, Hinton and Tran2008; Hanssen and Tran, Reference Hanssen and Tran2019). Furthermore, in line with literature on the predominantly gendered nature of care-giving among collectivist cultures (Fast et al., Reference Fast, Eales and Keating2001; Chadiha et al., Reference Chadiha, Adams, Biegel, Auslander and Gutierrez2004; Stewart et al., Reference Stewart, Neufeld, Harrison, Spitzer, Hughes and Makwarimba2006), socially constructed and locally accepted assumptions (also by women) that care-giving is a woman's natural role (Hooyman, Reference Hooyman, Biegel and Blum1990; Al-Ghanim, Reference Al-Ghanim2017), a prevailing expectation that children will care for their older parents (Liu et al., Reference Liu, Hinton and Tran2008; Schwartz et al., Reference Schwartz, Weisskirch, Hurley, Zamboanga, Park, Kim, Umaña-Taylor, Castillo, Brown and Greene2010; Hanssen and Tran, Reference Hanssen and Tran2019), also tend to influence who does the care-giving for older persons with ADRD. Ultimately, societal expectations surrounding care impact care-givers’ attitudes towards their role, as will be explored further through the course of the present paper.
Dementia care-giving has been described by some as a difficult hidden ‘career’ that impacts on the physical and psychological health of individual family members (Aneshensel et al., Reference Aneshensel, Pearlin, Mullan, Zarit and Witlatch1995; Etters et al., Reference Etters, Goodall and Harrison2008). Additionally, the literature notes that many care-givers will have both positive and negative experiences of care-giving, with positive aspects often acting as a buffer against the stressful aspects of the care-giving role (Langner, Reference Langner1995; Roth et al., Reference Roth, Fredman and Haley2015). The negative aspects of care-giving can be identified within the concept of burden of care. Although the notion of burden has been critiqued due to the voice of blame it carries towards the cared-for or patient (McPherson et al., Reference McPherson, Wilson and Murray2007; Cahill et al., Reference Cahill, Lewis, Barg and Bogner2009), we use the term burden of care for two reasons. The first is that burden is the word that the care-givers give when they describe the impact of care-giving on different aspects of their lives. The second is that care-giver burden is used frequently within the health-care literature. Despite this frequent use, there is still no clear definition of the concept (Liu et al., Reference Liu, Heffernan and Tan2020). In this paper, we adopt the definition of Liu et al. (Reference Liu, Heffernan and Tan2020: 442) of care-giver burden as ‘the level of multifaceted strain perceived by the caregiver from caring for a family member and/or loved one over time’ due to its consistency with how care-givers in our study experienced and articulated the care-giving journey. With most studies on burden of care and positive rewards generated in the WestFootnote 6 and few within the Qatari context (Al Sulaiti et al., Reference Al Sulaiti, Abdelnour and Ramadan2008; Abdelmoneium et al., Reference Abdelmoneium, Rankin and Corman2017; Hammad et al., Reference Hammad, Kane, Daher-Nashif and Al-Wattary2019), it is evident that more attention and research is called for considering the region's growing ageing population, the associated risks for higher incidences of ADRD among this population group and a predominant reliance on family care-givers.
In this context and using Qatar as a case study, we explore the range of sociocultural influences specific to this context and their role in shaping family care-givers’ choices and attitudes towards older persons living with ADRD. Sociocultural beliefs and practices in this paper refer to the social conditions and cultural beliefs, of which religious beliefs are part of the Qatari Arab context. These are examined in regard to the provision of care-giving within the family, the willingness to give care or seek help, and responses to feelings of care-giver burden or reward, as well as locally defined perceptions of ADRD (Dilworth-Anderson, Reference Dilworth-Anderson2001; Soskolne and Halevy-Levin, Reference Soskolne and Halevy-Levin2007). This paper considers how such influences are appropriated as coping mechanisms and motivators for care, with the aim of contributing insights that may strengthen existing interventionsFootnote 7 for care-giving families and those living with ADRD and support them more effectively along their care-giving journeys.
Methodology
This paper presents the findings of a larger multi-stage studyFootnote 8 that explored the experiences of family care-givers for persons living with ADRD in Qatar in the home sphere.Footnote 9 It addresses the questions outlined in the introduction of this paper, seeking care-givers’ experiences and voices through a qualitative exploratory design that was deemed most suited to accessing meanings and attitudes underpinning the care-giving experience for older persons with ADRD. Since this study is the first of its kind in Qatar, we used a grounded theory approach for a better and deeper understanding of care-givers’ experiences (Strauss and Corbin, Reference Strauss and Corbin1998). Furthermore, a qualitative research approach is recommended in sensitive health-care research to which stigma may be attached and has been used extensively to study lived experiences of family care-givers in the field of ADRD care (Dempsey et al., Reference Dempsey, Dowling, Larkin and Murphy2016).
Participants
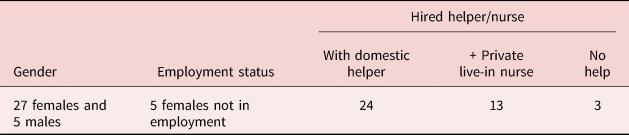
The research participants targeted in this study were family care-givers who identified themselves as the primary care-givers of the older person with ADRD. A total of 32 family care-givers were interviewed. This included 12 daughters, three granddaughters, nine daughters-in-law, one sister, two wives and five sons.Footnote 10 To reflect the composition of society in Qatar and geographic spread, 15 families were Qatari nationals, 15 were non-Qatari Arabs residing in Qatar (mostly Palestinians, one Algerian, a Syrian and a Jordanian) and two non-Arab residents (Indian and British nationals). All family members interviewed defined themselves as primary care-givers, regardless of employment status or the support of domestic help or other family members. Of those families, all Qatari nationals had at least a domestic helper and often one dedicated private nurse assisting in the care, and all but three of the non-Qatari Arab care-givers had a live-in helper who contributed with some care-giving roles (see Table 1). All but one participant in this study – a Christian British spouse of a person living with ADRD – followed the Muslim faith. Within this sample, older persons being cared for had been formally diagnosed with ADRD at the time of the research by the Homecare Department of the Centre for Empowerment and Care of the Elderly (also known as the Ehsan Centre), a local civil society organisation dedicated to older population groups, or self-reported as living with ADRD by family care-givers at the outset of the interview.
Table 1. Primary care-givers’ profiles
Participants’ recruitment
Due to the sensitivity attached to the research topic, participants were initially recruited through word of mouth or referral among students and staff at the university, after which principles of snowball sampling were applied: those interviewed were asked to nominate or refer us to other care-givers within their family or social circles who might agree to contribute to the study. Additionally, leaflets distributed at awareness-raising events on dementia at the university and other venues attracted some participation – albeit few due to the sensitivity of the topic. This necessitated reaching out to care-giving families registered with homecare outreach teams of the Ehsan Centre.
