


Both acute exposure and chronic exposure to some sedentary behaviours (activities that involve sitting or reclining while expending ≤ 1·5 metabolic equivalents(1)) have been reported to be associated with excess food intake and weight gain in children and youth(Reference Chaput, Visby and Nyby2–Reference Burke, Beilin and Simmer5). Chaput et al. (Reference Chaput, Visby and Nyby2) reported that in comparison with seated rest, 45 min of seated video game play resulted in significant increases in acute food intake and positive energy balance in adolescent males. Similarly, a recent systematic review by Tremblay et al. (Reference Tremblay, LeBlanc and Kho3) concluded that sedentary behaviour (generally measured as time spent watching television) was consistently associated with increased body weight and levels of other markers of adiposity among school-aged children. This evidence has led some to suggest that sedentary behaviour may be a key contributor to increasing paediatric obesity rates(Reference Thivel, Aucouturier and Doucet6–Reference Saunders and Chaput8). However, while there is evidence that some common modalities of sedentary behaviour are likely to increase energy intake in children and youth, the impact of sitting per se is yet to be investigated(Reference Thivel, Aucouturier and Doucet6).
The influence of an imposed bout of prolonged sitting on subsequent physical activity (PA) levels in children and youth is also unclear. It has previously been suggested that PA levels among this population are regulated by an ‘activitystat’(Reference Rowland9–Reference Wilkin, Mallam and Metcalf11). In support of this view, several reports(Reference Rowland9–Reference Thivel, Isacco and Montaurier12) have suggested that in response to an imposed bout of PA, youth may consciously or unconsciously compensate by reducing their PA levels throughout the rest of the day. However, no study has yet examined whether an imposed bout of sedentary behaviour (i.e. sitting) results in a similar behavioural compensation in free-living conditions. If activity levels are regulated by a central mechanism similar to the ‘activitystat’, it is plausible that youth may compensate for a prolonged period of sitting or inactivity by reducing their level of sedentary behaviour and increasing their level of PA later in the day. Given that North American children spend most of their waking time engaged in sedentary behaviours(Reference Colley, Garriguet and Janssen13–Reference Leatherdale and Ahmed15), it is pertinent to investigate the impact of prolonged sitting on subsequent food intake and PA levels, both of which are important health-related behaviours.
The objective of the present randomised cross-over study was to determine whether 1 d of uninterrupted sitting would result in different compensatory changes in ad libitum food intake and/or spontaneous PA levels in healthy children and youth in comparison with a day of sitting interrupted by light-intensity walk breaks, with and without structured PA. Based on the available evidence, we hypothesised that prolonged sitting would result in a compensatory increase in subsequent spontaneous PA levels, a reduction in sedentary behaviour levels and no change in ad libitum food intake.
Experimental methods
Subjects
In the present intervention study, twenty healthy children and youth (twelve males and eight females) aged 10–14 years participated. There were no limits placed on the weights or activity levels of the participants. The present study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the institutional Research Ethics Boards at the Children's Hospital of Eastern Ontario and the University of Ottawa. Written informed consent was obtained from the parents of all the participants. Oral assent was obtained from the participants who were aged 10–13 years (assent was witnessed and formally recorded), while participants aged 14 years provided written consent before participation. The present trial has been registered at ClinicalTrials.gov (identification no. NCT01398059).
Baseline testing session
The present analysis is part of a larger study examining the metabolic impact of prolonged sitting in children and youth, which has been described previously(Reference Saunders, Chaput and Goldfield16). The participants attended one baseline session and three experimental sessions, each separated by at least 1 week. All sessions began at 07.30 hours, and the participants were instructed to fast and abstain from structured exercise for 12 h before each visit. The baseline session included measurements related to anthropometry, PA, sedentary behaviour, cardiorespiratory fitness (VO2 peak) and resting energy expenditure. During this initial visit, the participants were asked to identify any food allergies or intolerances that might impact the standardised breakfast and buffet meals provided during the experimental sessions. Weight was measured to the nearest 0·1 kg using a BWB-800AS calibrated electronic scale (Tanita Corporation of America, Inc.). Standing height was measured to the nearest 0·5 cm using a Tanita HR-100 wall-mounted stadiometer (Tanita Corporation of America, Inc.). BMI was calculated as weight divided by height squared (kg/mReference Chaput, Visby and Nyby2). Children were categorised as overweight/obese using the International Obesity Task Force cut points(Reference Cole, Bellizzi and Flegal17). Waist circumference was measured at the midpoint between the lower border of the last rib and the upper border of the iliac crest after a gentle expiration. Pubertal development was assessed using self-reported Tanner stages as validated previously by Taylor et al. (Reference Taylor, Whincup and Hindmarsh18).
