This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
Background: The disease caused by SARS-CoV-2, COVID-19, has caused a pandemic leading to strained healthcare systems worldwide and an unprecedented public health crisis. Lower respiratory tract infections (LRTIs) and hypoxia caused by COVID-19 has led to an increase in hospitalizations. We sought to define the impact of COVID-19 on antimicrobial use and antimicrobial resistance (AMR) in an urban safety-net community hospital. Methods: Retrospective review of antimicrobial use and AMR in a 151-bed urban community hospital. Antimicrobial use was calculated in days of therapy per 1,000 patient days (DOT/1,000 PD) for ceftriaxone, piperacillin-tazobactam and meropenem during 2019 and 2020. Ceftriaxone, piperacillin-tazobactam and meropenem were reviewed for calendar year 2019 and 2020. AMR was assessed by comparing the carbapenem resistant Enterobacteriaceae (CRE) infection incidence rate per 1,000 patient days between 2019 and 2020. Results: The average quarterly DOT/1,000 PD increased from 359.5 in 2019 to 394.25 in 2020, with the highest increase in the second and fourth quarters of 2020, which temporarily correspond to the first and second waves of COVID-19. Ceftriaxone and meropenem use increased during the first and second waves of COVID-19. Piperacillin-tazobactam use increased during the first wave and declined thereafter (Figure 1). Rates of CRE increased from a quarterly average of 0.57 to 0.68 (Figure 2). Conclusions: Antimicrobial pressure increased during the first and second waves of COVID-19. Ceftriaxone was the most commonly