Abstract link:https://www.ncbi.nlm.nih.gov/pubmed/29986857
Full citation: Osmond M, Klassen T and Wells G. Validation and refinement of a clinical decision rule for the use of computed tomography in children with minor head injury in the emergency department. CMAJ 2018;190:E816–22
Article type: Diagnosis
Ratings: Methods – 4/5 Usefulness – 3/5
INTRODUCTION
Background
Clinical decision rules such as CATCH, derived in 2010 with near-perfect sensitivity, provide physicians with an evidence-based approach to determining which children with minor head injury need imaging.
Objectives
1) Prospectively validate the CATCH clinical decision rule for children with minor head injury to determine who requires computed tomography (CT) imaging; and 2) explore clinical decision rule refinement to improve its performance.
METHODS
Design
Prospective multicentre cohort study.
Setting
Nine Canadian emergency departments.
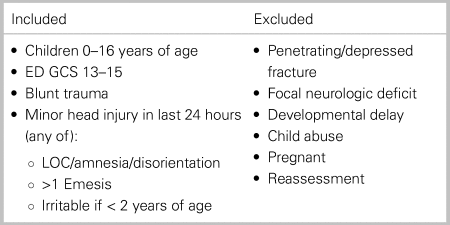
Subjects
Table 1. Inclusion and exclusion criteria of study
Intervention
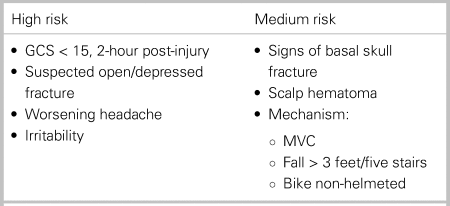
Application of CATCH for CT imaging:
Table 2. CATCH decision rule criteria
RESULTS
A total of 4,494 eligible patients were enrolled with 4,060 included in the final analysis. Mean age was 9.7 years; 463 (11.4%) of patients were younger than 2 years; 1,417 (34.9%) patients underwent CT imaging.
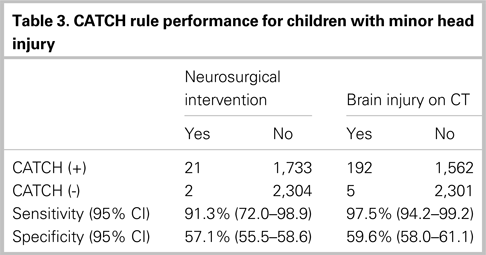
Table 3. CATCH rule performance for children with minor head injury
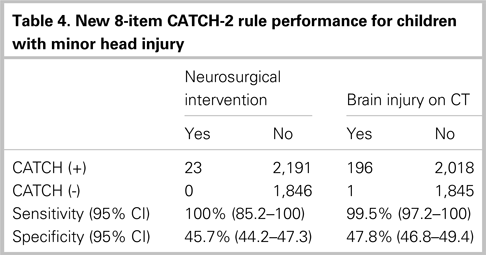
The removal of high and medium risk stratification and the addition of 8th criterion (≥ 4 episodes of emesis) provided improved performance.
Table 4. New 8-item CATCH-2 rule performance for children with minor head injury
APPRAISAL
Strengths
• Relevant, important clinical question
• Unbiased, consecutive, prospective patient enrolment process
• Multicentre, nationwide study
• Congruity of CATCH rule to derivation study
• Good inter-observer interpretation of predictor variables (kappa = 0.67)
• High degree of physician comfort with rule (81.5%)
• Patient follow-up at 14 days post discharge to ensure no missed adverse outcomes
• Clear description of recursive partitioning process to refine rule
Limitations
• High proportion lost to follow-up (n = 434; 9.7%)
• Event rate unclear in children < 2 years (n = 463)
• Low primary outcome event rate resulting in wide confidence intervals
• Bootstrap analysis of CATCH-2 completed with original CATCH derivation cohort, posing risk of sample bias
CONTEXT
The 2010 CATCH derivation studyReference Osmond, Klassen and Wells1 reported 100% sensitivity for high-risk and 98.1% sensitivity for medium-risk variables aiming to rule out pediatric minor head injuries requiring neurosurgical intervention. In contrast, the prospective validation of CATCH (91.3% sensitivity) is less sensitive than other validated clinical decision rules (PECARN: 100% sensitivity if < 2 years; 96.8% sensitivity if > 2 years).Reference Kuppermann, Holmes and Dayan2,Reference Lyttle, Crowe and Oakley3
By refining the 7-item CATCH rule to the 8-item CATCH-2 rule, 100% sensitivity for neurosurgical intervention is achieved at the cost of increased CT rate compared with CATCH and PECARN. CATCH-2 provides a user-friendly “list” compared with PECARN and CHALICE,Reference Lyttle, Crowe and Oakley3 but validation of CATCH-2 is necessary prior to use.