Resting energy expenditure and VO2 peak were measured using an Ultima PF/PFX (MedGraphics) metabolic cart. VO2 peak was assessed using the Dubowy graded treadmill protocol(Reference Dubowy, Baden and Bernitzki19). The participants wore an Actical accelerometer (Philips Respironics) on their right hip for seven consecutive days following baseline testing. Accelerometer data were processed using standardised reduction procedures(Reference Colley, Garriguet and Janssen13) in SAS version 9.2 (SAS Institute) and used to assess baseline levels of PA and sedentary behaviour. Accelerometer cut points of 100, 1500 and 6500 counts/min were used to identify light-, moderate- and vigorous-intensity physical activities, respectively(Reference Puyau, Adolph and Vohra20). Total energy expenditure during each of the experimental conditions was estimated using the following formula, where the thermic effect of food is fixed at 10 %: (resting energy expenditure+PA energy expenditure during the session) × 1·11(21).
Experimental sessions
The participants were exposed to the three experimental conditions in a random order, as determined using a random number generator in Microsoft Excel (Microsoft Corporation). The participants arrived at the laboratory at 07.30 hours for all the experimental sessions and began sitting. During the Sedentary condition, the participants remained seated without interruption until 16.30 hours (when necessary, the participants were transported to the washroom via wheelchair) (Fig. 1). The Sedentary With Breaks (Breaks) condition was similar to the Sedentary condition, with the exception that the participants walked for 2 min on a treadmill at an intensity equivalent to 30 % of VO2 peak every 20 min beginning at 08.40 hours (i.e. 08.40, 09.00 and 09.20 hours). Finally, the Sedentary With Breaks and PA (Breaks+PA) condition was similar to the Breaks condition, but in addition to walking at a light intensity every 20 min, the participants also performed two 20 min bouts of moderate-intensity PA by walking or jogging on a treadmill at 60 % of VO2 peak from 08.40 to 09.00 hours and from 12.40 to 13.00 hours.
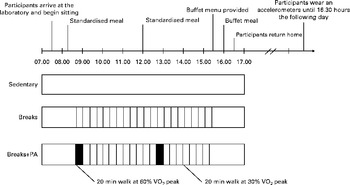
Fig. 1 Overview of the study protocol (modified from Saunders et al. (Reference Saunders, Chaput and Goldfield16)). Sedentary, a day of uninterrupted sitting; Breaks, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min; Breaks+physical activity (PA), a day of sitting interrupted with a 2 min light-intensity walk break every 20 min as well as 40 min of moderate-intensity PA.
During all the three experimental conditions, the participants engaged in a standardised set of common sedentary behaviours in an identical order: 4 h of watching movies and television programmes; 2 h of solving puzzles and doing other forms of mental work; 2 h of playing video games. Each experimental condition concluded with a buffet meal, which lasted from 16.00 to 16.30 hours. The participants wore accelerometers for the duration of each experimental condition and the 24 h following exposure to each experimental condition to assess the levels of PA and sedentary behaviour.
Standardised meals
Standardised meals were provided at breakfast (08.15 hours) and lunch (12.00 hours), using a menu developed for the paediatric population(Reference Shomaker, Tanofsky-Kraff and Zocca22). Breakfast consisted of white bread, butter, peanut butter, cheddar cheese and orange juice, while lunch included chicken strips, tortilla chips, grapes, baby carrots, 2 % milk, lemonade, ketchup and Oreo cookies. Both meals were standardised relative to the estimated daily energy requirements (rather than to the macronutrient intake) with breakfast and lunch, respectively, providing 25 and 40 % of the estimated daily energy requirements. Daily energy requirements were estimated as the sum of resting energy expenditure and average daily PA-related energy expenditure recorded at baseline. The mean intakes at breakfast and lunch were 2322 (sd 410) and 3669 (sd 799) kJ, respectively. The proportions of kJ derived from carbohydrates, fat and protein, respectively, at breakfast were 52 (sd 5), 36 (sd 5) and 12 (sd 1) %, while at lunch they were 57 (sd 2), 31 (sd 3) and 12 (sd 3) %. Participants with allergies or food intolerances (n 3) had individual food items replaced. However, each participant received identical meals at each of the three visits and was asked to consume all food that was provided.
