This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
Background: The Ohio State University Wexner Medical Center identified a cluster of coronavirus disease 2019 (COVID-19) cases on an inpatient geriatric stroke care unit involving both patients and staff. The period of suspected severe acute respiratory coronavirus virus 2 (SARS-CoV-2) transmission and exposure on the unit was December 20, 2020, to January 1, 2021, with some patients and staff developing symptoms and testing positive within the 14 days thereafter. Methods: An epidemiologic investigation was conducted via chart review, staff interviews, and contact tracing to identify potential patient and staff linkages. All staff who worked on the unit were offered testing regardless of the presence of symptoms as well as all patients admitted during the outbreak period. Results: In total, 6 patients likely acquired COVID-19 in the hospital (HCA). An additional 6 patients admitted to the unit during the outbreak period subsequently tested positive but had other possible exposures outside the hospital (Fig. 1). One patient failed to undergo COVID-19 testing on admission but tested positive early in the cluster and is suspected to have contributed to patient to employee transmission. Moreover, 32 employees who worked on the unit in some capacity during this period tested positive, many of whom became symptomatic during their shifts. In addition, 18 employees elected for asymptomatic testing with 3 testing positive; these were included in the total. Some staff also identified potential community exposures. Additionally, staff reported an employee who was working while symptomatic with inconsistent mask use (index employee) early in the outbreak period. The index employee likely contributed to employee transmission but had no direct patient contact. Our epidemiologic investigation ultimately identified 12 employees felt to be linked to transmission based on significant, direct patient care provided to the patients within the outbreak period (Fig. 1). In addition, 3 employees had an exposure outside the hospital indicating likely community transmission. Conclusions: Transmission was felt to be multidirectional and included employee-to-employee, employee-to-patient, and patient-to-employee transmission in the setting of widespread community transmission. Interventions to stop transmission included widespread staff testing, staff auditing regarding temperature and symptom monitoring, and re-education on infection prevention practices. Particular focus was placed on appropriate PPE use including masking and eye protection, hand hygiene, and cleaning and disinfection practices throughout the unit. SARS-CoV-2 admission testing and limited visitation remain important strategies to minimize transmission in the hospital.
