INTRODUCTION
Tumor lysis syndrome is a well-described oncologic emergency requiring rapid recognition and treatment. It is commonly seen in the context of rapidly proliferating tumors, particularly hematologic malignancies. The initiation of chemotherapy, radiation, or steroids can result in massive cell lysis leading to hyperkalemia, hyperphosphatemia, hypocalcemia, hyperuricemia, elevated lactate, dehydrogenase (LDH) and lactate and renal failure secondary to uric acid nephropathy. Evidence-based treatment consists of aggressive hydration, allopurinol or rasburicase, correction of hyperkalemia, and, possibly, urine alkalinization. Spontaneous tumor lysis syndrome occurring without cytotoxic therapy is relatively rare, particularly with solid tumors.Reference Firwana, Hasan and Hasan 1 - Reference Vaisban, Braester and Mosenzon 3 The mortality rate from spontaneous tumor lysis syndrome secondary to solid malignancies may be as high as 30% with renal failure and hyperkalemia being the leading immediate causes of death.Reference Vaisban, Braester and Mosenzon 3
CASE
A 48-year-old previously healthy male was admitted to a community hospital with a 1-week history of anorexia, weight loss, nausea, fatigue and chills, and right upper quadrant pain. Lab work disclosed elevation of liver enzymes. Imaging revealed dense liver lesions consistent with metastatic disease with a possible colorectal primary. A colonoscopy showed an annular lesion on the sigmoid, which on biopsy revealed adenocarcinoma. Prior to discharge, arrangements were made with a regional cancer centre for subsequent assessment and treatment. At 1 week post-discharge, he presented to a nearby tertiary care centre with worsening abdominal pain, jaundice, weakness, and anorexia. A physical examination was remarkable for jaundice, hepatomegaly, possible ascites, and peripheral edema. No cytotoxic therapy had been administered prior to his presentation.
Labs
WBC 33.7×109/L ( N 4-10.0×109/L)
PMN 30×109/L (N 2-7×109/L)
Hb 104 g/L (N 140-174 g/L)
Platelets 44×109/L (N 130–400×109/L)
INR 2.1 (N 0.9–1.2)
Lactate 8.6 mmol/L (N 0.9–1.8 mmol/L)
K 6.5 mmol/L (N 3.5-5.0 mmol/L)
Urate 836 mmol/L (N 180-420 mmol/L)
Urea 25.9 mmol/L (N 2.5-8.0 mmol/L)
Cr 202 µmol/L (N 70-120 µmol/L)
Ca 2.68 mmol/L (N 2.18-2.58 mmol/L)
PO4 0.49 mmol/L (N 0.80-1.50 mmol/L)
Bili 185 µmol/L ( N < 26 µmol/L)
AST 157 U/L (N 0-35 U/L)
ALT 222 U/L (N 3-36 U/L)
ALP 139 U/L (N 35-100 U/L)
GGT 633 U/L (N 8-61 U/L)
LDH 226 U/L (N 95-195 U/L)
ECG Normal
Repeat imaging showed marked progression of the liver metastases with a large tumor burden. A presumptive diagnosis of tumor lysis syndrome was made, and treatment was initiated with allopurinol, hydration with normal saline, dextrose, and insulin. Oncology consultation advised against chemotherapy given the advanced nature of the disease. The patient was admitted to the palliative care service and died 2 days later. At the time of presentation, rasburicase was not on the hospital formulary.
DISCUSSION
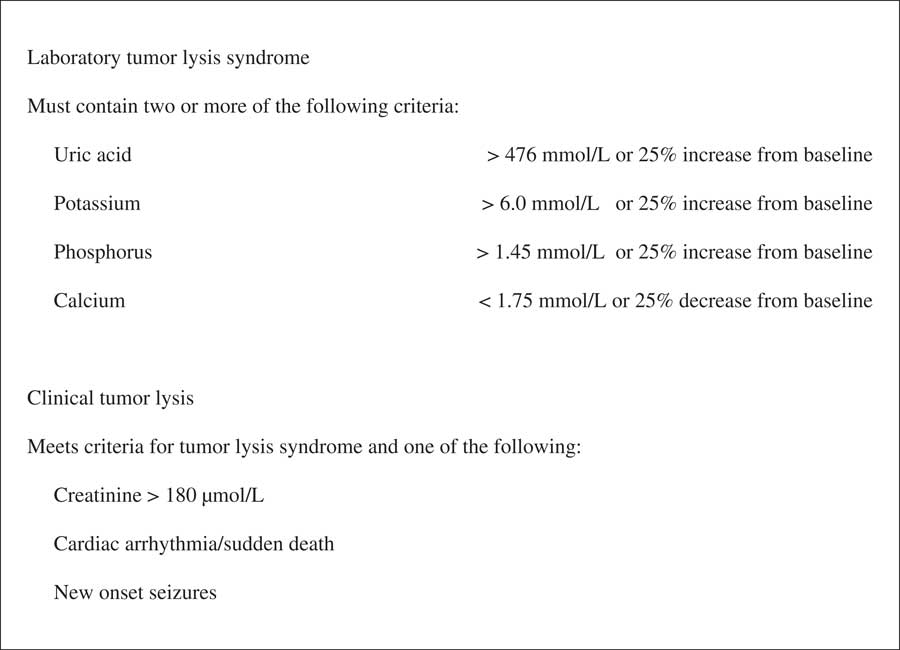