BOTTOM LINE
This validation study of the CATCH clinical decision rule for pediatric minor head injury failed to provide a sensitivity as high as its derivation study. The results make CATCH inadequate to be safely applied in the emergency department. Consequently, the authors used recursive partitioning to derive the CATCH-2 clinical decision rule by removing “high risk” and “medium risk” stratification and instead adding an eighth criterion of “vomiting ≥ 4 episodes.” These changes provided 100% sensitivity for neurosurgical intervention. Although CATCH-2 shows promise, it has not yet been prospectively validated, a requisite step prior to clinical implementation.Reference McGinn, Guyatt and Wyer4




 You have
Access
You have
Access
Abstract link:https://www.ncbi.nlm.nih.gov/pubmed/29986857
Full citation: Osmond M, Klassen T and Wells G. Validation and refinement of a clinical decision rule for the use of computed tomography in children with minor head injury in the emergency department. CMAJ 2018;190:E816–22
Article type: Diagnosis
Ratings: Methods – 4/5 Usefulness – 3/5
INTRODUCTION
Background
Clinical decision rules such as CATCH, derived in 2010 with near-perfect sensitivity, provide physicians with an evidence-based approach to determining which children with minor head injury need imaging.
Objectives
1) Prospectively validate the CATCH clinical decision rule for children with minor head injury to determine who requires computed tomography (CT) imaging; and 2) explore clinical decision rule refinement to improve its performance.
METHODS
Design
Prospective multicentre cohort study.
Setting
Nine Canadian emergency departments.
Subjects
Table 1. Inclusion and exclusion criteria of study
ED GCS = emergency department Glasgow Coma Scale; LOC = level of consciousness.
Intervention
Application of CATCH for CT imaging:
Table 2. CATCH decision rule criteria
GCS = Glasgow Coma Scale; MVC = motor vehicle collision.
Outcomes
■ Primary: Neurosurgical intervention within 7 days.
■ Secondary: Brain injury on CT.
RESULTS
A total of 4,494 eligible patients were enrolled with 4,060 included in the final analysis. Mean age was 9.7 years; 463 (11.4%) of patients were younger than 2 years; 1,417 (34.9%) patients underwent CT imaging.
Table 3. CATCH rule performance for children with minor head injury
The removal of high and medium risk stratification and the addition of 8th criterion (≥ 4 episodes of emesis) provided improved performance.
Table 4. New 8-item CATCH-2 rule performance for children with minor head injury
APPRAISAL
Strengths
• Relevant, important clinical question
• Unbiased, consecutive, prospective patient enrolment process
• Multicentre, nationwide study
• Congruity of CATCH rule to derivation study
• Good inter-observer interpretation of predictor variables (kappa = 0.67)
• High degree of physician comfort with rule (81.5%)
• Patient follow-up at 14 days post discharge to ensure no missed adverse outcomes
• Clear description of recursive partitioning process to refine rule
Limitations
• High proportion lost to follow-up (n = 434; 9.7%)
• Event rate unclear in children < 2 years (n = 463)
• Low primary outcome event rate resulting in wide confidence intervals
• Bootstrap analysis of CATCH-2 completed with original CATCH derivation cohort, posing risk of sample bias
CONTEXT
The 2010 CATCH derivation studyReference Osmond, Klassen and Wells1 reported 100% sensitivity for high-risk and 98.1% sensitivity for medium-risk variables aiming to rule out pediatric minor head injuries requiring neurosurgical intervention. In contrast, the prospective validation of CATCH (91.3% sensitivity) is less sensitive than other validated clinical decision rules (PECARN: 100% sensitivity if < 2 years; 96.8% sensitivity if > 2 years).Reference Kuppermann, Holmes and Dayan2,Reference Lyttle, Crowe and Oakley3
By refining the 7-item CATCH rule to the 8-item CATCH-2 rule, 100% sensitivity for neurosurgical intervention is achieved at the cost of increased CT rate compared with CATCH and PECARN. CATCH-2 provides a user-friendly “list” compared with PECARN and CHALICE,Reference Lyttle, Crowe and Oakley3 but validation of CATCH-2 is necessary prior to use.
BOTTOM LINE
This validation study of the CATCH clinical decision rule for pediatric minor head injury failed to provide a sensitivity as high as its derivation study. The results make CATCH inadequate to be safely applied in the emergency department. Consequently, the authors used recursive partitioning to derive the CATCH-2 clinical decision rule by removing “high risk” and “medium risk” stratification and instead adding an eighth criterion of “vomiting ≥ 4 episodes.” These changes provided 100% sensitivity for neurosurgical intervention. Although CATCH-2 shows promise, it has not yet been prospectively validated, a requisite step prior to clinical implementation.Reference McGinn, Guyatt and Wyer4
Competing interests
None declared.