


The 1992 American Association on Mental Retardation's definition and classification of mental retardation differs from the previous classification system in that: (a) a single diagnostic code of mental retardation is used if the individual meets the three criteria of age of onset (18 years or under), significantly sub-average abilities in intellectual functioning, and related limitations in two or more adaptive skills areas; (b) the individual's strengths and weaknesses are described in reference to four dimensions – (i) intellectual functioning and adaptive skills, (ii) psychological and emotional wellbeing, (iii) health, physical wellbeing and aetiology, and (iv) life activity environments; (c) a profile of required support is developed across the four dimensions(Reference Schalock, Stark, Snell, Coulter, Polloway, Luckasson, Reiss and Spitalnik1).
In Japan, methods of appropriate nutritional management for disabled individuals have attracted increasing attention following the implementation of the Handicapped Individual Independence Support Law in April 2006. However, epidemiological research dealing with the health and diseases of individuals with intellectual and/or motor disabilities lags far behind that dealing with the health and diseases of individuals with no intellectual and/or motor disabilities. Among apparently healthy individuals, particularly elderly individuals, low serum albumin is used as an indicator of poor nutritional status(Reference Starker, Gump, Askanazi, Elwyn and Kinney2–Reference Kergoat, Leclerc, PetitClerc and Imbach7). In Japan, the following indicators are used to assess the malnutrition risk level among the elderly: low risk, ≥ 36 g/l; medium risk, 30–35 g/l; high risk, < 30 g/l(Reference Sugiyama8). However, no epidemiological studies have been conducted that deal with the distribution and correlates of serum albumin levels. We conducted a cross-sectional study examining the distributions and correlates of serum albumin levels among institutionalised individuals with intellectual and/or motor disabilities based on blood profile tests conducted periodically at their facility. A previous report found that the zinc sulfate turbidity test (ZTT), which reflected inflammation, was a cause of reduced Hb levels, which is an indicator of nutritional status(Reference Ohwada, Nakayama, Nara, Tomono and Yamanaka9). Therefore, correlations between inflammatory factors and the serum albumin level, which is another important indicator of nutritional status, were primarily studied.
Methods
The present study analysed the data of 315 individuals with intellectual disability, ninety with cerebral palsy, thirty-three with Down's syndrome, and thirty-nine with severe motor and intellectual disabilities. The subjects were a population of 477 individuals with intellectual disability (286 males, average age 40·6 (sd 12·3) years; 191 females, average age 45·1 (sd 11·6) years) institutionalised at a public facility located in Ibaraki prefecture (109 km north of Tokyo, with a population of approximately 3 million), Japan. In 2001, 12 600 individuals in Ibaraki prefecture were recognised as being intellectually disabled. This public facility houses the more severely disabled individuals; over 95 % of the residents were judged as having a severe intellectual disability.
In Japan, periodic health check-ups are provided for individuals in order to prevent lifestyle-related diseases, including circulatory diseases. The tests that are done have been previously recommended as screening tests for various diseases. The present study retrospectively analysed the existing health check-up data for each resident. The following information was collected during periodic health check-ups done in 2001: blood biochemistry examinations, blood pressure, main disability, main diagnosis, intelligence quotient, and information regarding medications. The modified Binet test for Japanese was used to calculate the intelligence quotient on admission.
Correlates of serum albumin levels were assessed on multiple regression analysis using the serum albumin level as a dependent variable, and age, BMI, anticonvulsants and/or major tranquilisers, minor tranquilisers, other medications (i.e. gastrointestinal drugs, drugs for the common cold, cardiovascular medications), and serum Hb, as well as C-reactive protein (CRP) and ZTT as indices of inflammation. The ZTT is a turbidity test in which reagents are added to the serum samples; the ZTT findings reflect the levels of γ-globulins, particularly IgG. Multivariate analysis was conducted using only three categories of individuals with intellectual disability. Since the characteristics of individuals with severe motor and intellectual disabilities were very different from individuals in the other categories, individuals with intellectual disability, cerebral palsy and Down's syndrome were combined into one category.
All statistical analyses were performed using SPSS® version 15.0 statistical software (SPSS Inc., Chicago, IL, USA). Significance was established at the P = 0·05 level. The research protocol was approved by the Institutional Review Board at Miyagi Gakuin Women's University, with which the first author (H. O.) was affiliated at the time the present study was conducted.
Results
Tables 1 and 2 show the characteristics of the 315 institutionalised individuals with intellectual disability, the ninety with cerebral palsy, the thirty-three with Down's syndrome and the thirty-nine with severe motor and intellectual disabilities. The average BMI was 21·5 kg/m2 for male subjects and 22·0 kg/m2 for female subjects with intellectual disability, 20·7 kg/m2 for male subjects and 21·6 kg/m2 for female subjects with cerebral palsy, 22·2 kg/m2 for male subjects and 24·0 kg/m2 for female subjects with Down's syndrome, and 14·3 kg/m2 for male subjects and 15·1 kg/m2 for female subjects with severe motor and intellectual disabilities. With respect to the blood profiles, the average erythrocyte count, leucocyte count, serum Fe level, total protein level, serum albumin level, total cholesterol level, and HDL-cholesterol level were all within their respective normal ranges. The average Hb level for males with severe motor and intellectual disabilities was 130 g/l, which was lower than the normal range (135–176 g/l). In contrast, the average Hb levels for individuals in the other categories were all within normal ranges. The average ZTT level for individuals with Down's syndrome (male and female) was 15·5 units, which was slightly higher than the normal range (4–12 units). The average CRP for the four categories of individuals, which ranged from 6 to 11 mg/l, was higher than the normal range (0–3·0 mg/l).
