



According to the WHO, between 1975 and 2016, the prevalence of overweight/obesity in children and adolescents, aged 5–19 years, increased from 4 % to over 18 %, worldwide. In 2016, more than 124 million children and adolescents (6 % females and 8 % males) were obese(1). In Brazil, data collected in a national sample between 2008 and 2009 indicate that 37·2 % and 21·6 % of adolescents aged 10–11 and 14–15 years, respectively, were overweight/obese(2). A more recent evaluation carried out in the year 2015, with schoolchildren aged 13 to 15 years, revealed 25·1 % of overweight/obesity(3).
Overweight or obese children and adolescents tend to present dissatisfaction with their bodies because of their desire to attain a different body shape. This body perception is a multidimensional and complex manifestation that involves cognitive, affective, social, cultural and motor aspects, including sports competence, physical condition, appearance and physical strength(Reference Martin4).
Dissatisfaction with body image (BI) can be influenced by several factors, including the media(Reference Fortes, Filgueiras and Oliveira5,Reference Shah, Das and Muthiah6) . It is increasingly frequent among adolescents to achieve a body shape closer to the standards created by society, in the search for an appearance considered socially appropriate(Reference Frank, Claumann and Felden7,Reference Mallick, Ray and Mukhopadhyay8) .
BI dissatisfaction since early adolescence can lead to weight control behaviours(Reference Fortes, Almeida and Cipriani9) that can range from healthier behaviours, such as moderate dieting and exercise, to potentially harmful behaviours, such as purging, laxative use, diet pill use and skipping meals(Reference Boutelle, Neumark-Sztainer and Story10,Reference da Silva, Barufaldi and Andrade11) . Teenagers’ reasons for dieting are varied, but BI dissatisfaction and a desire to be slimmer is the motivating factor for the majority(12).
A study conducted in the city of Florianópolis (Southern Brazil) found that the lifestyle adopted by children and adolescents is unhealthy, since they rather skip meals and consume sweetened beverages and food rich in sugar, Na and fat more than three times a day; skipping meals is a practice predominantly associated with overweight/obesity conditions.(Reference D’Ávila, Silva and Vasconcelos13) These habits could make it difficult to maintain adequate body composition(Reference D’Ávila, Müller and Gonsalez14), in addition to the fact that adolescence is a life cycle marked by major bodily, psychological and social transformations(Reference Frank, Claumann and Felden7), including changes in body shape and size, physical appearance, and interaction with peers in social groups and life preferences(Reference Boutelle, Neumark-Sztainer and Story10). Due to these transformations, adolescents are more vulnerable to pressures imposed by society, family, friends and the media, in order to achieve the perfect body, as a way to obtain acceptance and social success(Reference Frank, Claumann and Felden7).
In another study carried out in the city of Florianópolis with students aged 7 to 10 years, it was observed that dissatisfaction with BI occurred in 82·9 % of students, in which 59·9 % wanted to have a smaller body size and 23·0 % wanted to have a larger body size(Reference Costa, Alvarenga and Vasconcelos15). In the search for a body that is believed to be the ideal, dissatisfied adolescents enrolled in the first years of high school in the metropolitan region of Rio de Janeiro showed more chances of skipping the main meals(Reference Carvalho, Nunes and Moraes16). Weight control practices in adolescence increase the chances of developing eating disorders, and consequently, studying the practice of purgative behaviours facilitates the identification of this condition at an early stage, enabling adequate treatment and prevention of health complications(Reference Dell’Osbel, Donatti and Henn17). Therefore, it is important to explore the weight control strategies used by overweight adolescents given the high percentages of overweight individuals in this group, the high frequency of body dissatisfaction found in Brazilian studies (from 26 to 77 %)(Reference Carvalho, Nunes and Moraes16,Reference Souza-Kaneshima, França and Kneube18–Reference Dell’Osbel, Donatti and Henn22) and the consequences that inadequate weight reduction practices can cause in the short and long term.
This study aimed to investigate the association of overweight/obesity and the presence of purgative behaviours with BI in adolescents, aged 11–14 years, in the city of Florianópolis/SC, Brazil. Our hypothesis was: body dissatisfaction and purgative behaviours are prevalent among girls, and body dissatisfaction with BI is associated both with overweight/obesity and with some of the purgative behaviours related to body weight control.
