



Type 2 diabetes mellitus (T2DM) affected 10·5 % (536·6 million individuals) of adults aged 20–79 years around the world in 2021, and it is estimated to grow to 12·2 % by 2045. Based on the International Diabetes Federation report (IDF diabetes atlas), the Middle East and North Africa region has the highest comparative diabetes prevalence, which was responsible for 32·6 billion USD T2DM-related health expenditure in 2021(Reference Sun, Saeedi and Karuranga1). It also causes complications such as kidney failure, peripheral arterial disease, myocardial infarction, stroke, retinopathy, cancer and increased mortality(Reference Harding, Pavkov and Magliano2).
Medical nutrition therapy (MNT), as an integral part of all diabetes care and management, is known to be cost effective(Reference Briggs Early and Stanley3). Nutrition education is a segment of the MNT for patients with diabetes, and the delivery of nutritional education is believed to be a priority for improvement in T2DM treatment outcomes(Reference Grammatikopoulou and Goulis4). Moreover, pieces of evidence have shown that nutrition education can effectively reduce disability and mortality caused by diabetes(Reference Sahyoun, Pratt and Anderson5). The value of nutrition education programmes depends on their effectiveness. In addition, nutritional education programmes could effectively amend nutritional behaviours(Reference Najimi, Azadbakht and Hassanzadeh6). Previous studies have shown that nutrition education could change people’s attitudes and behaviour and improve awareness that could possibly improve blood sugar control indicators in individuals(Reference Najimi, Azadbakht and Hassanzadeh6,Reference Miller, Edwards and Kissling7) . However, increasing awareness cannot improve blood sugar control indicators in all cases(Reference Beeney and Dunn8).
The extended parallel process model (EPPM) is one of the several health education models that is used for adopting desirable health behaviour. This model is based on the potential interaction between an individual’s emotions (perceived threat) and rationale (perceived efficacy) for the intention to change health behaviour(Reference Witte9). According to the EPPM, since health messages are transmitted to people by various sources and techniques, the interactions between their perceived threat (susceptibility to health danger and its severity) and perceived efficacy (self-efficacy and response efficacy) made them draw conclusions and take action according to the messages. Consequently, one can show no response (believed to be low susceptibility to danger or the severity is low), danger control response (believed to be highly susceptible but has high self-efficacy) and fear control response (highly susceptible and low in efficacy)(Reference Zareharofteh and Karimi10).
Message framing majorly affects the audience’s response to health-related education(Reference Witte9). Both loss-framed and gain-framed messaging are observed to affect health-related behaviours(Reference Zareharofteh and Karimi10). Loss-framed messaging (LFM) informs about how risky behaviours or not following healthy behaviours may cost or adversely affect health. This type of messaging often leads to fear control response(Reference Ruiter, Kessels and Peters11). While gain-framed messaging (GFM) emphasises on the benefits and positive outcomes of advised healthy behaviours. Individuals are more prone to develop healthy behaviour by GFM. This is while findings about the behaviour change due to these two types of message framing are still contradictory in nutrition education(Reference O’Keefe, Jensen, Batra, Keller and Strecher12–Reference Pakpour, Yekaninejad and Sniehotta15).
According to the elevating prevalence of T2DM, and its adverse health outcomes and health costs, behavioural changes using nutrition education as a part of medical nutrition therapy seem to be necessary. The present study aimed to assess the effect of nutritional education based on the EPPM including GFM, LFM or their combination (G\LFM) in comparison with the usual diabetic education on knowledge, attitude, practice, dietary intake, anthropometrics, blood glucose and lipid profile.
Methods
Study design
A four-arm randomised, double-blind, controlled, factorial field trial was designed. In the present study, nutritional education based on the EPPM including GFM, LFM or G\LFM v. usual diabetic education was conveyed to adults aged 30–59 years with T2DM for 3 months.
Ethical considerations
The protocol of the present study was in accordance with the Declaration of Helsinki for medical research involving human subjects, and ethical approval was obtained from the Ethics Committee of Shiraz University of Medical Sciences (SUMS) (referral code: IR.SUMS.SCHEANUT.REC.1400.012). The study protocol was also registered in the Iranian Registry of Clinical Trials (irct.ir; trial registration: IRCT20230104057040N1).
Prior to participation, volunteers were informed about the research objectives, methodology, and any possible advantages and disadvantages, assured of the confidentiality of their personal information, and notified of their right to leave the study at any stage while this would not affect their routine clinical care. Then, the written informed consent was signed by the volunteers.
Study population and sampling
The participants were adults aged 30–59 years who were residing in the urban area of Bavanat, Fars, Iran. T2DM patients who met inclusion criteria if had fasting blood sugar (FBS) over 125 mg/dl, 2-hour postprandial blood glucose (2hPG) higher than 200 mg/dl, not using insulin, or particular medications, not following dietary medical interventions, not suffering from chronic illness (cancer, liver or hepatic diseases), non-smoker, non-pregnant and not in breast-feeding period, were eligible. After including in the study, if conditions such as incidence of any acute disease, dangerous sudden blood sugar disorders (hyper or hypoglycemia), hospitalisation or undergoing surgery, acute infections and respiratory infection (e.g. COVID-19) and starting to follow a dietary regimen or high-intensity physical activity were met, the participants were excluded from the study.
Among eight urban health centres of Bavanat, four were randomly selected by multi-stage sampling. Then, among eligible individuals who were referred to each health centre, twenty two were randomly selected and included in the study. Each health centre was randomly allocated to a group of study to avoid contamination biases (with lottery). Thus, by adopting each centre as a different group, patients were blinded to the study protocol and they were not informed of groupings and various educations. On the other hand, the person analysing the data was also blinded to the study groups. Hence, the study was conducted as a double-blind trial. The main investigator generated the random allocation sequence, enrolled participants and assigned them to the interventions.
Study procedure
After determining urban health centres, the sampling procedure was started. Eligible and motivated individuals to participate were informed about the study and signed the informed consent. Participants filled out demographic, dietary, physical activity, knowledge and attitude questionnaires. In addition, anthropometric indices were assessed. Then, based on the health center, participants received the related intervention instructions for receiving the predefined messages to follow for 3 months. Finally, participants were also referred to the laboratory for blood tests.