Figure 1.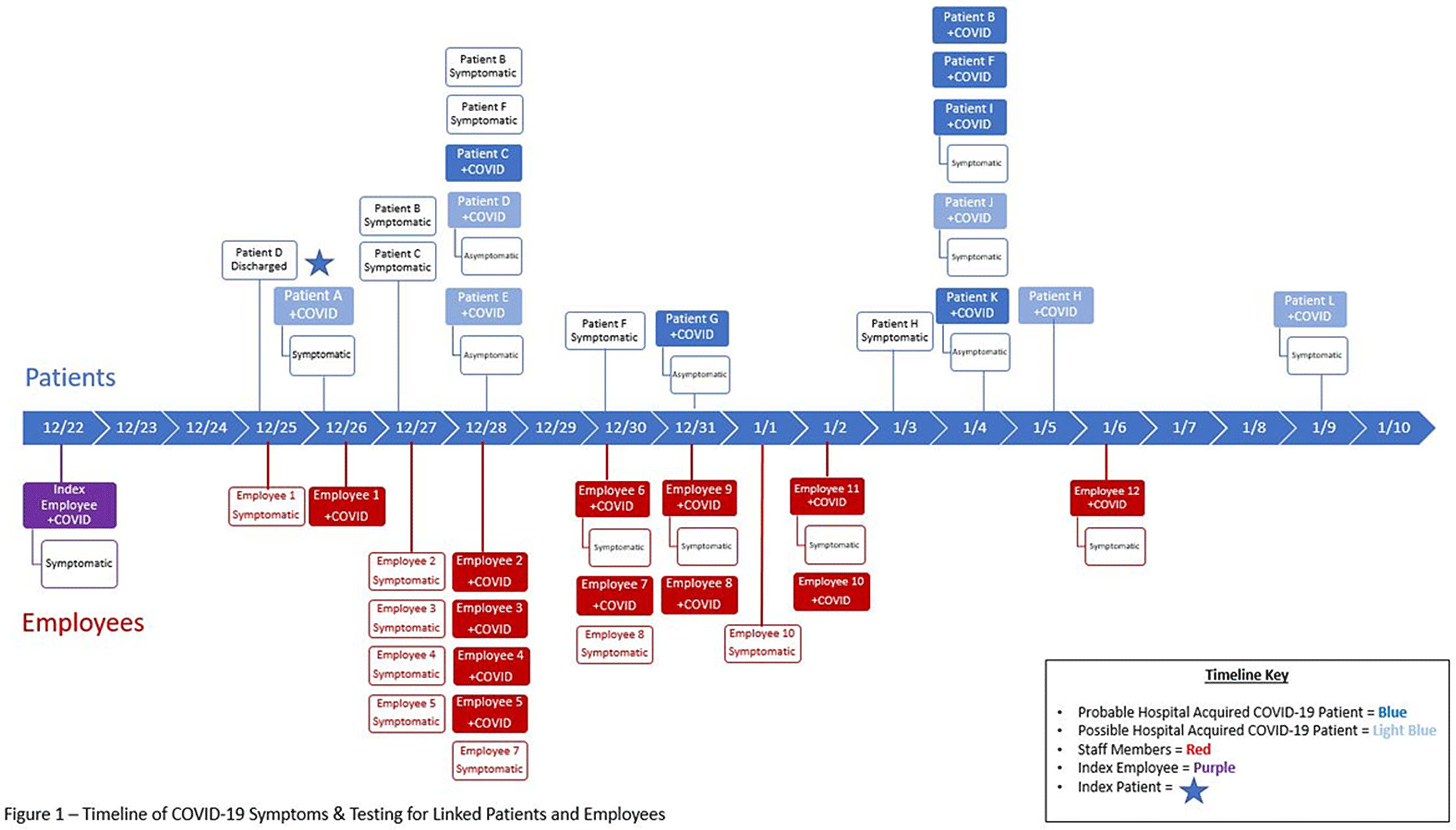
Funding: No
Disclosures: None
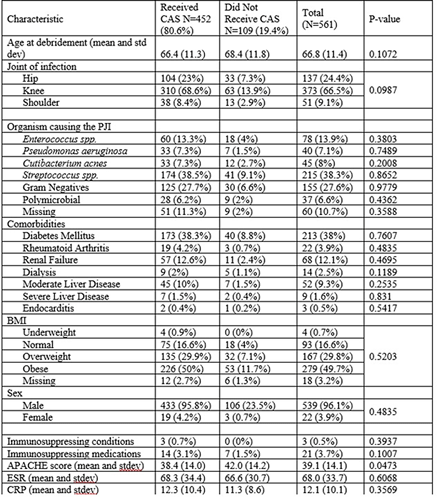
Background: Early postoperative and acute prosthetic joint infection (PJI) may be managed with debridement, antibiotics, and implant retention (DAIR). Among patients with nonstaphylococcal PJI, an initial 4–6-week course of intravenous or highly bioavailable oral antibiotics is recommended in the Infectious Diseases Society of America (IDSA) guidelines, with disagreement among committee members on the need for subsequent chronic oral antimicrobial suppression (CAS). We aimed to characterize patients with nonstaphylococcal PJI who received CAS and to compare them to those who did not receive CAS. Methods: This retrospective cohort study included patients admitted to Veterans’ Affairs (VA) hospitals from 2003 to 2017 who had a PJI caused by nonstaphylococcal bacteria, underwent DAIR, and received 4–6 weeks of antimicrobial treatment. PJI was defined by Musculoskeletal Infection Society (MSIS) 2011 criteria. CAS was defined as at least 6 months of oral antibiotics following initial treatment of the PJI. Patients were followed for 5 years after debridement. We used χ2 tests and t tests were used to compare patients who received CAS with those who did not receive CAS. Results: Overall, 561 patients had a nonstaphylococcal PJI treated with DAIR, and 80.6% of patients received CAS. The most common organisms causing PJI were streptococci. We detected no significant differences between patients who received CAS and those who did not receive CAS, except that modified Acute Physiology and Chronic Health Evaluation (mAPACHE) scores were higher among patients who did not receive CAS (Table 1). Conclusion: Patients not on CAS were more severely ill (by mAPACHE) than those on CAS. Otherwise, the 2 groups were not different. This finding was contrary to our hypothesis that patients with multiple comorbidities or higher mAPACHE scores would be more likely to get CAS. A future analysis will be conducted to assess treatment failure in both groups. We hope to find a specific cohort who may benefit from CAS and hope to deimplement CAS in others who may not benefit from it.