Table 1 Characteristics of institutionalised individuals with intellectual disability in Ibaraki prefecture, Japan
(Mean values and standard deviations)

ZTT, zinc sulfate turbidity test.
* For intelligence quotient, 107 male subjects and eighty-one female subjects with intellectual disability.
† For intelligence quotient, twenty-four male subjects and twenty-two female subjects with cerebral palsy.
Table 2 Characteristics of institutionalised individuals with intellectual disability in Ibaraki prefecture, Japan
(Mean values and standard deviations)
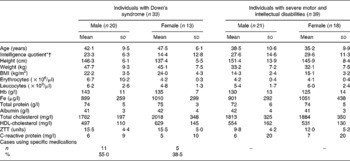
ZTT, zinc sulfate turbidity test.
* For intelligence quotient, thirteen male subjects and eleven female subjects with Down's syndrome.
† For intelligence quotient, eleven male subjects and five female subjects with severe motor and intellectual disabilities.
Fig. 1 shows the serum albumin level distribution among the 474 institutionalised individuals with intellectual and/or motor disabilities. Only six of 474 individuals (1·3 %) had a low serum albumin level (serum albumin ≤ 35 g/l), including two men and two women with intellectual disability and one man and one woman with severe motor and intellectual disabilities. None of the individuals with cerebral palsy or Down's syndrome had a low serum albumin level.
Fig. 1 The serum albumin distributions among 474 institutionalised indiviudals with intellectual and/or motor disabilities in Ibaraki prefecture, Japan. (a) Men with intellectual disability (n 196): mean 44 (sd 3·6), range 31–52 g/l, missing data for one man. (b) Women with intellectual disability (n 116): mean 44 (sd 3·6), range 29–51 g/l, missing data for two women. (c) Men with cerebral palsy (n 48): mean 43 (sd 3·2), range 38–54 g/l. (d) Women with cerebral palsy (n 42): mean 44 (sd 2·6), range 37–50 g/l. (e) Men with Down's syndrome (n 20): mean 41 (sd 2·7), range 38–49 g/l. (f) Women with Down's syndrome (n 13): mean 42 (sd 3·7), range 36–49 g/l. (g) Men with severe motor and intellectual disabilities (n 21): mean 42 (sd 4·5), range 27–50 g/l. (h) Women with severe motor and intellectual disabilities (n 18): mean 41 (sd 3·2), range 35–48 g/l.
Fig. 2 shows the relationship between BMI and serum albumin. In all groups with a BMI from ≤ 15·0 kg/m2 to a BMI of ≥ 27·1 kg/m2, the mean serum albumin levels were between 43 and 44 g/l among men and between 41 and 44 g/l among women, indicating that there were no cases of hypoalbuminaemia.
Fig. 2 Relationship between BMI and albumin among 455 institutionalised individuals with intellectual and/or motor disabilities in Ibaraki prefecture, Japan: (a) males (n 271); (b) females (n 184). Data were missing for fifteen males and seven females.
Table 3 shows the predictors of the serum albumin level among the 433 institutionalised individuals with intellectual and/or motor disabilities. The following factors were identified as being correlated with a low serum albumin level: age, use of anticonvulsants and/or major tranquilisers, use of other medications, high CRP, high ZTT, low serum Hb and low serum Fe among men, as well as high CRP and ZTT among women.
Table 3 Correlates of low serum albumin in 433 institutionalized individuals with intellectual and/or motor disabilities in Ibaraki prefecture, Japan*
ZTT, zinc sulfate turbidity test.
* Dataset for analysis excluded thirty-nine individuals with severe motor and intellectual disabilities from a total of 477 subjects. Additionally, data were missing for five subjects.
† In the multiple regression the dependent variable is serum albumin.
‡ Medications other than anticonvulsants and/or major tranquilisers, minor tranquilisers and Fe replacement (i.e. gastrointestinal drugs, drugs for the common cold, cardiovascular medication).
§ Reference: individuals with intellectual disability.
Discussion
To date, no large-scale epidemiological studies dealing with individuals with intellectual and/or motor disabilities residing in the same environment at a single facility have been conducted. The present findings are significant in terms of broadening our view of the health status of individuals with intellectual and/or motor disabilities.