After finishing the 3-month study period, participants were presented to the health center for post-intervention assessments.
Message framing
Three types of messages were prepared based on the EPPM method and they were delivered to the patients based on the virtual methods. Then, four study groups received messages:
1) Gain frame messages (GFM): These messages emphasised the benefits of consuming food items to help blood glucose control. In addition, health, nutritional and lifestyle messages were included in the gain frame messages.
2) Loss frame messages (LFM): Loss frame messages contained the complications of consuming foods that are inappropriate and cause blood glucose disturbances.
3) Combination of both types of messages (G\LFM): G\LFM combined both gain frame and loss frame messages about daily food items consumed by the Iranian population, health and lifestyle factors ameliorating or worsening their blood sugar levels.
4) Control group (CG): In this group, participants received standard messages that are used in the routine care of diabetic patients in the Iranian health system in the form of text messages or descriptions.
It is noteworthy to state that messages pertinent to routine moderate physical activity were conveyed to all participants in the intervention groups. Moreover, standard messages about physical activity were included in the CG education as well.
Messages for the GFM, LFM and G\LFM groups were prepared in the form of video clips, info graphs and texts, with the assistance of the faculty members of Community Nutrition, Health Education departments and Virtual School, Comprehensive Center of Excellence for Advanced Electronic Learning in Medical Sciences of Shiraz University of Medical Sciences.
Coordination of all groups was done using face-to-face meetings and also telephone calls were made to reduce the presence of participants at health centers during the COVID-19 pandemic. Moreover, using the WhatsApp instant messaging application, virtual groups were created to deliver educational content and keep in touch with participants in all four groups, and weekly telephone calls were made to ensure the use of content by participants. It should be noted that, after finishing the study, prepared messages for the study were handed to the CG participants.
Knowledge, attitude, practice assessment
To assess the level of knowledge, a twenty-five item questionnaire was compiled. Questions were asked about the participants’ knowledge about awareness of diabetic nutritional recommendations and diabetes complications (e.g. ‘Can legume consumption improve blood glucose control?’, ‘Does dairy product consumption should be limited in the individual with diabetes?’, etc.). For each right answer, participants earned one point and for every wrong answer or in case of stating to have no idea, zero point was given. Finally, a mean score was calculated for each participant.
Another questionnaire based on Kim White’s instructions(Reference Witte16) was developed to measure the sub-scales of the EPPM including ‘perceived sensitivity’ (eight items), ‘perceived severity’ (nine items), ‘perceived self-efficacy’ (nine items), ‘perceived response efficacy’ (five items) and ‘behavioural intention’ (ten items). The questions were designed as multiple choices and the answers were based on a Likert scale from ‘I strongly agree’, ‘I agree’, ‘I disagree’ and ‘I strongly disagree’ and scored from 4 to 0, respectively. Participants’ score was measured by calculating the mean score for the questionnaire. This was used to assess the participants’ attitudes.
The face and content validity of the questionnaire was evaluated by a panel of experts consisting of faculties with nutrition and health education majors (n 10). The external and internal validity of the questionnaire was assessed on thirty individuals with the same criteria as the study population using the test-retest method and calculating Cronbach-α.
Moreover, the practice of the participants was evaluated by means of dietary intake and physical activity assessments.
Anthropometric assessment
Height was measured using the Seca scale (model: 803, GmbH & Co. KG), with the least possible clothing, while the participant was standing straight in the middle of the scale, with an accuracy of 0·1 kg. A tape measure was attached to the wall to record participants’ height with an accuracy of 0·1 cm. Participants stood straight with no shoes and hat while looking forward and the heels, buttocks and shoulders touched the wall. Waist and hip circumferences were measured using an inelastic tape measure to the nearest 0·1 cm. Waist circumference (WC) was assessed in the mid-point between the iliac crest and the lowest rib. The largest circumference of the hip was recorded as hip circumference. Waist:hip ratio (WHR) was calculated by dividing WC by hip circumference. BMI was calculated using the standard formula (weight/(height)2). All the aforementioned variables were considered secondary outcomes.
Blood biomarker assessments
At the beginning of the study phase and the end of the study, participants were recruited at the health center after overnight fasting. A 5 ml venous blood sample was taken to assess fasting blood sugar (FBS) and glycated Hb (HbA1C) tests by the nurse staff of the health centre. Moreover, 2 h after breakfast, another 2 ml blood sample for assessing 2-hour blood sugar was taken. The blood sample was divided into 2 tubes, one 1 ml for HbA1c measurement (tube containing EDTA anticoagulant) and the rest in a haemolysis tube to separate the serum for measuring fasting blood sugar (FBS) and lipid profile. Blood samples were kept in a − 70 °C freezer until conducting final analysis.
HbA1c was measured by a medical diagnosis laboratory using HPLC with a Roache Cobas analyser (Roche Austria GmbH). FBS, 2-hour blood sugar and lipid profile including total cholesterol, TAG, high- and low-density lipoproteins (HDL and LDL) were assessed using calorimetric method by auto-analyser BT1500 (Biotecnica Instruments, Italy) and the commercial kits (Pars Azmoon, Iran) in the laboratory of School of Nutrition and Food Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
HbA1c was considered as the primary outcome, and all other biochemical variables were considered as secondary outcomes.
Dietary intake and physical activity assessment
The dietary intakes of participants were recorded using a 3-day food recall questionnaire to report consumed food items and their ingredients for complex foods before and after the interventions. The 3-day food recall was analysed with Nutritionist 4 software (N4). Daily energy, protein, carbohydrate and fat intake were extracted from N4 results.
The physical activity level of participants was assessed using the MET questionnaire at the beginning and final phase of the study. Participants reported their daily physical activity from a predetermined list of physical activities and the time spent on each activity from a validated questionnaire. To calculate the energy consumed by each participant in physical activity, the amount of energy burnt by each activity per minute is multiplied by a day and the duration of the activity and is calculated based on the MET unit (metabolic equivalent), which is the amount of metabolic equivalent energy in the activity. MET for light intensity activity, walking, moderate, high and rigorous intensity activity are equal to 1·5, 3, 4, 5–6 and over 6, respectively. The total amount of energy consumed in physical activity for different activities was calculated(Reference Jetté, Sidney and Blümchen17).