Funding: No
Disclosures: None
Background: Effective inpatient stewardship initiatives can improve antibiotic prescribing, but impact on outcomes like Clostridioides difficile infections (CDIs) is less apparent. However, the effect of inpatient stewardship efforts may extend to the postdischarge setting. We evaluated whether an intervention targeting inpatient fluoroquinolone (FQ) use in a large healthcare system reduced incidence of postdischarge CDI. Methods: In August 2019, 4 acute-care hospitals in a large healthcare system replaced standalone FQ orders with order sets containing decision support. Order sets redirected prescribers to syndrome order sets that prioritize alternative antibiotics. Monthly patient days (PDs) and antibiotic days of therapy (DOT) administered for FQs and NHSN-defined broad-spectrum hospital-onset (BS-HO) antibiotics were calculated using patient encounter data for the 23 months before and 13 months after the intervention (COVID-19 admissions in the previous 7 months). We evaluated hospital-onset CDI (HO-CDI) per 1,000 PD (defined as any positive test after hospital day 3) and 12-week postdischarge (PDC- CDI) per 100 discharges (any positive test within healthcare system <12 weeks after discharge). Interrupted time-series analysis using generalized estimating equation models with negative binomial link function was conducted; a sensitivity analysis with Medicare case-mix index (CMI) adjustment was also performed to control for differences after start of the COVID-19 pandemic. Results: Among 163,117 admissions, there were 683 HO-CDIs and 1,009 PDC-CDIs. Overall, FQ DOT per 1,000 PD decreased by 21% immediately after the intervention (level change; P < .05) and decreased at a consistent rate throughout the entire study period (−2% per month; P < .01) (Fig. 1). There was a nonsignificant 5% increase in BS-HO antibiotic use immediately after intervention and a continued increase in use after the intervention (0.3% per month; P = .37). HO-CDI rates were stable throughout the study period, with a nonsignificant level change decrease of 10% after the intervention. In contrast, there was a reversal in the trend in PDC-CDI rates from a 0.4% per month increase in the preintervention period to a 3% per month decrease in the postintervention period (P < .01). Sensitivity analysis with adjustment for facility-specific CMI produced similar results but with wider confidence intervals, as did an analysis with a distinct COVID-19 time point. Conclusion: Our systemwide intervention using order sets with decision support reduced inpatient FQ use by 21%. The intervention did not significantly reduce HO-CDI but significantly decreased the incidence of CDI within 12 weeks after discharge. Relying on outcome measures limited to inpatient setting may not reflect the full impact of inpatient stewardship efforts and incorporating postdischarge outcomes, such as CDI, should increasingly be considered.
