


The so-called Mediterranean diet has been proposed as a model for a healthy diet(Reference Willet, Sacks and Trichopoulou1–Reference Keys3). Although the common denominator in Mediterranean countries is a high consumption of olive oil, important differences nevertheless exist concerning overall mortality and mortality associated with coronary disease. These differences have been attributed to variations in social, religious and cultural customs that confound associations between health and diet and the risk for disease(Reference Hu4). Over the second half of the 20th century, the populations of industrialised countries markedly increased fat intake. Although this increase has coincided in time with a rise in the prevalence of obesity, diabetes mellitus and CVD(Reference Willett5), a causal role of dietary fats in the development of these conditions has been much debated(Reference Willett5, Reference Bray and Popkin6). Most public-health programmes in Western countries have aimed at reducing the proportion of energy obtained from fat in the diet to below 30 %, an objective that should be very difficult to achieve in Mediterranean countries unless the intake of olive oil is reduced(Reference Serra-Majem, Ngo de la Cruz and Ribas7). In fact, nutritional recommendations are contradictory, as, on the one hand, they propose to reduce the amount of dietary fats and, on the other hand, to increase vegetable fats. Moreover, the recommendations on fats rich in PUFA are sometimes contradictory and the public are urged to consume less overall fat but more fats rich in MUFA, without taking into consideration the source of fat (virgin or refined olive oil, high oleic sunflower oil, etc)(Reference Alvarez de Cienfuegos, Badimon and Barja8). However, countries around the Mediterranean basin have witnessed important social, cultural and economic changes that have greatly influenced dietary habits(Reference Soriguer, Rojo and Rodriguez9).
Studies carried out in Spain have shown that persons who consume a greater proportion of olive oil consume foods that differ from those consumed by people using less olive oil(Reference Serra-Majem, Ngo de la Cruz and Ribas7). However, many studies on the intake of fats have been based either on 24 h food records, which have a poor sensitivity for representing the type of fatty acids consumed, or on FFQ, which reflect what people have bought or what they believe they consume, but not what they really consume(Reference Willett5). Additionally, the information a person has about the type of fat used in food is not always adequate, and during the cooking process, important changes are produced resulting in differences between what people say they consume and what they do, in fact, consume. In the present study, we considered the home kitchen as an uncontrolled experimental laboratory where important changes occur in the composition of the fats that are actually consumed. The aims of the study were: (1) to evaluate in a Mediterranean population the precision in people's awareness of the type of fat consumed, and the influence of food handling on the composition and quality of the fat, and (2) to assess the sociocultural and health profile of persons who preferentially consume olive oil.
Material and methods
Baseline study
The baseline study was undertaken in Pizarra, an inland town of 6600 inhabitants (5000 aged 18–65 years) located some 30 km (20 miles) from the city of Malaga, in southern Spain. The study characteristics have been reported in detail elsewhere(Reference Soriguer, Esteva and Rojo10, Reference Soriguer, Rojo-Martínez and Almaraz11). Fig. 1 shows the flow of participants in the study. Exclusion criteria included people who were institutionalised, pregnant women and persons with a severe clinical problem or psychological disorder. The final sample distribution by age and sex was not significantly different to the distribution of the general population.
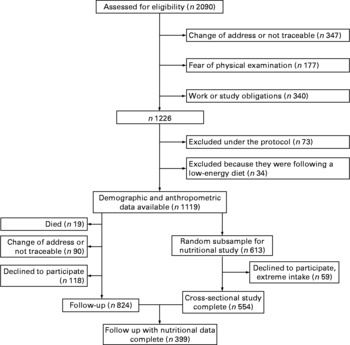
Fig. 1 Pizarra study sampling chart.
Follow-up
The cohort was re-evaluated 6 years later in 2003–2004. Persons who had completed the baseline study (n 1119) were invited by letter or by phone to attend another clinical and anthropometric examination (Fig. 1).
Procedures
Both at baseline and at follow-up, all participants underwent an interview and a standardised clinical examination. In addition, several home visits were made to the participants to collect nutritional data. The same methodology was used for both the baseline and the follow-up studies. Data were recorded on education (no studies, primary education, secondary education or apprentice training and university studies), smoking (current smoker of more than one cigarette per day) and the degree of physical exercise: slight (sit down or stand almost all day without walking), moderate (frequent walking with light loads) or intense (strenuous physical effort). Measurements were made of weight and height, and BMI was calculated as weight in kg divided by height in square metres. A fasting blood sample was drawn at baseline and the serum stored at − 70°C for later analysis.