Statistical analysis
Glycated Hb (HbA1c) was considered as the primary outcome for sample size calculation. By considering α = 0·05, test power of 80 %, mean differences of 0·36 and 0·04 and standard deviation of 17·49 and 13·06 for pre- and post-HbA1c, respectively(Reference Sharifirad, Entezari and Kamran18), the sample size was estimated to be 20. Finally, with a probability of 10 % dropouts, twenty-two participants were considered for each group.
Data analysis was performed in SPSS software (Version 23, IBM). Quantitative data are shown as mean ± s d, and categorical variables are summarised as frequency and percentage. The Shapiro–Wilk test showed no skewness in the data. Thus, the Wilcoxon signed-rank test was used for within-group analysis, and between-group comparisons were done using the Kruskal–Wallis test. In the case of significant differences between groups, the Mann–Whitney U test was performed to find groups with significant differences. The assessments of knowledge and attitude questionnaire content validity were done by an expert panel composed of ten specialists. The content validity ratio and the content validity index were evaluated. The reliability test, by a test-retest method, was done on thirty individuals with similar characteristics as the study population. The internal consistency of the questionnaire was assessed by Cronbach’s alpha test. Cronbach’s alpha > 0·7 was considered an acceptable internal consistency. A significance level of P > 0·05 was considered.
Results
The present study was carried out between January 2022 and June 2022. Among the 150 participants who were evaluated for eligibility, thirty two did not meet the predefined inclusion criteria and thirty were not willing to cooperate. Finally, eighty-eight eligible T2DM patients were randomly assigned to four study groups (twenty-two people in each group). During the study period, eight did not successfully finish the investigation (three from the control group, two from each GFM and LFM groups and one from the G\LFM group) and were excluded from the study. Therefore, the total number of eighty T2DM patients entered the final analysis. Figure 1 depicts the overall study flow diagram.
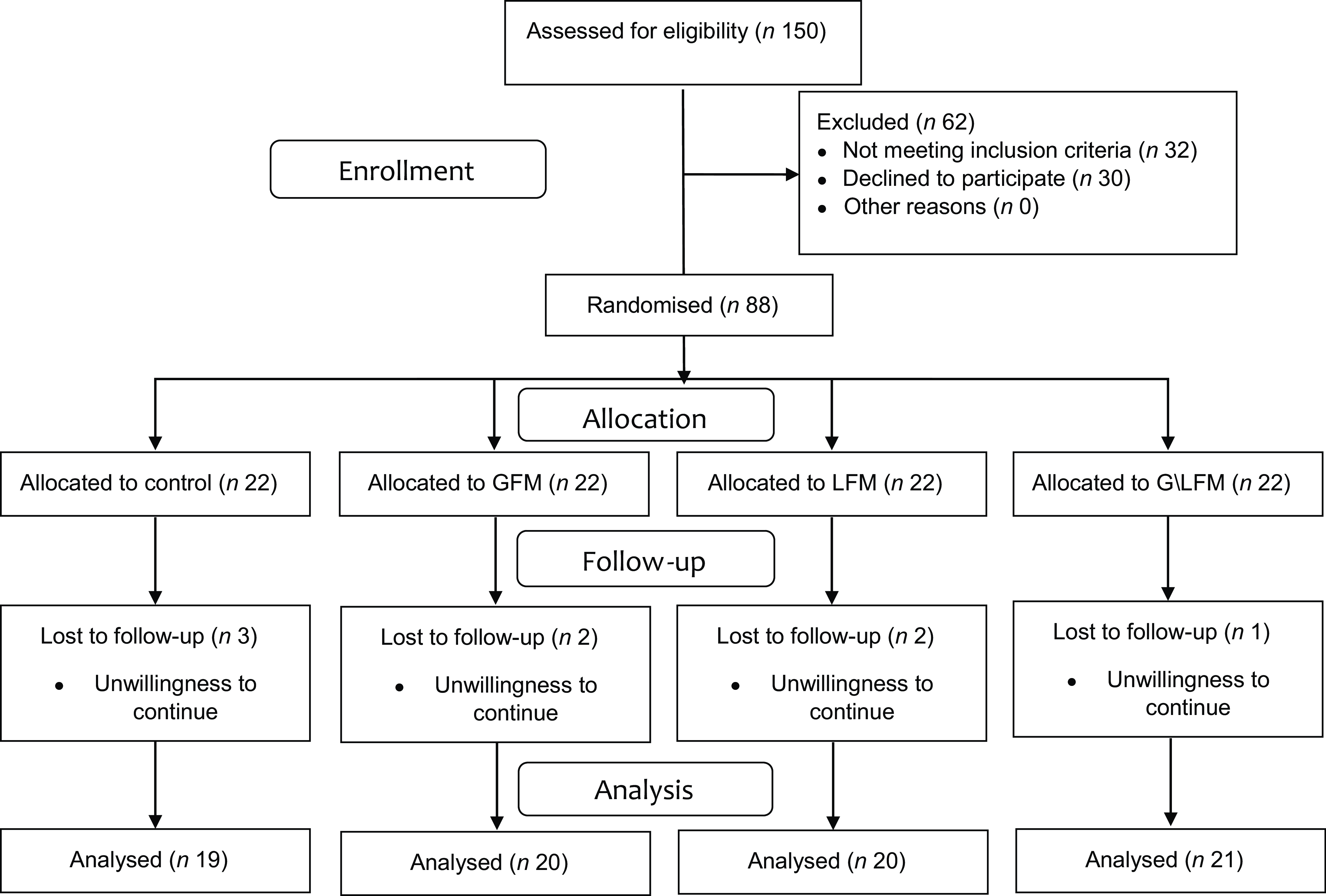
Fig. 1. Consort flow diagram of the study.
Table 1 shows the demographic characteristics of the study participants. Participants were not significantly different according to age between groups. In all four groups of the study, the majority of participants were female and had a middle income and a history of the diseases.
