



Introduction
Sports-related concussion (SRC) can be described as a temporary neurological dysfunction that results from a direct or indirect impact to the head (Carpenter, Lininger, & Craig, Reference Carpenter, Lininger and Craig2020; O'Reilly et al., Reference O'Reilly, Mahon, Reid, Hume, Hardaker and Theadom2020). SRCs can result from high-impact collisions, falls, and direct blows to the head, face, or neck, by an opponent (e.g., a player’s arm) or an object (e.g., a ball) (Labiste, McElroy, Chaniotakis, Duong, & Haffizulla, Reference Labiste, McElroy, Chaniotakis, Duong and Haffizulla2021; Mihalik, Lynall, Teel, & Carneiro, Reference Mihalik, Lynall, Teel and Carneiro2014). Physiologically, concussion causes a neurochemical cascade resulting in ionic shifts, altered metabolism, and decreased connections leading to alterations in neurotransmission in the brain (Giza & Hovda, Reference Giza and Hovda2001). These neurochemical changes in the brain result in the signs and symptoms we observe in cases of concussion (e.g., headache, amnesia, dizziness, difficulty concentrating, confusion, sleep disturbances, irritability, and mental fogginess) (Ferry & DeCastro, Reference Ferry and DeCastro2021). Recovery from a concussive episode takes an average of 7 to 10 days in 80%–90% of cases (Labiste et al., Reference Labiste, McElroy, Chaniotakis, Duong and Haffizulla2021), especially when guidelines are known and are appropriately followed by clinicians and athletes (Register-Mihalik et al., Reference Register-Mihalik, Guskiewicz, McLeod, Linnan, Mueller and Marshall2013a). Failure to follow these guidelines, due to a lack of awareness or dismissing the risk, combined with a return to sport before full resolution of the initial symptoms, can increase the risk of what is termed ‘second impact syndrome’. Second impact syndrome describes the diffuse and potentially catastrophic cerebral oedema caused by a second concussion (McLendon, Kralik, Grayson, & Golomb, Reference McLendon, Kralik, Grayson and Golomb2016). As such, to minimise the risk of this, and the potential long-term implications of repeated concussions, it is essential the symptoms, guidelines, and risk is fully understood by all parties involved in the management of SRC.
Due to the potential long-term implications, concussion is referred to as a major health concern (Finch, Clapperton, & McCrory, Reference Finch, Clapperton and McCrory2013). Hence, clinicians, researchers in sports medicine, and national governing bodies (e.g., Fédération Internationale de Football Association) have developed a keen interest in the symptoms, management, and long-term consequences of concussion (Fuller, Junge, & Dvorak, Reference Fuller, Junge and Dvorak2011). Additionally, the recognition of a concussion has been heavily prioritised by some, with several sports now introducing video technology (e.g., rugby league) and sensors (e.g., instrumented mouthguards) that are thought to support sports medicine clinicians in the detection and diagnosis of SRC (Mooney et al., Reference Mooney, Self, ReFaey, Elsayed, Chagoya, Bernstock and Johnston2020).
SRC continues to receive considerable attention by national governing bodies, governments, sports clubs, the media, and the medical community. According to the Centre for Disease Control and Prevention, 1.6–3.0 million concussions are sustained during sports and recreational activities in America each year (Langlois, Rutland-Brown, & Wald, Reference Langlois, Rutland-Brown and Wald2006). No such insight is available for less developed countries. Currently, SRC research is largely focused on American football, ice hockey and rugby given high-impact collisions are common, there are clearer mechanisms, and resources are available to capture this data. In continents such as Africa, there is limited evidence available on the epidemiology of concussion, and where this does exist, it largely focuses on rugby union in South Africa given the popularity of the sport and the emphasis World Rugby places on SRC (Patricios, Kohler, & Collins, Reference Patricios, Kohler and Collins2010; Viljoen, Schoeman, Brandt, Patricios, & Van Rooyen, Reference Viljoen, Schoeman, Brandt, Patricios and Van Rooyen2017). However, recently greater focus has been placed on SRC and sub-concussive forces in football (soccer) (Labiste et al., Reference Labiste, McElroy, Chaniotakis, Duong and Haffizulla2021). Football is the most popular and fastest-growing sport in the world with over 270 million people actively engaged (registered and unregistered) in the sport (FIFA Communications Division, 2007). Recent high-profile cases of [suspected] concussion, and the controversies of the 2014 World Cup (e.g., Germany’s Midfielder) and 2021 African Cup of Nations (e.g., Senegal’s Striker), have increased the awareness in football (Williams, Langdon, McMillan, & Buckley, Reference Williams, Langdon, McMillan and Buckley2016). The incidence of concussion in football is estimated to be 0.2–6.9 injuries per 1000 playing hours (Mooney et al., Reference Mooney, Self, ReFaey, Elsayed, Chagoya, Bernstock and Johnston2020). Additionally, elite male and female football players competing for 10 years have a 50% and 20% chance, respectively, of developing symptoms associated with multiple SRCs (Covassin, Swanik, & Sachs, Reference Covassin, Swanik and Sachs2003). In Africa, Wallace et al. (Reference Wallace, Mulenga, Bretzin, Delfin, Muyinda, Sichizya and Mulenga2021) recently stated that, amongst 125 Zambian footballers, 7.2% reported that they had previously sustained a concussion which is likely to be higher when considering reporting behaviours, attitudes and knowledge of players.