Materials and methods
This is a cross-sectional study nested within a broader investigation which general objective was to review the trend in the prevalence of overweight/obesity and associated factors in schoolchildren, aged 7 to 14 years, based on the comparison of data obtained at three investigation time points: 2002, 2007 and 2012/2013(Reference D’Ávila, Silva and Vasconcelos13–Reference Costa, Alvarenga and Vasconcelos15,Reference Rossi, Hinning and Corrêa24–27) . In this article, BI and anthropometric data were reviewed, as well as behaviour of students in relation to purgative trends for weight control and binge eating, collected in the third wave (2012/2013)(Reference D’Ávila, Silva and Vasconcelos13,Reference Costa, Alvarenga and Vasconcelos15,Reference Bernardo, Fernandes and Campos23–Reference Wagner, Fragas and Rossi26) . Because data on purging behaviours for weight control and overeating were collected only in the third wave of the study, cross-sectional analysis was performed in this work.
The study sample was taken from a population of 26·075 students, of both sexes, aged 11–14 years (adolescents), regularly enrolled in elementary education in eighty-five public and private schools, in the morning and afternoon shifts, in the city of Florianópolis (Santa Catarina), in 2010. The sample size was calculated based on the following parameters: expected prevalence of 38 % overweight/obesity, 5 % sampling error, 95 % CI, design effect of 1·8 and loss percentage of 10 %, resulting in a required sample size of 707 students.
The sampling process was carried out by conglomerates, having as primary sampling units eighty-five schools in the municipality that had all grades classes elementary school (from first to ninth grade), in the daytime period. To ensure sample variability in the schools’ selection, the schools were initially divided into ten strata, according to the administrative regions of the city of Florianópolis (Downtown, Continent, North, East and South) and the type of school (public or private). In each stratum, the schools included in the study were randomly selected, by simple drawing. Subsequently, the selection of classes to be evaluated in each school was carried out, through a systematic sampling process, based on the list of students available in each school(Reference D’Ávila, Silva and Vasconcelos13,Reference Costa, Alvarenga and Vasconcelos15,Reference Bernardo, Fernandes and Campos23–Reference Wagner, Fragas and Rossi26) .
Data collection and procedures
Data collection was carried out between September 2012 and June 2013, with the completion of the anthropometric assessment and the obtainment of sociodemographic and BI data. Prior to data collection, the team was trained and a pilot study was carried out, for field practice. The data collection team was composed of undergraduate students in Nutrition and Physical Education from the Universidade Federal de Santa Catarina and the Universidade Estadual de Santa Catarina(Reference D’Ávila, Silva and Vasconcelos13,Reference Costa, Alvarenga and Vasconcelos15,Reference Bernardo, Fernandes and Campos23–Reference Wagner, Fragas and Rossi26) .
Anthropometric measurements of body mass (in kilograms) and height (in meters) were performed according to the procedures recommended in the literature(27). The measurement of body mass was obtained using a Marte®, electronic scale model LC200-PP, with 200 kg maximum capacity and 50 g sensitivity. For the procedure, the students had to wear light clothes, be barefoot, in the orthostatic position (standing and body erect), with the weight distributed between the lower limbs, arms loose at the sides, shoulders relaxed and keeping the head in the Frankfurt plane (plane for cephalic orientation, in which the individual remains still with his eyes on the horizon).
Height was obtained using an Alturexata® stadiometer, with zero point at ground level and 0·5 cm scale. Adolescents were instructed to remain in the standing position, barefoot and feet together, with heels, buttocks and head in contact with the stadiometer, head in the Frankfurt plane, arms loosely lateral to the body and shoulders relaxed. In addition, the evaluated student was asked to take a deep breath, to reduce the effect of daily gravitational compression. With these data, the BMI in kg/m2 was calculated. The diagnosis of overweight and obesity in schoolchildren was defined based on the BMI curves for age and sex, according to a WHO(Reference Kakeshita29), considering overweight/obesity when the BMI ≥ z-score +1.