The protocol was approved by the Ethics and Clinical Research Committee of Carlos Haya Hospital. All participants provided written informed consent.
Composition of serum fatty acids
The fatty acid composition of serum phospholipids was determined as described(Reference Soriguer, Rojo and Dobarganes12). Briefly, after extraction of serum fat with chloroform–methanol (2:1) and butylated hydroxytoluene at 0·025 %(Reference Soriguer, Gonzalez-Romero and Esteva de Antonio13) and phospholipid separation by TLC, fatty acid methyl esters were formed by heating the extracted fat for 30 min with 0·61 m H2SO4 in anhydrous methanol. After extraction with hexane, fatty acid methyl esters were analysed in a Hewlett–Packard chromatograph, equipped with a flame ionisation detector and using a BPX75 fused-silica capillary column (SGE, Villebon, France).
Evaluation of food intake
For the baseline study, 554 persons completed a prospective, 7 d quantitative food questionnaire at two different times during the year as well as a FFQ. We used questionnaires previously validated in a similar population(Reference Mataix, Garcia and Mañas14).
The surveys were given by experienced dietitians previously trained for this project. After making an appointment by telephone, the dietitians handed over the questionnaire in the home of the participant and provided information about the nature of the survey. The questionnaires were collected from the homes 7 d later, at which point any doubts about completing the questionnaire were resolved. Photographs were used for determinate portion sizes. The transformation to energy and macronutrients was done by a computer program that included the composition of local foods based on food composition studies, previously done by some of the authors(Reference Soriguer, Serna and Valverde15, 16). For the follow-up study, 399 out of the 554 persons whose nutritional habits had been studied at baseline completed the same quantitative and FFQ, following the same procedure as before.
At the baseline study, four samples of cooking oil being used for frying were obtained from the kitchens of the participants at four different times of the year. For the second study, the samples were obtained only once.
Composition and quality of the fats used for frying
The fatty acids from frying fats were analysed by gas chromatography after derivatisation to fatty acid methyl esters with 2 m KOH in methanol and triheptadecanoin as an internal standard, according to the IUPAC standard method(Reference Wolf, Mordret and Dieffenbacher17). A HP 6890 chromatograph on a HP Innowax capillary column (Hewlett–Packard, Palo Alto, CA, USA) was used. Polar compounds were quantified by adsorption chromatography following the IUPAC standard methods 2.507(Reference Firestone, Perkins and Erickson18). TAG polymers were quantified by high-performance size exclusion chromatography following the IUPAC standard method(Reference Kleimbaun, Kupper and Keith19).
After analysis, samples were classified according to two criteria: fatty acid composition and level of polar compounds. Three groups of oils were defined: oils having levels of linoleic acid higher than 50 % were classified as sunflower oils (this is the seed oil principally commercialised and used in Spain), oils having less than 25 % linoleic acid were classified as olive oils, while those containing between 25 and 50 % linoleic acid were classified as mixtures. Two levels of polar compounds were considered in the present study, depending on whether they were higher or lower than 20 %. This value was selected as indicative of significant degradation, because current official regulations in Spain establish that frying fats and oils have to be discarded for human consumption when polar compound levels are close to 25 %(Reference Kleimbaun, Kupper and Keith19).
Statistical analyses
The results are presented as mean, standard deviation and proportions. The hypothesis contrast for qualitative variables was performed with the χ2 test and for continuous variables with Student's t test or ANOVA statistics. The concordance between discrete variables was calculated with the κ index. The strength of associations between one variable (dependent) and other potentially explanatory variables was measured by calculating the OR from the regression coefficients of a multivariable logistic model. The criteria of Kleimbaun et al. (Reference Miettinen20) were followed for the inclusion of the independent variables, and 95 % CI were calculated by the method of Miettinen(Reference Nestle21). In all cases, the level of rejection of a null hypothesis was α = 0·05 for two tails.
Results
Macronutrient intake
No significant sex differences in age or BMI were detected in the baseline study. As expected, men consumed greater daily amounts of carbohydrate, protein and fat than women. The proportion of energy from protein and carbohydrate was similar in men and women, but the overall contribution of fats to daily energy intake was significantly greater in women, at the expense of MUFA and n-3 fatty acids (Table 1). BMI increased during the 6-year follow-up, but energy intake decreases in both sexes. This decrease was at expense of carbohydrate and PUFA, while MUFA increased significantly.
