



Whey and soya protein, as animal- and plant-based sources, respectively, both represent complete proteins(Reference Lynch, Buman and Dickinson1,Reference Mobley, Haun and Roberson2) . However, there are some differences between these two types of protein, including amino acid composition, digestion and absorption. Whey protein, compared with soya, contains a higher amount of essential amino acids per g and 50 % more branched-chain amino acids(Reference Karlsson, Nilsson and Nilsson3,Reference MacLean, Graham and Saltin4) ; in addition, soya protein is less digestible than whey(Reference Gaudichon, Mahé and Benamouzig5,Reference Mariotti, Mahe and Benamouzig6) .
Resistance exercise with high protein intake, especially whey, has been shown to elicit a positive effect on muscle protein synthesis(Reference Biolo, Maggi and Williams7). Leucine is an essential amino acid and branched-chain amino acid that exists in soya and, in greater amounts, whey protein, and plays an important role in stimulating skeletal muscle protein synthesis at rest and following exercise(Reference Blomstrand, Eliasson and Karlsson8–Reference Garlick11). Indeed, this amino acid can affect the mammalian target of the rapamycin signalling pathway related to protein synthesis and therein enable synthesis(Reference Anthony, Anthony and Kimball12,Reference Anthony, McDaniel and Knoll13) .
Fat mass, particularly visceral adipose tissue, contributes to inflammation in obesity. Enhancing lean body mass can prevent, or at least ameliorate, the increase of fat mass and its consequences(Reference Clément, Viguerie and Poitou14,Reference Wajchenberg15) . Empirical data indicate that having high-protein meals (30 % of total energy intake) during periods of energy restriction, with exercise, especially dairy-source proteins that contain branched-chain amino acids, can promote greater fat mass loss and lean mass retention(Reference Josse, Atkinson and Tarnopolsky16). Further, branched-chain amino acids leucine inhibits adipocyte lipogenesis and stimulates lipolysis; therefore, whey protein that contains high amount of this amino acid can contribute to fat mass loss and lean body mass retention more than soya(Reference Churchward-Venne, Burd and Mitchell17–Reference Sun and Zemel19). Tahavorgar et al., in a 12-week, randomised, double blind clinical trial, in free-living overweight and obese men, indicated that whey protein elicits stronger effects on appetite, anthropometric indicators and body composition than soya protein(Reference Tahavorgar, Vafa and Shidfar20). Additionally, a 9-month resistance training and protein supplementation intervention, by Volek and colleagues, demonstrated that lean body mass gains were greater in the group supplementing with whey protein compared with soya protein(Reference Volek, Volk and Gómez21). On the other hand, in a study by Brown and colleagues, participants were supplemented with either soya or whey protein bars during a 9-week resistance training intervention and there were no significant differences between groups with regard to increases in lean body mass(Reference Brown, DiSilvestro and Babaknia22).
Inconsistent results from randomised controlled trials (RCT) might be explained by the variegated study designs, dose and duration of intervention, and variety of age groups and sex. An advantage of meta-analysis v. narrative reviews is the potential to yield less biased summaries of the published findings. Therefore, we sought to conduct a meta-analysis of published RCT to summarise the evidence on the comparison between whey and soya protein supplementation on body composition among healthy adults and to identify possible sources of heterogeneity between studies.
Methods
This meta-analysis was conducted according to the meta-analysis of RCT studies in epidemiology Cochrane library guidelines.
Search strategy
All articles were retrieved through PubMed, Scopus and Google Scholar, up to August 2020, to identify relevant articles. We utilised medical subject headings (MeSH) and non-MeSH keywords. The following terms were used in the electronic search: (‘body composition’[tiab] OR ‘fat mass’[tiab] OR ‘fat percentage’[tiab] OR ‘body fat’[tiab] OR ‘lean mass’[tiab] OR ‘body lean’[tiab] OR ‘body mass’[tiab] OR weight[tiab] OR ‘Weight loss’[tiab] OR ‘weight reduction’[tiab] OR Overweight[tiab] OR Obesity[tiab] OR ‘body weight’[tiab] OR ‘body mass index’[tiab] OR BMI[tiab] OR ‘Visceral adipose tissue’[tiab] OR ‘adipose tissue’[tiab] OR ‘Perinephric fat’[tiab] OR ‘muscle mass’[tiab] OR ‘Body Composition’[Mesh] OR ‘Adipose Tissue’[Mesh] OR ‘Overweight’[Mesh] OR ‘Adiposity’[Mesh] OR ‘Body Mass Index’[Mesh] OR ‘Obesity’[Mesh] OR ‘Body Weight’[Mesh] OR ‘Weight Loss’[Mesh] OR ‘Obesity, Abdominal’[Mesh] OR ‘Intra-Abdominal Fat’[Mesh] OR ‘Abdominal Fat’[Mesh]) AND (‘soy protein’]tiab[ OR ‘soy’]tiab[ OR ‘soy protein’]Mesh[ OR ‘Soy Bean Proteins’]Mesh[ OR ‘Dietary Soybean Protein’]Mesh[ AND ‘Whey’[tiab] OR ‘Whey protein’[tiab] OR ‘Whey’[Mesh] OR ‘Whey protein’[Mesh]. We had no date and language restriction. To reduce the likelihood of missing any study, the reference lists of all included studies were manually reviewed and we did not include unpublished results and grey literature, including congress abstracts, thesis, dissertations and patents.