used antimicrobial, reflecting internal guidelines and ASP interventions. CRE rates increased during COVID-19. This finding may be due to an overall increase in antimicrobial pressure in the community and in critically ill patients. Antibiotics are a precious resource, and antimicrobial stewardship remains important during the COVID-19 pandemic. Appropriate use of antimicrobials is critical to preventing AMR.
Funding: No
Disclosures: None
Figure 1.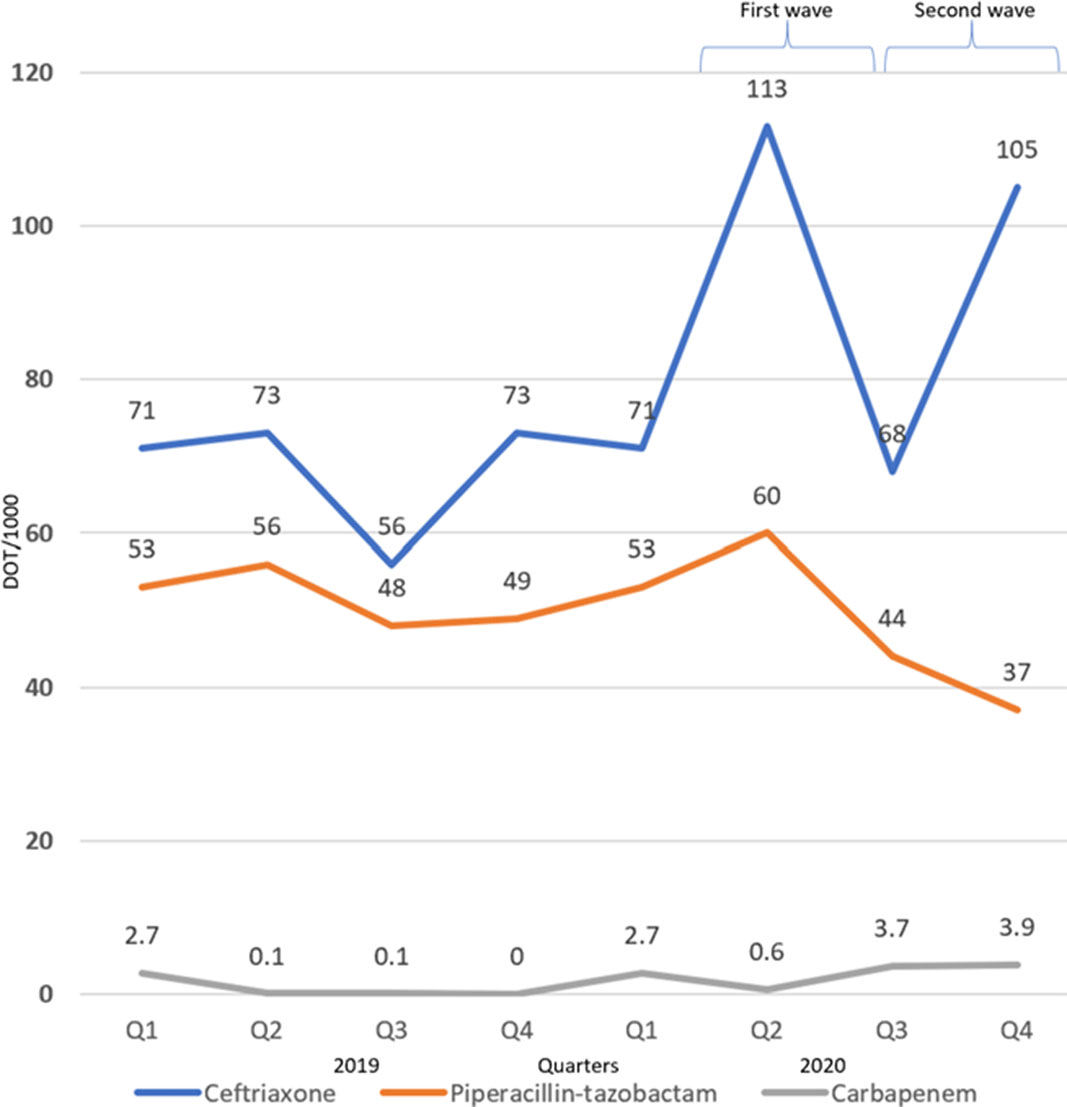
Figure 2.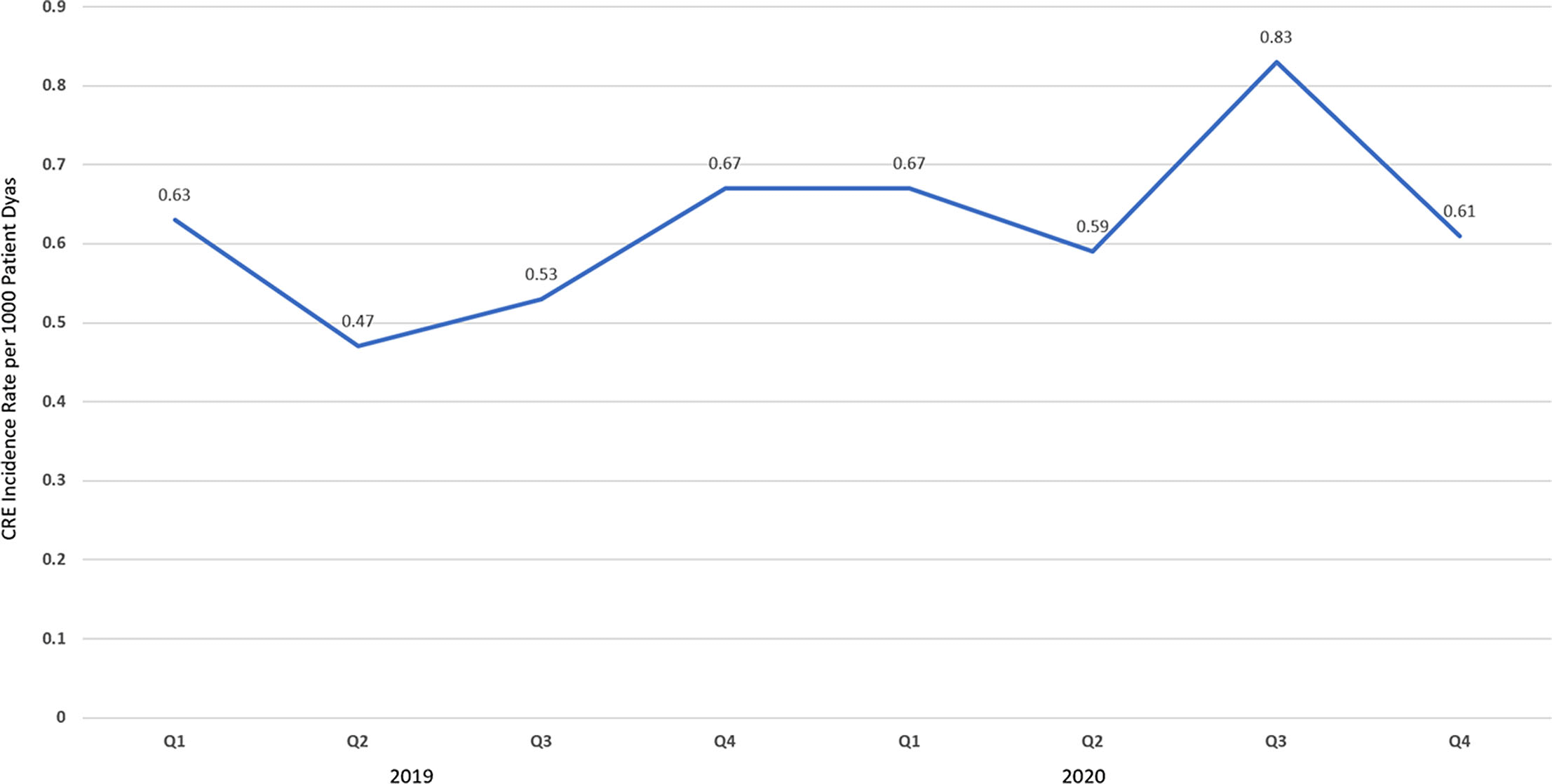
Background: The gold standard for diagnosis of COVID-19 has been SARS-CoV-2 detection by reverse-transcriptase-quantitative polymerase chain reaction (RT-qPCR), which provides a semiquantitative indicator of viral load (cycle threshold, Ct). Our research group previously described how African American race and poverty were associated with an increased likelihood of hospitalization due to COVID-19. We sought to characterize the relationship between Ct values and clinical outcomes while controlling for sociodemographic factors. Methods: We conducted a cross-sectional study of SARS-CoV-2–positive patients admitted to Froedtert Health between March 16 and June 1, 2020. Ct values were obtained by direct interrogation of either cobas SARS-CoV-2 or Cepheid Xpert Xpress platforms. Patient demographics, comorbidities, symptoms at admission, health insurance, and hospital course were collected using electronic medical records. A proxy for socioeconomic disadvantage, area-deprivation index (ADI), was assigned using ZIP codes. Multivariate models were performed to assess