Table 1 Age, BMI and intake of macronutrients in the study population at baseline and after a 6 year follow-up
(Mean values and standard deviations)

% En, nutrient intake as percentage of daily energy.
* P value, ANOVA for repeated measures with adjustment by sex.
Influence of diet on the fatty acid composition of serum phospholipids
The composition of SFA, MUFA and n-3 fatty acids in serum phospholipids was significantly associated with age and the type of cooking oil used, especially MUFA, which were significantly higher in persons using olive oil for frying (Fig. 2).

Fig. 2 Concentration of fatty acids (SFA, n-6, MUFA and n-3) in serum phospholipids according to age and type of oil commonly used in the kitchens. All P values are ANOVA. (a) Oil type, NS; sex, NS; age, < 0·001. (b) Oil type, < 0·001; sex, NS; age, < 0·001. (c) Oil type, < 0·05; sex, 0·03; age, NS. (d) Oil type, NS; sex, NS; age, < 0·001 (●, olive oil; ○, mixed oils; △, sunflower oil).
Serum n-3 fatty acids were higher in persons who consumed fish at least once a day (Fig. 3). There were no sex differences in fatty acid composition, although n-6 PUFA were slightly higher in women (data not shown). Similar results were observed regarding the concentration of MUFA in serum phospholipids depending on the type of oil used for cooking or seasoning (data not shown).

Fig. 3 Concentration of n-3 fatty acids in serum phospholipids according to fish intake. P (ANOVA): intake frequency, 0·001; sex, NS; age, < 0·001 (●, once a week or less; ■, 2–6 times per week; ▲, at least once a day).
The concentration of MUFA in serum phospholipids of persons who consumed margarine at least once a day, compared with those who consumed it less often, was 11·37 ± 2·39 v. 12·14 ± 2·64 %, P = 0·01. None of the other foods or food groups studied was associated with the concentration of MUFA in serum phospholipids (data not shown).
Type of cooking oil used
At the baseline study, most people used olive oil for frying (64·8 %), braising (85·1 %) and seasoning their food (91·5 %). The concordance between the type of oil used for frying as reported during the survey and that estimated from chemical analysis was: olive oil, 70·5 %; sunflower oil, 46·6 %; a mixture of olive and sunflower oils, 7·1 %. This concordance between the two procedures (questionnaire and laboratory analysis) to evaluate the type of oil used for frying was greater than expected by chance (χ2 = 92·06; P < 0·0001; κ = 0·50). Among persons who used olive oil for frying, 98·9 % and 95·8 % also used it for braising and seasoning, respectively, while only 29·0 % and 10·5 % of those who used sunflower oil for frying also used it for braising or seasoning.
After obtaining a first sample of cooking oil at baseline (sample 1 (olive oil = 54·3 %)), three more samples were also taken from the homes over a 12-month period (samples 2 (olive oil = 55·0 %), 3 (olive oil = 57·3 %) and 4 (olive oil = 61·4 %)). The concordance for olive oil of sample 1 with sample 2 (n 395) was κ = 0·68, for sample 3 (n 101) it was κ = 0·34, and for sample 4 (n 47) it was κ = 0·40. In all cases, concordance was significantly greater than expected by chance (P < 0·05).
In the follow-up study (sample 5), 6 years later, 81·9 % of persons who had consumed olive oil initially still used it, whereas only 57·4 % of those who had used sunflower oil still did so. The net result was an increase in the number of persons who consumed olive oil (71·4 %). The concordance between baseline and follow-up samples was significant (χ2 = 38·9; κ = 0·20; P < 0·0001).
Concentration of polar compounds in the oils used
The concentration of polar compounds and polymers in the oils used for cooking was significantly greater when the cooking oil was sunflower oil or a mixture of sunflower and olive oils, in all four samples from the first study (data are average of the four samples) as well as in the study undertaken 6 years later in the homes of the same persons (Table 2). A high concentration of polar compounds (>20 %) in the oils was significantly more frequent in the samples taken from families who used sunflower oil (16·5 %) or a mixture of sunflower and olive oils (15·0 %) than in the samples of those using olive oil (5·0 %). The use of refined olive oil or an electric deep fryer and the number of times the oil was used for frying were significantly associated with an increase in polar compounds and polymers in the oils of all samples taken (Table 3).