Studies have examined footballers’ knowledge of concussion, with results revealing mixed findings (Broglio et al., Reference Broglio, Vagnozzi, Sabin, Signoretti, Tavazzi and Lazzarino2010; Cournoyer & Tripp, Reference Cournoyer and Tripp2014; Gallagher & Falvey, Reference Gallagher and Falvey2017; Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). A mixed-methods study by Williams et al. (Reference Williams, Langdon, McMillan and Buckley2016) noted an average concussion knowledge score of 65.6% amongst English professional footballers. A slightly higher mean score (74.8%) was found in a cross-sectional study of Irish amateur and semi-professional players (Gallagher & Falvey, Reference Gallagher and Falvey2017). Similarly, in a study including junior soccer player in Canada, knowledge was on average 78.8% using the Rosenbaum Concussion Knowledge and Attitudes Survey student version (RoCKAS-ST) (Doucette, Du Plessis, Webber, Whalen, & Garcia-Barrera, Reference Doucette, Du Plessis, Webber, Whalen and Garcia-Barrera2021). Two studies conducted amongst high-school footballers revealed that over 50% were not aware of concussion symptoms and return to play guidelines (Anderson, Gittelman, Mann, Cyriac, & Pomerantz, Reference Anderson, Gittelman, Mann, Cyriac and Pomerantz2016; Cournoyer & Tripp, Reference Cournoyer and Tripp2014), meaning that most of the footballers studied would not have adequate knowledge to be able to report a concussion nor follow appropriate guidance. Clearly, increasing concussion knowledge is an important stage in the concussion-care-process for both coaches and players since it aids symptom recognition (Daneshvar et al., Reference Daneshvar, Yutsis, Baugh, Pea, Goldman, Grant and Sorcar2021; Register-Mihalik et al., Reference Register-Mihalik, Williams, Marshall, Linnan, Mihalik, Guskiewicz and McLeod2018). For example, a prospective cohort study by Kurowski, Pomerantz, Schaiper, Ho, & Gittelman (Reference Kurowski, Pomerantz, Schaiper, Ho and Gittelman2015) compared the effect of a pre-season, lecture-based education programme on concussion knowledge at a high school compared to a control school. Statistical improvements were identified in knowledge and self-reported behaviour/attitudes at the end of the season. Doucette et al. (Reference Doucette, Du Plessis, Webber, Whalen and Garcia-Barrera2021) also noted among a group of young rowers, soccer players and contact sport athletes, that the odds of past non-discloser of SRC or the intention of non-disclosure was slightly lower (odds ratio = 0.88–0.95) with greater SRC knowledge. Hence education on the symptoms, implications, and management strategies might be one route for improving concussion recognition, reporting, and management (Van Vuuren, Welman, & Kraak, Reference Van Vuuren, Welman and Kraak2020).
Many behaviours are influenced by one’s attitude, with more positive attitudes often being associated with the preferred behaviour (Raudsepp, Viira, & Hannus, Reference Raudsepp, Viira and Hannus2010). Some studies have examined the attitude of footballers towards SRC (Gallagher & Falvey, Reference Gallagher and Falvey2017; Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). Williams et al. (Reference Williams, Langdon, McMillan and Buckley2016) revealed that English players had an average attitude score of 79.4% which was similar in Irish players at 80% (Gallagher & Falvey, Reference Gallagher and Falvey2017) and Canadian junior soccer player at 85.4% (Doucette et al., Reference Doucette, Du Plessis, Webber, Whalen and Garcia-Barrera2021), suggesting a good attitude towards SRC. However, through a semi-structured interview, many respondents reported unsafe concussion behaviours despite accurately identifying the potential risks (Williams et al., Reference Williams, Langdon, McMillan and Buckley2016), with 64% indicating they would continue playing after a concussion (Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). Non-disclosure of concussions has been linked to several factors (Kirkwood, Parekh, Ofori-Asenso, & Pollock, Reference Kirkwood, Parekh, Ofori-Asenso and Pollock2015); for example, McCrea, Hammeke, Olsen, Leo, and Guskiewicz (Reference McCrea, Hammeke, Olsen, Leo and Guskiewicz2004) and Register-Mihalik et al. (Reference Register-Mihalik, Linnan, Marshall, Valovich-McLeod, Mueller and Guskiewicz2013b) found three common causes for not reporting athletic concussions with 66.4%–70.2% of athletes not believing the injury necessitated medical care, 36.5%–41.0% not wanting to be withdrawn from the game or suspended for future games, and 14.9%–36.1% were not aware they might have sustained a concussion.
Most of the literature exploring SRC comes from the Western World, with only a very small number of studies being undertaken in South Africa albeit involving rugby players (Patricios et al., Reference Patricios, Kohler and Collins2010; Viljoen et al., Reference Viljoen, Schoeman, Brandt, Patricios and Van Rooyen2017) and collegiate athletes (van Tonder, Kunorozva, Viviers, Derman, & Brown, Reference Van Tonder, Kunorozva, Viviers, Derman and Brown2021). With over 6.5 million footballers (men and women), Nigeria has the highest number of soccer players in Africa, and it serves as an instrument for personal development for individuals through increased physical activity (Owoeye, VanderWey, & Pike, Reference Owoeye, VanderWey and Pike2020). However, involvement in sports such as football exposes players to injury risk (Owoeye, Aiyegbusi, Fapojuwo, Badru, & Babalola, Reference Owoeye, Aiyegbusi, Fapojuwo, Badru and Babalola2017). In an underdeveloped country like Nigeria, where medical treatment is sometimes limited, the ‘horror of a player suffering an injury is unthinkable’. Unfortunately, there are only a few studies based in Nigeria which can help us understand the pattern of football injuries, especially concussions (Azubuike & Okojie, Reference Azubuike and Okojie2008; Owoeye et al., Reference Owoeye, Aiyegbusi, Fapojuwo, Badru and Babalola2017). A prospective cohort study by Owoeye et al. (Reference Owoeye, Aiyegbusi, Fapojuwo, Badru and Babalola2017) investigated the prevalence of injury amongst semi-professional soccer players during a national tournament in Nigeria. Concussion was found to account for 3.0% and 10.0% of injuries in male and female soccer players, respectively, as well as 13.0% of all time-loss injuries.
