



The ability of a muscle to apply force and generate active tension is defined as muscle strength(Reference Gaines and Talbot1). Muscle strength is an important marker of health that is associated with cardiometabolic risk(Reference Chong, Choi and Kong2–Reference Ramírez-Vélez, Correa-Bautista and Lobelo4). In addition, when muscle mass and strength fall below a threshold, sarcopenia is diagnosed, which leads to physical disability, mobility limitations, falls, institutionalisation and death(Reference Cruz-Jentoft, Baeyens and Bauer5). Although the ageing process is associated with a progressive and general decrease in muscle mass and strength, because of numerous contributing factors, such as food and levels of physical activity, there is no specific age at which muscle mass and strength start to decline. It makes all the age groups including the adults vulnerable to muscle loss(Reference Mitchell, McGregor and D’Souza6).
Dietary factors, along with several other contributors, seem to have a role in the strength and the capacity of muscles(Reference Shahinfar, Shahavandi and Tijani7). The contents of food modulate the process of methylation, which seems to be vital for the ability, differentiation and regeneration of the muscles(Reference Kato, Takegami and Seki8,Reference Naito, Mori and Inagawa9) . Betaine, choline, methionine, vitamin B12, vitamin B6 and folate are all considered methyl donors. Vitamin B6 catalyses processes in the folate cycle and trans-sulfuration pathway, whereas vitamin B12 serves as a cofactor for methionine synthetase, tying the methionine and folate cycles together, which might have an indirect effect on muscle strength(Reference Clare, Brassington and Kwong10,Reference Vordenbäumen, Sokolowski and Rosenbaum11) . Choline and methionine are involved in the synthesis of neurotransmitters such as acetylcholine which is a neurotransmitter critical for transmitting signals between nerves and muscles, influencing muscle contraction and, subsequently, strength(Reference Tardy, Pouteau and Marquez12).
Clinical studies have observed associations between deficiencies in methyl donor nutrients and conditions affecting muscle health, such as myopathies and muscle weakness(Reference Veeranki and Tyagi13,Reference Majumder, Behera and Jeremic14) . The modern diet may be deficient in methyl donors(Reference Likes, Madl and Zeisel15). According to several studies, 2·5–5 g of betaine per d, diet or supplementation, may be useful for improving body composition and muscle function(Reference Cholewa, Guimaraes-Ferreira and Zanchi16,Reference Cholewa, Paolone and Wood17) . Besides that, according to research, betaine may increase creatine synthesis by attaching a methyl group to guanidinoacetate through methionine, impactfully enhancing muscle strength(Reference Du Vlgneaud, Simmonds and Chaudler18), although a recent meta-analysis highlighted the lack of evidence for a clear impact of supplementation with betaine on strength and performance(Reference Ismaeel19). In addition, another study revealed that the consumption of vitamin B12, B6 and folate might be correlated with improved functional outcomes in older adults, which in turn strengthens the thesis that an increased intake of methyl donors might favour enhanced muscle strength(Reference Behrouzi, Grootswagers and Keizer20). This can be further observed in a study on aged adults which manifested a higher consumption of the sources of vitamin B6 such as fish and fruit was associated with a lower risk of impaired mobility(Reference Struijk, Lana and Guallar-Castillón21).
Only a few studies looked into the relationship between methyl donor micronutrients and muscle strength worldwide, and to the best of our knowledge, these studies have largely focused on a single methyl donor nutrient(Reference Ismaeel19,Reference Moretti, Paoletta and Liguori22–Reference Marchenkova, Makarova and Vasilieva24) . Therefore, this study aimed to evaluate the association between the consumption of methyl donor micronutrient score (MDMS) and muscle strength.