Ethical issues
The present study was approved in 2017 by the Qatar University Institutional Review Board and ethical standards were followed throughout the study. Following standard ethical conduct, prior written and verbal consent to participate in the study was obtained by the organisation from families as well as the researchers. Consent to audio record was requested prior to the interview, and participants were informed that they could request to stop the recording at any time or withdraw from the interview if any discomfort was felt. All interviews were anonymised using pseudonyms and file names were encrypted to ensure confidentiality.
Data collection
Qualitative semi-structured interviews lasting 45–60 minutes were used to obtain rich descriptions of the participants’ experiences as care-givers to an older family member with ADRD. They were conducted in Arabic by research team members inside care-givers’ homes; a handful of care-givers requested to be interviewed elsewhere. The interview guide covered the following main lines of inquiry (or broad questions) that were formulated with attention to the exploratory nature of this qualitative study and the related literature: awareness of care-givers about ADRD; awareness and access to existing health-care pathways for older persons with ADRD; care-givers’ experiences from noticing the first signs through first response, diagnosis and care management; and motives and challenges through the care-giving journey. These relatively open-ended questions were designed to give care-givers the opportunity to voice their experiences throughout the care-giving journey and express concerns from the home perspective. Each broad question was followed up by the researcher with further prompts to obtain deeper insight into interpretations and meaning-making processes, and ensure a fuller understanding of the phenomena or experience (Rubin and Rubin, Reference Rubin and Rubin1995).
Accompanying the Ehsan Centre's team on their home visits provided the research team with unprecedented opportunities to observe not only care-giver relationships with persons living with ADRD within the private sphere, but also how families adapted their home space to assure their safety and wellbeing. Researchers wrote field notes immediately after each interview, summarising key themes, recording impressions, observations and questions, and researcher reflections, which were later discussed among the research team and integrated into the analysis process.
Data analysis
After obtaining informed consent, interviews were audiotaped and transcribed verbatim into the language of the interview (Arabic). This was to capture meanings and experiences expressed through participants’ accounts in their natural modes of expression and in the context of their own sociocultural terminologies. A manual iterative qualitative thematic analysis process was followed, going back and forth in our analysis of the data to ‘identify, analyse, and report patterns (themes) within data’ (Braun and Clarke, Reference Braun and Clarke2006: 79) to the end of teasing out commonalities and differences in perceptions and experiences of research participants (Bradley et al., Reference Bradley, Curry and Devers2006). Drawing on Braun and Clarke's six-step process, we began by familiarising ourselves with the whole of the collected data followed by tandem coding by three research team members. This involved line-by-line review of two or three transcripts by each researcher and the generation of preliminary codes to describe the content and organise the data into meaningful patterns (or themes). These were then brought to the table and discussed collectively in relation to the study's research questions and clustered into agreed themes and sub-themes. The remainder of the transcripts were divided amongst the team members and the analysis continued accordingly. In the final stage of this rigorous process, a final review of the themes was conducted, ensuring that the voices of participants came to life telling a story through the themes and illuminating direct quotes. Observational data documented as field notes underwent this thematic analytic process, contributing to and enriching the combined qualitative findings presented along the themes identified.
Trustworthiness and authenticity measures
To strengthen the trustworthiness and authenticity of the data, methodological triangulation was performed through multiple methods and multiple perspectives (those of care-givers and professionalsFootnote 11) with tandem coding by four researchers to triangulate the analytic trail. Further, maintaining the data in its original language was to ensure the authenticity of the analysis and avoid losing meaning in the process of translation; selected direct quotes were extracted from original transcribed interviews and translated into English by the main author followed by a review of the translation by a second bilingual researcher to validate it and ensure no differences in interpretation of the narratives. Key words rooted in socioculturally rooted expressions were left intact (italicised) in their native Arabic language and discussed in the context of study findings.
Results: sociocultural and religious influences on the care-giver experience
Seven emergent themes were found to affect the care-giving journey according to participants’ accounts; they are underpinned by sociocultural and religious influences: (a) reasons and motivations for care-giving; (b) role of the extended family; (c) socio-demographic attributes of care-givers, their allocated responsibilities, and how these intersect; (d) socio-religious attitudes towards care-giving of older persons; (e) social stigma; (f) personal knowledge of ADRD; and (g) coping mechanisms.
Reasons and motivations for care-giving
Although care-giving for a person living with ADRD was described by families as demanding and time intensive, giving care to their older loved one (with ADRD) had positively impacted care-givers and their families. Almost half of the study sample expressed optimistic remarks about their care-giving experience with positive comments such as, ‘I see the cup as half full not half empty’, ‘Alhamdullilah [thanks be to God]’, ‘we enjoy being with him’ and ‘this is an opportunity to give back’. These expressions indicate a sense of gratitude for the presence of care-givers’ loved ones in their lives regardless of the disease. The mere presence of the older parent in the home of the care-giver was described as ‘a blessing’ (baraka) and ‘happiness itself’ by several families we interviewed. Because of that, for Um Hamdi, the care-giving job was even perceived to be ‘very easy’ and ‘not at all a burden’. As stated by one Qatari national:
[Taking care of my mother is] very, very, very, verrry [easy], let me tell you. I don't even feel I have a sick person in the house. I swear to God! I don't feel it at all! Some people say they have an invalid to take care of in their home, but [for] me not at all – she is not at all a burden. I mean, this is a blessing from God.
Moreover, the findings revealed why care-givers continued caring despite the challenges associated with ADRD. The primary motivation was the attachment between care-givers and the older person with ADRD, together with a deeply embedded sense of duty and responsibility. According to Kareem, a 46-year-old care-giving son, what kept him going was ‘simply love’. Mariam, a 30-year-old unmarried daughter, explained it was a commitment to ‘give back’ to her parents:
What I'm doing is – this is what is normal. It's a normal thing not to leave … [It] is very important for the wellbeing of the parent – psychologically – we can't leave them. It's wrong. They will feel neglected and abandoned.
Some interviewees were more motivated by a sense of duty towards one's elders, as explicitly stated in religious texts and teachings as silet rahem Footnote 12 and bir al walidein. Footnote 13 Muslims’ responsibility towards family and the significance of kinship ties is repeatedly emphasised in religious text. For instance, Safa, a non-Qatari care-giver who takes care of her mother with assistants, stated that:
Worship Allah and join none with Him (in worship); and do good to parents, kinsfolk, orphans… (Holy Qur'an, Surat An-Nisa 4:36)
The tie of kinship is suspended to the Throne and says: He who unites me Allah would unite him and he who severs me Allah would sever him. (Hadith, reported by Muslim 2555)
Being the single sibling was another reason to be the main care-giver. For example, Riham, a non-Qatari care-giver who takes care of his mother without employing an assistant, explained:
I am the closest to her, so the shock was bigger on me than the others I mean I shared a bed with her that's how attached I was to her. I am now the one who takes care of her most, together with my older sister.