Table 1. Demographic characteristics of participants based on the groups
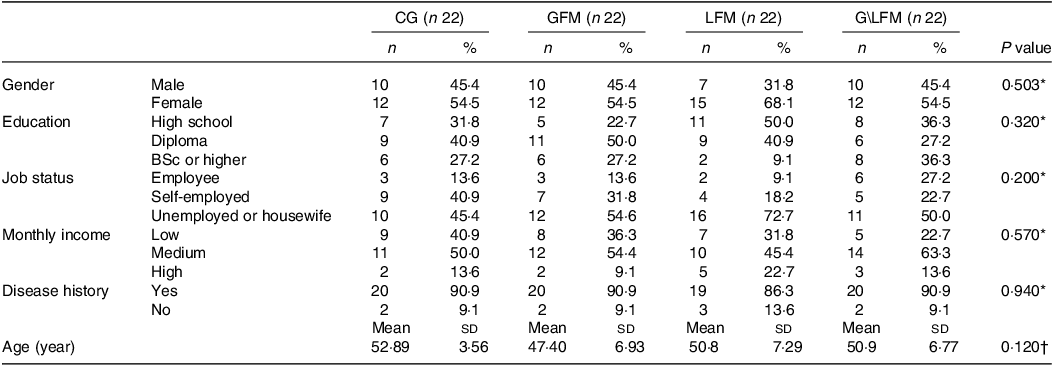
CG, control group; GFM, gain frame messages; LFM, loss frame messages; G\LFM, gain and loss frame messages; BSc, Bachelor sciences.
Data are presented as frequency (percent), only for age that is presented as mean (sd).
P values < 0·05 was considered significant.
* χ 2 test.
† Kruskal–Wallis test.
Knowledge and attitude questionnaires validity
Questionnaires were assessed for validity and reliability. Based on the opinions of the expert panel, the questionnaire has high content validity. The internal consistency of the knowledge questionnaire was fair (Cronbach’s alpha = 0·66), while other sub-scales showed desirable internal consistency (Cronbach’s α > 0·7). Table 2 summarises the results for questionnaire validity.
Table 2. Validity assessments of knowledge and attitude questionnaires

CVI, content validity index; CVR, content validity ratio.
* Cronbach’s alpha.
† Pearson correlation.
Extended parallel process model based education and knowledge and attitude
Baseline assessments of knowledge and attitude did not reveal any significant differences among participants (P > 0·05). After 3 months of intervention, within-group analysis showed increments in knowledge (P = 0·001 for all intervention groups), perceived sensitivity (P < 0·001 for all intervention groups), perceived severity (P < 0·001 for all intervention groups), perceived self-efficacy (P < 0·001 for all intervention groups), perceived response efficacy (P < 0·001 for LFM and G\LFM groups and 0·005 for GFM group) and behavioural intention (P < 0·001 for all intervention groups), but not for CG (P > 0·05). Between-group comparisons for mean changes showed significant differences in knowledge and EPPM subscales between control groups which was pertinent to the differences between each intervention group and the CG (P < 0·001 for all except perceived response efficacy: P = 0·029). Table 3 shows the knowledge and EPPM components score for participants based on their groups.
Table 3. Knowledge and EPPM components score of participants based on their groups during the study phase
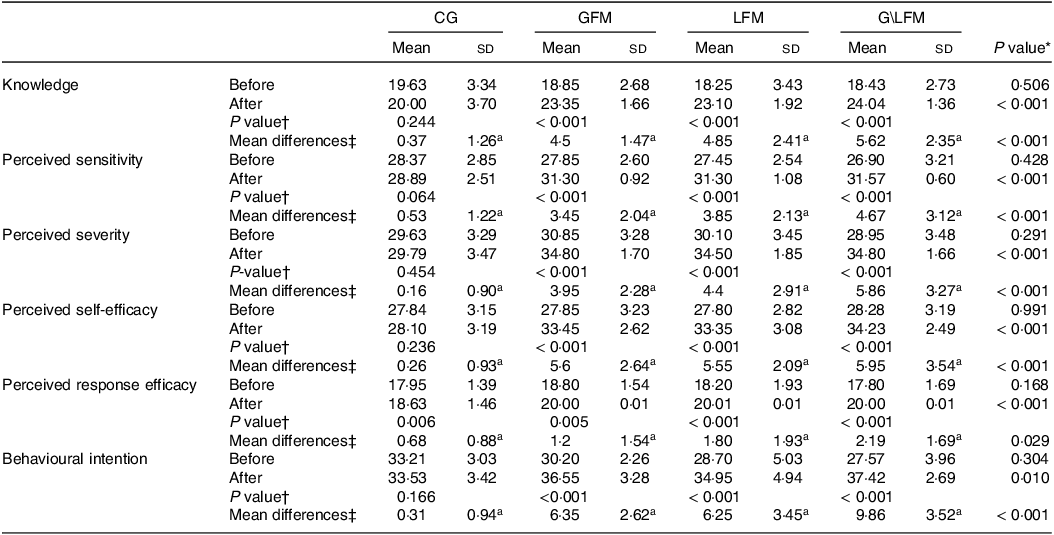
EPPM, extended parallel process model; CG, control group; GFM, gain frame messages; LFM, loss frame messages; G\LFM, gain and loss frame messages.
For before study n 22 in each group, after study n 19 for CG, n 20 for GFM, n 20 for LFM and n 21 for G\LFM.
Data are presented as mean (sd).
* Kruskal–Wallis test. Same superscript letters indicate between-group significant differences using Mann–Whitney U test.
† Wilcoxon signed rank test.
‡ Mean differences showed post-pre measurements.
Extended parallel process model based education and dietary intake and physical activity
Participants’ daily dietary intake for energy and macro-nutrients were similar before the study period. Mean changes in carbohydrate intake were different between CG and GFM groups (P = 0·036). Individuals in GFM (–17·15 ± 23·82 g/d, P = 0·004) and G\LFM (–11·33 ± 24·04 g/d, P = 0·034) had lower carbohydrate intake during the study period. Considering intragroup changes in fat intake, mean changes were different between CG and GFM groups (P = 0·036). Fat intake decreased after the intervention in the LFM (–4·45 ± 8·76 g/d, P = 0·034) and G\LFM (–4·33 ± 9·85 g/d, P = 0·047) groups.