Methods
Study population
In this cross-sectional study, 270 adults (118 men and 152 women) with an age range of 18–75 years, who were living in Tehran, Iran, were enrolled. The following formula was used to determine the sample size depending on the correlation coefficient(Reference Scott, Blizzard and Fell25,Reference Ng, Hairi and Jalaludin26) :
 $$N\, = \,\left( {\left( {z1\, - \,\alpha /2\, + \,z1\, - \,\beta \, \times \,\surd \left( {1 - r2} \right)} \right)2/{r^2}} \right)\, + \,3$$
$$N\, = \,\left( {\left( {z1\, - \,\alpha /2\, + \,z1\, - \,\beta \, \times \,\surd \left( {1 - r2} \right)} \right)2/{r^2}} \right)\, + \,3$$
The computed correlation coefficient was found to be r = 0·37(Reference Scott, Blizzard and Fell25,Reference Ng, Hairi and Jalaludin26) . We set the error type 1, α = 5 %, and the statistical power, 1-β = 95 %, resulting in N 135. However, 270 subjects were enrolled in this study due to a potential drop in the number of participants. Recruitment was performed via advertising and distribution of flyers from February 2018 to July 2019. People were encouraged to participate in the study for a free scientific weight gain or weight loss dietary plan if they wished to at the end of the study. The following eligibility criteria were considered for participation: (1) age range of 18–75 years, (2) no history of alcohol or drug abuse and (3) mere absence of particular weight loss and weight gain diets, chronic diseases concerning the muscles including kidney, liver and pulmonary disease, diabetes, hormonal and CVD, infectious or inflammatory diseases, pregnancy and lactation in women, usage of any special medication or supplements, malnutrition, inability to take the test, arthritis, and other complications of joint and disability. A multi-stage cluster random sampling method was used to select health centres from the five regions (north, south, west, east and centre) of Tehran. Right centres were selected from each region randomly. Finally, by dividing the sample size by the total quantity of healthcare centres, the number of participants in each healthcare centre was calculated. Participants were informed about all the needed procedures along with the project after signing a written informed consent before the start of the study. The study protocol was according to the ethical standards of the Tehran University of Medical Sciences (Ethics Number: IR.TUMS.VCR.REC.1396.4085).
Data collection
Participants completed a questionnaire designed to collect the information regarding participants’ demographic (age, education and marital status) and lifestyle (smoking, regular alcohol consumption and physical activity) status. Experienced researchers interviewed the subjects via these questionnaires.
Physical activity
We used a validated short form of the International Physical Activity Questionnaire (IPAQ) to evaluate the level of physical activity for each participant and then categorised them into three levels of physical activity according to calculated metabolic equivalents (MET): these levels consisted of low (<600 MET min/week), moderate (600–3000 MET min/week) and high (>3000 MET min/week)(Reference Moghaddam, Aghdam and Jafarabadi27,Reference Wareham, Jakes and Rennie28) .
Blood pressure
A digital sphygmomanometer (BC 08) was used to assess the blood pressure of each participant in a sitting position after a rest period of 10–15 min. This procedure was repeated for a second time, and the means of two assessments were used in the final analyses for systolic blood pressure and diastolic blood pressure.
Anthropometrics and body composition
The height of the participants was measured by a wall-mounted stadiometer with a precision of 0·1 cm while standing in a normal position without shoes (Seca). Weight was measured by a digital scale with a sensitivity of 0·1 kg (Seca 808, Seca), with light clothes on. BMI was calculated as weight per square of height. Waist circumference was measured, to the nearest 0·1 cm, at the centre of the inferior edge of the rib cage and the superior aspect of the iliac crest, using non-elastic tape. To calculate the waist:hip ratio, hip circumference was measured using a flexible anthropometric tape with a precision of 0·1 cm, in the correct horizontal location at the highest level from the lateral facet over a thin dress without any pressure on the body surface. A body composition analyser (InBody 720, Biospace) was utilised for the measurement of fat mass and fat-free mass.
Muscle strength
Muscle strength was estimated by a digital handgrip dynamometer (Saehan, model SH5003, Saehan Corporation). In a vertical position, with their forearm and arm positioned normally beside the body and an elbow arc of 180 approximately, participants were requested to squeeze the dynamometer as hard as they can to calculate the maximal force for each hand. The process was repeated three times with each hand, and in total, handgrip strength was measured six times. The mean muscle strength (MMS) was calculated using the mean score from both hands(Reference Vaz, Thangam and Prabhu29).
Dietary intake
We used a validated 168-item semi-quantitative FFQ to obtain data about the dietary intake of the subjects(Reference Ayoubi, Yaghoubi and Pahlavani30). FFQ used to assess the dietary intake of the Iranians have generally acceptable validity and reproducibility. In order to determine the daily intake of each dietary ingredient, we took into account the serving size and the reported average frequency during the prior year on a daily, weekly, monthly or yearly basis. Utilising the nutrient content of Iranian food items, Nutritionist IV software (First Databank) was used to determine the mean energy and nutrient intakes for each study participant.