Table 2 Proportion of polar compounds and polymers in the oils from the kitchens sampled during the first-field study and in the second study 6 years later
(Mean values and standard deviations)
* P value, differences among oil types by one-way ANOVA.
Table 3 Polar compounds and polymers according to the quality of the oil, the cooking utensil used for frying and the number of times the same oil was used for frying
(Mean values and standard deviations)

* P value, one-way ANOVA.
An ANOVA model in which the dependent variable was the concentration of polar compounds in the cooking oils and the independent variables were those in Table 3 showed that the type of oil (P = 0·05) and the use of a frying pan or deep fryer (P = 0·002) contributed independently to the explanation of the variance in the concentration of polar compounds, with a significant interaction between the use of a frying pan or deep fryer and the number of times the oil was reused (P = 0·01).
Intake of macronutrients according to the amount of MUFA consumed
Table 4 summarises the intake of macronutrients according to the 25th percentile (P25) and the 75th percentile (P75) of the intake of MUFA, expressed as a percentage of daily energy (P75 = 20·5 % of energy intake or P25 = 15·5 % of energy intake) and adjusted for age, sex and BMI. Subjects with a higher proportion of energy intake from MUFA consumed less energy per day, at the expense of a lower proportion of carbohydrates. Those who had an intake of MUFA >P75 also consumed a greater proportion of saturated and n-3 fatty acids. Finally, subjects with the highest MUFA intake also consumed less fibre.
Table 4 Intake of macronutrients according to the intake of MUFA, expressed as percentage of daily energy (% En)
(Mean values and standard deviations)

25th Percentile (P25) = 13·5 % and 75th percentile (P75) = 20·5 %.
* P value, one-way ANOVA adjusted by age, sex and BMI.
Nutritional habits according to the amount of MUFA consumed
The different behaviour in dietary habits according to the greater ( ≥ P75) or lesser ( ≤ P25) intake of MUFA is shown in Table 5. As the data are expressed as qualitative variables, they have been adjusted for age, sex and BMI in a logistic model in which the dependent variable was the intake of MUFA ≥ P75 or ≤ P25. The table only shows variables with significant differences between extremes of MUFA intake. Persons who consumed more MUFA used more olive oil for frying and less sunflower oil for braising and seasoning; ate more whole-meal bread, salads, asparagus, artichokes and cucumbers; and consumed less white bread, biscuits, nuts, peas, potatoes and sausages.
Table 5 Probability of intake of different foods by extremes of MUFA intake
(OR and 95 % CI values)

* Likelihood of consuming MUFA % En ≥ P75, OR adjusted by age, sex and BMI. Only foods with a significant association with MUFA intake are shown. The following foods were also evaluated but were not associated with MUFA: ice cream; cured cheese; caramel cream and custard; white cheese; semi-cured cheese; milk and yoghurt; lentils; beans; cereals; rice; pasta; margarine; butter; commercial mayonnaise; lard, eggs; marmalade; pastries; tinned fish; sea food; meat; mixed vegetables; braised vegetables; Swiss chard and spinach; artichokes; green beans; carrots; aubergine; courgette; onions; mushrooms; cabbage; broad beans; maize; pepper; beetroot; tomato; fresh fruit; coffee; legumes; fish.
Educational level and health habits according to the type of cooking oil used
Persons who used only olive oil (as evaluated by chemical analysis of the fats used for cooking) had a higher level of education, more often consumed alcoholic drinks and were more physically active (Table 6). The differences remained significant after calculating the probability of consuming olive oil v. sunflower oil (alone or mixed with olive oil) in a logistic model adjusted for age, sex and BMI.
Table 6 Educational level and health habits according to the oil used for cooking, as identified by measurement of the fatty acids by GC in the oils taken from the kitchen
(OR and 95 % CI values)
* All logistic regression models adjusted by age, sex and BMI.
