


As the prevalence of childhood obesity continues to rise in the developed world and countries in transition(1), it has become a public health priority. Although the genesis of obesity is complex, it is recognised that childhood overweight and obesity is associated with the metabolic syndrome(Reference Weiss and Caprio2) and that clustered metabolic risk has been shown to track from adolescence into young adulthood(Reference Andersen, Hasselstrom, Gronfeldt, Hansen and Froberg3). Given the insidious consequences of childhood obesity, understanding how best to prevent it remains a research priority. However, the design of potentially effective interventions is somewhat hampered by the general lack of good-quality data available, as highlighted by Wanless in his 2004 report(Reference Wanless4). In addition to this, historically the majority of studies have tended to focus upon one side of the energy balance equation: either physical activity or dietary intake alone.
The potential benefits of studying the determinants of energy balance-related behaviours, that is, both sides of the energy balance equation, are now recognised and may provide an intrinsic contribution to the development of future health intervention programmes(Reference Kremers, Visscher, Seidell, van Mechelen and Brug5). Currently large-scale group or population surveys rely on separate self-reported accounts of physical activity and dietary intake through diary records, frequency and recall questionnaires(Reference Kohl, Fulton and Caspersen6, Reference Livingstone, Robson and Wallace7). However, these methods are not only often labour intensive for researchers, and time consuming and monotonous for children to complete, but do not simultaneously assess energy balance-related behaviours. To the authors' knowledge there is currently no available validated methodology that simultaneously assesses both dietary intake and physical activity behaviours in school-aged children.
The Synchronised Nutrition and Activity ProgramTM (SNAPTM) was developed to address the need for a valid, reliable, low-burden, simple, cost-effective and engaging method of accurately assessing energy balance-related behaviours in children and adolescents at the group or population level. The present paper describes the development, evaluation and future potential of this new software.
Experimental methods
Participants and sampling
A convenience sample (n 121) of schoolchildren was recruited from a local (North East of England, UK) primary and secondary school, with demographically similar catchment areas. Children were recruited from the summer term of Years 3–10 (ages 7–15 years). Age 7 was determined as the minimum age, to reflect the approximate age at which most children have developed the necessary immediate (24 h) recall skills and time conceptualisation necessary to complete the program without parental assistance(Reference Haraldsdottir and Hermansen8Reference Sobo, Rock, Neuhouser, Maciel and Neumark-Sztainer9Reference Van Horn, Gernhofer, Moag-Stahlberg, Farris, Hartmuller, Lasser, Stumbo, Craddick and Ballew10). The study protocol was approved by the School of Health and Social Care Ethics Committee, University of Teesside and informed consent was obtained from every school, parent and child who participated in the study.
Measures
Description of the Synchronised Nutrition and Activity ProgramTM
SNAPTM is a web-based program written using PHP (version 4.0.1), MySQL (version 3.22), and JavaScript (version 1.3) to ensure secure data transfer and storage. The software was developed around the principles of dietary intake and physical activity recall, integrating new and established methods to enhance recall in children, such as: (1) 24 h recall of the structured school day, which has been shown to be more accurate for children within this age group, when compared with periods of longer duration, or of more irregular behaviour patterns associated with the weekend(Reference Haraldsdottir and Hermansen8, Reference Cale11); (2) delivery of the recall activity was in a segmented day format (wake up/before school, on the way to school, breakfast club, mid-morning, lunch, mid-afternoon, on way home from school, after school, evening meal and late evening/bedtime), which has been shown to enhance recall in children(Reference Cale11); (3) children were instructed to recall both their dietary intake and physical activities simultaneously, to facilitate recall aided by ‘behaviour chaining’ described by Baranowski & Domel(Reference Baranowski and Domel12); (4) children were also asked where they consumed their evening and midday meals to assist recall and begin to contextualise certain behaviour patterns; (5) the user interface was designed by a computer-gaming expert to create a novel user-friendly interface to enhance recall and engagement, a method shown to be successful in previous computer-delivered instruments(Reference Ridley, Dollman and Olds13Reference Ridley, Olds and Hill14Reference Welk, Dzewaltowski and Hill15Reference Totten16); (6) visual memory prompts were provided by food/drink and activity pictures (Fig. 1); (7) at the end of the program participants were reminded of all activities, food and drink recorded, and were provided with the opportunity to make final additions or corrections before finishing (Fig. 2).