Omar, a non-Qatari national and an only son to his mother, adds:
My mother and I were very close before she got sick. I am her only son. I do this simply out of love for her. Sick or not.
These perspectives are consistent with accounts of care-giving wives as well. Sharifa, for example, is a Qatari care-giving wife whose strong relationship with her husband was the key motivator for her dedicated care-giving. Care-givers expressed a realisation that care-giving for their loved one with ADRD had allowed them to focus on the bigger picture. For example, for Riham, being so close to this difficult disease was a reminder that one day it could be her, so she had decided to stop getting upset over mundane problems, e.g. work, relationships and others which now seemed ‘petty’ in the bigger scheme of things. To other care-givers, like Um Hamdi, the bigger picture was her view that everything was part of God's plan: in that context, her care-giving role was an ‘opportunity’ to receive a reward from God and blessings (baraka) for their household:
Um Hamdi: You see happiness between you and God, contentment between you and your God, and I say to Him, alhamdullilah [thank God] that you have given me this chance to serve and have birr for my mother at the end of her life.
Researcher: Given you a chance?
Um Hamdi: Yes it's an opportunity. I'm telling you, it's baraka [a blessing], I swear it's baraka.
Another motive driving care-givers was providing a role model for their children and grandchildren to ensure they learned the value of care-giving from their older family members. This is again linked with the religious duty of birr al walidein (duty towards parents) which is presented at more length in the section ‘Socio-religious attitudes towards care-giving for older persons’. Other care-givers had a more practical motive in mind, as Riham, a care-giver to her mother and mother of only boys, explains:
I want my boys to get used to this [supporting me in giving care to their grandmother]. I tell them maybe one of these days I will get old too, so you need to [learn] and get used to it.
Care-givers relied on several different mechanisms to cope with their care-giving roles.
Role of extended family
Perhaps one of the most important aspects of caring for persons affected by ADRD in the Arabian Gulf region is the cohabitation of intergenerational families. Families with numerous siblings, grandchildren and extended families cited the importance of these relationships (and their proximity) in the division of care-giving duties and providing respite to the primary care-giver. For instance, a Qatari care-giver emphasised that:
We used to go on family vacations a lot. Now we cannot travel, we cannot take a vacation all together because he will be very upset if we change anything in his environment. So we take turns staying with him.
Care-givers indicated the strong role of the family as a support system, more evident among families whose extended families lived either in the same household or were actively involved in the care-giving through regular visits. This applied primarily to Qatari families and a handful of Arab residents. Where extended families resided in different households, extended family members regularly came to visit and help, or to fill in if the older family member was not on their own. The role of grandchildren was particularly striking, as the quotes below by a Qatari national care-giver reveal:
I notice she likes to see her grandchildren. Sometimes she remembers them and even if she can't remember their names, she plays with them … I see this as a positive thing.
They all help but my middle son especially. For example, as soon as he comes home, he'll talk to her: ‘[Grandma], how are you? What did you do today? He'll try to give and take with her; whether they like it or not, one of them must always be with her.
Extended family members were also available in the event of a crisis to offer emotional and financial support, as Um Hamdi, a non-Qatari resident in Qatar explains:
Although my brother is far away, he helps by contributing financially to her care.
A care-giving daughter, Haneen, who spends half the year in Qatar and the other half with her immediate family abroad explains that when she cannot be physically there, she supports her sisters emotionally through an active WhatsApp group and daily calls. Ayman, a middle-aged non-Qatari care-giving son, has experienced more closeness with his siblings:
We get together every day. My older sister cooks my father's favourite dishes – he hasn't lost his love for good food (laughs). Not one day passes that all the brothers and sisters don't come see him and kiss his hand.
A number of accounts of care-givers with no extended family support report the disruptive impact on their parenting, social lives and careers, which points to the crucial role of extended family in care-giving for persons with ADRD. This was mostly the experience of expatriate residents living and working in Qatar who were caring for an older parent. Emma, a non-Qatari care-giving wife, explains:
I wasn't able to go out, I couldn't even go to the supermarket. [My daughter] resents her father because I miss her birthdays, I miss her graduation, I miss her first day at university. I can't do it all alone.
Another care-giving daughter, Maram, perceived that her two siblings’ lack of support to her two parents with ADRD had led to her not marrying, having children or even holding down a job.
Socio-demographic attributes of care-givers, allocated responsibilities and how these intersect
Other individual characteristics found to influence care-giving responsibilities were the position of the care-giver in the family (eldest, youngest, etc.), her marital status (single, married, divorced) and the age of her children. Unmarried female family members were the most likely to assume the responsibility of primary care-giving for persons with ADRD and to live with them. Most (94%) familial care-givers in this study were females: daughters, wives, daughters-in-law and nieces. Our findings indicated that the greater duty of care fell on care-giving daughters who were also mothers with multiple caring roles, unless delegated to the youngest unmarried female family member.
In this study sample, female family care-givers were the primary hands-on care-givers taking on most of the practical care and emotional support, and full-time accompaniment for the older person with ADRD. None of the females in our sample were in employment: they had either taken extended leave or resigned (to dedicate themselves to care-giving), or never worked. The majority of our sample had dedicated helpers and nursesFootnote 14 hired to support them in the special care entailed by ADRD; they tended to be financially secure as observed in living surroundings and confirmed by their narratives. According to them, having a live-in nurse saved trips to hospitals for mild medical care and minimised the irritability that older persons with ADRD experienced with long car trips and long waits. It is worth pointing out that despite the helper support in these families, the role of family care-giver cannot be described as mere management of care; on the contrary, they remained hands-on, always close, and attended to the personal and emotional needs of their parent, spouse or in-law. Care-givers described the support they received from helpers and other family members living in the same household as ‘assistance’ in tasks simply ‘too much for one person’. This included assistance in keeping her or his space clean and tidy, helping the daughter/son/wife with personal hygiene and clothing, assisting them use the toilet, bath, or move into a bed, sofa or wheelchair, and in a few cases giving the correct daily medication if the primary care-giver was out. Full reliance on the domestic helper or nurse was more prevalent among male care-givers (sons, spouses), or if the older person with ADRD was male, i.e. too heavy to handle physically by one person. In those cases, the primary nature of care shifted towards the nurse or helper and the family care-giver – usually working outside the house – could be described as a ‘care manager’ (Rosenthal et al., Reference Rosenthal, Martin-Mathews and Keefe2007). There were only two families who did not have the support of a domestic helper or nurse due to financial constraints (job insecurity and low income) or residency status (Syrian migrant family whose status was still under processing).