Discussion
Mediterranean countries show differences in dietary habits, food preparation and other health-related habits(Reference Soriguer, Esteva and Rojo22), but the common denominator in Mediterranean diets is the consumption of olive oil. The present report stems from the ‘Pizarra study’(Reference Soriguer, Rojo-Martínez and Almaraz11, Reference Mataix, Garcia and Mañas14, Reference Morcillo, Cardona and Rojo23, Reference Soriguer, Rojo and Esteva24), a prospective investigation of diet and health in a population from Southern Spain with a high prevalence of obesity and type 2 diabetes. The nutritional pattern in this population is defined by a higher intake of energy than recommended, and a high intake of energy from fat (average 41·1 % of daily energy), especially MUFA, accounting for 18·2 % of the daily energy consumption. This intake of MUFA, which can be equated to olive oil, is similar to that reported for Southern Italy(Reference Bargallo, Cavera and Sapienza25). The present study shows that in this population from Southern Spain, persons who consumed more MUFA consumed less energy per day, fewer carbohydrates and more total fat (some 47 % of the daily energy). They also consumed more SFA and n-3 PUFA than those who consumed less MUFA. These results differ in part from other studies undertaken in Northern Spain, which found that persons who consumed more MUFA also consumed a lower proportion of saturated fats(Reference Serra-Majem, Ngo de la Cruz and Ribas7). Despite this high intake of MUFA, the n-6:n-3 fatty acid ratio was very high, similar to that of other Western countries (>10:1)(Reference Bargallo, Cavera and Sapienza25) and far higher than that of diets in primitive societies(Reference Eaton, Konner and Shostak26). As expected, the n-6:n-3 fatty acid ratio was greater in persons who consumed less MUFA. On the other hand, persons with the greatest intake of MUFA (olive oil) consumed less white bread and sugar, fewer potatoes and sausages and more greens, such as salads or asparagus. Additionally, the persons who used olive oil for cooking had a higher level of education, drank more wine with meals and exercised more. The results are in partial agreement with those of other authors(Reference Serra-Majem, Ngo de la Cruz and Ribas7, Reference Bargallo, Cavera and Sapienza25), and confirm that the nutritional behaviour in the Mediterranean populations studied thus far is closely associated with the consumption of olive oil and depends in part on cultural level.
In a large, population-based cohort study, Trichopoulou et al. (Reference Trichopoulou, Costacoy and Bamia2) found that a higher degree of adherence to the Mediterranean diet, measured on a nine-point scale, was associated with a reduction in total mortality, even though no strong association was evident for the individual components of the Mediterranean diet score. These authors suggested various explanations for this finding. However, the quantification of the amount and type of fat in population studies are particularly difficult(Reference Willett5), due, among other reasons, to both intra- and inter-person variability. In the present study, we administered a 7 d quantitative food survey at two different times of the year, accompanied by a FFQ. In addition to identifying the oil used for cooking, we measured the fatty acids in samples of cooking oil taken from the homes of the participants. The questionnaire was validated by measuring the fatty acid composition of the serum phospholipids. Also, the study was undertaken in the context of a longitudinal study, which enabled us to evaluate the consistency of nutritional habits over time. The greatest source of MUFA was olive oil, which is used both for frying and braising, as well as for seasoning. On the other hand, many of the participants who used sunflower oil for frying used olive oil for braising or seasoning. The fatty acid composition in tissues is specific for each tissue, although it may be modified by the type of dietary fatty acid(Reference Soriguer, Tinahones and Monzón27–Reference Olveira, Olveira and Dorado29). Subjects who consumed olive oil had a greater proportion of MUFA in their serum phospholipids and those who consumed sunflower oil had a more n-6 PUFA, while the n-3 fatty acids' content was associated with the intake of fish, indicating that the questionnaires were sufficiently sensitive to correspond with the biological markers. The results of the present study nevertheless warn of the need to use objective measurements beyond food records, as 16 % of subjects who thought they were using olive oil were in fact cooking with a mixture of olive oil and sunflower oil, which led to an overrepresentation of the intake of MUFA in the overall evaluation. However, fatty acid exchange between the cooking oil and the food being cooked could explain in part the compositional differences in home oils(Reference Small, Oliva and Tercyak30). On follow-up, there was an increase in the intake of olive oil, which may be due to the Hawthorne effect in population-based studies(Reference McCarney, Warner and Iliffe31) or to campaigns by the health authorities on its healthy properties.