Fig. 1 An example of Synchronised Nutrition and Activity ProgramTM (SNAPTM) food, drink and physical activity graphics.

Fig. 2 A segment example of the Synchronised Nutrition and Activity ProgramTM (SNAPTM) final recall memory prompt.
The incorporated list of commonly consumed foods (n 40) and drinks (n 9) was developed from a combination of findings from the National Diet and Nutrition Survey(Reference Gregory, Lowe, Bates, Prentice, Jackson, Smithers, Wenlock and Farron17) and previous research into the dietary intake of local children (University of Teesside, unpublished results), and finalised by an expert steering group. A free-text option box labelled ‘other’ was also included to capture any unlisted food or drink. Given the documented difficulties of accurately assessing portion sizes in children(Reference Livingstone, Robson and Wallace7), all foods and drinks were analysed by count (i.e. the number of times a particular food was selected). It was assumed that counts of food and drink would provide the necessary proxy indicator of dietary behaviours.
The incorporated list of common physical activities (n 29; within the domains of sedentary, structured, household chores and play activities) was developed from a combination of common children's activities selected from the Compendium of Physical Activities(Reference Ainsworth, Haskell and Whitt18) and previous research into the physical activities of local children (University of Teesside, unpublished results). A free-text option box labelled ‘other’ was also included to capture any unlisted activities. Transport activities to and from school were investigated separately and categorised into: (1) walk or run; (2) cycle, skate or scoot; (3) bus, car, tram or train. Following the selection of an activity, the participant was questioned further about duration and intensity. Activity duration was estimated in min, by dragging a slider on a timeline, which ranged from 0 to 3 h, visually segmented into 10 min intervals for the first hour and 30 min intervals thereafter. Landmark intervals were illustrated with memory prompts, as shown in Fig. 3. The design of the timeline and associated memory prompts were similar to the trichotomous format described by Ridley et al. (Reference Ridley, Dollman and Olds13). As children have shown difficulty in conceptualising activity intensity(Reference Trost, Morgan, Saunders, Felton, Ward and Pate19), they were asked to click on one of three faces, which illustrated three levels of exertion (light, moderate or vigorous; Fig. 3).
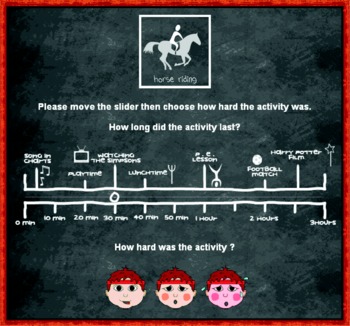
Fig. 3 An example of the Synchronised Nutrition and Activity ProgramTM (SNAPTM) activity duration and intensity assessment.
To enhance the usability of the program, large radio buttons, simple scrolling fields and text enlargement options were included. To aid data interpretation, after completing the recall, participants were asked a short series of questions to determine whether data recorded from the previous day were a typical representation of normal physical activity and dietary intake behaviour.
Each reported physical activity was assigned an intensity code (in metabolic equivalents; MET) drawn from the Compendium of Physical Activities(Reference Ainsworth, Haskell and Whitt18). A MET is the estimated resting energy expenditure with activities defined in multiples of resting metabolism. Although the Compendium values were derived from adult studies, the ratio of activity to resting energy expenditure (i.e. MET) is similar in children and adults(Reference Harrell, McMurray, Baggett, Pennell, Pearce and Bangdiwala20). The intensity thresholds adopted were 3 MET for moderate intensity and 6 MET for vigorous intensity activities. The primary outcome variable for physical activity behaviour was defined as the total min of moderate to vigorous physical activity (the sum of all reported activities of 3 MET and above).
Accelerometry
An objective measurement of physical activity behaviour using accelerometry (Actigraph GT1M; Actigraph, Fort Walton Beach, FL, USA) was used as a reference method for comparison against the SNAPTM self-report tool. The Actigraph is a small, lightweight motion sensor, worn on the right hip (secured by an elastic waistband). It captures and stores instances of vertical movement (in counts per min) and has been shown to produce reliable assessments of physical activity levels in children, although it is insensitive to cycling, load carriage, locomotion on a gradient and other non-ambulatory activities restricted mainly to upper torso movement(Reference Armstrong and Welsman21).