Inclusion criteria
We included all randomised clinical trials that investigated the effect of soya protein supplementation and whey protein supplementation on body composition in adults (≥18 years old). Studies that reported mean values and standard deviation, mean values with their standard errors or 95 % CI for body composition variables, such as lean body mass, fat mass, body mass and body fat percentage, before and after intervention, in the intervention and placebo group, were included.
Exclusion criteria
We excluded studies if they were observational, letters to the editor, review articles, in vitro studies, case reports, protocol studies or animal experiments. In addition, studies that had no control group to compare the results with intervention group or had no body composition related data were excluded. Finally, we excluded articles where their study population had diseases that are known to affect body composition.
Study selection
Titles and abstracts of all retrieved articles were evaluated independently by two reviewers (M. P. and A. M.). Articles that did not meet the eligibility criteria were excluded using a screen form, with a hierarchical approach, based on study design, population, intervention or outcome. Next, full texts of eligible articles were retrieved and subjected to a secondary evaluation by the same reviewers. Any disagreements were discussed and resolved by consensus.
Data extraction
Two independent reviewers (M. P. and A. M.) independently extracted data from the included publications, using a standard data extraction form. Data collected from each study included: first author’s last name, publication year, country, characteristics of the participant (number, age, sex, health status), study design, type and dose of intervention and placebo, and duration of intervention, mean and standard deviation and/or changes of the components of body composition, including lean body mass, fat mass, body mass and body fat percentage. If data were reported as se or 95 % CI, they were converted to sd by use of standard formulae.
Quality assessment for individual studies
Two reviewers (M. P. and A. M.) assessed the quality of each selected study and the associated risk of bias using the Cochrane Collaboration’s tool for quality assessment of RCT (Table 1). The quality assessment tool includes the following items: random sequence generation, allocation concealment, blinding of participants and personnel, and outcome assessment, incomplete outcome data, selective reporting and other biases.
Table 1. Study quality and risk of bias assessment using Cochrane collaboration’s tool
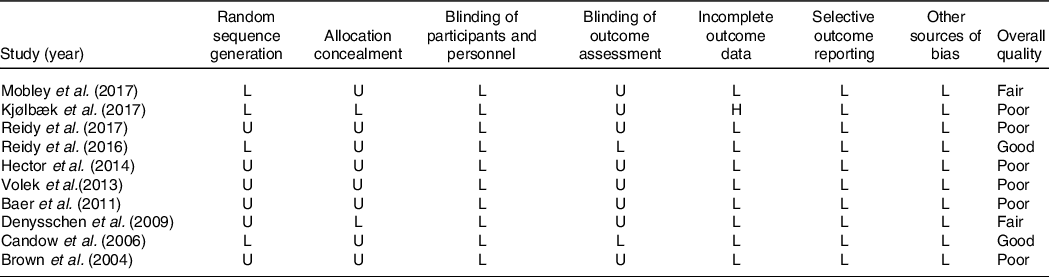
U, unclear risk of bias; L, low risk of bias; H, high risk of bias.
Statistical analysis
All effect sizes were calculated as mean and sd of changes in body composition components between intervention and control groups. The random effects model was used to calculate the overall effect size. We examined heterogeneity between studies by the Cochran’s Q test and I 2 statistic. To discern heterogeneity between studies, subgroup analyses were conducted based on sex (male/female), exercise (with exercise/without exercise), supplement dose (<50 or ≥50 g/d), duration of intervention (<12/≥12 weeks) and health status (healthy/overweight or obese). All statistical analyses were conducted using Stata software, version 13, and statistical significance was accepted, a priori, at P < 0·05.
Results
A total of 662 relevant articles were detected in the initial search, of which 170 were duplicate. The remaining 492 studies were screened based on titles and abstracts. Finally, fifty-five full-text articles were reviewed in detail, and ten were included in the final meta-analysis. The reviewing process is shown in Fig. 1.