Although baseline physical activity levels were similar between groups, after the study phase, physical activity metabolic equivalents were significantly increased in GFM (mean change = 3·63 ± 6·40 MET/min/d, P = 0·001), LFM (mean change = 2·83 ± 3·18 MET/min/d, P = 0·002) and G\LFM (mean change = 2·88 ± 2·60 MET/min/d, P < 0·001). Between-group analysis for mean changes in physical activity showed significant differences between groups which was related to the differences between the GFM (P = 0·005), LFM (P = 0·001 and G\LFM (P = 0·001) in comparison with the CG. Table 4 summarises the dietary intake and physical activity of participants.
Table 4. Daily intakes of energy and macronutrients and physical activity of participants during the study phase
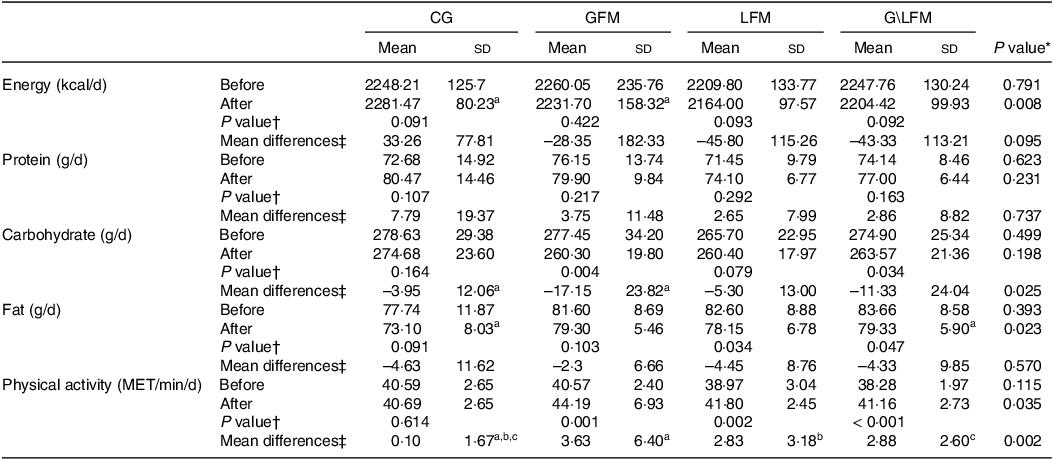
CG, control group; GFM, gain frame messages; LFM, loss frame messages; G\LFM, gain and loss frame messages.
For before study n 22 in each group, after study n 19 for CG, n 20 for GFM, n 20 for LFM, and n 21 for G\LFM.
Data are presented as mean (sd).
* Kruskal–Wallis test. Same superscript letters indicate between-group significant differences using Mann–Whitney U test.
† Wilcoxon signed rank test.
‡ Mean differences showed post-pre measurements.
Extended parallel process model based education and anthropometric indices
Table 5 describes anthropometric assessments of participants based on their groups. Analyses showed that participants were similar among groups for anthropometric indices at the beginning of the study phase. Although in the intervention groups’ weight, BMI, WC, hip circumference and WHR decreased, and results for changes in hip circumference, WC and WHR between groups did not show significant changes.
Table 5. Anthropometric characteristics of participants based on their groups during the study phase
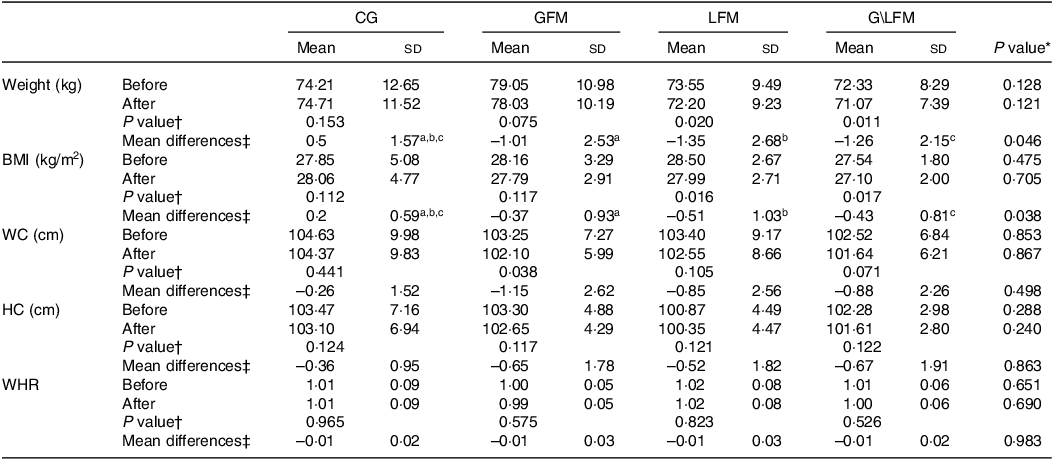
CG, control group; GFM, gain frame messages; LFM, loss frame messages; G\LFM, gain and loss frame messages; WC, waist circumference; HC, hip circumference; WHR, Waist:hip ratio.
For before study n 22 in each group, after study n 19 for CG, n 20 for GFM, n 20 for LFM and n 21 for G\LFM.
Data are presented as mean (sd).
* Kruskal–Wallis test. Same superscript letters indicate between-group significant differences using Mann–Whitney U test.
† Wilcoxon signed rank test.
‡ Mean differences showed post-pre measurements.
Between-group analysis for mean changes showed significant differences between groups considering weight (GFM: P = 0·041; LFM: P = 0·013; G\LFM: P = 0·017) and BMI (GFM: P = 0·039; LFM: P = 0·011; G\LFM: P = 0·021) in comparison to the CG (weight: 0·50 ± 1·57; BMI: 0·20 ± 0·59) (Table 5).