Participants were instructed to wear the device during waking hours, and remove it only during bathing, showering and swimming, making a note of the time and reason for removal and the time of subsequent replacement. The minimum wear time to represent the waking day was defined as 10 h, and this was cross-checked against the self-reported waking time from the SNAPTM tool (minus the reported periods of non-wear). In screening and processing the accelerometry data, the criterion for non-wear was 60 min of consecutive zero counts, cross-checked against the self-reported removal and replacement times.
Activity counts were analysed in epochs of 1 min, with each min assigned an intensity category according to a cut-point for counts per min defined by age-specific prediction equations(Reference Freedson, Melanson and Sirard22Reference Trost, Pate, Sallis, Freedson, Taylor, Dowda and Sirard23Reference Riddoch, Andersen, Wedderkopp, Harro, Klasson-Heggebø, Sardinha, Cooper and Ekelund24). As for the SNAPTM tool, the threshold for moderate intensity activity was defined as 3 MET. This processing permitted the estimation of the total number of min of moderate to vigorous physical activity.
24 h Multiple pass dietary recall
The 24 h multiple-pass recall method, originally developed for food surveys carried out by the United States Department of Agriculture(Reference Guenther, Cleveland and Ingwersen25) and further improved(Reference Moshfegh, Borrud, Perloff and LaComb26), was used as a reference standard to compare with the dietary intake data from SNAPTM. In essence the 24 h multiple pass is comprised of a five-step recall consisting of a quick list of all foods and drinks consumed the previous day, followed by a detailed description of the foods, with the interviewer probing for further information on time or occasion, forgotten foods and food details. All researchers were trained to deliver the multiple-pass interview before working with participants.
Method comparison protocol
Following child and parental consent, each child was fitted with an Actigraph for 2 d (day 1, to desensitise them to wearing the monitor and day 2, the day of activities to be recalled by SNAPTM). Children were given detailed instructions of how to care for and wear their Actigraph device. On day 3 the children returned their Actigraph and completed the SNAPTM program, after a standardised lesson plan was delivered to provide operating instructions. After completing the SNAPTM program the children were invited back to join two trained researchers who carried out the 24 h multiple-pass dietary recall exercise.
After completing SNAPTM and before being interviewed, each child was also asked to complete and return an anonymous questionnaire to gain qualitative feedback on what they liked, disliked and what they would like to change about SNAPTM.
Data analysis
For analytical purposes dietary intake from both SNAPTM and 24 h multiple pass was categorised into counts of twenty-one groups (codes shown in Table 1). Further grouping was carried out to investigate the following dietary behaviours: (1) fruit and vegetable intake (codes 1 and 2); (2) fizzy drink consumption (codes 2 and 3); (3) dairy intake (codes 6 and 16); (4) consumption of energy-dense foods (codes 7, 8, 9, 10 and 11); (5) consumption of complex carbohydrate-rich foods (codes 17, 18 and 19). The outcome variable for the physical activity data was the total min of moderate to vigorous physical activity estimated from the accelerometry v. the SNAPTM methods. The dietary and physical activity data from SNAPTM were compared with the reference methods (multiple pass and accelerometry, respectively) using a combination of the mean between-method differences and non-parametric limits of agreement techniques(Reference Bland and Altman27). Throughout, 90 % CI are reported, as recommended by Sterne & Smith(Reference Sterne and Smith28). Unless specified, all data analysis was carried out using STATA® version 8 (Stata Corp., College Station, TX, USA). Preliminary analyses revealed no substantial differences in measurement error between males and females. Consequently, all method comparison analyses are presented for the pooled sample to maximise precision of estimation.
Table 1 Food-group coding used to categorise dietary intake data

Dietary behaviour groups: * total fizzy drinks; † total dairy; ‡ total energy-dense foods; § total carbohydrate-rich foods; ‖ total fruit and vegetables; ¶ total fish (not takeaway).