Data related to BI were obtained through the Brazilian Silhouette Scale, developed and validated by Kakeshita(Reference De Onis, Onyango and Borghi28). The Silhouette Scale is based on a set of eleven figures stamped on individual cards for each sex, with dimensions of 12·5 cm × 6·5 cm, lined on the back. Each silhouette corresponds to an actual BMI range for subject classification purposes and a set mean BMI for calculation purposes. The first silhouette represents an adolescent with BMI 12 kg/m2 and the last a child or adolescent with BMI 29 kg/m². For each figure, there is a constant increment of 1·7 kg/m².
In order to illustrate the silhouettes, the authors considered the average height of the Brazilian population at 10 years of age, 140·15 cm for males and 141·25 cm for females. The scale proved to be reliable and satisfactory, ranging from 0·50 to 0·84 on the male scale and 0·67 to 0·73 on the female scale for the optimal and desired body for both sexes. The cards with the drawn silhouettes were presented face up, in ordered series, and the figures were scaled up from left to right. The interviewers asked each student to indicate the figure that represented the body most similar to their own and then, which figure they would like to look like (‘desired figure’). The presence of dissatisfaction with BI was obtained by subtracting the values referring to the figure of the body and the figure of the body they would like to have. Based on this calculation, the student was classified as satisfied (result = 0), dissatisfied when desiring to expand the silhouette (negative values) and dissatisfied when desiring to reduce the silhouette (positive values)(Reference De Onis, Onyango and Borghi28).
In order to assess the students’ eating behaviours in connection with purgative initiatives for weight control and binge eating, a questionnaire was applied with questions that characterized the absence or presence, and frequency of adoption of purgative methods, such as use of laxatives and diuretics, reduced food intake or no eating (with the objective of not gaining weight or losing weight), and induced vomiting to eliminate the ingested food, during the 3 previous months. Questions about the use of laxatives and diuretics were accompanied by a short explanation about its effects on health, as follows: diuretics (medications that induce the person to urinate excessively) and laxatives (medications that induce diarrhoea). It was also asked whether the adolescent had episodes of ingesting large amounts of food in a short period of time, during the last 3 months, accompanied by a feeling of loss of control over what or how much they had eaten. These questions contained four response options: (a) none, (b) less than once a week, (c) once a week, and (d) twice or more times a week. The variables were dichotomised, considering ‘yes’ for the use of each practice if the student answered ‘b, c or d’, and considering ‘no’ for the use of the practice if the answer was ‘a’. The questions were based on a previous study carried out by Ferreira and Veiga (2008)(Reference Kakeshita29).
Food consumption was assessed using the Previous Day’s Food Intake Questionnaire (PDFQ-3), which is characterised as a 24-h recall-type questionnaire. In PDFQ-3, all the six meals are ordered chronologically (breakfast, morning snack, lunch, afternoon snack, dinner and evening snack)(Reference Ferreira and Veiga30). Using this questionnaire, two variables were constructed: consumption of fruits and vegetables (FV) and number of daily meals. The determination of the adequate consumption of FV and number of daily meals was performed as follows: it was considered adequate when intake of FV was equal or greater than five servings per d and inadequate if it was less than five servings per d(Reference Assis, Benedet and Kerpel31,32) ; number of daily meals is considered adequate when three or more meals are eaten per d; and intake of less than three meals was considered inadequate(33).
Physical activity levels were assessed using a questionnaire(34,Reference Cabral, Costa and Liparotti35) which asked if the adolescents had practiced (or not) eleven different types of physical activities within the last day, including: dancing, walking/running, biking, housework, climbing stairs, soccer, jumping rope, swimming, gymnastics, skateboarding and playing with the dog. Adolescents were also asked about the intensity level of physical activity (slow, fast and very fast). The general level of activity was determined by adding the scores of the activities that the student reported performing. Three different weights were assigned as a way of considering the activities indicated by the student: weight one for light-intensity activities (slow), weight three for moderate-intensity activities (fast) and weight nine for vigorous-intensity activities (very fast), according to previous studies(Reference D’Ávila, Silva and Vasconcelos13,34,Reference Cabral, Costa and Liparotti35) . This variable was used in continuous form in the models.
Data on sex, date of birth, school grade and shift taken by the adolescents were retrieved directly in the schools, through the students’ enrollment forms. Data regarding parents’ education and monthly family income were obtained through a questionnaire filled out by the parents, delivered together with the consent form.
