


The Mediterranean diet (MD) emerged as a healthy food regimen long before it could be recognised which nutrients, or indeed which foods, were responsible for its observed benefits. From the rich picture that anthropologists provided from various Mediterranean countries, biologists and epidemiologists embarked on a long path towards a full understanding of the aetiology of the observed health benefits, first by investigating at single nutrients or foods, then by adopting a more holistic dietary pattern (DP) approach, and this is now being completed with a molecular understanding. Although health and science have always been associated with studies of the MD, other characteristics such as environmental and public health concerns are also important. The present study briefly considers the history of the emergence of the MD as a healthy DP, and this is followed by recent biological and epidemiological evidence for its stronger health benefits, before concluding with a brief discussion of its societal relevance.
Historical context
The MD was already characterised by the time of ancient Egyptian civilisation as illustrated by a sculpture on the tomb of Ramses II showing the association of cereals, olive trees and vine. However, it was Castelvetro(Reference Castelvetro1), an Italian exiled in England, who in 1634 first mentioned its relationship with health when, complaining about the local population eating too much meat and not enough fruit and vegetables, he praised the MD for a better health. Much later, in the second part of the twentieth century, the Rockefeller Foundation came to Greece and made an unexpected observation: ‘a people with good health and impressive longevity living in a country deprived of the modern developments present in the US, and eating vegetables floating in oil(Reference Nestle2)!’
But it was 10 years later before a scientific approach emerged on the effects of the MD, when in the 1960s Keys et al. (Reference Keys, Menotti and Aravanis3) initiated a large ecological study, the Seven Countries Study, with sixteen cohorts in Mediterranean and non-Mediterranean countries. This showed for the first time the low mortality rates in countries around the North shore of the Mediterranean (especially Crete). About 10 years later, the (Multinational MONItoring of trends and determinants in CArdiovascular disease) MONICA study was undertaken in Europe with CVD incidence as an end point (this is more relevant than mortality)(Reference Tunstall-Pedoe, Kuulasmaa and Mahonen4). Lower rates of CHD were observed in Spain and Southern France compared with Northern France and North European countries. In both studies, the Seven Countries Study and MONICA, dietary questionnaires were collected in subgroups of the cohorts and the main food groups typical of the MD were identified. These studies noted that in many regions on the North shores of the Mediterranean, people were eating the same types of food, even though recipes were different. These consisted of plenty of plant foods including whole grain cereals as staple food, vegetables and fruits (fresh or dried) eaten either raw or cooked. Legumes (lentils, chickpeas and beans), nuts (almonds, pistachios, hazelnuts and walnuts), herbs (thyme, rosemary and basil) and spices (nutmeg, cinnamon and saffron) were also consumed. Fish and seafood were frequent in meals, even in rural areas distant from the sea as they were dried or salted. Meat was only present in a few meals, generally for fiestas, and lamb was preferred. Dairy products were also consumed in moderation, often as fresh cheese from the milk of ewes or goats. Even though staple foods (rice, polenta, bulghur or bread), cooking practices, choice of fruits and vegetables, and use of wild herbs were different, there were two common denominators in the diets of Northern Mediterranean countries: olive oil and wine. Olive oil was used in all meals for cooking and salad dressings and wine was regularly drunk with meals in moderate amounts. Thus, nutritionists elaborated the MD model from these comprehensive observations of the traditional food habits (Table 1).
Table 1 The components of the Mediterranean diet
Biology
Fatty acids
The quality of fatty acids is an important nutritional factor in disease prevention, and it was Keys et al. (Reference Keys, Menotti and Aravanis3) who first proposed that the ratio of MUFA:SFA was the key component for the health benefits of the MD. Then, after the Lyon Diet Heart Study, α-linolenic acid appeared as important for the prevention of post-myocardial infarct death(Reference de Lorgeril, Salen and Martin5). This was explained by the observation that α-linolenic acid, when present in sufficient amounts, is an efficient precursor of EPA, and it is EPA that is responsible for the observed benefits(Reference Mozaffarian, Ascherio and Hu6). Thus, long-chain n-3 fatty acids, together with their metabolites (anti-inflammatory leukotrienes), were reported as essential for the prevention of CVD.