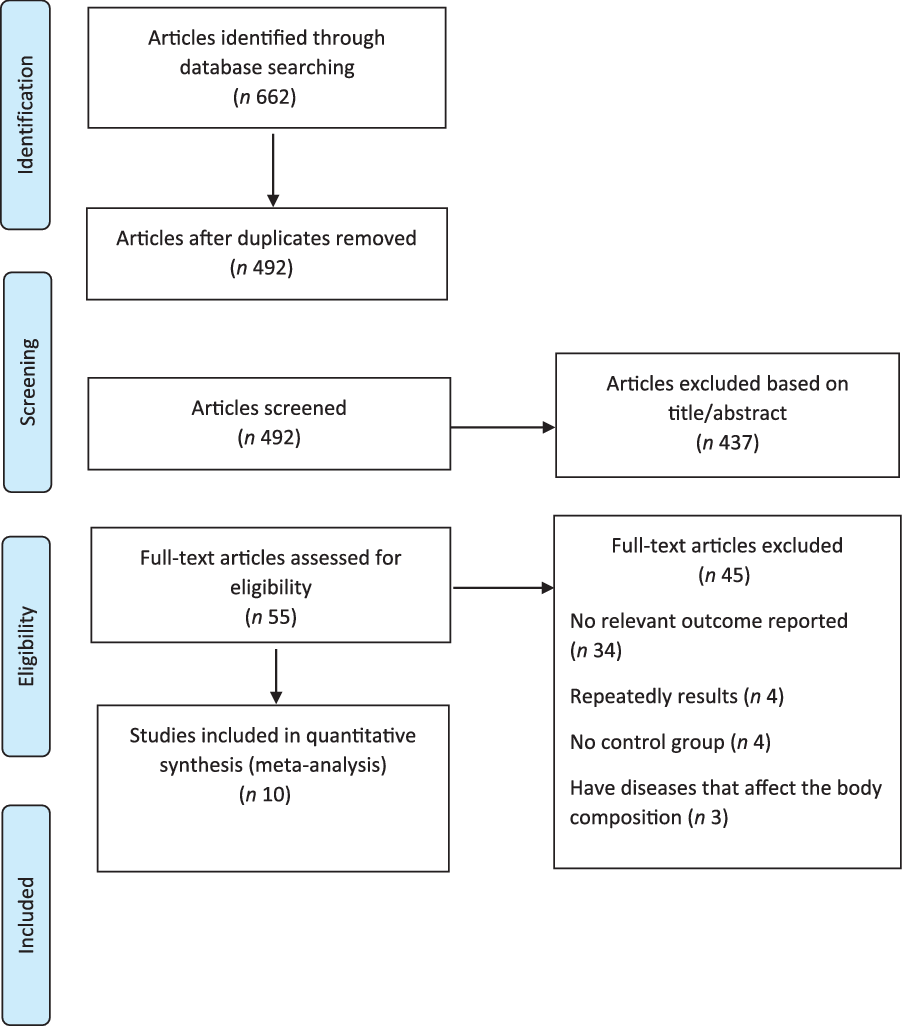
Fig. 1. PRISMA flow chart of the study selection process.
Ten trials, with 596 subjects, were included, of which 356 participants were in the intervention and 240 in control group. Study characteristics are presented in Table 2. Seven studies enrolled healthy individuals(Reference Volek, Volk and Gómez21,Reference Brooks Mobley, Haun and Roberson23–Reference Reidy, Fry and Igbinigie28) , and three studies enrolled overweight or obese individuals(Reference Baer, Stote and Paul29–Reference Kjølbæk, Sørensen and Søndertoft31). Seven studies were conducted in the USA(Reference Volek, Volk and Gómez21,Reference Brooks Mobley, Haun and Roberson23,Reference Brown, DiSilvestro and Babaknia24,Reference DeNysschen, Burton and Horvath26–Reference Baer, Stote and Paul29) , two trials were performed in Canada(Reference Candow, Burke and Smith-Palmer25,Reference Hector, Marcotte and Churchward-Venne30) and one was performed in Denmark(Reference Kjølbæk, Sørensen and Søndertoft31). Participants consisted of both male and females, whose mean ages varied from 18 to 65 years. The intervention periods lasted from 2 to 36 weeks, and all studies were parallel RCT that were blinded. The dosage of soya protein ranged from 22 to 70 g/d, while the dosage of whey protein ranged from 22 to 56 g/d.