Statistical analysis
To characterise the sample, the variable education system was dichotomised into public v. private, and mother and father level of education was categorised into: no education/incomplete primary education, complete primary education, complete secondary education and complete higher education.
STATA software (Statistical Software for Professionals, Texas) version 14.0 was used for descriptive and inferential analyses. The study design and sampling plan were considered in the analysis using the svy weighting command. Association analyses were performed using Pearson’s χ 2 test of heterogeneity (bivariate analysis for comparison between groups), and multivariate logistic regression, controlled by age (in whole years – continuous variable), sex, type of school (as a proxy to family income) intake of FV, food intake (daily meals) and physical activity level (continuous form), to obtain the OR and 95 % CI, for comparison of odds among adolescents presenting v. not presenting the outcomes.
The dichotomous variables overweight/obesity, overeating, not eating, use of laxatives, vomiting induction and use of diuretics were evaluated as outcomes, while satisfaction with BI (polytomic) was tested as an independent variable in each model of analysis.
The significance level adopted for the hypothesis tests, considering the occurrence of type I error, was 5 %, rejecting the null hypotheses once the p value was lower than the type I error value.
Ethical considerations
This study was carried out in accordance with the guidelines established in the Declaration of Helsinki, and all procedures involving humans were approved by the Ethics Committee for Research with Humans of the Universidade Federal de Santa Catarina/CCS (Consubstantiated Opinion nº 120·341/2012).
Approval from the municipal entity was also obtained. The study only includes students who signed the informed consent form, which was also signed by their parents. Adolescents with difficulties on communication skills or whose BMI could not be assessed were not included in the sample.
Results
A total of 976 adolescents aged 11–14 years were evaluated; the majority of the sample was composed of females (n 531; 59·0 %). Almost a third of the adolescents reported mothers with university degree and over 1/4 of the fathers were reported as having the same level of education. The sample was composed by a majority of adolescents enrolled in public schools (67·8 %). Regarding BMI assessment, 29·0 % of the individuals were overweight/obese, and 77·0 % of the adolescents were dissatisfied with their BI (31·9 % wanted to expand their silhouette and 45·3 % wanted to reduce it). There was no statistically significantly difference between sexes and BI dissatisfaction (Table 1).
Table 1. Characterisation of adolescents’ sample in the city of Florianópolis, 2012/2013
(Number and percentages)

* Variables with unanswered data (losses).
** Pearson’s χ 2 for differences in the prevalence of overweight/obesity between sexes: P = 0.221.
*** Pearson’s χ 2 for differences in the prevalence of satisfaction with body image between sexes: P = 0.692.
Regarding the presence of purgative or fasting behaviours besides no statistical significant differences, it was observed that the younger the adolescent the higher the prevalence of the use of purgative methods for weight control, while the older the adolescent the higher the habit of fasting and the perception of overeating as compared with the younger individuals (Table 2).
Table 2. Purgative behaviours, overeating and not eating in adolescents, according to sex, age, and anthropometric status, in the city of Florianópolis, 2012/2013
(Number and percentages)
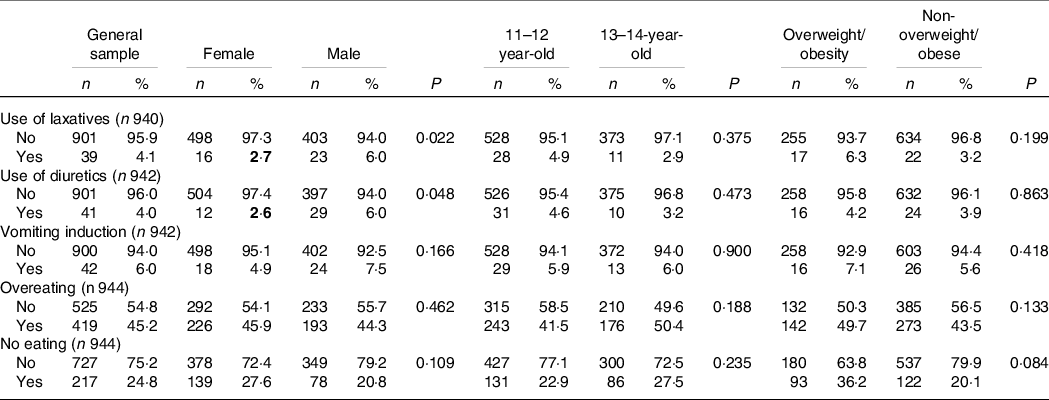
It was also observed that almost half of the overweight/obese adolescents reported that they ‘overeat’ and 36·1 % ‘do not eat’. The ‘use of laxatives’ and ‘diuretics’ are methods that have been indicated to be more used by males when compared with females (P = 0·022; P = 0·048, respectively). Among adolescents without overweight/obesity, 20·8 % of them reported ‘no eating’, in order to attempt to control their weight (Table 2).