Extended parallel process model based education and biochemical indices
Table 6 indicates blood glucose and lipid profile assessments of participants based on their groups. Biochemical indices were not statistically different among study groups at baseline measurements. The 3-month intervention led to a significant reduction in within-group analysis for FBS (P for GFM: 0·016, LFM: 0·006 and G\LFM: 0·012), 2hPG (P for LFM: 0·020 and G\LFM: 0·031) and TAG (P for GFM: 0·033, LFM: 0·00·028 and G\LFM: 0·030).
Table 6. Blood glucose and lipid profile of participants based on their groups during the study phase
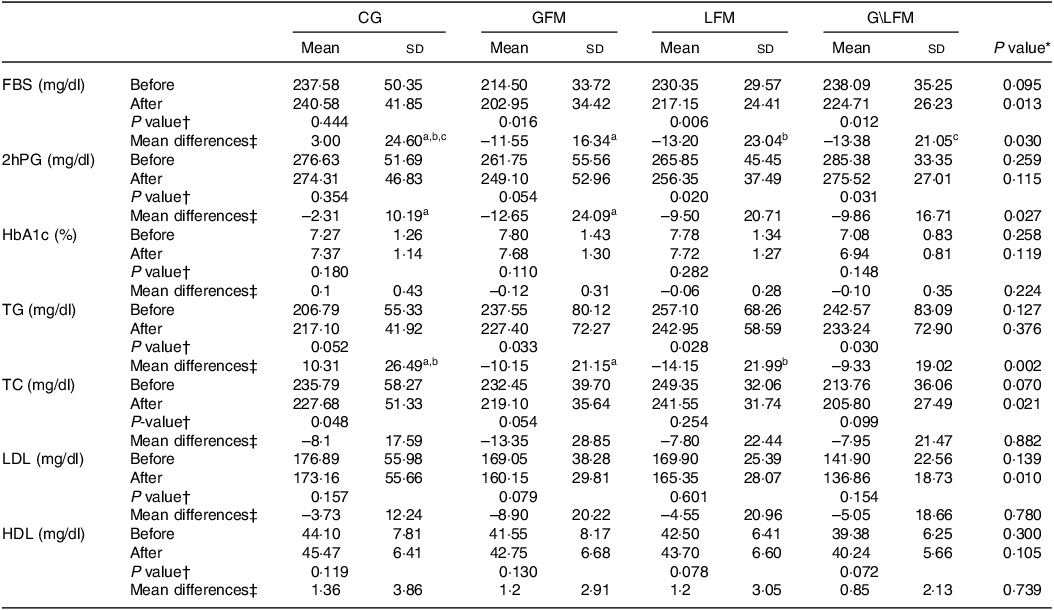
CG, control group; GFM, gain frame messages; LFM, loss frame messages; G\LFM, gain and loss frame messages; FBS, fasting blood sugar; 2hPG, 2-hour postprandial blood glucose; HbA1c, glycated Hb; TC, total cholesterol.
For before study n 22 in each group, after study n 19 for CG, n 20 for GFM, n 20 for LFM, and n 21 for G\LFM.
Data are presented as mean ± sd.
* Kruskal–Wallis test. Same superscript letters indicate between-group significant differences using Mann–Whitney U test.
† Wilcoxon signed rank test.
‡ Mean differences showed post-pre measurements.
In comparison with the CG, statistically significant differences were observed for mean changes in FBS (P for GFM: 0·037, LFM: 0·021 and G\LFM: 0·018), 2hPG (P for GFM: 0·008) and TAG (P for GFM: 0·048, LFM: 0·011).
Discussion
In the present study, the EPPM educational model has been used to educate T2DM patients. The results showed positive effects of nutritional education in the intervention groups compared with the control group and supported the results of the previous studies(Reference Hosseini-Amiri, Aliyari and Zareiyan19–Reference Boogar, Talepasand and Norouzi27). Nutrition education using the EPPM model in 3 groups (GFM, LFM and G\LFM) of diabetic patients improved knowledge and awareness of T2DM patients in comparison with the CG. In all groups, carbohydrate and fat intakes decreased, while changes in carbohydrate intakes were only significantly different between the CG and GFM groups. Moreover, nutrition education based on the EPPM model could decrease weight and BMI.
Extended parallel process model based education and knowledge and attitude
The EPPM-based nutritional education increased perceived sensitivity, perceived severity, perceived self-efficacy, perceived response efficacy and behavioural intention. In line with the results of the present study, Hosseini et al.(Reference Hosseini-Amiri, Aliyari and Zareiyan19) observed similar results after 30 d of EPPM health education on obese soldiers for weight management. Soldiers in the intervention group showed higher scores in perceived sensitivity, which indicates higher awareness of being exposed to obesity and its consequences. Individuals with diabetes were also educated by Shamsi and colleagues. Education led to increments in perceived sensitivity and perceived intensity(Reference Shamsi, Sharifirad and Kachoyee28), which supports the current study findings. Similarly, other studies stated that the EPPM model, along with other interventions, has a significant effectiveness in expanding people’s goals and performance in preventing high-risk behaviours and promoting health(Reference Hatchell, Bassett-Gunter and Clarke20–Reference Hajian, Shariati and Mirzaii Najmabadi23). Moreover, studies that examined the relationship between educating T2DM patients using the EPPM model and the level of health literacy and awareness showed higher knowledge can increase self-efficacy in patients(Reference Bohanny, Wu and Liu24–Reference Boogar, Talepasand and Norouzi27). In the present study, three approaches were performed to assess the effect of nutrition education focusing on possible harms (LFM), possible benefits (GFM) and their combinations (G\LFM) on health behaviours in individuals with T2DM. Hence, in addition to utilising LFM in a study arm, the GFM has also been examined in another arm which showed that being aware of the benefits of a healthy attitude could possibly increase the probability of changing attitude, intention and behaviour increases. Thus, EPPM-based education could possibly improve T2DM patients’ knowledge and encourage them to follow healthy behaviours and all methods of EPPM used in various intervention groups had almost the same effects and no prior style was determined according to the current study. These behavioural improvements could possibly amend diabetes outcomes and prevent further complications of the disease through dietary modifications; however, the education in some groups may pose hypersensitivity and mental effects.