For the dietary variables, the accuracy of the computer tool against the multiple-pass method was given by the mean difference (systematic bias) in counts between methods (computer tool minus reference method). The precision of the tool was assessed by calculating the proportion of the sample displaying between-method agreement to within ± 1 count. For the physical activity data, accuracy of the SNAPTM against the accelerometry was assessed initially by the mean difference between methods (computer tool minus accelerometry). A more complete analysis of the accuracy of the computer tool (systematic and proportional bias) was provided by a Passing–Bablok method comparison technique(Reference Bablok, Passing, Bender and Schneider29, Reference Passing and Bablok30) using the Analyze-it® clinical laboratory software (Analyze-It Software Ltd, Leeds, UK). The total min of moderate to vigorous physical activity for the predictor method (computer tool) was regressed on the reference method (accelerometry). Unlike ordinary least-squares regression, the Passing–Bablok method permits measurement error in both the reference method and the comparison method. Importantly, with respect to the present study, this imprecision can have non-constant variance over the sampling range, and the regression line is not adversely affected by outliers. Fixed bias was indicated if the 90 % CI for the intercept did not include zero. Proportional bias was revealed if the slope differed from unity. The overall mean bias of the computer tool compared with the accelerometry was calculated from the Passing–Bablok regression equation at the mean of the reference method distribution. The bias was calculated as Ŷ – X, where Ŷ is the total min of moderate to vigorous physical activity on the computer tool predicted from the regression equation at the mean accelerometry value (X). Precision was assessed by comparing the proportion of the sample that met recommendations of 60 or 90 min of moderate to vigorous physical activity in the previous day. The physical activity method comparison is based on 106 children (fifteen paired data points were eliminated due to missing accelerometry data or incomplete SNAPTM data).
Results
Study characteristics
In total 121 children took part in the validation study; seventy-two girls and forty-nine boys, aged 10·7 (sd 2·2) years. All children were in mainstream education and all except seven spoke English as their first language. Time to complete SNAPTM ranged from 15 to 40 min dependent primarily on reading ability and Internet connection speed. No child was unable to complete the program, although in general more assistance was required for the younger children. When compared qualitatively with the dietary and physical activity validation reference methods, completion of SNAPTM was faster and far less disruptive to the school day.
Dietary behaviours
A summary of the dietary intake data analysis (n 121) categorised by dietary behaviour group (total fizzy drinks, total dairy, total energy-dense food, total carbohydrate-rich food, and total fruit and vegetables; Table 1) is shown in Table 2. In general, SNAPTM underestimated mean counts of dietary constituents and the accuracy decreased with increasing counts. However, the mean difference between methods was substantially less than 1 count for all but three categories – confectionery and cakes (1·15 counts), total energy-dense foods (1·52 counts), and total carbohydrate-rich foods (0·97 counts).
Table 2 Method comparison for the dietary behaviours

MP, multiple pass; SNAPTM, Synchronised Nutrition and Activity ProgramTM (computer tool).
On average, the children consumed approximately one fizzy drink per d, with sugary varieties preferred to the diet alternative. Children also consumed, on average, just over one fruit or vegetable per d. The intake of complex carbohydrate-rich foods was relatively high, so too was the consumption of energy-dense foods, which were consumed between three and five times per d.
Physical activity analysis
Table 3 illustrates how many children participated in the different activity options (not including transport activities) illustrated in SNAPTM. From these data it is clear that only 3 % of all reported activities were sedentary, with the most popular activities being football, running, walking, basketball or netball, cycling and dance.
Table 3 Number of children participating in Synchronised Nutrition and Activity ProgramTM (SNAPTM) activities (not including transport activities)

* Sedentary activities.
The total moderate to vigorous physical activity was 112 (sd 74) min according to the accelerometry method and 103 (sd 71) min with the computer tool. The 90 % CI for the mean difference between methods (systematic bias) of − 9 min was − 23 to 5 min. The results of the Passing–Bablok method comparison are shown in Table 4. Neither the intercept nor the slope differed substantially from the line of identity, revealing no fixed or proportional bias. Applying the Passing–Bablok regression equation at the mean accelerometry value (112 min) resulted in a predicted computer tool value of 108·4 min – an overall bias (fixed and proportional combined) of less than 4 min.
Table 4 Checks for fixed and proportional bias for the computer tool (Synchronised Nutrition and Activity ProgramTM; SNAPTM) against the accelerometry criterion for total min of moderate to vigorous physical activity

* Values are the 90 % CI for fixed bias (intercept ≠ 0) and proportional bias (slope ≠ 1).
The percentage of children who met the recommended 60 min of daily moderate to vigorous activity on this particular day was 70 % according to the computer tool and 68 % with the accelerometry method (difference in proportions 0·02; 90 % CI − 0·08, 0·12). The percentage of the sample meeting 90 min of physical activity at the same intensity was 52 % according to the computer tool v. 54 % with the accelerometry method (difference in proportions − 0·02; 90 % CI − 0·11, 0·07).