Fried foods are popular all over the world due to their crunchiness and smell, and to their ease of cooking. Even though a certain amount of potentially toxic products are produced during frying (such as polar compounds or polymers), fried foods are considered safe(Reference Artman32, Reference Chao, Hsu and Lin33). Previous laboratory studies have shown that olive oil is more resistant than sunflower oil to deterioration by reuse in frying(Reference Mataix, Garcia and Mañas14, Reference Cuesta, Sánchez-Muñiz, Varela, Varela, Bender and Morton34–Reference Pérez-Camino, Márquez Ruiz and Ruiz-Mendez36). The present study confirms that in a natural environment, as is the home, persons who use sunflower oil more often have a high proportion of polar compounds and polymers in their cooking oil. The study also shows that the concentration of polar compounds and polymers in the oils depends on the way they are used with oil from kitchens using a deep fryer having a higher proportion. The evaluation of potentially toxic compounds produced by the inadequate use of vegetable oils in the kitchen is not usually contemplated in nutritional surveys. Recent experimental studies have shown that oxidised frying oil can have important effects on lipid metabolism(Reference Chao, Hsu and Lin33), and we have recently reported an association between the concentration of polar compounds in the oil used for frying in the kitchens of family homes and the risk of hypertension(Reference Soriguer, Rojo and Dobarganes12).
The present study also shows that persons with a greater intake of MUFA from olive oil had a higher educational level, were more physically active and consumed more vegetables than those who consumed sunflower oil, which resulted in a lower daily energy intake. This is a particularly important point if we consider that the prevalence of obesity and a sedentary lifestyle is very high in this population(Reference Soriguer, Rojo Martinez and Esteva37), although similar to that reported in other countries(Reference Bargallo, Cavera and Sapienza25, Reference Martínez, Varo and Santos38).
The association found between a greater intake of MUFA and a higher educational level suggests that the concept of a ‘Mediterranean diet’ is mainly associated with the intake of olive oil, as well as with other healthy habits linked to adequate health information. Important changes have occurred over recent years in the nutritional patterns of countries about the Mediterranean basin. As pointed out by Willett(Reference Willett39) paradoxically, the discoveries concerning the biological value of the Mediterranean diet are in fact proving more useful for other countries that are changing their nutritional habits to approach the pattern of a Mediterranean diet than for the Mediterranean countries themselves. The increased prevalence of obesity in Mediterranean countries(Reference Soriguer, Rojo and Esteva24, Reference Bargallo, Cavera and Sapienza25) is an example of this change in lifestyle. The present study shows the difficulty reconciling the usual recommendations in Western countries to reduce dietary fats with the traditional nutritional behaviour associated with the Mediterranean diet, in which there is a high intake of fat as olive oil. However, none of the studies undertaken in Mediterranean populations has shown an association between the intake of olive oil and increased BMI(Reference Serra-Majem, Ngo de la Cruz and Ribas7, Reference Soriguer, Rojo and Esteva24, Reference Trichopoulou, Gnardellis and Benetou40). Additionally, the role of fat in the genesis of the epidemic of obesity in industrialised countries is still unsettled(Reference Willett5, Reference Bray and Popkin6). The increased intake of saturated fats associated with the higher intake of MUFA found in the present study points to the need of designing selective educational strategies depending on the dietary and cooking habits of each region at any one time(Reference Serra-Majen, Ferro-Lizzi and Bellizi41, 42).
The results show concordance in the use and consumption of olive oil in the same population over time, but also reflect imprecision in the awareness of the type of fat or vegetable oil being used. They also show that the preferential intake of MUFA from olive oil is associated with other health and nutritional habits. This association was conditioned by the educational level of the study population. The study also suggests that nutritional epidemiology would benefit from incorporating techniques for controlling home cooking, with the kitchen being considered as a small, non-controlled experimental laboratory. Finally, the results support the idea that the general recommendations on changes of what is known as the ‘Western diet’ should be adjusted to the Mediterranean countries, and to their particular culinary and health habits.
Acknowledgements
We are grateful to Ian Johnstone for his help with the English language version of the manuscript. The present study was supported by Fondo de Investigación Sanitaria (PI041883, PI051307), Junta de Andalucía (0124/2005, P06-CTS-01 684) and Fundación Centro de Excelencia en Investigación sobre Aceite de oliva y Salud (CEAS). CIBERDEM and CIBEROBN are initiatives of Instituto de Salud Carlos III, Spain.
Conflicts of interest. None disclosed.
Contribution of each author. Design and coordination: F. S. Provision of original data: M. C. A., I. C., J. M. G.-A., F. L., S. M., E. G.-E., M. C. D., G. O., V. H., S. V., M. S. R.-A. and I. E. Analysis of data and writing the draft of the manuscript: F. S., G. R.-M. Interpretation of results and contributions to the writing of the manuscript: all authors. Sources of support. Grants from ISCIII (PI041883, PI051307), Andalucia Government (0124/2005) and Asociación Maimónides.