Visual analogue scales
Hunger and prospective food consumption were assessed immediately before the participants were provided with the buffet food menu at 15.30 hours and again immediately following the buffet meal, which occurred from 16.00 to 16.30 hours. This was done using 100 mm visual analogue scales adapted from those described by Hill & Blundell(Reference Hill and Blundell23), which are reliable both before and after consumption of a meal(Reference Arvaniti, Richard and Tremblay24) and have been employed previously in paediatric populations(Reference Chaput, Visby and Nyby2, Reference Rumbold, Gibson and Allsop25). The subjects were asked to place a mark at the position that approximated their level of hunger and the amount of food that they thought they could eat at that time.
Buffet meals
Spontaneous food intake was assessed using an ad libitum buffet meal at 16.00 hours during each experimental condition. The buffet has been validated previously(Reference McNeil, Riou and Razmjou26), and it allowed for the assessment of total energy intake as well as macronutrient composition. The meal consisted of a variety of foods differing in macronutrient composition. The participants selected items from a written menu, were instructed to eat ad libitum and were provided with additional servings on request. The participants were given 30 min for consuming this meal, and all foods were weighed to the nearest 0·1 g before and after ingestion. Energy and macronutrient intakes were calculated using The Food Processor (ESHA Research).
Statistical analyses
As has been described above, the present analysis is part of a larger study investigating the metabolic impact of prolonged sitting in the paediatric population(Reference Saunders, Chaput and Goldfield16). The primary outcome of the study was insulin sensitivity, which was used to estimate the sample size necessary to assess significance. The sample size for the present analysis was, therefore, predetermined. However, given the levels of variability observed in the present study, a post hoc sample size calculation revealed that we had greater than 80 % power to detect a difference of 12 min/d in moderate PA levels, 5 min/d in vigorous PA levels or 600 kJ in energy intake across the study conditions.
Buffet food intake (both in kJ and g), absolute protein intake, percentage of fat intake, and both visual analogue scale scores following consumption of the buffet meal were non-normally distributed and were transformed using Box–Cox transformations to improve normality. Baseline differences between the male and female participants were assessed using the independent-samples t test for continuous variables and using the χ2 test for proportions.
To determine whether males and females could be combined in subsequent analyses, sex × condition interactions were assessed for all the dependent variables. No significant interactions were detected; therefore, males and females were combined for all the analyses to maximise statistical power and improve clarity. A linear mixed model was fitted for each food intake-related outcome, with effects for condition, age, sex, Tanner stage, BMI, and baseline PA and sedentary behaviour. Similar models were used for PA- and sedentary behaviour-related outcomes, with additional adjustment for accelerometer wear time. The present study was not sufficiently powered to investigate the impact of BMI on these results, and therefore BMI × condition interactions were not examined. Statistical significance was defined as a two-sided α-level of 0·05, and a Bonferroni correction was used to adjust for multiple comparisons in post hoc tests following the use of the mixed-effects model. Data are presented as means and standard deviations. All statistical tests were carried out in SAS 9.2.
Results
The characteristics of the study participants are given in Table 1. In comparison with their female counterparts, the male participants were significantly older and spent more time engaged in sedentary behaviour and less time engaged in light-intensity PA at baseline (all P< 0·03). In contrast, at baseline, there were no differences between males and females with respect to BMI, waist circumference, self-reported Tanner stage, or daily moderate-and-vigorous intensity PA (all P>0·15).
Table 1 Characteristics of the study participants at baseline* (Mean values and standard deviations)
LPA, light physical activity; MVPA, moderate-and-vigorous physical activity.
* Baseline differences between the male and female participants were assessed using the independent-samples t test (continuous variables) and the χ2 test (proportions).