Socio-religious attitudes towards care-giving for older persons
The data revealed that a deep and widespread respect of the older person influenced care-giving practices, and this was extended to how family care-givers viewed their role and duty of care in the context of ADRD. Enactment of this respect for the person with ADRD was manifested in different ways. For example, the care-giving role appeared to be automatically taken on without question or complaint. Participants explained that this was because it was drilled as a social expectation, on the one hand, but also perceived and internalised as an unquestioned duty-of-care towards one's ageing parents, on the other. Amira recounts the popular saying that ‘whoever doesn't do good for his mother will not do good for others’, emphasising that caring for one's parent was ‘the normal thing to do in our culture’. Care-givers spoke repeatedly of the special status of parents to younger family members according to religious beliefs and socialisation from a young age. Parental care was seen as a ‘pathway to heaven’ and instilled in the teachings to every son and daughter from a young age (birr al walidein). Birr al walidein entailed kindness, respect, reverence, as well as the specific responsibility of care-giving. Care-giving for a person with ADRD was also viewed as an extension of one's faith; the Muslim's belief system urges children to repay their parents through birr al walidein in their old age. Um Hamdi refers to the relevant verses from the Qur'an and explains:
Every home and family with a sick older person showing signs of dementia or loss of awareness must internalise this and remember the reward [from God] and respect and remember not to tell them [say] ‘ooff’ – it is a sign of disrespect!
Other forms of birr depended on the circumstances of the offspring. For instance, a son who lived abroad made a monthly financial contribution to the care of his mother. There were many references to ADRD as ‘a test from God’. Faith was seen as a source of strength that helped calm many family care-givers, making them more resilient. There was fear among some care-givers that failing to care for the older person in accordance with Islamic duties could result in punishment from God.
Social stigma
Perceptions of ADRD profoundly affected how families coped with and spoke about their loved ones’ disease. Social stigma was articulated most strongly by Qatari nationals with established social networks, and whose family name and reputation were at stake, as the following quotes by two Qatari care-giving granddaughters show:
Society is still not ready. Why? Because they [people] are afraid, they're afraid of a bad reputation … Our society has a problem – a problem in that it's not OK to be sick – but being sick should be normal.
Many care-givers expressed similar experiences, emphasising that more stigma is attached to psychological illness than physical illness; for instance, the following quote by a non-Qatari participant emphasised that:
The rest of illnesses [like cancer] people talk about [them], but no one talks about psychological illnesses, even if the person himself or herself has it, he or she won't say I have a problem, but will keep quiet. I don't understand why. I tell people she is sick, but I don't say psychologically … in the end, it's something personal. The family knows, close people who love him or her know, but to people outside [the family and close friends], I just say my mum is not well – in our society, it's weird to say we need to see a psychologist.
In many cases, the shame expressed by care-givers was more about the associated behaviour (with ADRD) such as shouting, inappropriate talk and aggression. For example, one interviewee said, ‘what will the neighbours say’ in reference to constant shouting of their family member with ADRD. These accounts suggest that most care-givers preferred to keep diseases such as ADRD behind closed doors and were ‘ashamed’ by it.
Stigma also prevented most families from seeking help until they had reached advanced stages. This was explained as a way of avoiding jeopardising their family members’ dignity and their conviction that it was ultimately ‘in his or her best interests’. One Qatari care-giving daughter stated:
We are a conservative society. Arabs don't like to share private details – maybe they see it as I don't know, maybe they see it as naqs (a limitation) – a loss of the dignity of this family. The problem is, for some people, traditions and norms say its aib (taboo),Footnote 15 for example, to let out secrets from the house; others don't want to say anything so as not to embarrass themselves.
Another Qatari granddaughter similarly said:
My grandmother is in good health … even if she has minor memory issues. I will not take her to doctors or health clinics. She will stay here in my house and I will never allow anyone to interfere.
Care-givers’ accounts show how the stigma associated with ADRD influenced how families caring for a person with ADRD engage (or do not engage) with surrounding social spaces, neighbours and friends. This kind of ‘shame’ is known in the Arab world as the culture of aib and has been well-cited in relation to the stigma and social shame attached to mental illness (Ciftci et al., Reference Ciftci, Jones and Corrigan2013). Heibeh,Footnote 16 another element that families need to safeguard for their older parent, is the social prestige gained along his or her life: the family finds it hard to change his or her image in society. For example, it was perceived by many care-givers as socially unacceptable for them to be seen in public places; consequently, they tended to be kept within the confines of the house or surrounding garden. Indeed, most older loved ones with ADRD were found to be kept home due to the difficulties of taking them to public noisy spaces that could irritate them and expose them to putting their dignity at risk (the perceptions of aib and heibeh). Family care-givers also safeguarded their own social standing by evading possible societal stigma that could affect the wider family, as a care-giver explained: ‘they [society] think if one [member of the family] has dementia then they all have the same disease’. As a result, the quality of life for persons affected by ADRD is restricted and house-bound, while family members’ primary concern becomes keeping this affliction a secret to protect their loved ones and themselves.
Personal knowledge of ADRD
Care-giver accounts revealed misinformation about the nature of the disease, and a lack of understanding at which point medical care should be sought. This was attributed to misinformation about its symptoms, presentation and the causes of ADRD. Among the most recurring assumptions was that older family members were simply ageing, as Kat's aunt, a non-Qatari care-giver, kept insisting:
My aunt keeps saying, he's healthy, he's fine, but he's just old, so all this is normal. We just need to keep reminding him of things – my auntie was just refusing the Alzheimer word.
An insistence on not using the terms Alzheimer's, dementia and its Arabic equivalent kharaf Footnote 17 and such misconceptions lead to delays in diagnosis, refusal to get a diagnosis and high levels of frustration over unexplained behavioural changes. Most care-givers said that they relied on informal channels of information such as Google, YouTube, prior experience with a family member, hearsay or WhatsApp groups of family and friends who advise. Moreover, the findings revealed that most care-givers were unaware of services available to support persons affected by ADRD; some like Rowaida, a non-Qatari care-giver, wished that they had been aware of them earlier on in the disease:
I think if I get the same experience again, I will seek for health services, because if we have it, why we don't benefit from it? I will ask them to give more advice, maybe there is medication to help him.
Such accounts confirm an urgent need for the education and training of families and the general public on the nature, symptoms and progression of the disease to improve recognition and preparedness.
Coping mechanisms
The main coping mechanism cited by care-givers in our study was drawing upon their faith and spirituality; this manifested as reading the Qur'an, prayer, frequenting places of worship, repentance, acceptance that this was a test from God or an opportunity to practise birr al walidain. A non-Qatari care-giving daughter expresses this clearly:
Subhan Allah [praise be to God]. God must have a reason, and surely, I mean surely, I must be better off than others. You know, when you know that things could get worse you accept or live with the situation as it is, in a much better way.