Before researchers and clinicians can design appropriate interventions, there is a need to understand the current level of knowledge and attitude towards SRC within an under-studied group of soccer players (Provvidenza et al., Reference Provvidenza, Engebretsen, Tator, Kissick, McCrory, Sills and Johnston2013) as extrapolation from other populations such as the UK, America or New Zealand may be inappropriate (Broglio et al., Reference Broglio, Vagnozzi, Sabin, Signoretti, Tavazzi and Lazzarino2010; Kaut, DePompei, Kerr, & Congeni, Reference Kaut, DePompei, Kerr and Congeni2013; McCrea et al., Reference McCrea, Hammeke, Olsen, Leo and Guskiewicz2004) given the differences in various contextual factors (e.g., ethnicity, access to medical services) (Salmon et al., Reference Salmon, Mcgowan, Sullivan, Muphy, Walters, Whatman and Romanchuk2020). Furthermore, many of the surveys used in previous research possess poor psychometric qualities. Hence, the Rosenbaum Concussion Knowledge and Attitudes Survey (RoCKAS) was created for student athletes, coaches and medical personnel with the reliability and validity established (Rosenbaum & Arnett, Reference Rosenbaum and Arnett2010). The student athlete version has also recently undergone a slight modification to the SRC symptom checklist, thus enhancing the validity of this survey further.
The purpose of this study was to assess Nigerian footballers’ knowledge and attitudes surrounding concussions using a psychometrically appropriate survey as well as to determine associated contextual factors.
Methods
A cross-sectional study design was used to assess the knowledge and attitude of Nigerian footballers towards SRC. This design allowed for data to be gathered across a wide range of sub-populations engaging in football in Nigeria. Accordingly, several contextual factors such as age group, sex, level of education, playing experience, playing level, ethnicity and whether they had suffered a SRC previously were captured. Ethical approval for the study was granted by the Faculty of Health and Education Research Ethics Committee at Manchester Metropolitan University (number: 35654).
An estimation of the required sample size was completed using the Raosoft Sample Size calculator, and a sample size of ∼300 participants was deemed sufficient to give adequate precision of players’ concussion knowledge index (CKI) and concussion attitude index (CAI) using 95% confidence intervals. The response distribution was set at 50:50 as to not bias any perceptions of the responses, an estimated sample of over 20,000 was used, where thereafter, it makes minimal difference in the required sample, and the error was set at 5%.
An introduction letter was sent to Nigerian football clubs via their publicly available email addresses to gauge their interest and willingness to support this research. Those that agreed to support were provided with a link to the questionnaire, and were free to share this via any appropriate channel they chose (i.e., social media, newsletters, website) to potential participants. Consent was implied by participants completing the questionnaire. The use of an online questionnaire allowed for the publication on the World-Wide-Web, thus meaning individuals in Nigeria could complete the questionnaire despite it being a UK-based study. A pilot study was completed by selecting seven Nigerian footballers who were not part of the larger sample, and having them check the language and logic of the questionnaire before distributing it on a larger scale (Thabane et al., Reference Thabane, Ma, Chu, Cheng, Ismaila, Rios and Goldsmith2010). Following the completion of the pilot study, the questionnaire was made available online for eligible participants.
The inclusion criteria for participation included being affiliated to a football club that plays organised 11-aside football and is registered under the Nigeria football association. The players were required to be over the age of 18 years and have played organised football for a minimum of 12 months. Players were excluded if they were unable to read or write, unable to access the internet, or engaged in solely ‘non-official’ versions of the sport (e.g., 5-aside, 7-aside and walking football). The online survey was made available from August 2021 until December 2021 for any footballer who met the inclusion criteria.
Concussion knowledge and attitudes were measured using an amended version of the Rosenbaum Concussion Knowledge and Attitudes Survey student version (RoCKAS-ST) (Rosenbaum & Arnett, Reference Rosenbaum and Arnett2010). Permission was granted to use this tool by one of the authors of the RoCKAS-ST questionnaire. The RoCKAS-ST questionnaire was developed in an online format via JISC online survey. The questionnaire is made up of six sections. Section one collected information about the participants and history of SRC. Specifically, section one asked if participants have ever been diagnosed with a SRC, if they think they have had a SRC but were not diagnosed, and if they suspected a SRC but did not seek medical help. The same participant could select “Yes” or “No” to each of these questions. Section two and three examined the participant’s knowledge of concussion. This comprised of 21 true/false questions which included 4 distractor questions. Sections four and five consisted of 18 questions to assess attitude towards concussion, each in a Likert Scale format, ranging from “strongly disagree” to “strongly agree”. These were then used to classify participant’s responses as “safe”, “neutral” and “unsafe”. Section four had three distractor questions. Section six contains a checklist of eight common concussion symptoms and eight distracting symptoms. The 16 potential symptoms were based on previously published symptom studies and the distractors were seen to be more reasonable (abnormal sense of smell/taste, black eye and neck pain) than the original RoCKAS distractors (hair loss, excessive studying and arthritis) (Saunders, Burdette, Metzler, Joyner, & Buckley, Reference Saunders, Burdette, Metzler, Joyner and Buckley2013) as well as increasing the reliability and validity of this tool (Viljoen et al., Reference Viljoen, Schoeman, Brandt, Patricios and Van Rooyen2017).