More recently, the importance of the SFA carbon chain length was evoked. Whereas C12 to C16 SFA are known to be atherogenic, SFA with a medium carbon chain length (caproic C6, caprylic C8 and capric C10) are directly β-oxidised in the liver and so are less atherogenic. Caprylic acid is also an inhibitor of the apoB(Reference Rioux and Legrand7). This is relevant to the health benefits of the traditional MD, as these fatty acids are in higher concentrations in goats and sheep – the main sources of meat and milk in the MD – than in cows(Reference Hoffman and Gerber8).
Phenolics
Due to the rich diversity of plant foods in the MD, there is a high and varied intake of phenolic compounds, including flavonoids and various non-flavonoids such as phenolic acids, stilbenes and lignans. Total polyphenol intake by the Prevención con Dieta Mediterránea (PREDIMED) cohort was recently estimated at 820 (sd 323) mg/d, with coffee, fruits, olive oil and wine being the major sources(Reference Tresserra-Rimbau, Medina-Remon and Perez-Jimenez9). The importance of phenolics for the cardiovascular benefits of extra virgin olive oil (EVOO) has been shown by comparing olive oils that are high and low in phenolics. For example, olive oil increased HDL-cholesterol level and lowered oxidised LDL-cholesterol level in proportion to the phenolic content of the oil(Reference Covas, Nyyssonen and Poulsen10), and the European Food Safety Authority has now recognised the importance of olive oil polyphenols for protecting LDL particles from oxidative damage. Phenolics in wine may also help protect individuals against CVD by contributing to the overall antioxidant effects of the MD, especially when the body is under conditions of oxidative stress that occurs after a meal(Reference Covas, Gambert and Fito11).
Although in vitro studies identified phenolics as direct antioxidants, other more likely in vivo targets are now being identified. These include increasing phase II enzymes in order to eliminate xenobiotics such as carcinogens, by repressing molecules involved in proliferation (such as protein kinase C (PKC), c-Jun and c-Fos), and by inducing apoptosis (caspases). Inhibition by phenolics of the pro-inflammatory transcription factor nuclear factor-κB (NF-κB), the pro-oxidant transcription factor activator protein 1 (AP-1), and activation of the antioxidant transcription factor NFE2-related factor 2 (Nrf2) may be involved in reducing oxidative stress and low-grade chronic inflammation and may contribute to the wide ranging benefits of phenolics against chronic diseases(Reference Ma12, Reference Leonarduzzi, Sottero and Poli13). Consumption of polyphenol-rich olive oil as part of a MD has also been shown to decrease the expression of a number of genes associated with oxidative stress and inflammation(Reference Konstantinidou, Covas and Munoz-Aguayo14). Phenolics generally have low bioavailability and low concentrations in the systemic circulation, and this tends to confirm that direct antioxidant activity is not their main mechanism of action in vivo (Reference Hollman, Cassidy and Comte15).
A group of phenolics known as secoiridoids (such as oleuropein) and their breakdown products (such as hydroxytyrosol) are found almost exclusively in olives and olive oil and so are of particular interest in relation to observations that EVOO may confer specific benefits as part of a MD (discussed below). One recently reported target for EVOO secoiridoids (and also resveratrol in red wine) is activation of the energy-sensing enzyme AMP-activated protein kinase(Reference Menendez, Joven and Aragones16). AMP-activated protein kinase is currently attracting a good deal of attention as it switches on catabolic pathways, such as increased uptake and oxidation of glucose and fatty acids, and this is implicated in decreasing the risk for obesity, type 2 diabetes and some cancers.