Funding: No
Disclosures: None
Figure 1.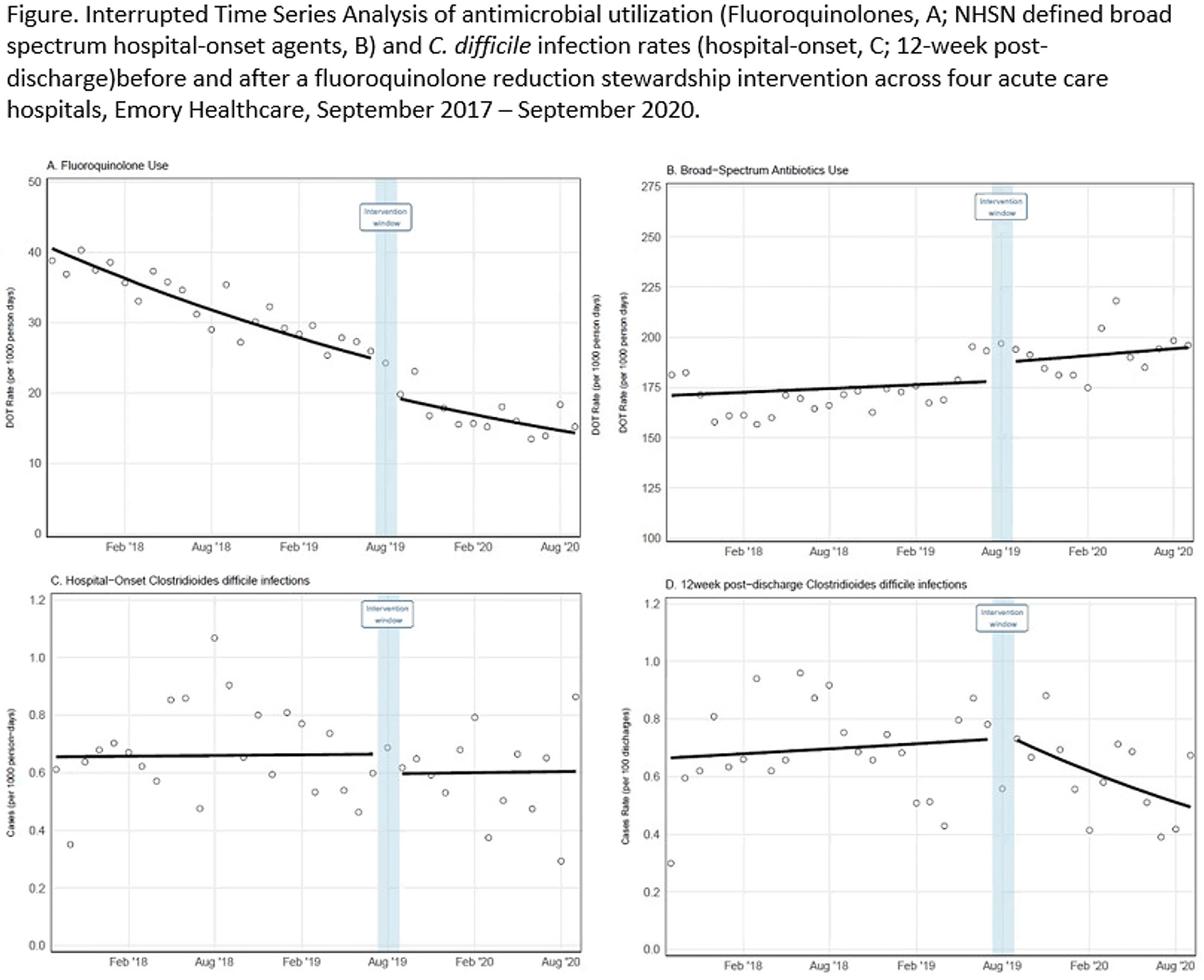
Background: Antibiotics targeted against Clostridioides difficile bacteria are necessary, but insufficient, to achieve a durable clinical response because they have no effect on C. difficile spores that germinate within a disrupted microbiome. ECOSPOR-III evaluated SER-109, an investigational, biologically derived microbiome therapeutic of purified Firmicute spores for treatment of rCDI. Herein, we present the interim analysis in the ITT population at 8 and 12 weeks. Methods: Adults ≥18 years with rCDI (≥3 episodes in 12 months) were screened at 75 US and CAN sites. CDI was defined as ≥3 unformed stools per day for <48 hours with a positive C. difficile assay. After completion of 10–21 days of vancomycin or fidaxomicin, adults with symptom resolution were randomized 1:1 to SER-109 (4 capsules × 3 days) or matching placebo and stratified by age (≥ or <65 years) and antibiotic received. Primary objectives were safety and efficacy at 8 weeks. Primary efficacy endpoint was rCDI (recurrent toxin+ diarrhea requiring treatment); secondary endpoints included efficacy at 12 weeks after dosing. Results: Overall, 287 participants were screened and 182 were randomized (59.9% female; mean age, 65.5 years). The most common reason for screen failure was a negative C. difficile toxin assay. A significantly lower proportion of SER-109 participants had rCDI after dosing compared to placebo at week 8 (11.1% vs 