CKI was derived by summing the scores across sections two, three and six. Correctly answered items received one point and incorrectly answered items received no points. Possible scores on the CKI ranged from 0 to 25 (Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). CAI was derived by totalling the scores from 15 questions across sections four and five. Possible scores on the CAI ranged from 15 to 75 (Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). The RoCKAS survey demonstrated fair to satisfactory test-retest reliability when assessed 2 days apart amongst students, with CKI and CAI scores having intraclass correlation coefficient (ICC) of 0.67 and 0.79, respectively (Rosenbaum & Arnett, Reference Rosenbaum and Arnett2010). The 16-item symptom recognition has a reliability of 0.89, an ICC of 0.88, and a Cronbach’s alpha of 0.83 (Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). An internal validity index consisting of three true/false questions in section two (15, 21 and 26) was added, and a score of <2 resulted in the test being considered invalid (Rosenbaum & Arnett, Reference Rosenbaum and Arnett2010). In such instances, these responses were removed. Levels of concussion knowledge and attitude were categorised as >80% very high, 60%–80% high, 40%–59% moderate, 20%–39% low, and <20% very low (O'Reilly et al., Reference O'Reilly, Mahon, Reid, Hume, Hardaker and Theadom2020).
Participant characteristics, with reference to sub-grouping, are presented as frequencies and percentages. CKI and CAI are presented as mean and standard deviation and as a percentage of the total possible score. The distribution of data for CKI and CAI as scale variables was checked using the Shaprio–Wilk statistic. As the data was not compatible with the assumptions of a normal distribution, the Spearman Rho correlation test was used, with r interpreted as trivial (<0.10), small (0.11–0.30), moderate (0.31–0.50), large (0.51–0.70), very large (0.71–0.90) and perfect (>0.90) (Hopkins, Reference Hopkins2002). The association between contextual factors (i.e., age group, sex, level of education, playing experience, playing level, ethnicity and previous SRC) and a high (≥60%) CKI and CAI were determined using a univariable and multivariable binary logistic regression. Sixty percent was chosen to represent “high” knowledge and attitude based on the work of O'Reilly et al. (Reference O'Reilly, Mahon, Reid, Hume, Hardaker and Theadom2020). Some individuals chose options such as “prefer not to say” or “other”, and these were excluded from the uni- and multivariable analysis, resulting in a sample of 281. Multicollinearity was assessed alongside the binary logistic regression with a value of 0.7 and above considered substantial multicollinearity. Finally, to aid in the readers interpretation of significance in the uni- and multi-variable regression, the proportion of the sample in each category were compared using a chi squared statistic. All analysis was conducted using SPSS (version 27; Statistical Packages for Social Sciences, Armonk, NY).
Results
In total, 331 participants completed the online survey reflecting 10 registered football clubs within Nigeria. All participants completed all sections to derive the CKI and CAI scores and passed the validity index (mean = 2.5 ± 0.5, range = 2–3). A summary of the frequencies can be found in Table 1.
Table 1. Participant characteristics
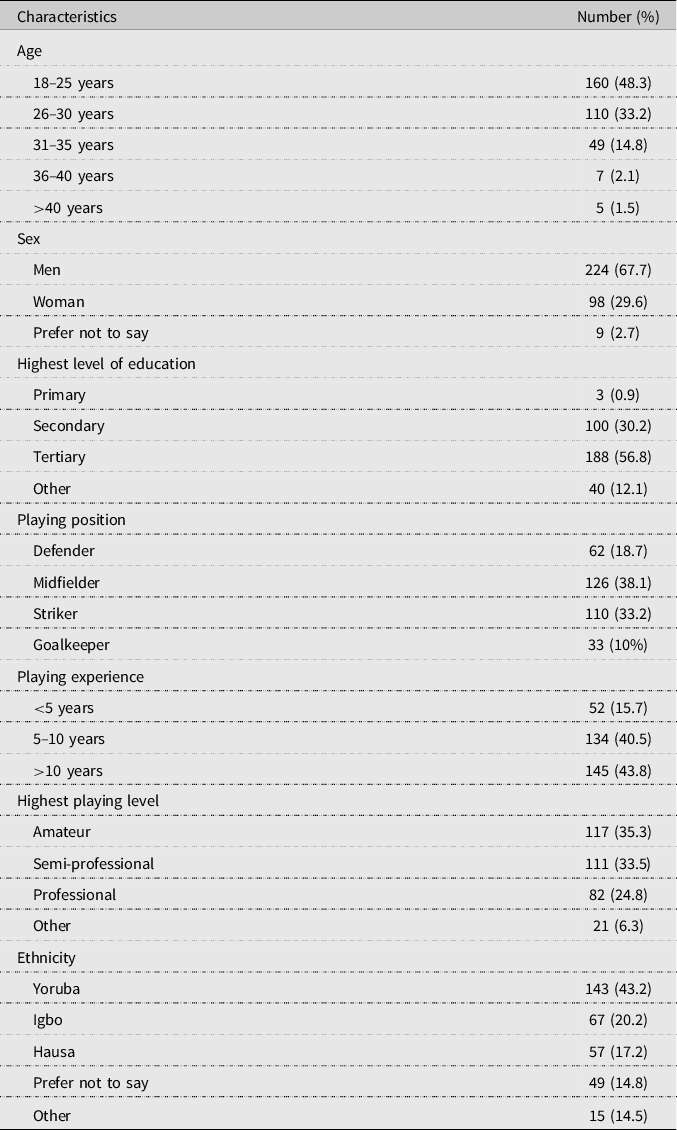
Note: Data presented as frequency and percentage.