Table 2. Characteristics of included studies
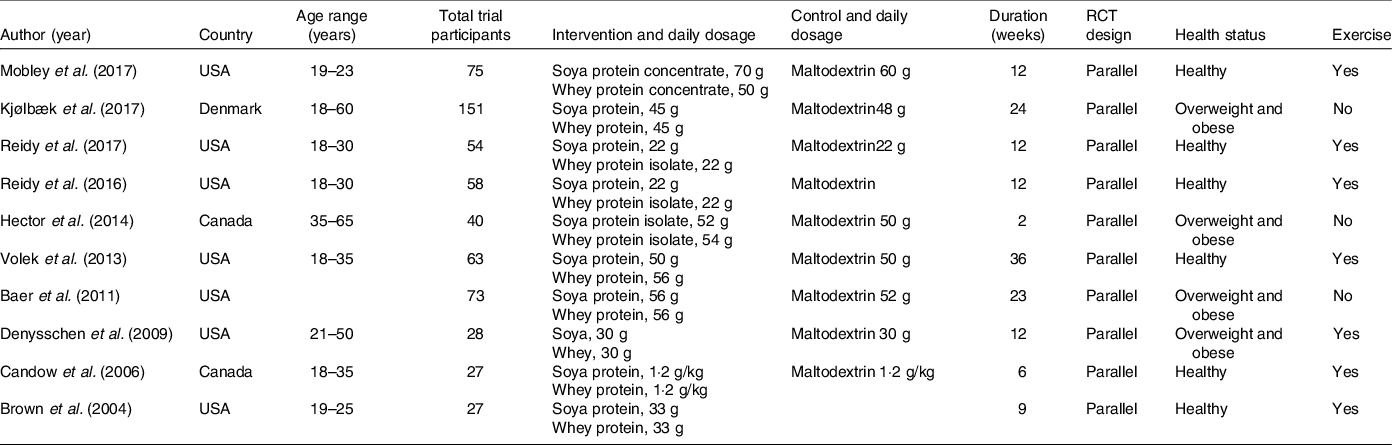
RCT, randomised controlled trials.
Table 3. Subgroup analysis for the effect of soya and whey protein on lean body mass
(Odds ratio and 95 % confidence intervals)
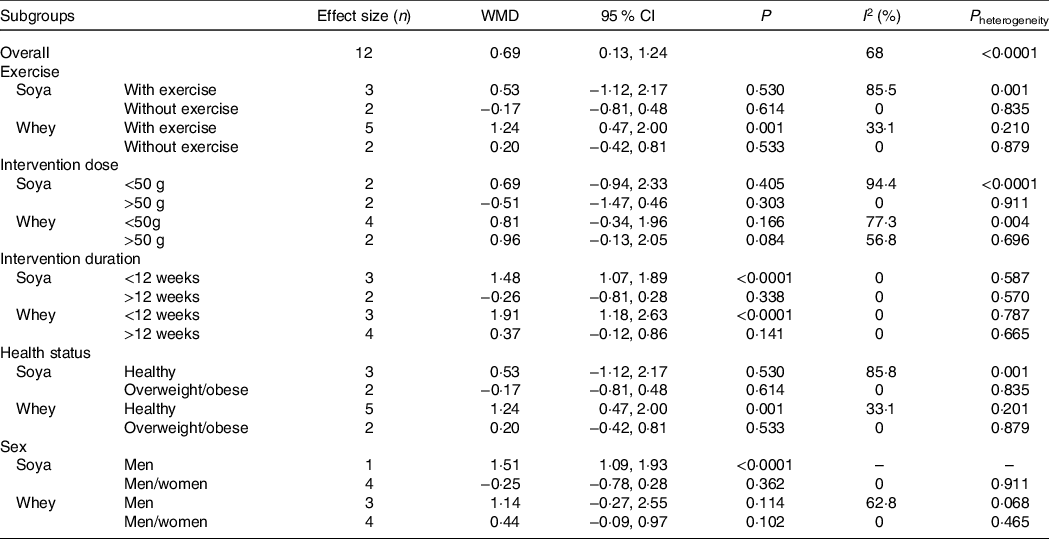
Table 4. Subgroup analysis for the effect of soya and whey protein on body mass
(Odds ratio and 95 % confidence intervals)

Table 5. Subgroup analysis for the effect of soya and whey protein on fat mass
(Odds ratio and 95 % confidence intervals)
Effect of soya protein and whey protein on lean body mass
Seven trials, containing 420 individuals (257 of them in the intervention and the remainder in the control group), were evaluated to investigate the effect of soya and whey protein on lean body mass (Table 3). Based on a random effects model, there was a significant increase in lean body mass between the intervention and control groups (weighted mean differences, WMD: 0·69 kg; 95 % CI 0·13, 1·24; I 2 = 68 %; P heterogeneity < 0·0001). There was no significant effect on lean body mass between intervention and control groups for soya protein (WMD: 0·30 kg; 95 % CI –0·89, 1·50, P = 0·621; I 2 = 85 %; P heterogeneity < 0·0001). Also, there was no significant change in lean body mass between intervention and control groups for soya or whey protein (WMD: 0·87 kg; 95 % CI –0·24, 1·98; P = 0·126, I 2 = 0 %, P heterogeneity = 0·898). There was a significant increase in lean body mass between intervention and control groups for whey protein (WMD: 0·91 kg; 95 % CI 0·15, 1·67, P = 0·019; I 2 = 56·9 %; P heterogeneity = 0·031) (Fig. 2).