Qualitative feedback
Themes emerging from the qualitative questionnaires are shown in Table 5. Generally the feedback was very positive, with the majority of children reporting that they enjoyed using SNAPTM and were able to complete it without great difficulty. However, they also provided some useful feedback which will be incorporated into the next version of SNAPTM, such as more food and activities options and format improvements.
Table 5 Qualitative themes emerging from the feedback questionnaires

SNAPTM, Synchronised Nutrition and Activity ProgramTM; IT, information technology.
Discussion
The SNAPTM software produced a quick, low-burden, simple, cost-effective and engaging method of assessing energy balance behaviours at a group level. Preliminary analysis demonstrated acceptable measurement agreement with the standard method comparators and the majority of participating children enjoyed completing the program and provided positive feedback.
Although on average SNAPTM underestimated moderate to vigorous activities, this was not significant or substantial. The total bias between methods (fixed and proportional combined) of less than 4 min provides a strong indication that SNAPTM is accurate at a group or population level. A high percentage of children from this sample met the current recommendations of 60 min of physical activity per d(31). Over half of this group also met the newer recommendation(Reference Andersen, Harro, Sardinha, Froberg, Ekelund, Brage and Anderssen32) of 90 min.
SNAPTM also provided an acceptable indication of dietary intake behaviour markers similar to the food-frequency work published previously(Reference Johnson, Hackett, Roundfield and Coufopoulos33, Reference Hackett, Gibbon, Sratton and Hamill34). For most food groups, the mean differences were close to zero, although in a few instances SNAPTM underestimated dietary intake by between 1 and 1·5 counts when compared with the findings from the multiple-pass questionnaire. Given the number of dietary components and the size of the study population, more detailed analysis on the dietary data were not feasible, but will be investigated in a larger second-phase study. The CI for the mean difference between methods indicate that the SNAPTM is sufficiently accurate.
The dietary intake recorded is representative of children from this area (University of Teesside, unpublished results). Although consumption of carbohydrate-rich foods was relatively high (approximately 3 counts per d), this was coupled to a very high mean intake of energy-dense foods (four per d) and a fruit and vegetable count that falls far short of the recommended five per d(35). While measurement agreement between the two methods is good, it is important to note that as agreement was calculated to within ± 1 count, it is clear that food groups with smaller counts (such as pies and pasties) will have better agreement than groups with much larger counts (such as confectionery and cakes).
At a group level both the physical activity and dietary data generated from the SNAPTM were comparable with the data generated from the existing standard methods of population-level dietary and physical activity assessment. While the preliminary findings are positive, it is important to note that this was a very small pilot study with very little ethnic, social and cultural diversity. Further studies, which will address and build upon the qualitative findings from the children's questionnaires, are therefore required within a nationally representative population. This second phase should also explore the reliability of SNAPTM and examine the potential use of SNAPTM in recording habitual energy balance-related behaviours over longer time periods.
The potential benefits of this energy balance-related behaviour assessment tool may provide opportunities to examine clustering effects(Reference Kremers, De Bruijn, Schaalma and Brug36) and a link to other important datasets such as educational attainment and body weight(37). The future of such tools, which exploit the popularity, privacy and engagement of the computer interface (in addition to the possibility of data linkage), could make a substantial contribution to future public health monitoring and research.
Acknowledgements
All authors contributed equally to the present study, which was funded internally by the University of Teesside. The authors would like to sincerely thank all the children and staff who participated in the study, alongside Rebekah McNaughton, Nicola Heslehurst, Anna Hatton, Sarah Smith, Leah Avery, Frances Hillier, Aimee Heavyside and Sue Jones for their assistance during the data collection exercise. The authors would also like to thank the Food Standards Agency and the National Centre for Social Research for providing the protocol and permission to use the 24 h multiple-pass methodology and to Dr Helen Crawley for her contributions to the dietary assessment expert steering group. The authors have no conflicts of interest to declare.
Ethical approval for the present study was received from the School of Health and Social Care, University of Teesside Ethics Committee in May 2006. The present study was funded by the University of Teesside. None of the authors has any conflicting interests to declare. All authors declare that this is original work that has not been and will not be published in or submitted to any other journal.