41.3%, respectively; relative risk [RR], 0.27; 95% confidence interval [CI], 0.15–0.51; p-value <0.001). Efficacy rates were significantly higher with SER-109 vs placebo in both stratified age groups (Figure 1). SER-109 was well-tolerated with a safety profile similar to placebo. The most common treatment-emergent adverse events (TEAEs) were gastrointestinal and were mainly mild to moderate. No serious TEAEs, infections, deaths, or drug discontinuations were deemed related to study drug. Conclusions: SER-109, an oral live microbiome therapeutic, achieved high rates of sustained clinical response with a favorable safety profile. By enriching for Firmicute spores, SER-109 achieves high efficacy while mitigating risk of transmitting infectious agents, beyond donor screening alone. SER-109 represents a major paradigm shift in the clinical management of patients with recurrent CDI. Clinicaltrials.gov Identifier NCT03183128. These data were previously presented as a late breaker at American College of Gastroenterology 2020.
Funding: Seres Therapeutics
Disclosures: None
Figure 1.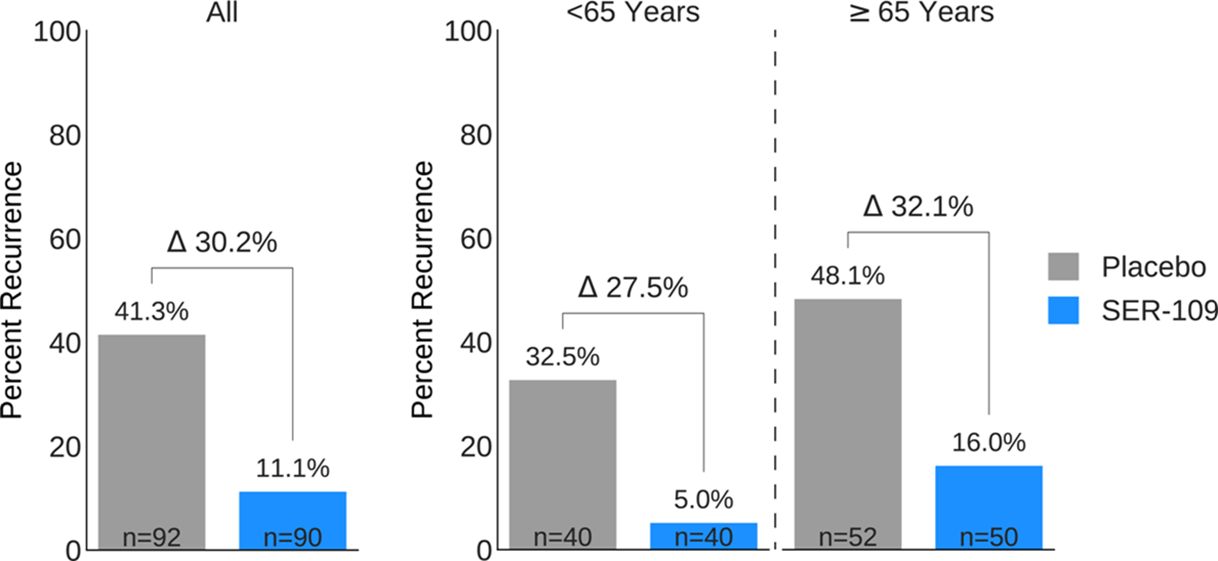
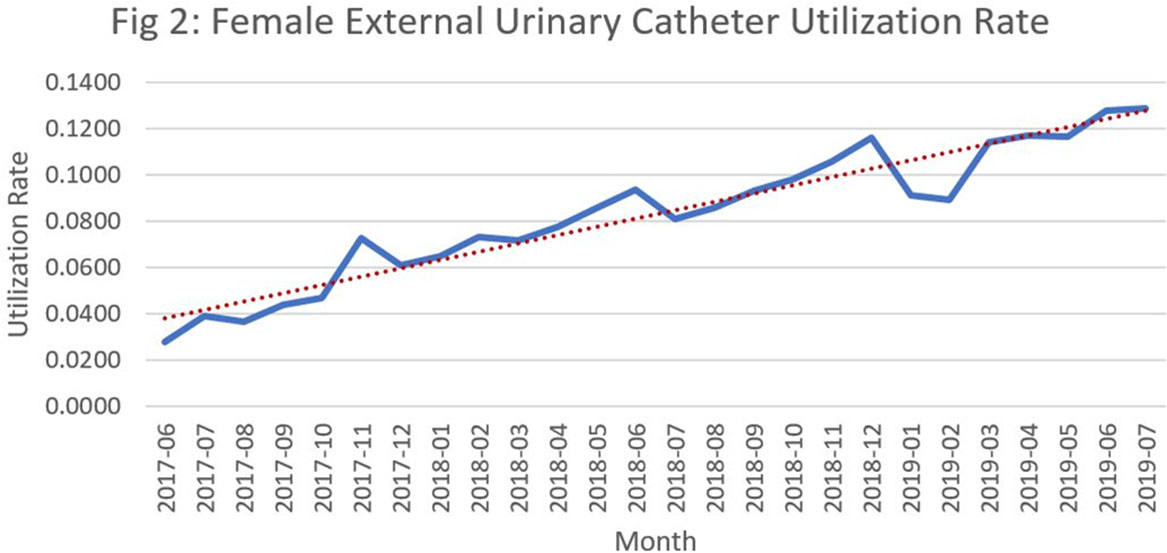
Background: Catheter-associated urinary tract infections (CED: TIs) are one of the most prevalent healthcare-associated infections. They can lead to bacteremia and increased length of stay, healthcare costs, and mortality. Indwelling urinary catheter (IUC) prevention bundles, nurse-driven removal protocols, and the use