Extended parallel process model based education and dietary intake
Results indicated significantly lower consumption of carbohydrates in GFM and G\LFM groups during the study. Moreover, fat consumption was significantly lower at the end of the study in LFM and G\LFM groups in comparison with baseline. Between-group comparisons showed a significant reduction in carbohydrate intake in the GFM in comparison with CG. These results are in line with the findings of the study by Zamani et al.(Reference Zamani, Akhoundzadeh and Hojjati29) Zamani et al.(Reference Zamani, Akhoundzadeh and Hojjati29) showed that EPPM education could increase the adherence to the diets and self-efficacy of patients. Other studies also supported these findings(Reference Mostajabi, Jahanishoorab and Kordi30,Reference Parsaee, Sahbaei and Hojjati31) . Mutagwanya et al.(Reference Mutagwanya, Nyago and Nakwagala32) conducted a 4-month nutritional education intervention. In this study, 4 months of intervention led to improvements in dietary habits and lifestyle which included increments in the frequency of meals, fluid and water and fruit and vegetable intakes. It was claimed that these changes are due to the increased levels of knowledge after nutritional education.
Several other nutritional education interventions have led to diet improvements including alleviating the glycaemic index of diet(Reference Ziaee, Afaghi and Sarreshtehdari33), reduction of excessive red meat consumption(Reference Fehrenbach34) and higher intake of green vegetables and fruits(Reference Sushma and Anita35). It is believed that the implementation of educational programmes for diabetic patients can be effective in their adherence to the diet. Therefore, educating how to follow a healthy diet can increase the self-efficacy of diabetic patients(Reference Parsaee, Sahbaei and Hojjati31). This is due to following a proper diet along with changing unhealthy eating habits, maintaining an ideal weight, maintaining blood sugar within a normal range, providing sufficient energy and maintaining blood lipids at optimal levels which will bring health to T2DM patients(Reference Wheeler, Dunbar and Jaacks36). The results of the present study are in line with the above-mentioned studies.
The EPPM along with the provision of preventive strategies has significant effectiveness in creating psychological immunity to refuse food over-consumption(Reference Parsai, Sahbaei and Hojjati37). In fact, this model suggests that people compare perceived threat against perceived efficacy in a complex cognitive evaluation pathway. Therefore, the interaction between threat and efficiency will be predictable(Reference Hajian, Shariati and Mirzaii Najmabadi23). Therefore, the significant difference between the intervention and CG in the present study indicated the positive effect of EPPM education on increasing nutritional knowledge and its application, which was able to have a positive effect on food intake, although this change was mainly evident in the GFM group. Thus, it can be concluded that the effect of the GFM was more in sensitising and subsequently stimulating patients for behavioural changes. Therefore, it can be seen that nutrition education through GFM in EPPM-based education could be possibly more effective in higher diet compliance, especially regarding carbohydrate consumption.
Extended parallel process model based education and anthropometric indices
The results of anthropometric evaluations showed that EPPM-based nutritional education led to a significant reduction in weight and BMI in the GFM, LFM and G\LFM groups compared with the control groups. Although weight loss and BMI improvement have been shown in several nutritional education interventions(Reference Nasser, Cook and Dorsch38–Reference Qian, Wang and Dawkins40), which are related to WHR, but the present study did not show any reduction in WHR. This result could be due to the short duration of the studies. Mostajabi et al.(Reference Mostajabi, Jahanishoorab and Kordi30) declared that EPPM education significantly reduced females’ weight in the short term, but in the long term, observations’ effectiveness of the threats of exceeded weight were not different in comparison with the control groups. Thus, it can be concluded that the duration of the education is an important factor. The within-group comparison showed WC reduction in GFM. It can be concluded that the effect of GFM in creating a greater understanding of the sensitivity and severity, and as a result, increasing self-efficacy and the intention to modify the behaviour pattern was higher than other methods.
Shahmoradi et al.(Reference Shahmoradi, Zakerkish and Latifi41) educated diabetic patients based on ‘My Plate’ guidelines. In this experiment, decreases were observed in weight, BMI, WHR and WC. The discrepancies in their finding with the current study could be due to the education method. On the other hand, Simmons et al.(Reference Simmons, Fleming and Voyle42) did not observe any changes in weight and BMI after lifestyle, physical activity and awareness intervention. Some differences in the study population can justify these differences in finding to present study. First, their population was at risk of T2DM, not T2DM mellitus, second the age range of participants could possibly affect the results. Moreover, different features of the studies including educational method, duration of education and sample size could justify the difference between results.
In addition, energy intake and dietary habits in T2DM patients are important. The reduction in energy intake could affect anthropometric indices(Reference Sadowska-Krępa, Gdańska and Přidalová43). In the current study, energy intake was insignificantly reduced in the GFM, LFM and G\LFM groups. However, weight and BMI modifications could indirectly be related to the awareness of participants in following a healthier diet and higher levels of physical activity.
Extended parallel process model based education and biochemical indices
The present study revealed that EPPM-based education caused improvements in FBS, 2hPG and TG. Based on the results of the present study, it can be interpreted that GFM creates more motivation for behavioural change in patients and this could affect glycaemic control.
Najimi et al.(Reference Najimi, Azadbakht and Hassanzadeh6) indicated that theory-based educational intervention can improve HbA1c and FBS, which in the case of FBS was in line with the present study. Kulkarni and colleagues(Reference Kulkarni, Castle and Gregory44) showed that nutritional education can reduce HbA1c levels after 3 months of intervention. Similarly, intervention done by Miller and colleagues(Reference Miller, Edwards and Kissling45) stated that 3 months of intervention can cause FBS (–18 mg/100 ml) and HbA1c (–0·5 %) reduction in T2Dm patients. Moreover, according to Jafari et al.(Reference Jafari, Pasdar and Rezaei46), using the e-learning technique has shown promising effects on FBS in comparison to traditional methods including physical activity as a part of the program. Nutrition education as an important component of diabetes management could improve clinical outcomes through enhancing dietary habits, physical activity and lifestyle behaviours(Reference Thuita, Kiage and Onyango47). Thus, for glycaemic control in T2DM patients, along with MNT, nutritional education with electronic methods could be helpful.