We clarify that a logistic regression analysis was performed only with those who present purgative behaviours – use of laxatives, use of diuretic and vomiting (n 82). There were no statistical differences in BI satisfaction and dissatisfaction between adolescents who had only one purgative behaviour (n 52) and those who had more than one purgative behaviour (n 30) (data not shown).
The entire sample reported some level of physical activity, the scores ranged from 1 to 64, but no statistical differences were observed between adolescents satisfied or dissatisfied with their BI, as well as food intake regarding FV and number of daily meals (data not shown).
Among the overweight/obese adolescents, 9·6 % were satisfied with their bodies, and the majority wanted to reduce their silhouette. Among adolescents without overweight/obesity, the prevalence of satisfaction increases; however, 45·4 % of these adolescents also wanted to increase their silhouette and 26·0 % wanted to reduce it. There was a significant difference between the prevalence of non-overweight/obese and overweight/obese adolescents who were satisfied with their BI and who wanted to increase or reduce their silhouette (P < 0·001) (Table 3).
Table 3. Food intake, consumption of fruits and vegetables, purgative behaviours, overeating and not eating and overweight/obesity in adolescents aged 11–14 years, according to satisfaction or dissatisfaction with body image, in the city of Florianópolis, 2012/2013
(Number and percentages)

OW, overweight; OB, obesity.
Among those who wanted to reduce their silhouette, the majority used ‘vomiting induction’ (P = 0·039) as a method for weight control, followed by ‘use of laxatives’ (P = 0·014) and ‘no eating’ (P = 0·025) as a method for weight control. Overeating was also significantly higher among the group that wanted to reduce body size (P = 0·019) (Table 3).
The multivariate association between overweight/obesity and BI revealed that the OR for the outcome overweight/obesity is higher among adolescents who wanted to reduce their silhouette (OR = 11·20; CI = 5·55, 22·58). The association of weight control methods with BI, on the other hand, reveals higher OR for the ‘use of diuretics’ among adolescents dissatisfied with their BI, with the chance of ‘using diuretics’ being three times greater among those adolescents who wanted to reduce their silhouette (OR = 3·08; CI = 1·78, 5·32). The odds of using laxatives was higher among those who wanted to reduce their silhouette (OR = 2·10; CI = 1·20, 3·68). ‘Overeating’ is used both by adolescents who want to increase their silhouette (OR = 1·78; IC = 1·12–2·85) and by those who want to reduce it (OR = 1·81; IC = 1·03–3·19) (Table 4).
Table 4. Overweight/obesity, purgative behaviours, overeating and not eating and their association with body image dissatisfaction in adolescents, aged 11–14 years, Florianópolis, 2012/2013 (Odd ratio and 95 % confidence intervals)

* Outcomes: overweight/obesity and each of the purgative behaviour variables; independent variables: satisfaction with body image in each model. The models were controlled for age, sex, type of school (public or private), intake of fruit and vegetables, food intake (number of daily meals) and physical activity level (scores).
Discussion
Our initial hypothesis that body dissatisfaction and purgative behaviours were higher among girls was not confirmed in the bivariate analysis, because the use of laxatives and diuretics was higher among boys and body dissatisfaction did not differ between sexes. However, we have confirmed the hypothesis that dissatisfaction with the BI (want to reduce their silhouette) is associated both with overweight/obesity and some of the purgative behaviours, such as using diuretics and laxatives. Additionally, ‘overeating’ is associated with BI in adolescents who want to increase their silhouette and in those who want to reduce it.