of external catheters can help reduce CED: TIs. However, female external urinary catheters (FEUCs) have only recently become widely available. FEUCs were introduced at our institution in July 2017. The purpose of this study was to evaluate the impact of FEUC on IUC utilization ratio and overall CED: TI rate in an 844-bed teaching hospital in southeastern Michigan. Methods: We retrospectively evaluated the utilization ratio of FEUCs (female FEUC days per patient days ×1,000) and female IUCs (IUC days per patient days ×1,000), and labia hospital-acquired pressure injury (HAPI) rate due to FEUC from July 2017 through June 2019. We compared the overall (male and female) CED: TI rate per 1,000 IUC days in the preintervention period (January 2016 to June 2017) to the postintervention period (July 2017 to June 2019). Results: In total, 4,013 FEUCs were placed during the intervention period. The utilization ratio of FEUC increased by 59% and the utilization ratio of female IUC decreased by 13% over the course of the 2 years. Only 1 HAPI was reported during the observation period at a rate of 0.025% (1 of 4,013). The overall CED: TI rate decreased from 1.60 to 1.40 (P = .372). Conclusion: Introduction of a FEUC was associated with a decrease in the IUC utilization ratio in female patients with minimal adverse events; however, there was no significant difference in the overall CED: TI rate.
Funding: No
Disclosures: None
Figure 1.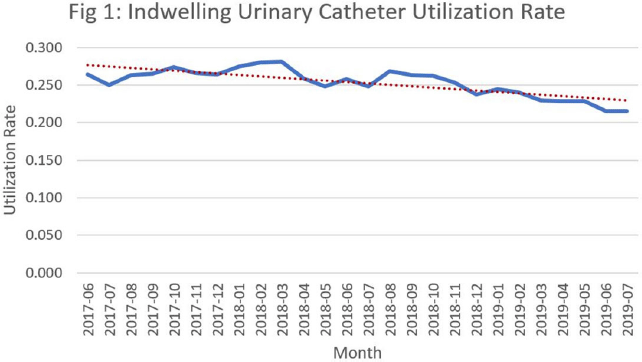
Figure 2.