


No CrossRef data available.
Article contents
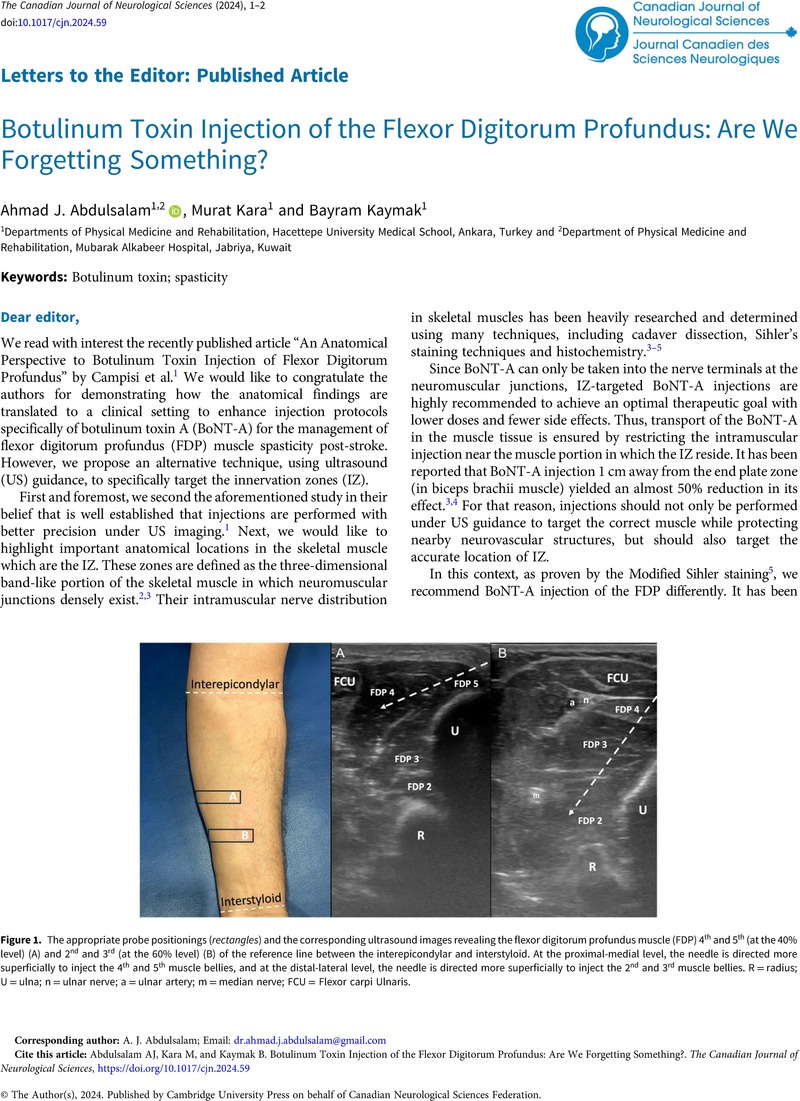
Botulinum Toxin Injection of the Flexor Digitorum Profundus: Are We Forgetting Something?
Published online by Cambridge University Press: 24 April 2024
Abstract
An abstract is not available for this content so a preview has been provided. Please use the Get access link above for information on how to access this content.
Keywords
Information
- Type
- Letters to the Editor: Published Article
- Information
- Copyright
- © The Author(s), 2024. Published by Cambridge University Press on behalf of Canadian Neurological Sciences Federation
References
Campisi, ES, Khan, O, Agur, AMR, et al. An anatomical perspective to botulinum toxin injection of flexor digitorum profundus. Can J Neurol Sci. 2024:1–2. DOI: 10.1017/cjn.2024.34.CrossRefGoogle ScholarPubMed
Rodríguez Cruz, PM, Cossins, J, et al. The neuromuscular junction in health and disease: molecular mechanisms governing synaptic formation and homeostasis. Front Mol Neurosci. 2020;13:610964.CrossRefGoogle ScholarPubMed
Kaymak, B, Kara, M, Yağiz On, A, et al. Innervation zone targeted botulinum toxin injections. Eur J Phys Rehabil Med. 2018;54:100–9.CrossRefGoogle ScholarPubMed
Kara, M, Kaymak, B, Ulaşli, AM, et al. Sonographic guide for botulinum toxin injections of the upper limb: EUROMUSCULUS/USPRM spasticity approach. Eur J Phys Rehabil Med. 2018;54:469–85.CrossRefGoogle ScholarPubMed
Won, SY, Hur, MS, Rha, DW, et al. Extra- and intramuscular nerve distribution patterns of the muscles of the ventral compartment of the forearm. Am J Phys Med Rehabil. 2010;89:644–52.CrossRefGoogle ScholarPubMed
Dodd, SL, Rowell, BA, Vrabas, IS, et al. A comparison of the spread of three formulations of botulinum neurotoxin a as determined by effects on muscle function. Eur J Neurol. 1998;5:181–6.CrossRefGoogle ScholarPubMed