Methyl donor micronutrient score
MDMS was calculated using the method constructed by Lotfi et al.(Reference Lotfi, Keshteli and Saneei31). The dietary intake of six methyl donor micronutrients, vitamin B6, vitamin B9, vitamin B12, betaine, choline and methionine, was obtained from FFQ using Nutritionist IV software. Participants were divided into energy-adjusted deciles of each methyl donor nutrient intake. Participants in the first decile of each of these nutrients received a score of 1, whereas those in the last decile received a score of 10 for each of the six mentioned nutrients. Scores for the other deciles were calculated as well using the exact same method. Finally, to create a total MDMS, we summed up each micronutrient score for each subject. The final scores of MDMS for each participant ranged from 6 to 60.
Statistical analysis
We used the residual model to compute energy-adjusted intakes of each methyl donor micronutrient(Reference Willett, Howe and Kushi32). Participants were categorised into quartiles of MDMS. The Statistical Package for the Social Sciences (SPSS version 26, SPSS Inc.) was used to perform all of the statistical analyses. We analysed the study participants’ characteristics according to MDMS quartiles, using one-way ANOVA to compare continuous variables and χ2 tests for categorical variables. The ANCOVA was used to compare nutrient intake and muscle strength across quartiles of the MDMS, adjusting for likely confounders, such as age (years), sex (men/women), education (diploma and under-diploma/higher educated), occupation (employed/unemployed), marriage (single/married), smoking(no/current/quit), the fat mass (kg), physical activity (low/moderate/high), supplement intake (yes/no), dyslipidaemia (yes/no) and energy intake (kcal/d). Finally, we employed the forward stepwise linear regression model to assess the linear association of MDMS with muscle strength while adjusting for confounders. A multi-collinearity test was conducted with variance inflation factors. Multi-collinearity was considered high when the variance inflation factor was >10(Reference Slinker and Glantz33). P < 0·05 was considered statistically significant.
Results
Two men and one woman were excluded at the end because of missing data. The mean age of participants was 36·8 ± 13·2 years with an average BMI of 25·6 ± 4·68 kg/m2. The general characteristics of participants, across the quartiles of MDMS, are presented in Table 1. The study sample included 267 subjects (116 men and 151 women) with a mean age of 36·6 years. Individuals in the top quartile of MDMS, when compared with the first quartile, were significantly higher educated and more physically active and had a higher rate of dietary supplement intake.
Table 1. General characteristics of study participants across quartiles of methyl donor intake
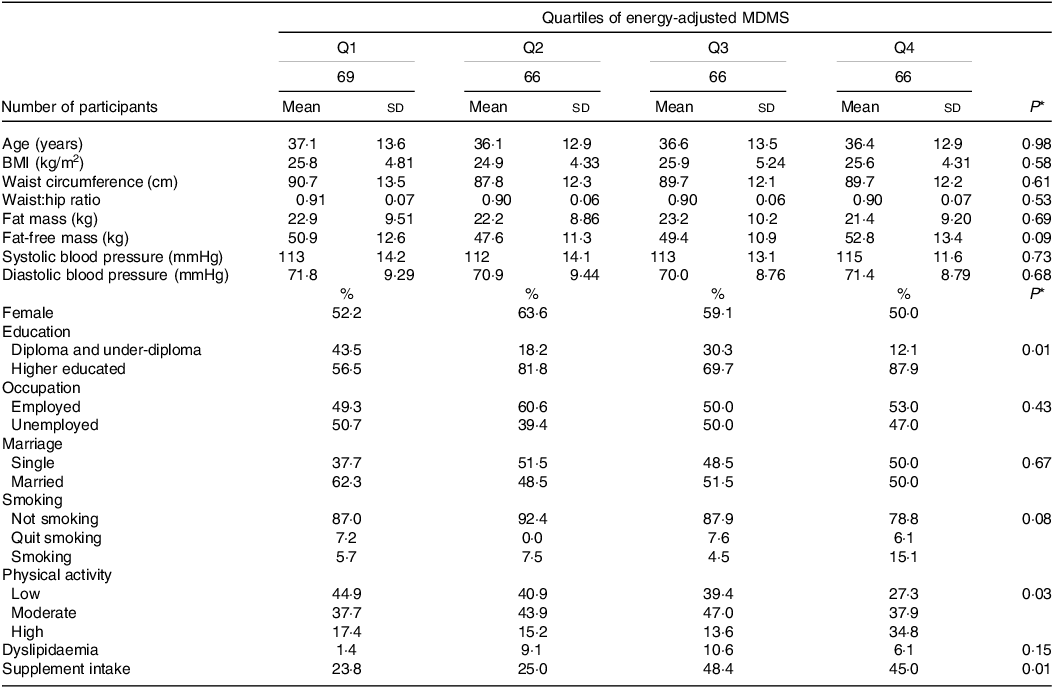
MDMS, methyl donor micronutrient score; Q, quartile.