associations between Ct values and clinical outcomes while controlling for ADI, race, and type of insurance. Results: Overall, 302 patients were included. The mean age was 60.89 years (SD, 18.2); 161 (53%) were men, 177 (58%) were African Americans; and 156 (51%) had Medicaid or were uninsured. Of the 302 inpatients, 158 (52%) required admission to the ICU, 199 (65.9%) were discharged to home, 49 (16.2%) were discharged to a nursing home, and 54 (17.9%) died. Lower Ct values (higher viral load) were associated with Medicaid or lack of insurance (coefficient, −2.88, 95% confidence interval [CI], −4.96 to −0.79, P = .007) and age >60 years old (coefficient, −2.98, 95% CI −4.87 to −1.08, P = .002). Contrary to what was expected, higher CT values (lower viral load) were associated with higher ADI scores (coefficient, 2.62, 95% CI, 0.52–4.85; P = .017). However, when patients were stratified into low, medium, and high ADI, those with Medicaid or no insurance had the lowest mean Ct values (23.3, 25.9, and 27.6, respectively) compared to Medicare or other insurance (Figure 1). Body mass index (odds ratio [OR], 1.04; 95% CI, 1.02–1.07; P = .001) and male sex (OR, 2.15; 95% CI, 1.28–3.60; P = .004) were independently associated with ICU admission. Every increase of a CT point (OR, 0.90; 95% CI, 0.85–0.95; p <0.001) and age >60 years old (OR 2.62, 95% CI; 1.14-6.04; p=0.023) was associated with death. Conclusions: In this cross-sectional study of adults tested for COVID-19 in a large midwestern academic health system, lower Ct values were independently associated with poverty and age >60 years old.