Fig. 2. The effect of soya and whey protein on lean body mass.
We found that there was no significant publication bias for lean body mass (Eggers test P = 0·466). The funnel plot is presented in Supplementary Figure 1.
Effect of soya protein and whey protein on body mass
Six trials, containing 430 individuals (243 of them in the intervention and the remainder in the control group), were evaluated to discern the effect of soya and whey protein on body mass (Table 4). Based on a random effects model, there was no significant effect on body mass between intervention and control groups (WMD: −0·63 kg; 95 % CI −1·24, −0·02; I 2 = 9·9 %; P heterogeneity =0·348). There was no significant effect on body mass between intervention and control groups for soya protein (WMD: −0·58 kg; 95 % CI −1·32, 0·16, P = 0·126; I 2 = 0 %; P heterogeneity =0·895). Also, there was no significant effect on body mass between intervention and control groups for whey protein (WMD: −0·46 kg; 95 % CI −1·92, 1·00, P = 0·537; I 2 = 9·9 %; P heterogeneity = 0·068) (Fig. 3).

Fig. 3. The effect of soya and whey protein on body mass.
We found that there was no significant publication bias for body mass (Eggers test P = 0·279). The funnel plot is presented in Supplementary Figure 2.
Effect of soya protein and whey protein on body fat percentage
Two trials, containing ninety-one individuals (sixty of them in the intervention and the remainder in the control group), were evaluated to investigate the effect of soya and whey protein on body fat. Based on a random effects model, there was no significant effect on body fat between intervention