*P values result from ANOVA for quantitative variables and χ2 test for qualitative variables, statistically significant if <0·05.
Daily intakes of selected nutrients of study participants across quartiles of MDMS are shown in Table 2. The intake of all methyl donor micronutrients increased significantly across quartiles of MDMS with the expectation of betaine. Individuals in the last quartile of MDMS had significantly higher intakes of proteins, cholesterol, Ca, Mg, Zn, vitamin A, vitamin C, vitamin D, vitamin B2, vitamin B3, dietary fibre, meat and dairy products, compared with participants in the first quartile. In contrast, those in the lowest quartile of MDMS had significantly higher intakes of carbohydrates and grains, compared with people in the first quartile.
Table 2. Multivariable-adjusted daily dietary intakes of selected nutrients of study participants across quartiles of methyl donor intake
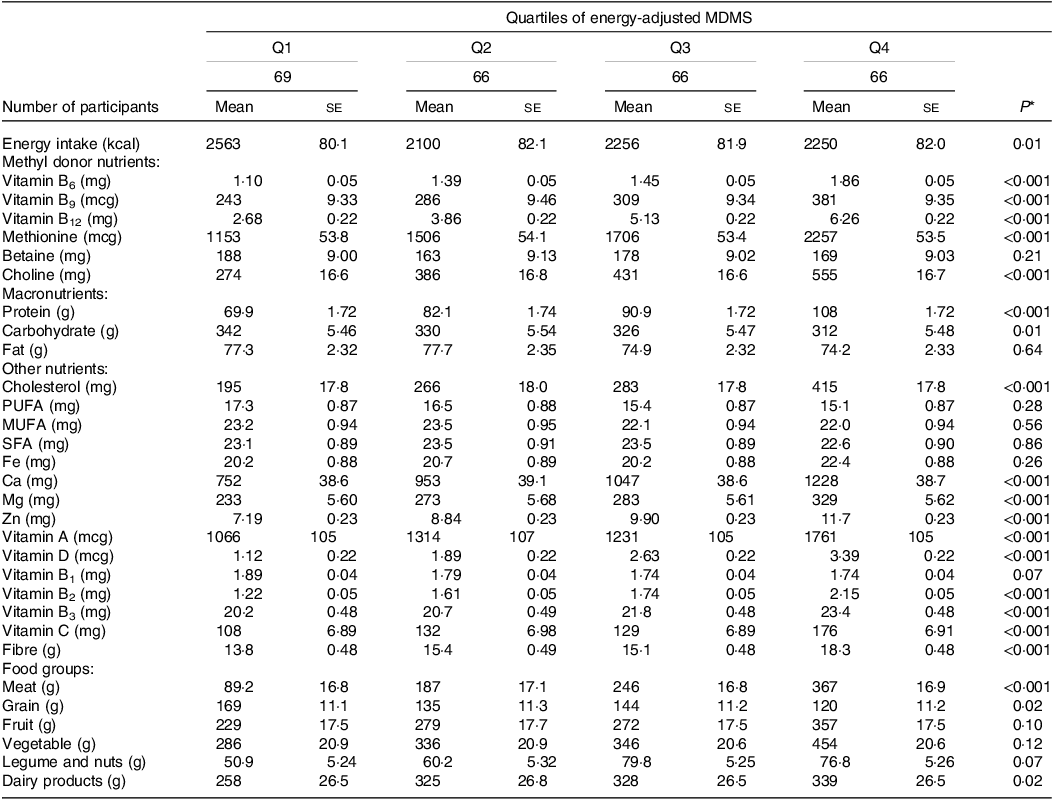
MDMS, methyl donor micronutrient score; Q, quartile.
Energy intake is adjusted for age and sex; all other values are adjusted for age, sex and energy intake.
*Obtained from ANCOVA, statistically significant if <0·05.
Table 3 shows the MMS across quartiles of MDMS. There was a significant increase in MMS of the left hand (MSL) after the adjustment for potential confounders, but the MMS of the right hand (MSR) and MMS did not differ significantly in quartiles of MDMS.