A total of 25 (7.6%) participants reported being diagnosed with a SRC, whilst 40 (12.1%) suspected they had experienced a SRC, but it went undiagnosed. Thirty-three (10.6%) participants suspected a SRC but did not seek medical help. As these questions were independent, participants were able to provide an answer of “Yes” or “No” to each question. Ten participants (3.0%) answered “Yes” to being diagnosed previously and suspecting an undiagnosed SRC, whilst seven of these individual also answered “Yes” to being diagnosed previously and not seeking medical help in subsequent case. A total of 24 participants (7.3%) answered “Yes” to suspecting an undiagnosed SRC and not seeking medical help. Three individuals answered “Yes” to all three questions indicating they had been diagnosed with an SRC, suspected an SRC but it went undiagnosed, and did not seek medical help for a suspected SRC.
Mean CKI was 14.0 ± 3.0 (56.2 ± 13.2%) with a range of 6 (24.0%) to 22 (88.0%). The most common misconception about SRC was in reference to diagnostic scans whereas the most common correct answered referred to emotional changes being evident. A full breakdown for all 14 statements can be found in Figure 1.

Figure 1. Frequency and percentage of responses answering “true” to CKI statements.
In examining CKI, the following scenario was given to the participants: “While playing in a game, player Q and player X collide with each other, and both suffer a concussion. Player Q has never had a concussion in the past. Player X has had 4 concussions in the past”. When asked if player Q’s and X’s concussion will affect their long-term health and well-being, 197 (59.6%) and 230 (69.5%), respectively, answered “true” correctly. Using a second scenario of “Player F suffered a concussion in a game. He continued to play in the game despite the fact that he continued to feel the effects of the concussion”, 255 (77.0%) of participants correctly answered “False” when asked if player F’s performance will be the same as when he had not suffered a concussion. A summary of the correctly and incorrectly identified symptoms associated with SRC are presented in Figure 2.
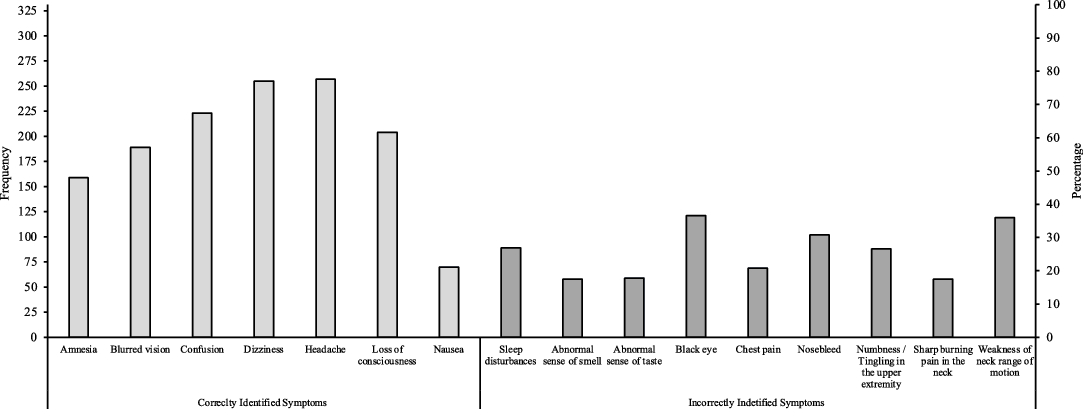
Figure 2. Frequency and percentage of responses identified correct and incorrect SRC symptoms.
Mean CAI was 54.5 ± 9.4 (72.6 ± 12.5%) with a range of 35 (47.0%) to 22 (100.0%). In evaluation of their attitudes, five questions were posed with the results presented in Figure 3.

Figure 3. Frequency and percentage of safe, neutral, and unsafe responses to CAI statements.
Participants were shown four scenarios to assess their CAI, which were as follow:
Scenario 1: Player R suffers a concussion during a game. Coach A decides to keep player R out of the game. Player R’s team loses the game.
Scenario 2: Athlete M suffered a concussion during the first game of the season. Athlete O suffered a concussion of the same severity during the semi-final playoff game. Both athletes had persisting symptoms.
Scenario 3: Athlete R suffered a concussion. Athlete R’s team has a physiotherapist on staff.
Scenario 4: Athlete H suffered a concussion and has a game in two hours. He is still experiencing symptoms of a concussion. However, athlete H knows that if he tells his coach about the symptoms, his coach will keep him out of the game.
Responses to the four scenarios indicated that most individuals gave a “safe” response with the exception of question 2 in scenario 2 where the highest proportion of “unsafe” responses was given. The greatest proportion (76.7%) of safe responses was observed for question 1, scenario 4. A full breakdown of the responses for each scenario is presented in Table 2.