The effect of nutritional education on lipid profile was previously assessed. Qian et al.(Reference Qian, Wang and Dawkins40) reported TAG reduction after nutritional education in cardiovascular patients. Diehl and colleagues(Reference Diehl48) also had similar observations. Both above-mentioned studies are in line with the findings of the current study with regard to the TAG levels. On the other hand, Miller and colleagues(Reference Miller, Edwards and Kissling45) did not find any effect of nutritional education on lipid profile after 3 months of intervention. Also, after a 12-month intervention, no significant reduction was observed in lipid profile(Reference Pimentel, Portero-Mclellan and Oliveira39). These discrepancies can be justified by factors such as educational method, sample size, study duration and study population.
The reduction in the TAG levels in the intervention groups, especially in the LFM group, and elevation in CG could be due to a decreasing trend in simple carbohydrate and fat consumption during the study as the education focused on improving dietary habits. This finding has been reported in other studies similarly(Reference Nasser, Cook and Dorsch38,Reference Miller, Edwards and Kissling45) .
Nutrition education is the most basic way to achieve changes in eating habits, and it can be effective in improving individuals’ knowledge, attitude, practice. But, it should be noted that in order to change biochemical indicators, it is necessary to carry out the interventions for a longer period. Moreover, weight loss during the study period was effective in TAG reduction.
As it was observed, only in the GFM group, a significant decrease in all three indicators of FBS, 2hPG and TAG occurred. On the other hand, carbohydrate intake in the GFM group had a significant and more obvious decrease than other groups and since carbohydrate intake is an important factor affecting the level of all three biochemical indicators, these could justify the better results observed in the GFM group. In fact, it may be possible to conclude that in this study, the effect of GFM in sensitising and increasing motivation for changes in behaviour (diet modification, increasing physical activity, etc.) was greater, and it could be effective in improving essential blood indicators for T2DM patients, including FBS, 2hPG and TAG. It was observed that the effects of GFM or LFM depend on the nature of behaviours. Less risky behaviours such as dietary habits could be affected more by GFM rather than LFM(Reference Pavey and Churchill49). Thus, this could possibly justify the better results seen in the GFM group in the current study.
Most of the previous studies using the EPPM model investigated the effect of LFM on the various indicators including anthropometric and biochemical variables and nutrient intake. In this study, in addition to examining the effect of threat and arousal of fear (LFM), the effect of encouragement (GFM) and their combination (G\LFM) have also been investigated. In fact, in this study, the effects of GFM and LFM, once separately from each other and once in combination (G\LFM), were investigated more widely.
This study had some strengths and limitations. In the present study, interventions were done on middle-aged T2DM patients. This is while the prevalence of T2DM is higher in older adults and elderlies. However, receiving nutrition education at younger ages could help in better management of diabetes in older ages. Also, the comprehensive examination of the effectiveness of the educational intervention in the present study on the state of knowledge and attitude, self-efficacy and intention of the individuals, anthropometric factors, physical activity status, nutrient intakes and finally biochemical indicators are other strengths of the present study. Providing training without the need for face-to-face meetings and using messengers can be another strength of this study, which despite many problems, also has many advantages, especially due to the convenience and ease of access to training for the participants. Hence, due to the aforementioned advantages, nutrition education via virtual media and social media platforms could be highly popular in the future, which is recommended for further studies. One of the important limitations of this study is the relatively short follow-up period, which suggests conducting studies with a longer period of time in this field. The reluctance of some patients to participate in the study due to the lack of enough time to complete the questionnaire and receive the educational content was another limitation of this study, which was partly due to the explanation of the purpose of the study, the use of messengers and electronic tools to provide training, choosing the right time for completing the questionnaire in person, as well as frequent follow-ups of the participants under study by phone. Another limitation is that the study was conducted in a small city in Fars province, and the results should be interpreted with caution. Therefore, for the generalisability of the findings, it is suggested to conduct studies in other cities as well. Another limitation of this study was the limited age range of the research samples. Considering that other age groups, including the young and the elderly, are also prone to diabetes, it is better to conduct a study in other age groups and investigate the effect of this method of educational intervention. On the other hand, it is possible that individual situations such as fatigue, anxiety and mental state have some effects on how to answer the research questions, which was out of the researcher’s control. Another limitation of the study is the importance of measuring insulin and its related indicators, which were excluded from the study due to budget limitations.
Conclusion
After 3 months of conveying nutritional education via GFM, LFM and G\LFM based on EPPM, the knowledge and awareness of T2DM patients raised in comparison with the CG. Nutritional education was shown to be effective in lowering dietary carbohydrate and fat intakes, while intake reduction for carbohydrates was only significantly different between GFM and CG groups. In addition, EPPM-based nutritional education was able to reduce weight and BMI. EPPM-based nutritional education could be possibly a beneficial cost–benefit approach in T2DM as a part of their medical nutrition therapy. Further studies with higher sample sizes and durations and in various populations are proposed to reach concise results.
Acknowledgement
The authors would like to thank the participants of the study for taking part in this research. This study was extracted from the master thesis by Tayebe Dehghan and supported by Shiraz University of Medical Sciences, Shiraz, Iran (Grant number: 23033).
The study was supported by Shiraz University of Medical Sciences with the grant number: 23033.
T. D.: Research idea, study design, data acquisition, data interpretation and writing and preparation of the manuscript. M. A. M.: Data interpretation, writing and preparation of the manuscript and critical revision of the manuscript. M. K.: Research idea, study design, data acquisition, data interpretation and critical revision of the manuscript. M. M.: Research idea, study design, data acquisition, data interpretation and critical revision of the manuscript. M. Z.: Research idea, study design, data analysis and interpretation, critical revision of the manuscript. M. A.: Research idea, study design, data interpretation and critical revision of the manuscript. A. K.: Data acquisition, data interpretation, critical revision of the manuscript. F. F.: Data acquisition, data interpretation and writing and preparation of the manuscript. Z. S.: Research idea, study design, data acquisition, data interpretation and writing and preparation of the manuscript.
There are no conflicts of interest.