Table 3. Muscle strength by quartiles of methyl donor intake

MDMS, methyl donor micronutrient score; Q, quartile; MSL, mean muscle strength of the left hand; MSR, mean muscle strength of the right hand; MMS, mean muscle strength.
Adjusted for age, sex, education, occupation, marriage, smoking, fat mass, physical activity, supplement intake, dyslipidaemia and energy intake.
*Obtained from ANCOVA, statistically significant if <0·05.
Crude and multivariable-adjusted β-coefficients of MMS across quartiles of the dietary methyl donor micronutrient intake are presented in Table 4. No significant association was observed between methyl donor micronutrient intake and MSL, MSR, and MMS in the first two models; however, after adjusting for all potential confounders including age, sex, education, occupation, marriage, smoking, fat mass, physical activity, supplement intake, dyslipidaemia and energy intake, we found a significant association between the dietary methyl donor micronutrient intake and MSL (β: 0·09, 95 % CI 0·02, 0·17, P = 0·03) and MMS (β: 0·08, 95 % CI 0·00, 0·16, P = 0·04).
Table 4. The relationship between muscle strength and methyl donor intake
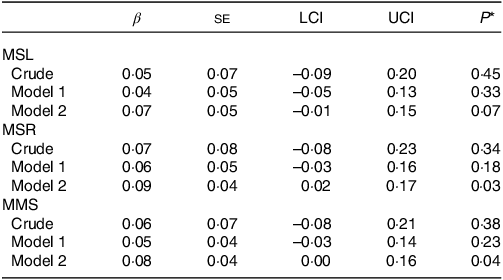
LCI, lower confidence interval; UCI, upper confidence interval; MSL, mean muscle strength of the left hand; MSR, mean muscle strength of the right hand; MMS, mean muscle strength.
Model 1 adjusted for age, physical activity level, smoking and sex; model 2 adjusted for age, sex, education, occupation, smoking, dyslipidaemia, supplement intake, total energy, BMI and physical activity level.
*Obtained from linear regression, statistically significant if <0·05.
Discussion
To the best of our knowledge, this is the first study that investigated the relationship between methyl donor micronutrients including vitamin B6, vitamin B9, vitamin B12, betaine, choline, and methionine and muscle strength. In the current study, a significant positive association was observed between the dietary methyl donor micronutrient intake and MSR and MMS.
In several studies, the effect of methyl donors on physical performance has been investigated. Gage et al. probe the acute effect of choline-based multi-ingredient supplements on physical performance. In this randomised double-blind crossover trial, the choline-based multi-ingredient supplements or a placebo was administered to the fourteen male college football players (20·4 ± 1·0 years old) 60 min before the physical performance tests, including maximum vertical jumps, maximum voluntary isometric contractions, maximal voluntary concentric contractions and fatiguing contractions, for 7 d. According to the findings, acute supplementation showed no improvements in vertical jump height, strength, power, muscle contractile properties and voluntary activation at baseline, but the rate of torque development and impulse was higher in the group that received the supplement than in the placebo group during fatiguing contractions (P = 0·018, P < 0·001, respectively)(Reference Gage, Phillips and Noh34).
The results of studies for betaine were conflicting. In a study conducted by Moro et al., the effect of betaine consumption on body composition and muscle performance during CrossFit training was investigated. The results showed no significant difference between the two groups (betaine (n 14) and placebo (n 15) groups) after 6 weeks(Reference Moro, Badiali and Fabbri35). In another study, betaine supplementation for 14 weeks in young professional soccer players showed improved projected muscular strength, maximal oxygen uptake and repeated sprint ability performance(Reference Nobari, Cholewa and Castillo-Rodríguez36).
In line with our study, Grootswagers et al. revealed positive associations between vitamin B6 intake and chair rise test times in a group of healthy European older people and handgrip strength in those with low levels of physical activity. No indication of a connection between niacin intake, vitamin B12 intake, or folate intake and physical performance, or a connection between niacin status and homocysteine concentrations, was discovered in this investigation(Reference Grootswagers, Mensink and Berendsen37). In another study, the relationship between diet and handgrip strength was investigated in 68 002 participants (age 63·8 ± 2·7 years, 50·3 % women, 49·7 % men) from UK Biobank; the intake of oily fish, retinol and Mg had a positive relationship with grip strength in both sexes, while carbohydrate intake was found to have negative associations. A positive correlation was discerned between some nutrients similar to red meat, fruits and vegetables, vitamin E, Fe, vitamin B12, folate, and vitamin C and grip energy in women. Bread and processed meat were only associated with weaker grip strength in men(Reference Gedmantaite, Celis-Morales and Ho38). Other studies have also shown a positive relationship between serum folate and vitamin B12 concentrations and muscle strength and handgrip strength(Reference Ao, Inuiya and Ohta39–Reference Zhang, Sun and Li42).