Table 2. Responses to four scenarios to evaluate concussion attitudes
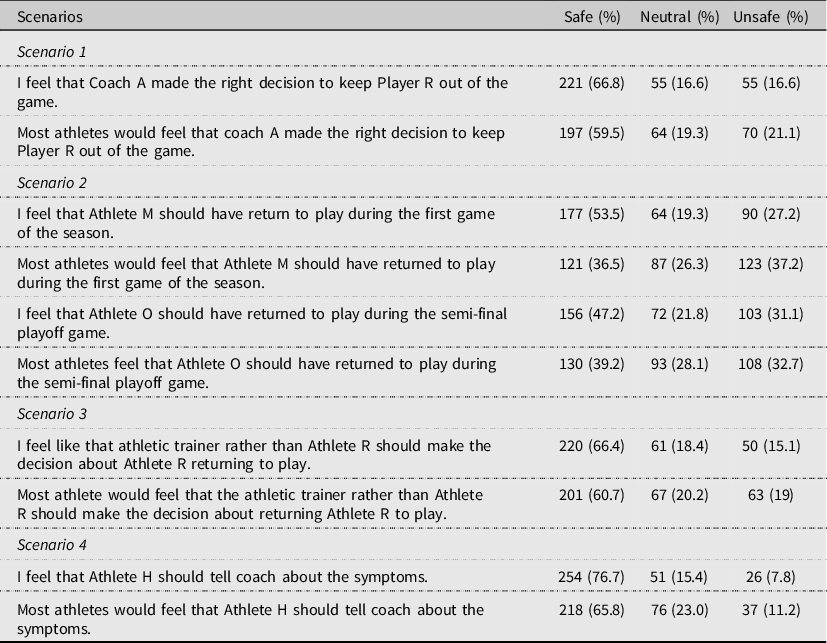
Note: Data presented as frequency and percentage.
The relationship between CKI and CAI indicated a large correlation (r = 0.530, P < 0.001), with 28% of the variance between scores explained. When considering CKI, the chi squared statistic indicated differences in the proportion represented for age (χ2 = 13.770, P = 0.008), sex (χ2 = 27.586, P < 0.001), playing experience (χ2 = 17.316, P < 0.001), ethnicity (χ2 = 23.062, P < 0.001) and those diagnosed with concussion (χ2 = 6.034, P < 0.014). For CAI, differences were observed for age (χ2 = 30.412, P < 0.001), sex (χ2 = 68.286, P < 0.001), playing position (χ2 = 11.701, P = 0.008), playing experience (χ2 = 31.471, P < 0.001), playing level (χ2 = 16.595, P < 0.001), and ethnicity (χ2 = 53.926, P < 0.001). Overall, there was little presence of multicollinearity with the minimum and maximum correlation values being 0 to −0.37 and 0.001 to −0.55 for CKI and CAI, respectively. Univariate logistic regression, based on 281 participants, revealed that sex, playing position (defender), playing experience and ethnicity were associated with a high CKI, however, only sex and playing experience remained in the full and final models. For these, the OR indicated that the odds of being classified with a “high” knowledge were 4.86 times greater for men, and 46%–63% lower odds for those with less than 10 years of playing experience (Table 3). For CAI, sex, playing position (defender) and playing experience (5–10 years) were associated with a “high” CAI at a univariable level. In addition, when considering the full model, semi-professional status was associated with 79% lower odds of being classified as “high” compared to professional status. In the final model, only sex remained to indicate an association, with men having 7.11 greater odds of being classified as having as a “high” CAI. Age, ethnicity, and previous history regarding SRC were not “significantly” associated with CKI or CAI in the full model (Table 4).
Table 3. Association between contextual information and the likelihood of scoring high on concussion knowledge index

Note: SRC – sport-related concussion. ***p < 0.001; **p < 0.01; *p < 0.05. OR = odds of falling in the high CKI group. Multivariable model included factors to determine the effect of each factor when fully adjusted. The final model included all factors that met the stopping criteria of p < 0.05 in both the univariate and multivariate model.
Table 4. Association between contextual information and the likelihood of scoring high on concussion attitude index

Note: SRC – sport-related concussion. ***p < 0.001; **p < 0.01; *p < 0.05. OR = odds of falling in the high CAI group. Multivariable model included factors to determine the effect of each factor when fully adjusted. The final model included all factors that met the stopping criteria of p < 0.05 in both the univariate and multivariate model.
Discussion
This study aimed to determine the CKI and CAI amongst Nigerian footballers as well as potential factors associated with being categorised as “high” CKI and CAI. We report a moderate CKI and high CAI, with a degree of shared covariance between these. Furthermore, we have shown that sex, playing position and playing experience are associated with greater or lesser odds of being considered “high” for CKI and/or CAI. The results of this study also suggest that age group, ethnicity and previous history of concussion (i.e., diagnosed or not; reported or not) was not associated with a higher CKI or CAI at an alpha level of 0.05.
In this study, 7.6% of participants reported being diagnosed with SRC which is lower than 23.4% and 29.9% recorded in high school and university football players, respectively (Delaney, Lacroix, Leclerc, & Johnston, Reference Delaney, Lacroix, Leclerc and Johnston2002; McCrea et al., Reference McCrea, Hammeke, Olsen, Leo and Guskiewicz2004). This was, however, similar to the 7.2% reported by Wallace et al. (Reference Wallace, Mulenga, Bretzin, Delfin, Muyinda, Sichizya and Mulenga2021) who studies the incidence of SRC amongst Zambian footballers. In total, 12.1% of respondents felt they might have had a SRC but did not receive a formal diagnosis, whilst 10.6% felt they might have had a SRC but did not seek medical help. Of those who reported being diagnosed with an SRC previously, most (7/10) also said they suspected another SRC, but no formal diagnosis was given. Similarly, most also stated that suspected another SRC but did not seek medical help. These findings support the notion that only a small proportion of SRCs are being diagnosed in Nigeria (McCrea et al., Reference McCrea, Hammeke, Olsen, Leo and Guskiewicz2004) and that the overall prevalence might be under-represented in this study as many do not receive a formal diagnosis or seek medical help.