A low serum albumin level is widely used as an indicator of poor nutritional status(Reference Starker, Gump, Askanazi, Elwyn and Kinney2–Reference Kergoat, Leclerc, PetitClerc and Imbach7). Physiologically, serum albumin levels of 35 and ≤ 28 g/l have been reported to result in visceral protein depletion and oedema, respectively(Reference Starker, Gump, Askanazi, Elwyn and Kinney2). Epidemiologically, a serum albumin level of ≤ 35 g/l has been shown to be an independent risk factor for total mortality (all-cause mortality)(Reference Salive, Cornoni-Huntley, Phillips, Guralnik, Cohen, Ostfeld and Wallace3–Reference Corti, Guralnik, Salive and Sorkin5). Clinically, a serum albumin level of ≤ 30 g/l has been associated with a 2- to 3-fold increase in the incidence of post-operative complications(Reference Rudman and Feller6), as well as a 3·5-fold increase in mortality at 12 weeks post-operatively (38·1 %), while a serum albumin level of ≤ 35 g/l has been reported to result in a 1·9-fold increase in mortality at 2 years post-operatively (63·2 %)(Reference Kergoat, Leclerc, PetitClerc and Imbach7). In addition, a serum albumin level of ≤ 35 g/l has been reported to represent a medium risk for protein–energy malnutrition in acute and long-term care facilities in the USA. In Japan, a serum albumin level of ≤ 35 g/l is noted in approximately 40 % of elderly individuals admitted to medical facilities and in approximately 30 % of elderly individuals requiring homecare, such as nutrition and diet consultations(Reference Matsuda10). Although we initially thought that a high proportion of institutionalised individuals with disabilities would have a serum albumin level of ≤ 35 g/l, in fact an unexpectedly small number of such cases was found. The primary reason for this result may be that the individuals institutionalised at the present facility regularly received meals of adequate quality and quantity and their intake was monitored(Reference Iwaoka, Yokoyama, Masayasu, Fuchi, Nakayama and Tanaka11). The 2005 version of the Japanese dietary reference intakes expresses protein intake in terms of the estimated average requirement, RDA, and target intake (% energy, < 20 %). Since the present facility provided meals according to the target intake, which corresponds to the highest level of protein intake, the residents of this facility appear to have maintained adequate protein levels. Second, albumin is synthesised in the liver. Since in the present study the aspartate transaminase and alanine transaminase levels of all individuals with a low serum albumin were within the normal ranges, their liver function and synthetic capacity were relatively maintained.
Cross-sectional investigation of the correlates of a low serum albumin level identified the following correlates: age, use of anticonvulsants and/or major tranquilisers, use of other medications, high CRP, high ZTT, low serum Hb and low serum Fe among males, as well as high CRP and high ZTT among females. The present findings suggest that males taking medications have an increased risk of a low serum albumin level, though no such relationship was observed in females. The present data regarding medications were obtained through a review of existing medical records and only took into account the use of the medications at the time of the survey. A detailed analysis of the medications' duration of use and dose could not be performed. The relationship that was observed only in males may have been attributable to higher drug doses in males than in females.
Since a high ZTT is thought to reflect high IgG levels, a high ZTT level may be related to chronic inflammation. While chronic and acute inflammation may conceivably reduce the serum albumin level, the focus of this relationship must be clarified. As described in our previous report, though no particular factors were identified on the general systematic evaluation done as part of the periodic health check-ups, the presence of periodontal disease and caries resulting from poor oral hygiene may be related to chronic inflammation(Reference Sugiyama8). Disabled individuals may have difficulty maintaining oral hygiene without assistance. The authors plan to assess data obtained from dental health check-ups in a subsequent study.
BMI is an indicator of nutritional status, and may thus be related to the serum albumin level(Reference Gray12). In the present study, however, there was no relationship between BMI and the serum albumin level. In addition, with respect to the relationship between BMI and the serum albumin level, the average serum albumin among individuals with a BMI of ≤ 15·0 kg/m2 was 44 g/l for males (n 15) and 41 g/l for females (n 15); both of these were within the normal range. This finding may be due to the fact that the present facility ensured that its residents maintained an adequate protein intake; in addition, even individuals with a low BMI maintained reasonable liver function, as indicated by their normal aspartate transaminase and alanine transaminase levels. Third, in a previous study that compared the body compositions of individuals with intellectual disability and healthy individuals, individuals with intellectual disability were found to have a higher body fat percentage and a lower lean body mass than healthy individuals with the same BMI(Reference Iwaoka, Yokoyama, Masayasu, Fuchi, Nakayama and Tanaka11). Therefore, differences in BMI among disabled individuals may primarily reflect the amount of body fat that is present.
The present study found an unexpectedly low incidence of low serum albumin levels among institutionalised individuals with intellectual and/or motor disabilities. In addition, a low serum albumin level was found to be correlated with the use of medications and the presence of chronic and acute inflammation. Further research, using the present study as a baseline, is required to prospectively analyse the relationship between serum albumin levels and prognosis.
Acknowledgements
The present study was supported by a grant from Miyagi Gakuin Women's University. The authors declare that there are no conflicts of interest associated with this manuscript. H. O. and T. N. conceived of the study, and participated in its design, conducted the survey, analysed the data and wrote the manuscript.