Acceptance of their loved one's cognitive changes as part of the ageing cycle was another way of coping, as mentioned earlier. In some cases, acceptance was coupled with a denial that these changes were symptoms of dementia, as in Majed's case, a middle-aged Qatari son who refused to use any labels for his father's disease nor seek diagnosis and treatment. The word kharaf, in particular – the popular term for dementia – held a strong negative connotation and was fiercely rejected by him:
No no let's not call it kharaf … but it doesn't really matter, we don't like to diagnose anyway (nervous laugh) … He simply forgets things but then remembers them again. You know people reach a certain age … (chuckle) and we are on our way too … it is the circle of life. First it's the stage of youth then comes old age.
Others, like Rowaida's aunt, were convinced ‘there was nothing wrong with her sister’ and visits continued as usual while her behavioural changes were interpreted as ‘ageing’, a common reaction among several participants.
Discussion
Understanding the care-giving role in the context of family members living with ADRD requires a pluralistic and multilevel analysis. The complexities of care-giving can be elucidated using Bronfenbrenner's ecological systems framework. Conceptualised as such, care-givers are located simultaneously in tiered ecosystems, ranging from the intimacy of the family home to the broader health-care system, all of which are embedded in the larger sociocultural context at a specific temporal moment. Situated as such, each care-giver is enmeshed in and engages with a unique constellation of individual, immediate and external factors, all of which shape the outcome of his or her care-giving. According to Bronfenbrenner's model, the care-givers in this study share a similar Chronosystem, that is, caring for patients with ADRD at a time when the petrocarbon-rich nation has started to invest heavily in its domestic health-care system. Qatar has recognised its need to expand more comprehensive and ancillary care services to its growing geriatric population. The establishment of the Dementia Stakeholder Group, the Ministry of Public Health's development of the National Dementia Plan 2018–2022 (Ministry of Public Health, nd) and joining the Global Dementia Observatory are important milestones that have been achieved during the period of time that our care-givers were interviewed. The political will to support dementia care, coupled with national policy-level commitments towards healthy ageing and strong families geared to ensure the wellbeing of older persons, is generating an Exosystem that is intended to be more conducive to supporting dementia care-givers in Qatar. This unprecedented support and recognition of the role of dementia care-giving also speaks to the realisation that in the absence of a cure and the crucial role of the family alongside formal care pathways, family care-giving is an indisputable component of patient care and long-term management.
Similarly, the care-givers of this study are ensconced in a predominantly Arab Islamic community. This means that both Arab mores and Islamic values contour the care-giving journey. These sociocultural and religious influences impact on how family care-givers perceive ADRD, their care-giving role, and contribute to whether and how help is sought. They, together with policies, benefits and care pathways in place for nationals and residents of Qatar, constitute both enablers and inhibitors. Access to accurate information about ADRD, existing support services and policies affect the decision and mode of help seeking among family care-givers. Similarly, certain sociocultural attitudes towards cognitive illness and religious beliefs towards older family members and care-giving duties distinctly shaped how they cared for and coped with ADRD within the family. These are illuminated through the Bronfenbrenner ecological model (Figure 1) which illustrates how the different layers or systems indeed intersect and, to a large extent, directly influence care-giving experiences at the individual and family level (the Microsystem).
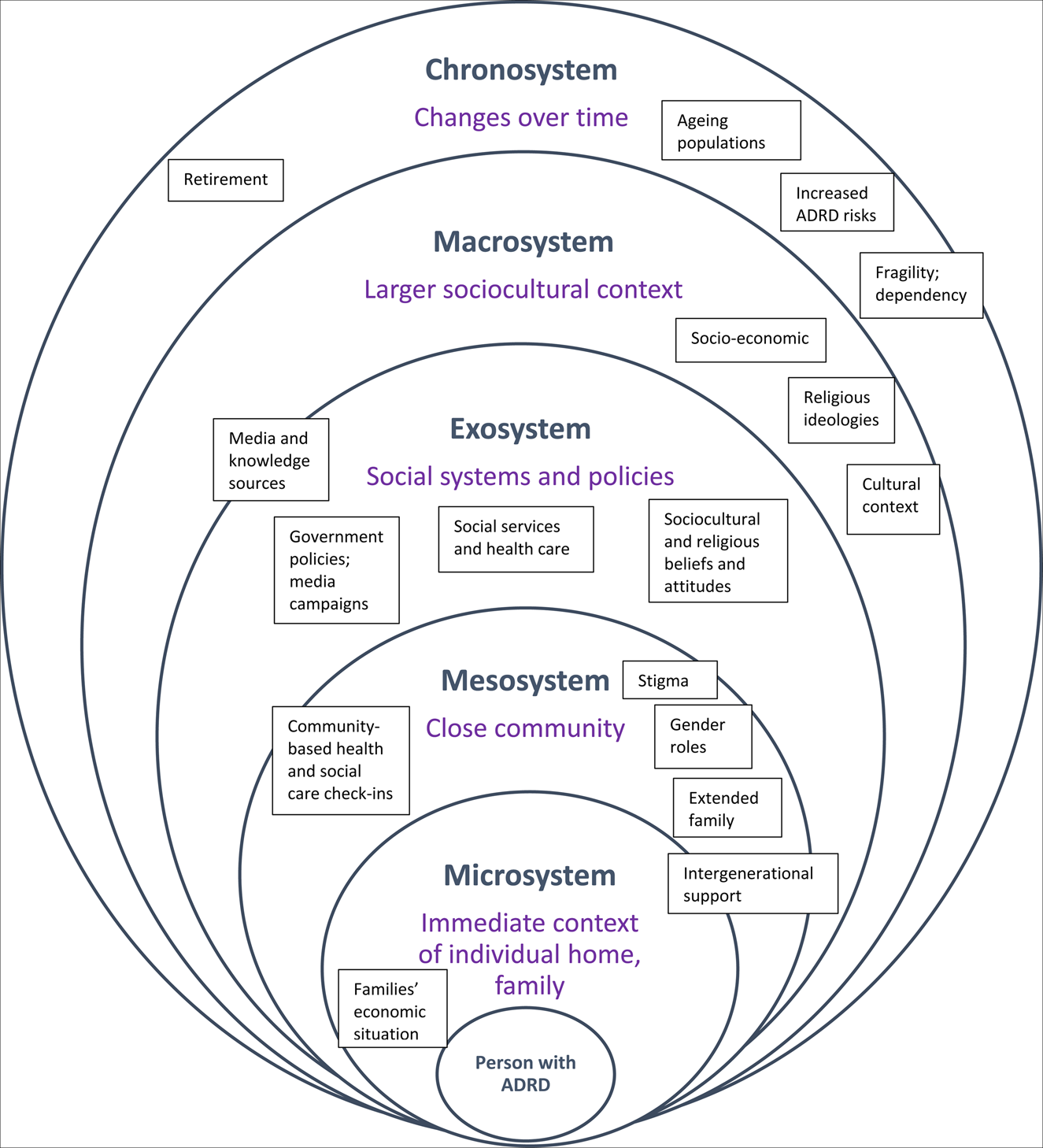
Figure 1. Findings viewed through Bronfenbrenner's ecological model.