and control groups (WMD: 0·48 kg; 95 % CI −0·37, 1·33; I 2 = 0 %; P heterogeneity = 0·693). There was no significant effect on body fat between intervention and control groups for soya protein (WMD: 0·81 kg; 95 % CI −0·44, 2·07, P = 0·204; I 2 = 0 %; P heterogeneity = 0·755). Also, there was no significant effect on body fat between intervention and control groups for whey protein (WMD: 0·20 kg; 95 % CI 0·96, 1·36, P = 0·736; I 2 = 0 %; P heterogeneity = 0·354) (Fig. 4).
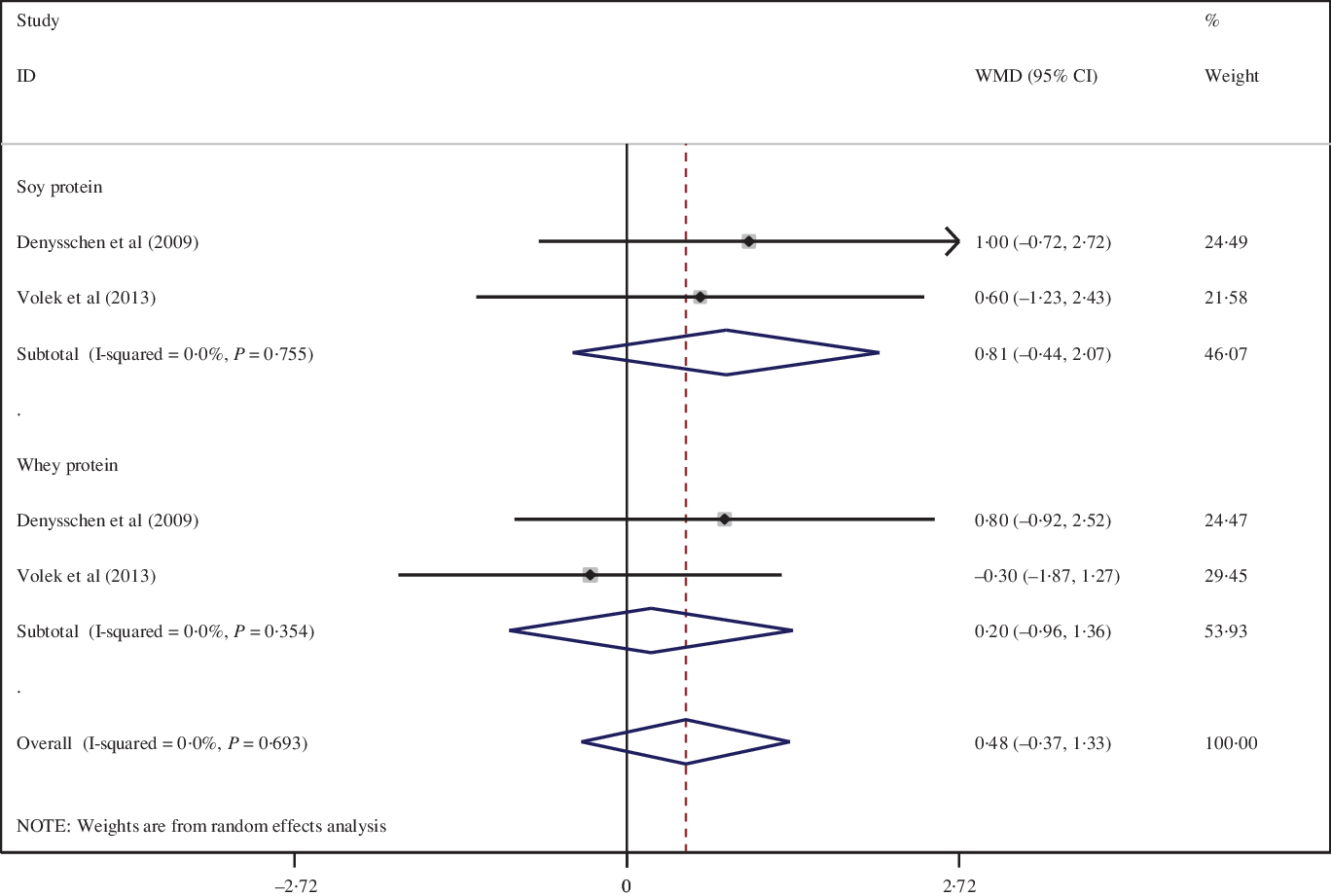
Fig. 4. The effect of soya and whey protein on body fat percentage.
We found that there was no significant publication bias for body fat percentage (Egger’s test P = 0·241). The funnel plot is presented in Supplementary Figure 3.
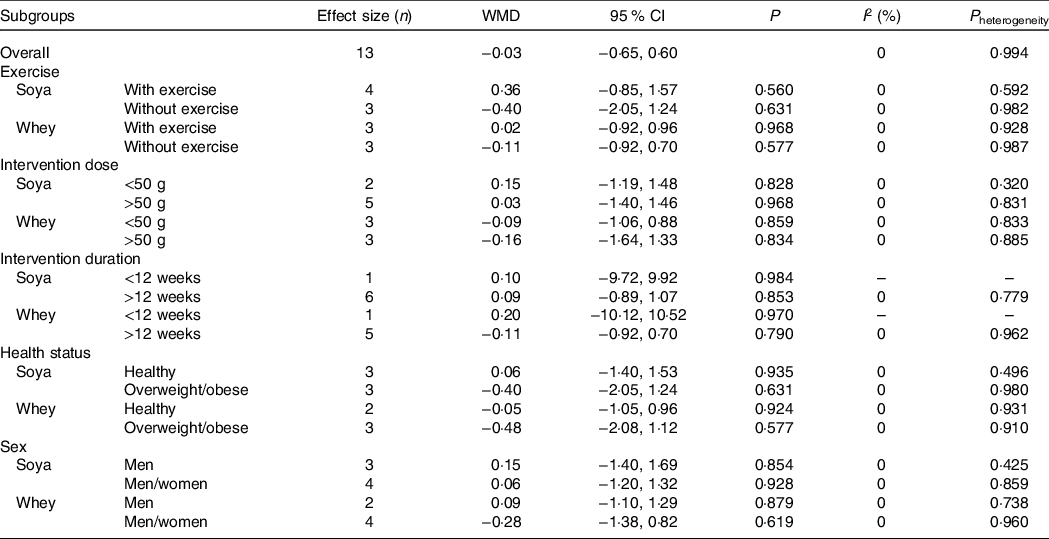
Effect of soya protein and whey protein on fat mass
Seven trials, containing 488 individuals (283 of them in the intervention and the remainder in the control group), were evaluated to investigate the effect of soya and whey protein on fat mass (Table 5). Based on a random effects model, there was no significant effect on fat mass between intervention and control groups (WMD: −0·03 kg; 95 % CI −0·65, 0·60; I 2 = 0 %; P heterogeneity = 0·994). There was no significant effect on fat mass between intervention and control groups for soya protein (WMD: 0·09 kg; 95 % CI −0·88, 1·07, P = 0·852; I 2 = 0 %; P heterogeneity = 0·871). Also, there was no significant effect on fat mass between intervention and control groups in whey protein (WMD: −0·11 kg; 95 % CI −0·92, 0·70, P = 0·792; I 2 = 0 %; P heterogeneity = 0·987) (Fig. 5).