The amounts of sedentary behaviour and light- and moderate-intensity PA accumulated during each experimental condition are given in Table 2. As imposed, the three experimental conditions varied significantly with respect to sedentary time, light- and moderate-intensity PA, and total steps during the in-laboratory portion of the study (all P< 0·01). According to accelerometer data, during the Sedentary condition, the participants spent 97·1 % of the laboratory time engaged in sedentary behaviour, compared with 86·5 and 81·0 % in the Breaks and Breaks+PA conditions, respectively. As expected, there were no differences in vigorous PA levels across the three study conditions (P= 0·18), and we observed no differences for any measure related to hunger, food intake or satiety across the three study conditions during the in-laboratory portion of the study (all P>0·06) (Table 2 and Fig. 2). These results were similar with and without adjusting for age, sex, Tanner stage, BMI, and baseline PA and sedentary behaviour. The estimated energy expenditure during the in-laboratory portion of the study differed significantly across the three experimental conditions (all P< 0·01), and it is presented with energy intake in Fig. 2.
Table 2 Measures of sedentary behaviour, physical activity (PA), hunger and energy intake during the time spent in the laboratory engaging in prolonged sitting, with and without breaks and structured PA (Mean values and standard deviations, n 20)
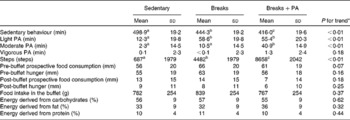
Sedentary, a day of uninterrupted sitting; Breaks, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min; Breaks+PA, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min as well as 40 min of moderate-intensity PA.
a,b,cMean values within a row with unlike superscript letters were significantly different (P< 0·05; Bonferroni correction).
* Significance was assessed using a linear mixed model, with effects for condition, age, sex, Tanner stage, BMI, and baseline PA and sedentary behaviour.
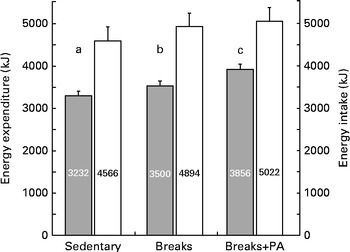
Fig. 2 Energy intake (■) and estimated energy expenditure (![]() ) while in the laboratory during a day of sitting with or without interruptions and structured physical activity (PA). Sedentary, a day of uninterrupted sitting; Breaks, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min; Breaks+PA, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min as well as 40 min of moderate-intensity PA. Energy intake was assessed using an ad libitum buffet meal, while energy expenditure was estimated as (resting energy expenditure+PA energy expenditure) × 1·11. Values are means, with their standard errors represented by vertical bars. Significance was assessed using a linear mixed model, with effects for condition, accelerometer wear time, age, sex, Tanner stage, BMI, and baseline PA and sedentary behaviour. a,b,cMean values with unlike letters were significantly different (P< 0·05; Bonferroni correction).
) while in the laboratory during a day of sitting with or without interruptions and structured physical activity (PA). Sedentary, a day of uninterrupted sitting; Breaks, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min; Breaks+PA, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min as well as 40 min of moderate-intensity PA. Energy intake was assessed using an ad libitum buffet meal, while energy expenditure was estimated as (resting energy expenditure+PA energy expenditure) × 1·11. Values are means, with their standard errors represented by vertical bars. Significance was assessed using a linear mixed model, with effects for condition, accelerometer wear time, age, sex, Tanner stage, BMI, and baseline PA and sedentary behaviour. a,b,cMean values with unlike letters were significantly different (P< 0·05; Bonferroni correction).
The volume of sedentary behaviour and PA accumulated during the 24 h period immediately following exposure to each experimental condition is presented in Table 3. We observed no significant differences for any PA-related variable (all P>0·25). These results were consistent whether examining the absolute levels of activity, as a percentage of total wear time or as a change score relative to baseline levels, or restricting analyses to only those participants who had ten or more hours of wear time (data not shown). These results were not affected by adjustment for age, sex, Tanner stage, BMI, baseline PA and sedentary behaviour, or accelerometer wear time.
Table 3 Sedentary behaviour and physical activity (PA) levels in the 24 h immediately following prolonged sitting with or without breaks and structured PA (Mean values and standard deviations, n 20)
Sedentary, a day of uninterrupted sitting; Breaks, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min; Breaks+PA, a day of sitting interrupted with a 2 min light-intensity walk break every 20 min as well as 40 min of moderate-intensity PA.
* Significance was assessed using a linear mixed model, with effects for condition, accelerometer wear time, age, sex, Tanner stage, BMI, and baseline PA and sedentary behaviour. There were no significant differences between the experimental conditions.