Note: ADRD: Alzheimer's disease and related dementias.
At the Macrosystem level, two central pervasive societal beliefs stood out: religious belief systems which translate into widespread convictions and practices, and a powerful subtext of cultural expectations. These were found largely to shape peoples’ understandings of ADRD, older persons’ place in society and their expected roles towards them. The collectivist culture characterising the Arab/Islamic Exosystem in Qatar affected the support (of social systems and policies) into which care-givers could tap. The data have indicated the extent to which sociocultural and religious beliefs and attitudes were formative in the mindsets and attitudes of care-givers. Despite the presence of solid health and social services pathways of care, these attitudes impacted upon the choice and time to acknowledge ADRD and seek help. Knowledge sources – media, internet and, again, societal assumptions on what ADRD is and is not – also played a role alongside these two macro-level influencers. While this is slowly changing due to Qatar's bold steps in policy setting and awareness campaigns, the influence of the Macrosystem spills over into the Exo- and Mesosystems, highlighting questions of access, information and where the duty of care lies.
The presence of solid social solidarity in the care-giving journey for the loved one with ADRD was highlighted at the Mesosystem level through extended family structures and intergenerational support. This applied particularly to Qatari families with more-established family ties in the country and extended families living in relatively close proximity to each other or within the same household.
This was found to be central in the long-term care and emotional support to both persons living with ADRD as well as primary care-givers. Our findings reflected that, to many, the care-giving role was facilitated due to previously close family relationships, a point that begs the question of whether this role is taken on in the same way when families are not as close-knit prior to ADRD onset. Further, narratives repeatedly mentioned care-givers’ moral commitment and reverence towards their older parents, and it became apparent that expressions of duty-of-care as an obligation were derived and sustained through socio-religious teachings. The collectivist nature of the Arab-Muslim family has indeed been cited as a cornerstone for mental health support for persons with mental illness (El-Islam, Reference El-Islam2008; Hamdan, Reference Hamdan2009), as well as a strong influence on attitudes towards help-seeking (Youssef and Deane, Reference Youssef and Deane2006). This study's findings reinforce such research, extending the influence of Arab-Muslim norms and beliefs to care-giving practices as well. In the Qatari context, the extended family has been described as a ‘strength’ in the care of older persons (Abdelmonieum et al., Reference Abdelmoneium, Rankin and Corman2017; Defrain et al., Reference DeFrain, Asay, Badahdah, Abdelmoneium and Abdennadher2018), and the data confirmed the significance of this role with grandchildren's involvement, continuous visits of extended family and, in the majority of cases, sibling support in care-giving and respite. Family involvement in the care of a person with ADRD provides crucial emotional and financial support (Chaaya et al., Reference Chaaya, Phung, Atweh, El Asmar, Karam, Khoury and Gunhild2017), although the nature of this role differed for a few non-Qatari Arab population residents in Qatar with no extended family residing in the country. Their accounts indicated that the absence of extended family members led to a heavier load on their older children and their spouses, and thus had a greater impact on their daily lives and livelihoods. For example, those with limited financial resources could not afford domestic or nursing help at home, which in turn affected the quality of their loved one with ADRD as well as their own capacity to cope and self-care (a Syrian and Palestinian family in our sample); while others (like Maram and Um Hamdi) relied on financial remittances from a sibling abroad while they handled the physical care-giving role. Of interest is how this distance from extended families or siblings helped create an alternative form of family solidarity: a transnational support mechanism with family and friends abroad via WhatsApp family chat groups and regular calls for advice, problem solving and emotional support. Closer examination of the relationship between income levels, employment status and burden would be beneficial in future studies,Footnote 18 as would be a closer look at the subtle differences in experiences of care management and direct care-giving among males in particular.
Sociocultural and religious assumptions played a dual role. While they fuelled resilience and sense-making of the care-giving journey, they also appeared to intensify the stigma associated with ADRD in Qatari society. Our study reveals a strong preference for privacy in family affairs, particularly in relation to mental illness. The ‘social shame’ (referred to in Arabic as wasma or khajal ijtima'i) of the ADRD afflicting their older loved one was evident in families’ preference to conceal or deny the disease and even rename it. For example, care-givers preferred to use expressions such as ‘he [she] is forgetting’ or ‘he [she] has become old’. Some of the responses indicate an attempt to dissociate the stigma from the family in order to maintain their reputation and social standing. This tendency resonates with the notion of vicarious stigmas, emotions and practices noted when parents witness their child being the object of prejudice and discrimination due to their mental health and/or a neurodevelopmental disorder (Serchuk et al., Reference Serchuk, Corrigan, Reed and Ohan2021). Our study indicated that this behaviour tended to be rooted in a desire to protect their older loved one from experiencing stigma from society, but pointed to the perhaps unintended consequence of delaying help-seeking and minimising their social interaction, important for persons with ADRD. Namely the prerogative of maintaining the ‘dignity’ of the older person would often be the reason for concealing the disease and keeping them out of the public eye. This finding aligns with stigma research in other settings (Whitehouse et al., Reference Whitehouse, Ganes, Lindstrom and Graham2005; Leibing and Cohen, Reference Leibing and Cohen2006; Corrigan et al., Reference Corrigan, Morris, Michaels, Rafacz and Rusch2012). While global statistics indicate an increase in health-seeking behaviours and an uptake of services (Picco et al., Reference Picco, Abdin, Chong, Pang, Shafie, Chua, Vaingankar, Ong, Tay and Subramaniam2016), in many cultures, stigma will still deter people from seeking a diagnosis (Abdullah and Brown, Reference Abdullah and Brown2011). For instance, Liu et al. (Reference Liu, Hinton and Tran2008) pointed out Chinese families’ tendency to delay formal help-seeking for family members with cognitive issues because of the deeply discrediting impact of mental illness for the entire family. Further, Morgan et al. (Reference Morgan, Semchuk, Stewart and D'Arcy2002) revealed that family care-givers kept their relatives at home for as long as possible, despite the great physical and emotional cost. The reason was related to the social stigma issues and their attempt to ‘hold the image that community members have of their relative’ (Morgan et al., Reference Morgan, Semchuk, Stewart and D'Arcy2002: 1133). In small close-knit communities like Qatar, where personal information has the potential to spread quickly, this is particularly pertinent. Fears of disclosing a diagnosis laden with stigma are heightened and contribute to hindering treatment for older loved ones, as our study and others (Barbarino et al., Reference Barbarino, Lynch, Khamis, Rayaz, Malik, Hammad and Almeer2020; Kevahyan et al., Reference Kevahyan, Hammad, Alharahsheh, Haque, Gilstrap and Ghuloom2020) have confirmed. Our study confirms the need for desensitisation of the stigma-laden discourse surrounding mental illness including ADRD, especially as age-related illnesses in Qatar become more common (Hammad et al., Reference Hammad, Al-Harahsheh, Salihy, Haque, Gilstrap and Ghuloom2020). The implication of this finding is quite significant, as it highlights the issue of stigma as one that dementia care-giving providers must take into account in preventive and early diagnosis stages.