Despite being high, the prevalence of BI dissatisfaction among adolescents in Florianópolis is in line with the trend of high frequency of body dissatisfaction among adolescents regardless of the evaluation method. Among adolescents in Rio de Janeiro, 41·4 % wanted a slimmer silhouette and 33·7 % wanted a bigger silhouette, that is, 75·1 % were dissatisfied and reported their desire to have a different silhouette from the one in which they perceived themselves(Reference Barros, Assis and Pires36). Moehlecke et al. carried out a study with a probabilistic sample of national representation with 71·740 Brazilian adolescents aged 12 to 17 years; when questioned how they felt about their BI, 45 % of the adolescents answered they were not satisfied(Reference Moehlecke, Blume and Cureau21).
Dissatisfaction with BI, in general, is high in different age groups in Brazil. According to Laus et al (2014)(Reference Justino, Enes and Nucci37), in Brazil, the body plays a fundamental role in people’s lives to achieve social ascension and develop successful relationships.
But, in addition to this context, the dissatisfaction is more evident in adolescents because adolescence is a period marked by important physical and social changes that can lead to a negative BI(Reference Laus, Kakeshita and Costa38) which makes them more vulnerable to pressures imposed by society, family, friends and the media to reach the perfect body as a way of obtaining acceptance and social success(Reference Senín-Calderón, Rodríguez-Testal and Perona-Garcelán39). Internalisation of the ideal of beauty by sociocultural influences and social comparison facilitate development of a negative BI and unhappiness with appearance(Reference Frois, Moreira and Stengel40,Reference Carey, Donaghue and Broderick41) .
In the present study, no statistically significant values were obtained when comparing BI dissatisfaction between sexes. However, we observed among males, from Florianópolis, larger ‘use of laxatives and diuretics’ in comparison with females. The results of the National Adolescent Health Survey (PeNSE) collected in 2015, evaluating a national sample of adolescents in Brazilian capitals, revealed that 7·0 % of students in the ninth year of elementary school in the country reported having induced vomiting or taken laxatives in the last 30 d, as a means of losing weight or avoiding gaining weight. The assessment by sex shows that among boys, this rate was 6·5 % and among girls, 7·5 %. This trend is reversed in some states of the country. The practice of ingesting medication, formulas or some product to lose weight, without medical supervision, was more common in the country, among boys (6·8 %) than among girls (5·2 %). However, among students who wanted to gain weight or muscle mass, the use of medication, formula or another product was higher among boys (8·6 %) compared with girls (5·6 %)(3). These findings demonstrate that both females and males need to be protected against harmful information regarding the use of purgative methods for weight control in Brazil.
Regarding purgative behaviours, in the multivariate analysis, only the use of laxatives and diuretics remained associated with BI dissatisfaction. Laxatives and diuretics are medications often inappropriately used to rid the body of energy content. They result in weight loss simply by eliminating water weight, which can cause dehydration(Reference Rao, Zong and Zhang42). Scientific evidence has reported that abusive use of these drugs can also lead to elevated serum levels of aldosterone and vasopressors, melanosis coli, cathartic colon, and functional impairment, cardiac arrhythmias, and electrolyte disturbances(Reference Mahoney43).
Extreme concern with weight and BI can lead the individual to behavioural change such as eating restrictions or use of purgatives, such as self-induced vomits, use of laxatives and diuretics. In our study, students dissatisfied with their bodies, who wanted to lose weight, performed purgative practices two (use of laxatives) to three (use of diuretics) times more than the rates presented for students who were satisfied with the BI. These purgative practices can correspond to partial manifestations that can evolve into full frames of eating disorders, what alerts parents and physicians for the importance of early identification of such manifestations.
Body dissatisfaction is considered a risk factor shared by obesity and eating disorders. In a systematic review study, Shagar et al. (Reference Mehler and Rylander44) found a positive association between BI concerns and weight-related behaviours of adolescents and emerging adults. Their study identified that higher body dissatisfaction had a significant association in the development of eating disorders and extreme weight-loss behaviors.
Also in the multivariate analysis, episodes of overeating were associated with both adolescents wanting to increase their silhouette as well as wanting to reduce their silhouette. This result shows that an undesirable eating behaviour, such as compulsive eating, can develop not only in obese people or those who wish to lose weight but also in those who seek to increase their body size. This alerts us to the importance of promoting satisfaction with BI among adolescents, regardless of their weight status.