More disease-specific mechanisms for phenolics have also been reported including reduced plaque formation by oleuropein aglycone in a mouse model for Alzheimer's disease(Reference Grossi, Rigacci and Ambrosini17) and anti-diabetic and anti-cancer effects by flavonoids(Reference Babu, Liu and Gilbert18, Reference Romagnolo and Selmin19). Polyphenols in EVOO promote the proteasomal degradation of human epidermal growth factor receptor 2 (HER2)(Reference Menendez, Vazquez-Martin and Garcia-Villalba20), although it has not been established if this is associated with beneficial effects in HER2+ breast cancer. Olive oil (both virgin and non-virgin) was also identified as the major dietary source of lignans in the PREDIMED cohort(Reference Tresserra-Rimbau, Medina-Remon and Perez-Jimenez9). Lignans act as phyto-oestrogens in the body and were reported to be associated with a reduced risk of breast cancer in post-menopausal women, although it is unclear if additional anti-cancer mechanisms may also be involved(Reference Buck, Zaineddin and Vrieling21).
There is now an increased understanding of how crosstalk between phenolics and other nutrients may contribute to disease prevention(Reference Nadtochiy and Redman22), and this is helping to provide a mechanistic basis for explaining the epidemiological evidence which suggests that it is the overall MD that is most important for its benefits. This is discussed in the next section.
Epidemiology
Science: the holistic approach
After the historical studies described above, the Harvard group listed the beneficial foods of the MD and those which were either absent or consumed in moderation(Reference Kushi, Lenart and Willett23, Reference Kushi, Lenart and Willett24). But the health benefits of individual nutrients or foods were never completely convincing; it is the holistic approach that best captures the evidence(Reference Gerber25).
Different epidemiological designs can be used in this holistic perspective: DP and intervention studies using a nutritional approach. Two techniques are commonly implemented to study the relationship between DP and diseases. A posteriori analysis is a principal component analysis that defines DP in a population. These analyses are transformed into summary scores that can be analysed by regression analysis in order to examine the risk of a disease related to the identified patterns. This technique gives information on the effects of a MD only if a sample of the population follows this model. In the a priori model, a predefined score is applied to the nutritional data of a population. With regard to the MD, the Mediterranean diet score (MDS) of Trichopoulou first described in 1995(Reference Trichopoulou, Kouris-Blazos and Wahlqvist26), and completed and finalised in 2003 by the introduction of fish intake(Reference Trichopoulou, Costacou and Bamia27), has been used most often. However, it is apparent that the Trichopoulou score, including the quantitatively and qualitatively typical MD of the elderly Greeks, was until recently only appropriate for Mediterranean populations, because (1) in the Greek situation, the MUFA:SFA ratio reflects mainly the consumption of olive oil, which is not the case for North European countries or the USA; (2) the median defining fruit and vegetable consumption in the elderly Greek population (vegetables ≥ 500 g/d, fruits ≥ 350 g/d) is not commonly attained in North European countries or in the USA and therefore the MDS based on the median consumption of these North European countries or the USA may not show a benefit of MD as it did not reflect the typical quantitative characteristics of the MD. Thus, several modifications have been published that adapt the MDS to diverse populations, and in these cases, the health benefits are generally lower than those observed in Mediterranean countries (for a complete evaluation of DP and MD, see Hoffman & Gerber(Reference Hoffman and Gerber28)).
A few intervention studies(Reference Bos, de Vries and Feskens29–Reference Vincent-Baudry, Defoort and Gerber32) have implemented a nutritional approach to study the effects of a MD on markers of risk for CVD, with advice for a MD in the experimental group, and either a high intake of SFA, or a prudent diet or an American Heart Association diet as a control group. However, only PREDIMED(Reference Estruch, Ros and Salas-Salvado31) had a sample large enough and a follow-up that allowed CVD incidence and mortality to be recorded.
The results of these recent approaches constitute a body of studies with convincing levels of evidence with regard to some health effects, namely all-cause mortality and cardiovascular mortality. They also highlight areas requiring further investigation, such as the specific effects of olive oil.