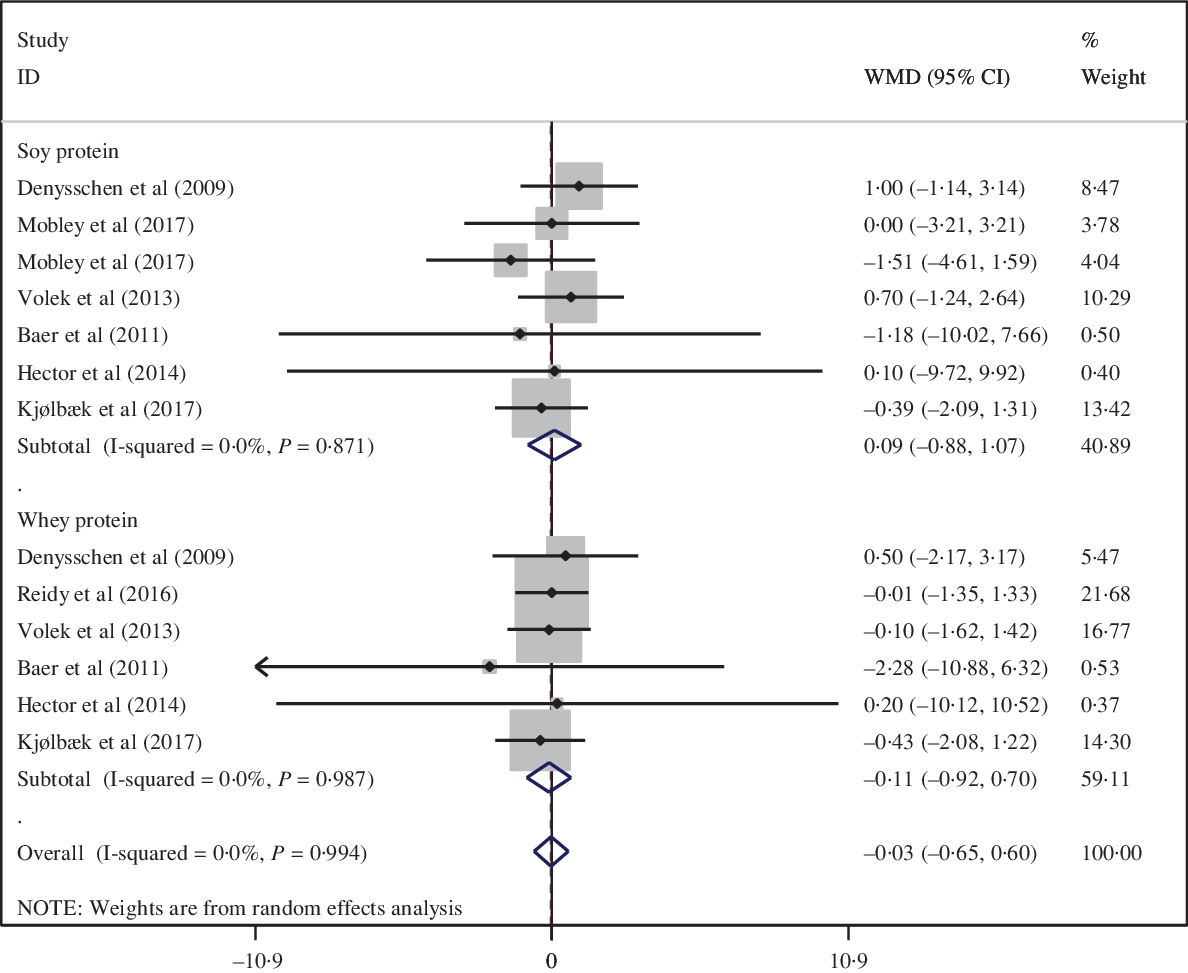
Fig. 5. The effect of soya and whey protein on fat mass.
We found that there was no significant publication bias for fat mass (Eggers test P = 0. 587). The funnel plot is presented as Supplementary Figure 4.
Discussion
In the current meta-analysis, whey supplementation, compared with placebo, was associated with a significant increase in lean body mass, with no concurrent change in body mass, fat mass and body fat percentage. However, soya supplementation, compared with placebo, was not associated with any significant change in lean body mass, body mass, fat mass and body fat percentage. Subgroup analysis indicated that the duration of intervention may play a role in modifying the effect of whey protein and soya protein in increasing lean body mass. For instance, a significant increase in lean body mass was observed among individuals who received 12 weeks or less whey and/or soya protein. A significant increase in lean body mass was observed among individuals with exercise in the whey protein, but not soya protein, group.