Discussion
The findings of the present study, although exploratory and hypothesis generating, suggest that children may not compensate for an acute bout of prolonged sitting by reducing subsequent food intake or increasing PA levels. Although there were differences in the levels of sedentary behaviour, PA and estimated energy expenditure during the three study conditions, we observed no differences in ad libitum food intake immediately following each session and nor were there any differences in PA or sedentary behaviour levels in the subsequent 24 h period. Future studies are needed to examine whether prolonged sitting results in sustained positive energy balance or whether subsequent adaptations in energy intake or expenditure are able to maintain energy homeostasis.
These results suggest that it is the behaviours that youth commonly engage in while seated (e.g. watching television(Reference Harris, Bargh and Brownell4), playing video games(Reference Chaput, Visby and Nyby2) or doing mental work(Reference Chaput and Tremblay27)) rather than sitting per se that result in the increased food intake associated with sedentary behaviour. This is supported by the work of Epstein et al. (Reference Epstein, Roemmich and Paluch28–Reference Epstein, Roemmich and Paluch30), who have reported that reductions in screen-based sedentary behaviour levels have an important influence on both energy intake and body weight among children and youth. For example, Epstein et al. (Reference Epstein, Roemmich and Paluch28) reported that reducing daily screen time by 25–50 % resulted in a spontaneous reduction in energy intake of 1938 kJ/d in a group of non-overweight teens over a 3-week period. Although PA-related energy expenditure also increased following the reduction in screen time, it was of a much smaller magnitude than the reduction in energy intake (474 kJ/d)(Reference Epstein, Roemmich and Paluch28). Collectively, these findings suggest that focusing on a reduction in screen-based sedentary behaviour levels may have a greater impact on energy balance than a similar focus on total sedentary time.
The findings of the present study also support the assertion that energy intake is not acutely coupled with energy expenditure in the paediatric population(Reference Thivel, Aucouturier and Doucet6, Reference Thivel, Blundell and Duché31). Instead, the available evidence suggests that any acute influence of PA on food intake in children and youth is likely to be related to the intensity of the activity, rather than to the associated energy expenditure. For example, Thivel et al. (Reference Thivel, Isacco and Montaurier12) have recently compared the impact of high-intensity (75 % VO2max) and low-intensity (40 % VO2max) exercise on ad libitum food intake in obese adolescents. They reported that despite both activity bouts expending roughly 1400 kJ of energy, only the high-intensity bout reduced subsequent food intake at lunch and dinner, in comparison with a day without structured exercise. Although the Breaks+PA condition in the present study did include a total of 40 min of structured exercise at 60 % of VO2 peak, it may be that this intensity was insufficient to influence subsequent food intake. It is also possible that the acute influence of exercise on energy intake in this age group may be different between the healthy-weight population and the overweight/obese populations(Reference Nemet, Arieli and Meckel32), although the present study was not sufficiently powered to examine such body weight interactions. Future studies should also investigate variations in the magnitude and direction of behavioural compensation (or lack thereof) following prolonged sitting, as exercise-induced variations in energy expenditure and body weight have been shown to vary considerably among adults(Reference King, Caudwell and Hopkins33).
The findings of the present study also suggest that PA levels are not acutely regulated by an internal ‘activitystat’(Reference Rowland9, Reference Frémeaux, Mallam and Metcalf10), as we observed no difference in PA or sedentary behaviour levels in the 24 h period following exposure to each experimental condition. Instead, these results support the recent findings of Goodman et al. (Reference Goodman, Mackett and Paskins34), who found no evidence that a bout of PA during one portion of the day was compensated for with reduced PA later in the day among a cohort of British children. These results are in contrast to those of Thivel et al. (Reference Thivel, Isacco and Montaurier12), who reported that an imposed bout of high- and low-intensity PA did not significantly increase 24 h energy expenditure above that observed during an inactive day among obese teenagers. However, it should be noted that Thivel et al. (Reference Thivel, Isacco and Montaurier12) assessed energy expenditure by placing participants in calorimetric chambers, which is likely to have substantially reduced their opportunities for spontaneous PA outside of their bouts of structured exercise. In contrast, following the in-laboratory portion of each experimental condition, the present study examined PA levels in free-living conditions, which may help to explain these discrepant findings.