Health: assessing the evidence
The inference of causality has been a long search for epidemiologists and was initiated by Hill(Reference Hill33). The World Cancer Research Fund(34) has established criteria for levels of evidence very close to Hill's proposal, with the improvement of introducing a hierarchy for assessing the validity of the designs of the studies, with intervention studies and prospective studies placed at the top. Meta-analyses are also of value as long as they include evaluation of heterogeneity, sensitivity and linear response analysis. An intervention study conducted on a representative population brings results that are the closest to demonstrating a causal relationship between an exposure and health. Consistent results of several prospective studies conducted in different populations in different countries also provide a strong level of evidence. Thus, the only studies presented here are those for which there is enough data to support a conclusion with a convincing or probable level of evidence for a relationship with the MD.
Mediterranean diet
Results are convincing with regard to the effect of a MD on all-cause mortality as illustrated by the meta-analysis of Sofi et al. (Reference Sofi, Abbate and Gensini35) and further supported by the latest results from the Women's Health Initiative (WHI) study(Reference Bertoia, Triche and Michaud36) and the Seguimiento Universidad de Navarra (SUN) study(Reference Zazpe, Sanchez-Tainta and Toledo37). Further evidence comes from the Nurses’ Health Study and Health Professionals Follow-Up Study(Reference Sofi, Abbate and Gensini35), although these cohorts had CVD at the beginning of the study(Reference Lopez-Garcia, Rodriguez-Artalejo and Li38). The risk reduction is always greater in Mediterranean countries (by 20–30 %) and always greater for cardiovascular mortality than for cancers, as shown in Table 2 for studies that have evaluated both all-cause and cause-specific mortalities(Reference Trichopoulou, Costacou and Bamia27, Reference Buckland, Agudo and Travier39, Reference Knoops, de Groot and Kromhout40). Table 2 also shows the remarkable consistency between different studies and populations for the hazard ratio for all-cause mortality and cardiovascular mortality.
Table 2 Association (fully adjusted Cox hazard ratio (HR)) between Mediterranean diet scores and all-cause mortality and cause-specific mortality (Hazard ratios and 95 % confidence intervals)
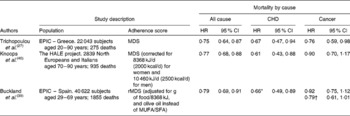
EPIC, European Prospective Investigation into Cancer and Nutrition; HALE, Healthy Ageing: a Longitudinal study in Europe; MDS, Mediterranean diet score; rMDS, relative Mediterranean diet score.
* CVD.
† Restricted to digestive, breast and prostate.
The PREDIMED intervention study best supports a risk reduction effect of the MD on CVD incidence. It has an interesting peculiarity in that there were two experimental groups: one enriched in nuts and the other enriched in EVOO. The control group consumed a low-fat American Heart Association type diet. Compared with the control group, there was a 28 % (95 % CI 0·54, 0·96) risk reduction in the nut-enriched group and a 30 % (95 % CI 0·54, 0·92) risk reduction in the EVOO-enriched group after 5 years of follow-up(Reference Estruch, Ros and Salas-Salvado31). Total mortality over 5 years (Kaplan–Meier) gave a hazard ratio of 0·81 (95 % CI 0·63, 1·05; P trend= 0·11) for the EVOO group and 0·95 (95 % CI 0·73, 1·23; P trend= 0·68) for the nut group, suggesting an advantage for olive oil consumption(Reference Estruch, Ros and Salas-Salvado31).
Thus, there is a convincing causal relationship between a DP similar to the traditional MD and overall mortality, and cardiovascular mortality and incidence.