When a rapidly proliferating tumor is present, the initiation of cytotoxic chemotherapy, radiation, or steroids (rarely) can result in tumor lysis syndrome. Rarely, as in this case, tumor lysis syndrome can also occur spontaneously. Rapid cell lysis leads to the release of large amounts of potassium, phosphate, and nucleic acids, the latter being rapidly metabolized to uric acid. Metabolic consequences include hyperkalemia, hyperphosphatemia, hyperuricemia, lactic acidosis, and secondary hypocalcemia resulting from calcium precipitating with phosphate. Calcium phosphate crystals may accumulate in the cardiac conducting tissues leading to arrhythmias. Both uric acid and calcium phosphate accumulate in the renal tubules, which, if untreated, may lead to renal failure. Widely accepted criteria for the diagnosis of tumor lysis syndrome are contained in the Cairo-Bishop definition (Figure 1).Reference Howard, Jones and Ching Hon 4 , Reference Cairo and Bishop 5
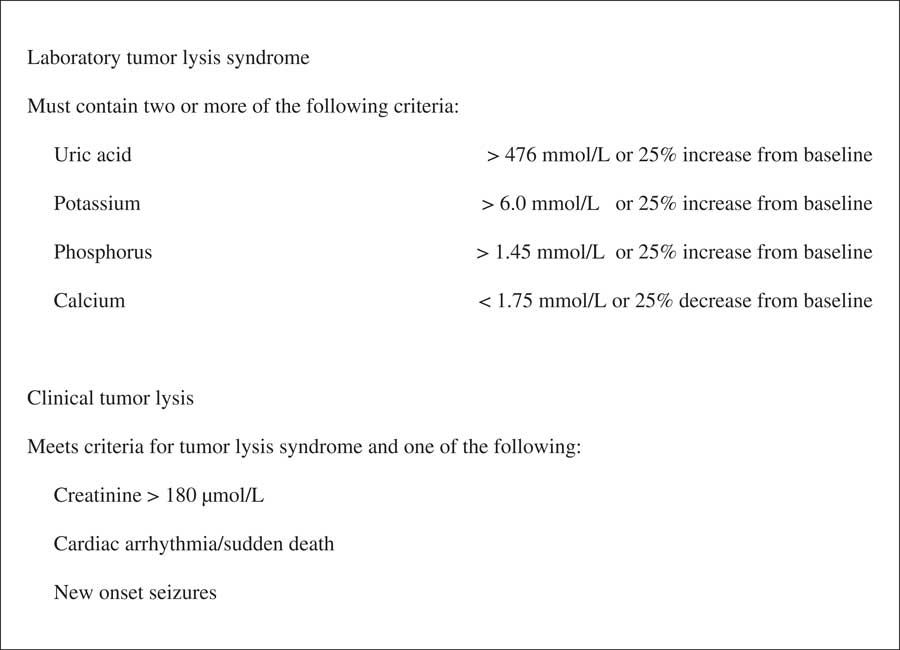
Figure 1 Cairo-Bishop definition of tumor lysis syndrome.
Of note, our patient fulfilled two of the biochemical criteria for tumor lysis syndrome but was mildly hypercalcemic and hypophosphatemic. Hyperphosphatemia is rarely observed in spontaneous tumor lysis syndrome because the phosphate released is thought to be quickly reused in the generation of new neoplastic cells that would be less likely to assimilate in the context of chemotherapy administration. As hypocalcemia occurs as a consequence of calcium binding excess phosphate, it is reasonable to assume that this derangement would occur less frequently with spontaneous tumor lysis syndrome.
Treatment measures include aggressive hydration with normal saline, use of hypouricemic agents such as allopurinol and rasburicase, management of electrolyte abnormalities, particularly hyperkalemia, and, in select cases, renal replacement therapy. If hypocalcemia is symptomatic then treatment is indicated.Reference Kekre, Djordjevic and Touchie 6 Aluminum hydroxide and hydroxyurea may be used for hyperphosphatemia.Reference Firwana, Hasan and Hasan 1 , Reference Weeks and Kimple 2 The efficacy of urine alkalinization remains unknown. Allopurinol is a purine that competitively inhibits xanthine oxidase, the enzyme that catalyzes the conversion of xanthine and hypoxanthine to uric acid. This eventually leads to the lowering of serum uric acid levels but at the expense of increasing xanthine levels, which may also contribute to a nephropathy. In addition, it may take 24 to 48 hours to see an appreciable reduction in uric acid levels.Reference Howard, Jones and Ching Hon 4 Rasburicase is a urate oxidase that converts uric acid to allantoin, a substance that is 5 to 10 times more soluble in the urine than uric acid and therefore causes a rapid reduction in uric acid levels.Reference Weeks and Kimple 2 , Reference Cairo and Bishop 5 The recommended dose is 0.1 to 0.2 mg/kg.
Spontaneous tumor lysis syndrome is extremely uncommon in metastatic colonic carcinoma. As of 2014, there has been only one previously reported case of spontaneous tumor lysis syndrome in the context of untreated metastatic colonic carcinoma.Reference Kekre, Djordjevic and Touchie 6 , Reference Mirrakhimov, Barbararyah and Khan 7
CONCLUSION
Tumor lysis syndrome is an oncologic emergency necessitating early diagnosis and treatment. When it manifests early after cytotoxic treatment, the diagnosis is often obvious. However, as this case illustrates, emergency physicians need to be aware of more subtle presentations. Rarely, spontaneous tumor lysis syndrome can be the initial manifestation of a yet undiagnosed malignancy.
Competing interests: None declared.