Finally, in the multivariate analysis, BI dissatisfaction (desire for a smaller body size) remained strongly associated with overweight/obesity in the present study. This result corroborates with other studies, which indicate that adolescents with overweight or obesity are prone to develop BI dissatisfaction, like this other psychological co-morbidities, including emotional and behavioural disorders, anxiety, and low self-esteem(Reference Shagar, Harris and Boddy45–Reference Alsaleem47).
In the systematic review conducted by Jiménez-Flores et al. (Reference Alsaleem47), which evaluated sixteen cross-sectional studies with children and adolescents, aged 5–19 years, in countries such as the UK, Italy, Brazil, Germany, Hungary, Spain, Australia, China and a multicentre study in Asia, a variation is found in the prevalence of dissatisfaction with self-perceived BI between 44 % and 83 % in those individuals with obesity, and between 6 % and 36 % in those individual with low weight, in nine countries that were evaluated. Most of the studies in the review by Jiménez-Flores et al. (Reference Alsaleem47) also found an association between BMI and BI dissatisfaction, as observed in Florianópolis.
In a review study by Sagar and Gupta(Reference Jiménez-Flores, Jiménez-Cruz and Bacardí-Gascón48), which sought to find evidence regarding psychological and psychiatric factors (depression, anxiety, eating disorders, stress, concerns about body shape and low self-esteem) associated with obesity in children and adolescents, several cross-sectional, case–control and prospective studies that found an association between increased BMI and psychopathology were identified.
Part of this relationship between psychological and psychiatric problems and obesity is due to the significant negative impact on the emotional development of obese children and adolescents, as they are more likely to be victims of discrimination, social isolation and bullying(Reference Sagar and Gupta49–Reference Fulton and Srinivasan51). Modern society has adopted negative beliefs that obese individuals are lazy and irresponsible and lack self-discipline even though genetic, socio-economic and environmental factors play a role in the development of obesity. These negative attitudes towards obese individuals have created a negative stigma that leads to prejudice and discrimination, which in turn leads to adverse physical and psychological health consequences for this population(Reference Browne50,Reference Roberts, Polfuss and Marston52) .
This whole framework that involves adolescents with overweight/obesity can contribute to their use of unhealthy weight control strategies. Overweight adolescents may be far from their ideal weight and could be looking for a quick solution. Overweight adolescents may also have failed to lose weight using diet and practicing exercise and may believe that these unhealthy weight control strategies are their last hope(Reference Boutelle, Neumark-Sztainer and Story10).
Recent evaluation of the trend of extreme attitudes towards body weight among adolescents in Brazilian capitals, using data from the National Adolescent Health Survey (PeNSE), in 2009, 2012 and 2015, totalling 166·358 adolescents, aged between 13 and 17 years, found increasing prevalence of extreme attitudes during the evaluated periods, in addition to identifying that adolescents who perceived themselves as fat had 142 % greater chances of extreme attitudes than those who perceived their weight as normal(Reference Haqq, Kebbe and Tan53). Therefore, it is possible to observe that the more dissatisfied adolescents are with their body, the greater the chances of using inappropriate methods for weight control, such as ‘laxatives and diuretics’, and the greater the ‘overeating’ and ‘not eating’, behaviours especially if the adolescent perceives himself/herself as overweight. A population-based, 10-year longitudinal study (Project EAT-III: Eating Among Teens and Young Adults, 1999–2010) that includes 2287 young adults examined the prevalence and tracking of dieting, unhealthy and extreme weight control behaviours, and binge eating from adolescence to young adulthood. Study findings indicate that disordered eating behaviours are not just an adolescent problem but continue to be prevalent among young adults. Use of extreme weight control behaviours during middle adolescence predicted greater risk for these behaviours 10 years later during middle young adulthood for the older cohorts of females and males, and binge eating during adolescence increased risk for binge eating during young adulthood for the older cohorts of females and males and for the younger females(Reference Ferreira and Andrade54).