The relationship between type 2 diabetes and the MD has progressed since two early Spanish publications(Reference Martinez-Gonzalez, de la Fuente-Arrillaga and Nunez-Cordoba41, Reference Salas-Salvado, Bullo and Babio42) and is now supported by the latest results of the PREDIMED study(Reference Salas-Salvado, Bullo and Estruch43), and by two meta-analyses(Reference Koloverou, Esposito and Giugliano44, Reference Schwingshackl, Missbach and Konig45). Both meta-analyses concluded that there was a benefit provided by MD in reducing the development of type 2 diabetes (0·81, 95 % CI 0·73, 0·90 and 0·77, 95 % CI 0·66, 0·89, respectively). Both analyses had significant heterogeneity, which was explained by either differences in the lengths of follow-up: the longer the length, the larger the risk reduction(Reference Schwingshackl, Missbach and Konig45); or in the health status of the cohort(Reference Koloverou, Esposito and Giugliano44): studies conducted on a cohort at CVD or diabetes risk showed the highest risk reduction. Both analyses observed that the risk reduction was non-significant in the US studies and significant in European countries, further suggesting greater benefits in Mediterranean countries, and the authors evoked the possible effects of other beneficial factors present in the Mediterranean lifestyle not revealed by the MDS(Reference Hoffman and Gerber28).
Thus, the level of evidence for a risk reduction of type 2 diabetes development is probable.
An interesting question remains to be elucidated: Which factors present in Mediterranean countries, in addition to the diet, are responsible for this beneficial effect?
Effects on cancer incidence are more difficult to elucidate since the best data come from observational prospective studies because of practical and ethical difficulties with intervention studies. Moreover, not only is each cancer type related to different etiological factors but even within a class of cancer there are different characteristics with regard to the risk factors, e.g. breast cancers with or without oestrogen receptors (ER). Several studies have found inverse associations between increasing MDS and cancer risk. These include studies that did not include olive oil in the score such as head and neck cancers(Reference Li, Park and Wu46), hepatocellular carcinoma(Reference Turati, Trichopoulos and Polesel47) and gastric cancer(Reference Praud, Bertuccio and Bosetti48) and other studies such as for gastric cancer and bladder cancer in smokers, which were analysed with the relative MDS in which olive oil consumption was assessed(Reference Buckland, Agudo and Lujan49, Reference Buckland, Ros and Roswall50). For breast cancer, a risk reduction was observed only when olive oil was present as a single food(Reference Bessaoud, Daures and Gerber51), or using an a posteriori DP including olive oil(Reference Cottet, Touvier and Fournier52) or when using a MDS applied to a Mediterranean population(Reference Trichopoulou, Bamia and Lagiou53), but not when applied to a non-Mediterranean population(Reference Couto, Sandin and Lof54).
Thus, it is probable that a MD is inversely associated with some cancers.
As for diabetes, the heterogeneity observed between Mediterranean and non-Mediterranean countries may possibly be explained by factors of the global Mediterranean lifestyle, such as physical activity, high vitamin D synthesis and quality of life, that correlate with the diet in Mediterranean countries.
Olive oil
Although studies are sparse and further studies are required, it is interesting to note that EVOO might have specific effects on some diseases. This is suggested in the PREDIMED intervention study, especially with regard to cardiovascular mortality(Reference Estruch, Ros and Salas-Salvado31). In a study conducted in Spain, there was a reduction of CVD incidence of 7 % for each increase of 10 g of olive oil intake per 8368 kJ (2000 kcal) ingested, especially with EVOO (risk reduction 14 %)(Reference Buckland, Travier and Barricarte55). In another study on the same population, an intake ≥ 29·4 g of olive oil/8368 kJ per d compared with < 14·9 g of olive oil/8368 kJ per d decreased the risk of overall mortality by 26 % (P trend< 0·001) and of CVD deaths by 44 % (P trend< 001)(Reference Buckland, Mayen and Agudo56). In the European Prospective Investigation into Cancer and Nutrition (EPIC) Greek cohort, olive oil was associated with a risk reduction of cerebrovascular disease incidence(Reference Misirli, Benetou and Lagiou57). In the latest report on diabetes and the PREDIMED subcohort(Reference Salas-Salvado, Bullo and Estruch43), the group treated with a MD enriched with EVOO had the lowest incidence of diabetes, and a significantly decreased RR compared with the group on the control diet (0·60; 95 % CI 0·43, 0·85). Investigating the effects of olive oil on breast cancer incidence in the Mediterranean cohorts of EPIC, a risk reduction was observed for ER − breast cancers, although the small number of these cancers did not allow for statistical significance(Reference Buckland, Travier and Agudo58). In the Three Cities Study, olive oil was associated with a decrease in cognitive impairment(Reference Berr, Portet and Carriere59).