A meta-analysis published in 2018 reported that supplementation may elicit an increase in lean mass, while not influencing fat mass or total body mass(Reference Bergia, Hudson and Campbell32). Another study reported a beneficial effect of whey protein on body composition components, including body mass, fat mass and lean body mass, whilst a greater effect was evident when whey protein supplementation was combined with resistance exercise(Reference Miller, Alexander and Perez33). In contrast to our findings, a meta-analysis published in 2019 reported a beneficial effect of whey protein supplementation on fat mass. Indeed, there may be several factors that may make a difference in our finding and previous study; for instance, the aforementioned study only included participants who adhered to resistance training, while in our study, participants without resistance training were also included(Reference Li and Liu34). A recently published meta-analysis indicated that there is no statistically significant overall effect of soya protein on body weight, fat mass and body fat percentage(Reference Glisic, Kastrati and Musa35). Further, discordant with our findings, Mu et al., in a meta-analysis, reported that soya product supplementation reduced body weight and fat mass(Reference Mu, Kou and Wei36). However, in Mu et al., the participants were only overweight and obese women and included various types of soya products, such as soya milk or soya shakes. In contrast, our meta-analysis considered healthy, overweight and obese people. We also considered both sex and included studies with soya protein supplements.
Consumption of whey protein has been indicated to suppress appetite and increase satiety more than other sources of protein, such as casein and albumin(Reference Miller, Alexander and Perez33). Whey protein provides higher amounts of essential amino acids(Reference Li and Liu34) and has a higher content of leucine, which promotes muscle protein synthesis(Reference Kimball and Jefferson37). Whey protein supplementation after resistance training has been shown to increase whole body net protein balance over 10–24 h of recovery, compared with a rested control day(Reference West, Abou Sawan and Mazzulla38). Indeed, whey protein intake results in an increase in fat metabolism, while decreasing the catabolism of protein(Reference Englund, Kirn and Koochek39). Furthermore, whey protein supplementation has been posited to yield decrements in fat mass through increasing post prandial lipolysis(Reference Miller, Alexander and Perez33).
The mechanisms regarding how soya may decrease adiposity are not well understood. Phyto-oestrogens, a constituent within soya, may affect body composition directly via binding with oestrogen receptors (mostly ERα), by mediating the action of hormones that are involved in the regulation of body composition, such as insulin, leptin and ghrelin, or by altering the metabolic activity of adipocytes(Reference Glisic, Kastrati and Musa35). In addition, soya isoflavones can decrease fat accumulation by restricting fat production and increasing fatty acid beta-oxidation(Reference Mu, Kou and Wei36).
Strengths and limitations
The main strength of this meta-analysis is that, to our knowledge, this is the first study to have examined the effect of soya protein and whey protein, comparably, on body composition. We performed several subgroup analyses to determine the factors affecting the results. The anthropometric indicators in this study were comprehensive, allowing a detailed insight into supplementation effects. In addition, all studies that were included examined both whey and soya supplementation, yielding a comprehensive understanding of the effect of soya and whey supplementation on body composition. However, despite the novelty of the present study, there are several possible limitations that should be considered. For instance, whey protein and soya protein were used in difference doses in the included studies. Also, study duration was varied among included studies; although, we tried to account for these discrepancies through pre-planned subgroup analyses. The limited sample size of included studies was another limitation, although, clearly, this is beyond the operational control of the study. Finally, most of the included studies were conducted in American countries, with only limited data available from Asian and European countries, thereby highlighting a distinct gap in the literature that should be addressed.
Conclusion
In conclusion, we found that whey protein supplementation was associated with a significant increase in lean body mass, with no concomitant change in body mass, fat mass and body fat percentage. Additionally, there was a significant increase in lean body mass for whey protein supplementation in individuals performing concurrent exercise and who received 12 weeks or less of whey protein. Finally, soya protein supplementation was not associated with any significant changes in lean body mass, body mass, fat mass or body fat percentage.
Acknowledgements
This study was supported by the student’s Scientific Research Center, Tehran, Iran.
Not applicable.
M. P., A. M. and K. M. contributed to the study concept and design; M. P. and A. T. designed search strategy and screened papers; S. M. performed statistical analysis; M. P. and E. D. wrote the first draft of manuscript; all authors read and approved the final manuscript.
There are no conflicts of interest.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114521001550