Further, an intergenerational dimension of care-giving and family solidarity towards the ill older person is apparent in our study. Fulfilling this role appeared to be an expectation that was enacted through intentional acts of role modelling in the presence of children and grandchildren. This finding supports research that recognises the role of intergenerational transmission as a means of cultural continuity (Nauck, Reference Nauck2001; Trommsdorff, Reference Trommsdorff and Schönpflug2008). The intergenerational continuity of care emphasises the powerful role of women in the transmission of values and practices within the family, particularly in regard to the socio-religious expected duties of care and respect towards older parents. Religious interpretations of care-giving were found to fuel resilience and sustained care-giving for older persons with ADRD within the family. Religious text and beliefs also strongly influenced health practices and attitudes towards mental illness. In the Arab Islamic context, deeply intertwined religious and cultural practices influence the perceptions and attitudes of those in the care-giving role: many believe illnesses are tests from God and an opportunity to purify the body (Rassool, Reference Rassool2015; Daher-Nashif et al., Reference Daher-Nashif, Hammad, Kane and Al-Wattary2021), which directly impacts family care-givers’ perceptions of their role and facilitated coping. For some, care-giving was an opportunity to fulfil a religious duty; for others, it was simply a blessing (baraka). The religious framework was drawn upon to ease the burden of care-giving and promised benefit in the present and the afterlife (Hammad et al., Reference Hammad, Kane, Daher-Nashif and Al-Wattary2019). This key finding is consistent with the wider literature pertaining to the positive effects of religion and spirituality on physical and mental health (Seybold and Hill, Reference Seybold and Hill2001; El-Islam, Reference El-Islam2008; Ciftci et al., Reference Ciftci, Jones and Corrigan2013). None of our respondents framed ADRD as divine punishment or an affliction caused by satanic powers (jinn), as earlier studies have shown (Al-Krenawi and Graham, Reference Al-Krenawi and Graham2000; Youssef and Deane, Reference Youssef and Deane2006). Only one care-giver mentioned the possibility of the ‘evil eye’ being the cause for her mother's cognitive decline. This could reflect a change in prevailing interpretations of sickness and health from an Islamic and cultural perspective, and is worthy of further research to investigate whether and how popular conceptions have changed over time.
At the Microsystem level – the immediate family context – discussed earlier, the quality and nature of family relationships contributed to shaping the care-giving role. The data at this level also indicated that individual characteristics of the care-giver influenced how the care was played out: whether single or married, in education, in employment or fully dedicated to care-giving, in the country or contributing from abroad, the role of siblings and their proximity to the house affecting levels of their engagement, and the means to hire one or more domestic helpers or nurses. It was evident that the individual profile of care-givers interplayed with the wider sociocultural context (within Bronfenbrenner's loops) that permeated the sphere of the family defining care-giver roles to a large extent. The gendered nature of primary care-giving was evident in our study: females were expected to assume the vast burden of care. This is a good example of the interplay between the individual and the patriarchal at Macrosystem level, which in turn influence the care-giving role. The findings revealed a default care-giving role particularly for the youngest, single female family member, highlighting a distinct intersectionality of their assumed role as care-givers for their older parents, in-laws or spouses with the prevailing sociocultural norms entrenched in Arab-Muslim societies. Being unmarried appeared to dictate that she should be the one to care for her parents which was seen as more important than her work or studies, while married sisters and brothers were relieved from the care-giving role even if they did not work. Women generally accepted this role and concealed their own mental distress due to a religious sense of duty and societal pressure, which is consistent with the existing literature (McCall, Reference McCall2005; Youssef and Deane, Reference Youssef and Deane2006; Ciftci et al., Reference Ciftci, Jones and Corrigan2013). Although traditional roles in Qatar are changing rapidly, the expectation for women to take on this role without question puts increasing pressure on them as they juggle motherhood, care-giving for the older person with ADRD and their work outside the household (Al-Ghanim, Reference Al-Ghanim2017). Al-Ghanim's (Reference Al-Ghanim2019) study on perceptions of women's roles concurs that traditional social structures perpetuate this gender inequality and limit their participation beyond the private sphere. Our interviews indicated the burden women experience throughout their care-giving experiences and reported on the impact on their quality of life in general. This includes physical, social and mental health. This burden was intensified when women were also wives, mothers or had no economic means to offer a domestic worker or a private nurse to help them. Gender hierarchy is one aspect of this structure whereby married Arab women are expected to fill the role of household managers and care-givers even when they work outside their home like their spouses. Married Arab women in general are expected to take care of their in-laws, while the same is not expected of their husbands. This was evident from our sample whereby the five men in our study, despite identifying themselves as ‘primary care-giver’ of their in-law, parent or spouse, had delegated the daily tasks of caring to a female domestic helper or to their wives or sister. This factor repeated itself among Arab women who are not Qataris and not working, i.e. being expat, not working and having economic hardships increased the burden of care. Subsequent studies on gendered burden and the shifting attitudes and needs of women in contemporary Arab socio-economic contexts are needed, as is the need for public awareness-raising of the importance of sharing care-giving responsibilities among family members given the particularly challenging nature of ADRD care-giving.
While Microsystem factors constituted a heavy load for these mostly female care-givers, their accounts showed that this role was facilitated significantly by these same factors. Rather than viewing care-giving as a ‘burden’, it was interesting to note from the data that family care-givers gave equal weight to the positive rewards associated with their care-giving duties. The motives underpinning these sentiments were rooted in sociocultural expectations but more so in the religious rewards they associated with the prolonged caring role for elders. This reflected a widespread perception that caring for a parent with ADRD was a ‘gift’ or ‘opportunity’ for reward in the hereafter or to ‘give back’, indicating the role of sociocultural and socio-religious beliefs as a source of great solace, resilience and support to care-givers.Footnote 19 Reframing the ‘burden’ into a positive reward enabled family care-givers to see their care-giving role very differently and cope better with the often-protracted care-giving journey. The ability of care-givers in this study to see care-giving in a positive light is not uncommon (Alpert and Womble, Reference Alpert and Womble2015), as is supported by substantive global research.Footnote 20 It suggests that positive coping techniques rooted in the local cultures are a positive mediating force that can facilitate long-term care-giving for persons with ADRD among the formal and informal providers. While it could be questioned whether sociocultural and religious influences played more of a disciplinary role setting non-negotiable expectations from family members towards their older loved ones with ADRD, our study suggested that this motivation for care was appropriated and embodied by care-givers through that socio-religious worldview and an extension of a loving relationship. Indeed, lifelong socialisation processes and seeing their elders doing it for their own older parents contributed to this consistent practice undisputed acceptance of their roles. We did see exceptions where daughters-in-law and one working son expressed more frustration about the pressures of care-giving, however, it was apparent that the absence of supporting domestic helpers or extended families played a role in magnifying these frustrations.