The mean CKI in this study was found to be 56.2% which was less than those studies using English professional footballers (65.6%; Williams et al., Reference Williams, Langdon, McMillan and Buckley2016), Irish semi-professional and professional footballers (74.8%; Gallagher & Falvey, Reference Gallagher and Falvey2017), Canadian youth soccer players (78%; Doucette et al., Reference Doucette, Du Plessis, Webber, Whalen and Garcia-Barrera2021), amateur South African rugby players (75%; Viljoen et al., Reference Viljoen, Schoeman, Brandt, Patricios and Van Rooyen2017) and cyclists from all global regions (75.8%; Hurst, Novak, Cheung, & Atkins, Reference Hurst, Novak, Cheung and Atkins2019). The findings of inadequate awareness of concussion causes, diagnosis and sequelae in this population specifically may be indicative of the fact that concussion research and public knowledge translation has been primarily focused on developed countries (Eagles et al., Reference Eagles, Bradbury-Squires, Powell, Murphy, Campbell and Maroun2016). Educational programmes have mostly been targeted towards footballers in the Western World (Daneshvar et al., Reference Daneshvar, Yutsis, Baugh, Pea, Goldman, Grant and Sorcar2021). There are several factors that might help explain our findings. For example, contextual factors are best understood in a socio-ecological model, which is a systems-based public health model that covers the complex interplay of policy, organisational, interpersonal and intrapersonal levels of influence on a health state and related behaviours (Register-Mihalik et al., Reference Register-Mihalik, Williams, Marshall, Linnan, Mihalik, Guskiewicz and McLeod2018). Firstly, considering policy in the United Kingdom as an example, the Football Association introduced rules that meant any player who sustains a suspected concussion should immediately be removed from the pitch and are unable to return until the appropriate assessment or treatment has been administered (Smith, Reference Smith2016). This kind of policy influences players’ knowledge indirectly, and no such policy exists in Nigerian Football (a non-FIFA competition) in which this study was conducted. Furthermore, unfavourable economic conditions in developing countries like Nigeria, as well as policy that prioritises other high-priority health issues e.g., malaria and HIV (Muhammad, Abdulkareem, & Chowdhury, Reference Muhammad, Abdulkareem and Chowdhury2017), could affect public awareness of concussion. Factors such as sex, playing experience, and playing position can influence the knowledge and attitude of an athlete, which our findings reinforce at a univariable level. Furthermore, ethnicity appeared to be associated with knowledge at a univariate level for the Hausa tribe, with this tribe having a lower knowledge index compared to other tribes. This could be because the Hausa tribe ranks lowest in literacy levels amongst the major tribes in Nigeria (Smith, Reference Smith2021) and traditionally live in small villages, so may reflect less exposure to outputs (e.g., written media about SRC) than others. Also, knowledge and safe attitudes have been found to be influenced by coaches, teammates, and parents’ education (Chrisman, Quitiquit, & Rivara, Reference Chrisman, Quitiquit and Rivara2013; Kraak et al., Reference Kraak, Bernardo, Gouws, Loubser, Vuuren and Coetzee2018), though in this study, their own education appeared to have minimal influence on CKI and CAI.
The most common misconception around knowledge amongst participants was that ‘after a concussion occurs, brain imaging typically shows visible physical damage to the brain’ which was incorrectly answered as “true” by 75.2% of participants. This misconception was similarly high among South African rugby players (Viljoen et al., Reference Viljoen, Schoeman, Brandt, Patricios and Van Rooyen2017). Further, in a mixed-methods study by Williams et al. (Reference Williams, Langdon, McMillan and Buckley2016), this accounted for the second most common misconception on a quantitative survey. However, despite thinking that concussion can be associated with bleeding in the brain, they still expressed during the interview that they felt it was not as serious as a leg break suggesting some degree of ‘downplaying the severity’ of concussion because concussion symptoms are often mild and non-visible. Another misconception was that ‘concussion can only occur if there is a direct hit to the head’, with 61.6% incorrectly answering “true”. A similar finding was found among junior (37%) and amateur rugby players (43%) (Viljoen et al., Reference Viljoen, Schoeman, Brandt, Patricios and Van Rooyen2017). This misconception highlights the need for the proper education for football (soccer) players on the causes, possible mechanism of SRC, and sequelae as the respondent’s understanding of these was inadequate.
The most recognised symptoms were headache, dizziness, and confusion. Similar patterns of responses were seen amongst high school and English footballers (Cournoyer & Tripp, Reference Cournoyer and Tripp2014; Williams et al., Reference Williams, Langdon, McMillan and Buckley2016), though they were identified by over 90% of participants in these studies compared to 67%–78% in this study. This small differences might be due to the growing publicity around SRC in the Western World (O’Reilly et al., Reference O'Reilly, Mahon, Reid, Hume, Hardaker and Theadom2020). It should also be noted that the previous studies had a smaller sample compared to this study. Nausea (21.1%), sleeping problems (26.9%), and amnesia (48%) were the least identified symptoms which were consistent with previous findings in football and rugby (Broglio et al., Reference Broglio, Vagnozzi, Sabin, Signoretti, Tavazzi and Lazzarino2010; Kraak et al., Reference Kraak, Bernardo, Gouws, Loubser, Vuuren and Coetzee2018). In addition, there was a misunderstanding between the symptoms of a concussion and those of a more severe brain or neurological injury, with 30.8% and 36.6% of respondents identifying bleeding nose and black eye, respectively, as symptoms of concussion. It is critical that footballers understand the differences between concussion and symptoms of severe brain injury to be able to seek the most appropriate medical care and allow for a degree of identification of SRC symptoms in themselves and others. Overall, these findings imply that, despite continued misunderstandings, most Nigerian footballers have a moderate understanding of SRC and can recognise some of the concussion symptoms. These misconceptions can be addressed via a targeted concussion education programme.