Funding: No
Disclosures: None
Figure 1.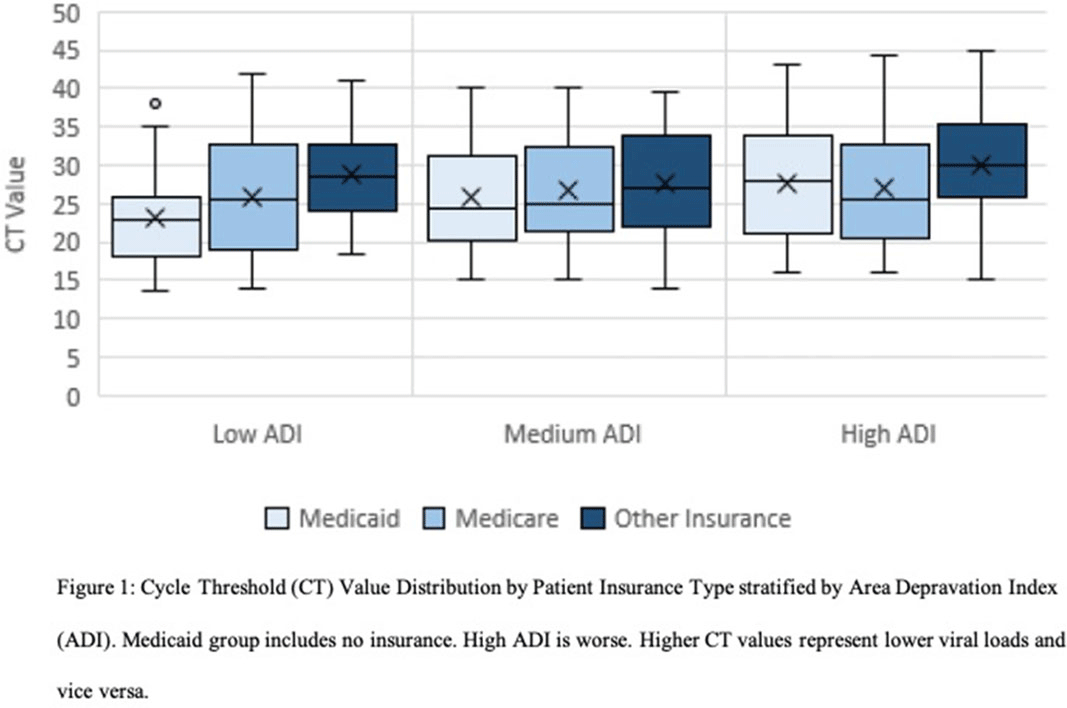
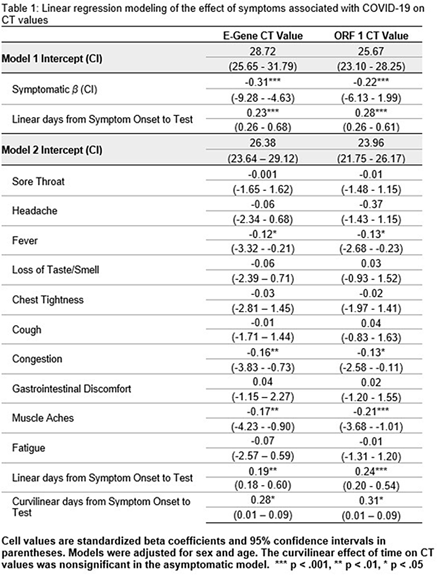
Background: SARS-CoV-2 detected by reverse transcription polymerase chain reaction (RT-PCR) can persist for weeks to months in some individuals. Cycle threshold (Ct) values represent the number of cycles needed to amplify viral ribonucleic acid (RNA) to reach a detectable level. As such, Ct values are inversely related to the amount of virus in a sample. As knowledge of SARS-CoV-2 viral dynamics continues to evolve, understanding the relationship between Ct values, type of symptoms, and timing of symptom onset can help determine when infected individuals are most likely to be infectious. Methods: We conducted a retrospective cohort study of 1,027 healthcare workers (HCWs) who tested positive for SARS-CoV-2 by RT-PCR from nasopharyngeal specimens between June 27, 2020, and September 21, 2020. All HCWs were interviewed within 72 hours of their diagnosis for symptom history. Due to multiple PCR platforms being in use in our facility, only 360 HCWs (35%) had Ct values available for analysis. Multivariate linear regression models examined the effect of COVID-19–related symptoms and timing of symptom onset to test on Ct values. Results: The most frequently reported symptoms were congestion (55.6%), cough (50.3%), and headache (46.7%). Other symptoms less commonly reported were fatigue (36.7%), loss of taste or smell (36.4%), fever (35.4%), muscle aches (33.3%), sore throat (27.4%), and diarrhea (26.7%). Symptomatic HCWs (88.3% of sample) had lower Ct values (ORF-1 M = 22.66, SD = 5.17; E-Gene M = 24.34, SD = 6.60) than asymptomatic individuals (ORF-1 M = 25.46, SD = 6.06; E-Gene M = 29.34, SD = 7.96). Of all symptoms measured, only presence of fever, congestion, and muscle aches predicted significantly lower Ct values. Mean Ct values decreased 2 days prior to symptom onset, were lowest the day of symptom onset, then increased in a curvilinear fashion. There were no significant 2-way interactions between symptoms and time of symptom onset to testing. Conclusions: The curvilinear pattern of Ct values over time from symptom onset are consistent with disease progression patterns and support current understanding of infectivity being highest 2 days prior to symptom onset through day 8. Presence of fever, congestion, and muscle aches are significantly correlated with lower Ct values, suggesting that these symptoms are associated with higher viral load. Although Ct values are not without limitations, our findings support the current understanding that presymptomatic and symptomatic individuals, particularly those with fever, congestion, and muscle aches, may pose higher risk of transmission to others.