Thus, there is some suggestion for a specific role of olive oil in the MD, but further studies towards understanding the precise effects of olive oil and of its specific phenolics are required.
Societal relevance
Public health
For a long time, the high lipid content of the MD has created opposition. Lipids represent 37–38 % of the total energy intake in published studies on the MD, which is slightly above the upper limit of 35 % proposed by the Food and Agriculture Organisation (FAO)(60), and almost at the limit of 35–40 % proposed by the French Food Safety Agency(61). Indeed, a MD might be a way to reduce the public health problem of obesity as (1) the glycaemic indices of most of foods (whole grain cereals, vegetables and fruits) in the MD are low, and the glycaemic load of the MD is decreased by the structure of the Mediterranean meal; (2) a high MDS reduces the risk of weight gain with increasing age as shown in the longitudinal SUN study(Reference Beunza, Toledo and Hu62); (3) a traditional MD is the best diet for maintaining a healthy weight after a regimen of weight loss(Reference Schwarzfuchs, Golan and Shai63).
Health economics
Stroke is a frequent event in people at cardiovascular risk and, in addition to the human suffering it causes, it is an increasing burden on health budgets due to the increasing longevity of European populations. In France, the mean cost of treating a stroke is €17 000, and the total cost to France is €5·3 billion. In 2006, annual direct health care costs associated with CHD were estimated at £3·2 billion in the UK, and the overall cost to the UK economy was nearly £9 billion(Reference Harland64). Increased longevity is also accompanied by an increased risk of other degenerative diseases (such as Parkinson's and Alzheimer's diseases), and some studies have shown a risk reduction for these diseases in people adhering to a MD(Reference Samieri, Sun and Townsend65, Reference Scarmeas, Luchsinger and Schupf66). Thus, prevention using a MD will save public money.
Environment
The moderate amounts of meat consumed as part of a MD means less animal-derived greenhouse gas production. Moreover, there is a preference for small ruminants, raised non-intensively, or mono-gastric animals, which produce less methane than beef(Reference Gerber, Steinfeld and Henderson67). The large variety of fruits and vegetables maintains biodiversity and promotes polyvalent agriculture as part of sustainable and organic agriculture and reduces contaminants. The recommendation for seasonal local consumption is also a factor that favours energy economy by reducing the need to heat greenhouses and the need to transport produce from southern hemisphere countries. Hence, adherence to a MD might help to develop sustainable agriculture.
Concluding remarks
It is important to promote the MD in its entirety to include the benefits of olive oil and to respect variety, diversity and other aspects of the MD such as the structure of the meals and their organisation through the day, and without snacking(Reference Tessier and Gerber68). And to remember that it is more than just a diet, there is also a Mediterranean lifestyle with physical activity – which is mainly outdoors and good for vitamin D synthesis, and also wine drunk in moderation with meals for gastronomy and conviviality. Because a MD is good for individuals, for public health, for health economics and for the environment, Mediterranean countries should treasure it and should work to promote it through information to the public and professionals, and by spreading knowledge of food quality and cooking practices. And, on a larger scale, this needs initiatives from public health and agricultural policies.
Acknowledgements
None of the authors has conflicts of interest.
The authors’ contributions are as follows: R. H. was responsible for the Biology section and editing of the article. M. G. was responsible for the other parts of the text.