Participants in this study reported a mean CAI score of 72.6%, which was similar to studies in English football (79.5%; Williams et al., Reference Williams, Langdon, McMillan and Buckley2016), Irish footballers (80.4%; Gallagher & Falvey, Reference Gallagher and Falvey2017), Canadian junior soccer players (85.5%; Doucette et al., Reference Doucette, Du Plessis, Webber, Whalen and Garcia-Barrera2021), and high school athletes (79.9%; Register-Mihalik et al., Reference Register-Mihalik, Linnan, Marshall, Valovich-McLeod, Mueller and Guskiewicz2013b). Respondents indicated conservative attitudes on the survey by providing safer responses on 14 out of 15 questions. For example, most respondents stated that footballers should inform their manager of suspected concussion even if it means removal from play (76.7%). Respondents also felt coaches need to be cautious when determining whether an athlete should return to play (71.9%), and that an athlete who is unconscious should be taken promptly to an accident and emergency department (68.3%). Two-thirds of participants (66.4%) felt that physiotherapist should be responsible for a return-to-play following a concussive episode. These findings show that most players know the role coaches and medical personnel play in identifying and managing concussion. Similar findings were found when a questionnaire was administered to English footballers (Williams et al., Reference Williams, Langdon, McMillan and Buckley2016). However, also in agreement with Williams et al. (Reference Williams, Langdon, McMillan and Buckley2016), 25.7% of respondents in this study felt concussions are not as important as other injuries and 33 participants suspected an SRC but did not seek help. This not only highlights the potential knowledge gap, but also a somewhat dismissive attitude, meaning footballers might not be aware of how severe concussion can be both in the short- and long-term. Furthermore, 15.7% and 21.8% of respondents reported an unsafe or neutral response when asked if they would return-to-play when experiencing a headache because of an SRC. This decision may be influenced by the fact that respondents may want to return to a game because of their competitiveness or the perceived importance of the game as evidenced by the 23.9% who reported an unsafe response regarding responsivity to return. This finding is not unique. Indeed, FIFA reported that 96% of players who were interviewed indicated that match importance influenced their decision to play or not when experiencing symptoms associated with concussion (Football IFOA, 2013). Doucette et al. (Reference Doucette, Du Plessis, Webber, Whalen and Garcia-Barrera2021) also demonstrated that competitiveness was positively associated with past non-disclosure or the intention of non-disclosure (OR 1.02–1.05) of an SRC in Canadian youth soccer players.
There was a relationship between CKI and CAI that reflected 28% shared covariance. This was found to be higher than a study amongst South African rugby players (Kraak et al., Reference Kraak, Bernardo, Gouws, Loubser, Vuuren and Coetzee2018), and suggests that educational interventions targeted at concussion knowledge could invariably help improve attitudes towards SRC amongst Nigerian footballers. The purpose of educational interventions is likely to be twofold: to increase people’s concussion knowledge and, more crucially, to modify people’s behaviour by encouraging them to report self-suspected concussions, seek medical help, and follow the guidance given (Kroshus, Daneshvar, Baugh, Nowinski & Cantu, Reference Kroshus, Daneshvar, Baugh, Nowinski and Cantu2014). However, such approaches should also consider the results from our regression analysis which highlighted that further education and attitude modification may be required for women, specific playing positions, and those with fewer years of playing experience.
Whilst this study provides valuable insight in the CKI and CAI in a population previously not reported upon, there are some limitations worthy of mention. Firstly, this study was cross-sectional in design and relied upon self-reported details and accounts of SRC. As such, we are unable to verify the true accuracy of the details provided despite the approach used (anonymous, online questionnaire) or if socially desirable results were given. Further, whilst a relatively large sample was used, for some sub-groups, the relatively small numbers did impact our statistical power and analysis (e.g., influence of age and ethnicity of CAI) meaning some associations might have gone undetected or the confidence intervals are wider than desired.
Overall, the results of this study highlight that those involved in Nigerian football have moderate knowledge, but generally good attitudes towards SRC, agreeing with previous literature in non-African countries. Furthermore, our results suggest that changes in knowledge might increase the attitudes towards concussion, and that an initiative to promote knowledge should consider the association with sex, playing position and playing experience. Our results indicate that, in Nigeria, further work is needed to educate footballers on all aspects of SRC especially in females and those with fewer years of football experience.
Acknowledgements
The authors would like to thank all the participants who completed the online questionnaire and gatekeepers who provided access.
Author contributions
OO and ND were involved in the conceptualisation, data collection, ethics submission, data analysis and implementation of the methodology. OO and ND wrote the draft manuscript which was read and edited by HR and ND. ND revised the article. All authors approved the final manuscript and any revisions.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. This project was approved by the Faculty of Health and Education Research Ethics Committee, Manchester Metropolitan University, UK. The approval number for the project is 35654.








 Open access
Open access