Funding: No
Disclosures: None
Figure 1.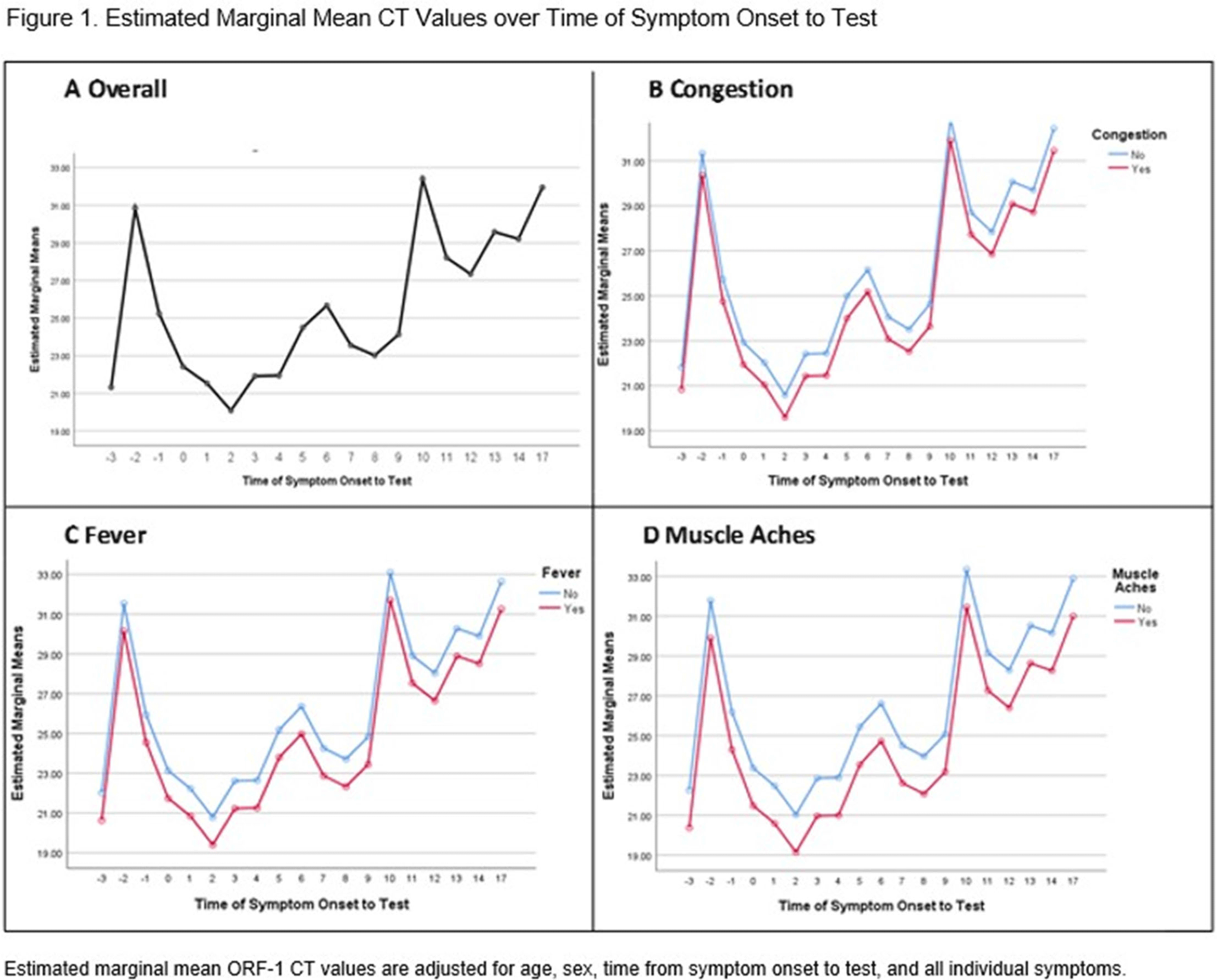
Figure 2.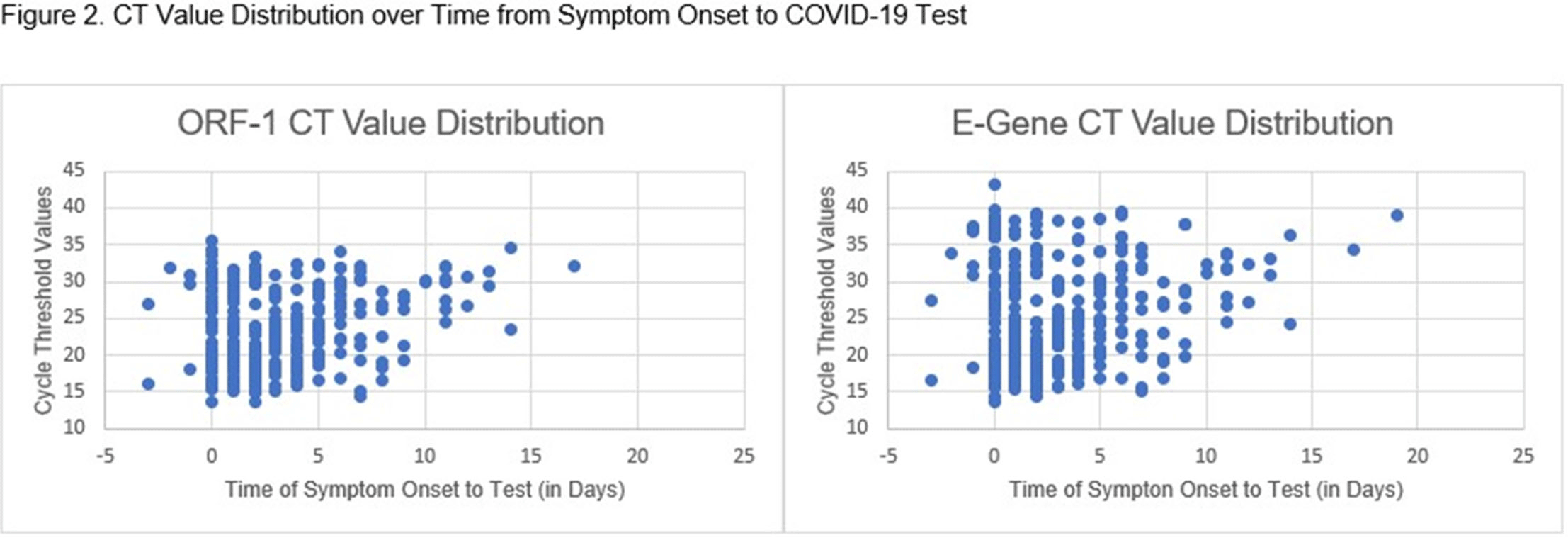
Background: The COVID-19 pandemic has created personal protective equipment (PPE) shortages, particularly of N95 respirators. Institutions have used decontamination strategies including vaporous hydrogen peroxide (VHP) to augment respirator supplies. VHP can be used to decontaminate nonporous surfaces without compromising material integrity. However, little is known about its impact on N95 respirator efficacy. We assessed whether repeated VHP reprocessing altered 4 key respirator efficacy qualities: quantitative fit, qualitative fit, seal check, and filtration rate. Methods: We conducted a prospective cohort study from June 15 to August 31, 2020. In total, 7 participants were fitted to a 3M 1860 small or regular N95 respirator based on qualitative and quantitative fit testing. Respirators underwent 25 disinfection cycles with the Bioquell BQ-50 VHP generator. After each cycle, participants donned and doffed respirators and performed a seal check. Participants were given 2 attempts to pass their seal check. Every 10 cycles, qualitative fit testing was done using an aerosolized Bitrex solution. Quantitative fit testing was conducted using a PortaCount Pro 8038 Fit Tester to generate a fit factor score. Appropriate fit is defined as a fit factor score of 100 or