Taken together, the above-mentioned findings suggest that acute sedentary behaviour may contribute to a positive energy balance due to its low level of energy expenditure and by failing to produce a compensatory reduction in energy intake or increase in energy expenditure subsequent to the behaviour. This effect is likely to be exacerbated through the increased energy intake that is associated with many common sedentary behaviours such as television viewing and video game playing(Reference Chaput, Visby and Nyby2, Reference Harris, Bargh and Brownell4, Reference Chaput and Tremblay27). However, the findings of the present study also suggest that the introduction of periodic bouts of light- and moderate-intensity PA throughout the day may increase energy expenditure without resulting in compensatory changes in energy intake or spontaneous PA levels. It is worth noting that PA intensity has been reported to be negatively associated with adiposity in the paediatric age group, and therefore the impact of breaks of vigorous intensity on energy balance are worthy of future study(Reference Leblanc and Janssen35). The present results suggest that activity breaks of at least light or moderate intensity spread throughout the day may be a simple way to promote or maintain energy balance in the current sedentary and obesogenic environment(Reference Chaput and Saunders36).
The present study has several strengths and limitations that warrant mention. The study employed a rigorous randomised cross-over design, which strictly controlled the energy intake, sedentary behaviour and PA levels of the participants across the three study conditions. However, energy intake was measured only once at the end of each in-laboratory session, and PA and sedentary behaviour levels were assessed only in the 24 h period immediately following each laboratory session. It is, therefore, unclear whether similar results would be obtained in response to chronic exposure to prolonged sedentary behaviours. The findings of the present study are also limited by the small sample size, and therefore the possibility of a type 2 error cannot be ruled out. It is also worth noting that the participants were required to eat standardised meals at both breakfast and lunch, which may have been different from the amount or type of food that they would consume on a normal day (habitual diet was not assessed in the present study). Similarly, in the present study, the participants consumed the buffet meal at 16.00 hours, which is earlier than the time the typical evening meal is consumed in North America. Furthermore, the participants of the present study were healthy and more physically active at baseline than the general Canadian population(Reference Colley, Garriguet and Janssen13). Thus, these results may not generalise to physically inactive, obese or diseased participants or to other age groups. In the present study, PA and sedentary behaviour levels were assessed using accelerometers, which cannot be used to accurately measure all forms of activities (e.g. swimming and cycling). However, the use of accelerometers allowed for the assessment of sedentary behaviour and PA in free-living conditions, increasing the ecological validity of these findings. Finally, the buffet in the present study included palatable items such as pizza and potato chips, which may have themselves influenced ad libitum intake or reduced differences across the experimental conditions(Reference Thivel, Aucouturier and Doucet6).
In conclusion, we found no evidence that children and youth compensate for an imposed bout of prolonged sitting, with or without breaks and structured PA, by decreasing their subsequent energy intake and/or increasing their PA levels. These findings suggest that a sedentary day may lead to a positive energy balance through reduced energy expenditure without compensatory reductions in energy intake or subsequent increases in PA energy expenditure. They also suggest that the introduction of light- or moderate-intensity activity breaks throughout an otherwise sedentary day may help to increase energy expenditure with no compensatory increase in food intake, thus promoting energy balance in the paediatric age group. Future studies with larger sample sizes are needed to further investigate the impact of prolonged sitting on energy balance in the paediatric population.
Acknowledgements
The authors acknowledge the study participants and their parents for making important contributions to the present study. They also thank Natalie Tremblay for aiding in participant recruitment, Kathryn Williams for her help with statistical analyses, and Ann Beninato, Isabelle Laforest, Mike Borghese, Niko Tzakis, Allana LeBlanc and Joel Barnes for their assistance with data collection.
The present study was supported by a Research Grant from the Children's Hospital of Eastern Ontario Research Institute to J.-P. C. T. J. S. was supported by Doctoral Research Awards from the Canadian Institutes of Health Research and the Canadian Diabetes Association, as well as an Excellence Scholarship from the University of Ottawa. The funding agencies had no role in the design and analysis of the study or in the writing of this article.
T. J. S. and J.-P. C. conducted the research; E. D. contributed the laboratory space and equipment; T. J. S. carried out the statistical analyses and wrote the first draft of the manuscript with J.-P. C. and M. S. T.; T. J. S. had primary responsibility for manuscript content; all authors contributed to the design of the research project and provided critical feedback and approved the final version.
The authors have no potential conflicts of interest to report.