Although the molecular mechanisms remain unknown, one of the mechanisms that can play a role in improving muscle strength and power is the transmethylation of homocysteine(Reference Williams and Schalinske43). According to research, betaine may increase creatine synthesis by attaching a methyl group to guanidinoacetate through methionine(Reference Du, Simmonds and Chaudler44), and betaine can also affect hormones in the body and signalling proteins in the muscles, for example, by reducing homocysteine and homocysteine thiolactone, betaine may increase muscle protein synthesis(Reference Ismaeel19). Mammalian mitochondria use folate-bound one-carbon moieties to methylate transfer ribonucleic acids in mitochondrial translation and oxidative phosphorylation. Disruption of whole-cell folate metabolism impairs the respiratory chain(Reference Morscher, Ducker and Li45). Consuming folic acid increases vascular conductance, which enhances blood flow in the working skeletal muscle of older people. These results support the therapeutic use of folic acid to increase blood flow to the skeletal muscles, and maybe exercise and functional ability, in human primary ageing(Reference Romero, Gagnon and Adams46).
This is the first study that investigates the relationship between dietary intake of methyl donor micronutrients and muscle strength not only in Iran but also in a universal aspect. Moreover, all data were gathered by experienced dietitians and assessed using validated questionnaires for better accuracy. Furthermore, a variety of potential confounding factors were considered in the analysis. We used handgrip as a proxy for overall skeletal strength. The muscles used in handgrip are distributed across the forearm and hand, and their strength is indicative of the overall muscle strength in these areas. Additionally, handgrip strength correlates well with strength in other muscle groups throughout the body(Reference Trinidad-Fernández, González-Molina and Moya-Esteban47). Also, the measurement of handgrip strength is non-invasive and does not require complex or expensive equipment. This makes it a practical choice for large-scale studies, screenings and routine health assessments. The obvious limitations of the present study include the cross-sectional nature of the study, which precludes the ability to suggest a causal relationship between methyl donor micronutrients and muscle strength. Also, there might be small errors in the dietary assessment, mostly due to misremembering the data and misclassification errors by using FFQ. Moreover, there is no biomarker for determining the overall methyl donor micronutrient intake more exclusively than FFQ as a proxy measure indicator. Additionally, some residual variables may still have an impact on the outcomes even after various confounders have been taken into account. Earlier studies have shown a correlation between the MDMS and a number of diseases, but the score has not been formally validated in our study population. Further randomised controlled trials and cohort studies are needed to confirm the veracity of our findings.
Conclusions
In conclusion, we found that a high intake of methyl donor micronutrients may be related to higher MMS, particularly in the right hand. As a result, more dietary sources of methyl donor micronutrient intake could be used to maintain and enhance muscle strength in people. Whole grains, a potent source of betaine and methionine, are rarely consumed in the Iranian community. Also, other methyl donor-rich food groups including dairy products, fish and nuts need to be consumed more frequently. A higher intake of these groups may lead to better muscle strength and overall health. For the confirmation of our results, experimental studies are necessary.
Acknowledgements
The authors thank all those who participated in this study.
A. M. and S. S-B. contributed to the conception/design of the research; N. B. and S. D. contributed to the acquisition, analysis or interpretation of the data; A. M., P. R. and M. C. drafted the manuscript; S. S-B. and K. D. critically revised the manuscript; and S. S-B. agreed to be fully accountable for ensuring the integrity and accuracy of the work. All authors read and approved the final manuscript.
The authors have no relevant financial or non-financial interests to disclose.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethical Committee of Tehran University of Medical Sciences (IR.TUMS.MEDICINE.REC.1400.375). All participants signed a written informed consent prior to the start of the study.
The authors give their consent for the publication of identifiable details, which can include photograph(s) and/or videos and/or case history and/or details within the text (‘Material’) to be published.
The datasets generated and/or analysed during the current study are not publicly available due to the privacy of the data but are available from the corresponding author upon reasonable request.