greater. Quantitative testing was done at cycles 1, 3, 5, 7, 10, 15, 20, and 25. Filtration efficiencies of particles ≥0.3 µm in diameter were measured using the TSI Optical Particle Sizer 3330 at cycles 1, 5, 10, 15, 20, and 25. The Fisher exact test was used to assess qualitative fit and seal check. The Kruskal-Wallis test was used to analyze quantitative fit and filtration rate. Results: We observed no seal-check or quantitative-fit test failures during the study window. All participants passed qualitative fit testing. Although there was a significant degree of variability in fit factor scores across disinfection cycles (mean score 163.5, p <0.05), there was no significant difference between participants (p = 0.6) (Figure 1). There was no statistically significant change in mean filtration rate from cycle 10 to 25 (P = .05), and the filtration rate remained >95% by cycle 25 (Figure 2). Conclusions: VHP reprocessing did not diminish the efficacy of N95 respirators based on the 4 metrics we assessed: filtration rate, seal check, qualitative fit, and quantitative fit. Of significance, the filtration rate remained well above the 95% standard filtration for N95 respirators—even through 25 cycles of reprocessing. VHP reprocessing is a safe, viable strategy to disinfect N95 respirators and extend their use, particularly during supply shortages.
Funding: No
Disclosures: None
Figure 1.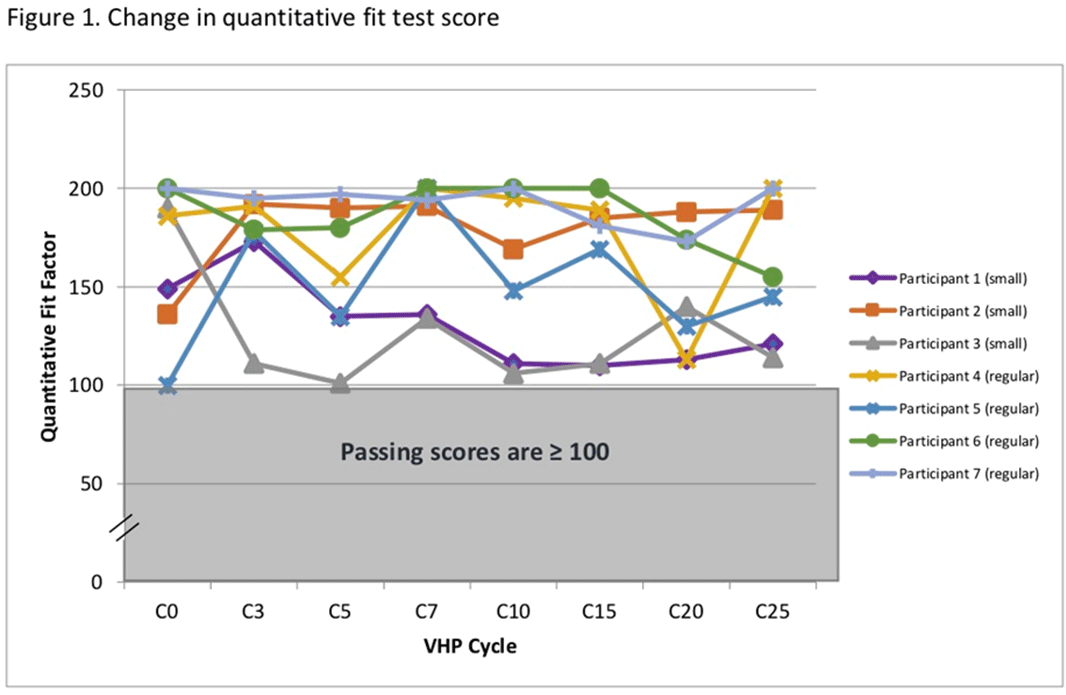