Because obesity is a multicausal problem, with serious consequences for health that can last throughout life, reflections on prevention strategies are necessary. Lee and Lee(Reference Neumark-Sztainer, Wall and Larson55) point to the necessity to educate adolescents to be more critical of BI and messages disseminated by the media. They also draw attention to the importance of including and educating parents about this same criticality, since they have a strong influence on the perception of BI among adolescents.
Jiménez-Flores et al. (Reference Alsaleem47) also make an important reflection on the way in which government programmes, the media and even universities have conveyed the message of prevention and intervention to obesity, sometimes focusing only on the need for a change in lifestyle, as if those who are above body weight are careless about a healthy lifestyle. Focusing on individual will and unattainable ideal weight for certain vulnerable groups, due to genetic, prenatal and postnatal, and environmental factors, can cause undesirable damage. The multifactorial origin of obesity should not be ignored; therefore, moderation in the messages conveyed and highlighting the need for change in the multiple environments that influence the development of obesity are priority attitudes to be pursued. Finally, in order to promote healthy weight management among overweight youths, it is important to assess whether adolescents correctly interpret healthy weight control messages, such as those recommending regular meals, low-fat foods, increasing FV consumption, and regular physical activity(Reference Boutelle, Neumark-Sztainer and Story10).
The main limitations of this study refer to its cross-sectional design, which makes it impossible to establish causal inferences between the variables, and the instrument used to assess BI, which, being a two-dimensional scale, does not provide a complete picture of a person and can have an impact on the self-perception of BI. In addition, it is important to note that the sample size was calculated taking into account the outcome overweight/obesity, and we added the assessment of the purgative behaviours also as outcomes. The number of adolescents who practice the purgative behaviours is low, resulting in wide CI. Hence, future studies evaluating adolescents’ purgative behaviours outcomes should consider larger samples because purgative behaviour prevalences is lower than the prevalence observed for overweight/obesity. In addition, we used the svy command in our analysis, as it is highly recommended to consider the weight of each person in the sample, even when variables have a smaller number of respondents (e.g. inducing vomit and not eating).
On the other hand, several strengths can be highlighted in this study such as being a representative sample of young adolescents (11–14 years old) from Florianópolis; assessment of two components of BI: attitudinal; use of an illustrated instrument to investigate BI developed and validated for Brazilian children; use of standardised protocols to objectively measure BMI in the sample; and the training of the data collection team. All these procedures contributed to the internal validity of the results. Moreover, our findings in young adolescents highlight the need for parents and physicians to observe closely if individuals from this age group are using non-medical prescription drugs with the aim of controlling their perceptual body weight. Future research with young adolescents should verify if the use of any type of diuretics or laxatives has been adopted upon medical recommendation, although the use of the medications described here are of no use for weight loss or weight control.
Conclusion
There was a high prevalence of BI dissatisfaction among adolescents, especially in those with overweight/obesity. BI influences the adoption of extreme weight control practices in adolescence. Adolescents who wanted to reduce their silhouette had greater odds of using laxatives and diuretics, while adolescents who wanted to increase or reduce their silhouette had greater chances of having episodes of binge eating. These data suggest that non-overweight as well as overweight adolescents are at risk for unhealthy eating patterns, being an alert for parental vigilance aiming at preventing the use of purgative behaviours for weight control by their children.
Acknowledgements
The authors thank the Universidade Federal da Fronteira Sul (UFFS), the Post Graduate Program in Nutrition at the Universidade Federal de Santa Catarina (UFSC) and the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) from Brazil, for the grants received for the implementation of this project.
This study was funded by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (Process nº 483955/2011–6) and by the Universidade Federal da Fronteira Sul (UFFS), Notice nº 459/GR/UFFS/2019. Supports had no decision-making role in the design, data collection, analysis or interpretation of the study, nor in the manuscript writing or in the decision to publish.
K. P. S. worked on data interpretation and manuscript writing; C. E. R. acted in the study design, analysis and data interpretation, as well writing and manuscript review; B. P. B contributed to revision of analysis methods and carried out statistical analysis; L. C. F. C. contributed to the writing and revision of the manuscript. F. A. G. V. guided all steps of the broader research, such as project design and data collection, and contributed to the manuscript review. All authors read and approved the final version of the manuscript.
The authors declare no conflicts of interest.