Conclusion
This study qualitatively examined the experiences of informal care-giving of family members for persons with ADRD in Qatar. It offers fresh insight into the less-studied private sphere of the home, showing how families respond to the onset and long-term care of persons with ADRD. The findings reveal the significance of the intersectionality of family care-givers’ lived experiences with ADRD care-giving with various sociocultural, religious and emotional influences. Sociocultural and religious beliefs, in particular, were found largely to underpin perceptions of ADRD, playing a dual role in shaping care-giving practices and the coping mechanisms of care-givers, on the one hand, and perpetuating stigma, misinformation and reluctance to seek help outside of the home, on the other. They offset the challenges of care-giving by highlighting its positive reward within the socio-religious context of Qatar's society, however, they also often played a role in perpetuating expected gender roles that tend to lead to inequalities in care-giving and affect the life choices of female family members.
Bronfenbrenner's ecological model provided a valuable holistic framework that contextualised our study's key findings within the mutually reinforcing influences of surrounding environment upon society, across generations, and into care-givers’ personal belief systems and practices. It helped illuminate the extent to which caring for an older adult with ADRD in an Arab-Muslim context involves an interaction between these various systems. The findings pointed to the mutually reinforcing interpellations and influences between and across systems that, in turn, affected how help-seeking calls are (or are not) made, as well as the quality of care and coping strategies of family care-givers. As previous studies have shown, the Bronfenbrenner model allowed us to examine closely the subtle influences of wider social, cultural and religious norms and expectations on care-giving, on the one hand, while teasing out context-specific challenges and bottlenecks that inhibit effective and timely care, on the other (Bosco et al., Reference Bosco, Schneider, Coleston-Shields and Orrell2019; Bowlby and McKie, Reference Bowlby and McKie2019). Our study identified the need for greater awareness around services, benefits, policies and accurate knowledge sources about ADRD best addressed at Macro- and Exosystem levels, given their direct impact on assumptions, stigma and societal reservations (derived from Micro- and Mesosystem levels). Our findings thus point to the indisputable importance of working with and not just for family care-givers: enhancing prompt detection of ADRD and better utilisation of the ample resources offered by the State of Qatar in support of persons with ADRD and their families. Insights viewed through these ongoing intersections across systems inform care-givers’ wellbeing and resilience, enable providers and policy makers to serve more effectively, both of which ultimately the quality of life of persons living with ADRD.
On a practical level, this study suggests that all these multilevel influences provide a more accurate understanding of care-giving practices for persons with ADRD in a number of Arab and Islamic communities with shared beliefs and practices. A major takeaway from our findings, with implications for policy and practice derived from our findings, is the importance of capitalising on insights from prevalent sociocultural and religious mores and convictions. Taking into account their dual – both positive and negative – roles, family assets that strengthen resilience in care-giving could be better recognised (DeFrain et al., Reference DeFrain, Asay, Badahdah, Abdelmoneium and Abdennadher2018), and those without extended family (namely non-Qatari residents with older parents) considered with the benefits dedicated for family care-givers of persons with ADRD. Qatar's National Dementia Plan (Ministry of Public Health, nd) and its explicit concern with the wellbeing of care-givers, interactions with families and care-giver training would benefit from incorporating these insights. A family-centred approach in dementia care should be recognised within policies and services, and made more explicit within care plans (Hao and Ruggiano, Reference Hao and Ruggiano2020). Further, it is worth investing more in home-based outreach teams that support persons living with ADRD and their family care-givers with attention to strengthening the social support and awareness component. From the other side, the challenge of stigma and associated reluctance to seek help sooner, that was found to be rooted in fear of loss of the older loved one's dignity and families’ social standing, indicates the need for intensive public sensitisation campaigns. The dissemination of correct information about ADRD to families could diffuse this social shame, address public misconceptions and stigma of dementia, and encourage families to seek help earlier (Thornicroft et al., Reference Thornicroft, Brohan, Kassam and Lewis-Holmes2008). Additionally, with a predominantly expatriate (non-Qatari) social and health-care professional workforce, regular training and sensitisation is crucial to ensure attentiveness to culture-specific issues and sensitivities surrounding ADRD.
Strengths and limitations of the study
Given the expected increase of older persons with ADRD in Qatar, this insight better attunes service providers to the critical role of sociocultural and religious beliefs – as both barriers to help-seeking as well as strong motivators for sustained care. This in turn ensures that community-based intervention, awareness programmes, and health and social care practices and policies are more relevant to current family attitudes and practices. We recommend that the following interventions could enhance the effectiveness of ADRD-related campaigns and services: integrating religious perspectives into awareness campaigns; engaging influential religious figures; sensitisation of health-care professionals/providers; supporting family care-givers’ mental health needs during (and after) a diagnosis and providing them with resources throughout their journey; and developing community-based support networks for families. The sensitive nature of the study furnished insufficient disaggregated data on the socio-demographic aspects of care-giving, and further research is recommended to scrutinise these differentials more closely.Footnote 21 The roles and experiences of domestic helpers and nurses who support families caring for older persons with ADRD could also be expanded upon. Inclusion of perspectives and lived experiences of persons with ADRD themselves, whilst challenging both practically and culturally in the conservative Arab context, is particularly important as well. Finally, we propose further evaluative research across the Arab region to compare and extract transferrable lessons from dementia care interventions and campaigns.
Author contributions
SHH drafted the first full draft of the paper, conceptualised and designed the overall study, collected and analysed the data, and was Lead Principal Investigator of the research team. Revisions were made as per reviewers’ comments. SDN, TK and NAW were co-Principal Investigators who reviewed the full draft paper and inputted into it, and were involved in the design of the research tools, data collection and analysis of the overall study, and contributed to the revised paper.
Acknowledgements
This paper is based on a study conducted at Qatar University in 2017/18, generously funded by Centre for Empowerment and Care of the Elderly (Ehsan Centre). It was conceptualised and led by the Centre for Humanities and Social Sciences at Qatar University under the leadership and support of Professor Kaltham Al-Ghanim, and in collaboration with faculty from the College of Medicine, Qatar University. The Centre for Empowerment and Elderly Care-Ehsan organised the official launch of the study in both Arabic and English in September 2019. For the full report of the study, see Hammad et al. (Reference Hammad, Kane, Daher-Nashif and Al-Wattary2019).
Financial support
This work was supported by the Centre for Empowerment and Care of the Elderly (Ehsan Centre) (grant number QUEX-CAS-EHSAN-17/18). The grant maker is a not-for-profit Qatari civil society organisation and its role was to provide the funds and support the research team as needed. They did not play a part in the design, execution, analysis or interpretation and write-up of the data.
Ethical standards
Ethical approval was granted by the Qatar University Institutional Review Board.