Figure 2.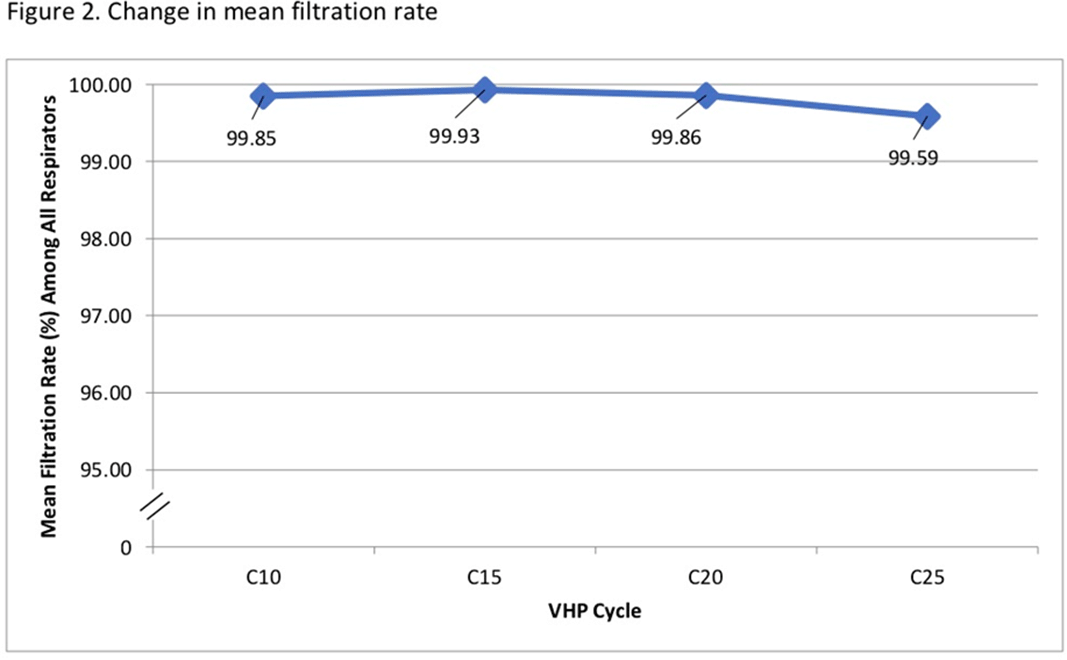
Background: A pathogenic group of invasive extraintestinal pathogenic (ExPEC) Escherichia coli possess the ability to infect normally sterile body sites and cause severe invasive ExPEC disease (IED). ExPEC is a leading cause of bacteremia and sepsis worldwide and is associated with older age and multidrug-resistant infections. Janssen Vaccines & Prevention is developing a novel multivalent glycoconjugate vaccine to prevent IED. We aimed to use an unbiased approach, with no prespecified potential risk factors, using machine-learning models, to screen for and identify IED risk factors for further validation. Methods: We used a patient-level prediction study design to model the probability of a patient developing IED within 14 days to 1 year from a given date based on their prior 2 years of health records. We used the Optum EHR database (~98 million subjects) in the common data model (CDM) format, with health features encoded in the following categories: conditions, procedures, drugs, healthcare visits, recent laboratory measurements, and age and gender. A gradient boosting model (XGBoost) was used with Shapley additive explanation (SHAP) values to identify which features were most important to the model’s decisions and to characterize precisely the relationship between features and outcomes (binary or continuous). Results: Study participants were aged ≥60 years at index with no previously recorded IED. Of ~6,500,000 cases included, ~8,000 had IED during the prediction window. We found that having ≥1 urinary tract infection (UTI) in the retrospective period increased the model’s probability of predicting IED for that patient, with more frequent or more recent UTIs increasing IED prediction chance (Figure 1). Higher age linearly increased the model’s likelihood of predicting that a patient would develop IED. The model also identified ≥1 inpatient or ER visit and laboratory values indicative of renal or immune dysfunction to be correlated with increased IED risk. This methodology is a generalizable approach to screening for potential risk factors for an outcome using EHR databases; it requires little to no prespecification of the health factors or precise relationship between the factors and outcome. Conclusions: Using a new, impartial methodology (with no prespecification), older age and a history of UTIs were key predictive features for IED, factors previously identified through traditional analysis, confirming the validity of the methodology. Novel features, including recent hospitalization, were shown to increase IED risk relative to existing criteria. Our findings may be used to inform the clinical development of preventive strategies.
Funding: Janssen Research and Development
Disclosures: None
Figure 1.
