Introduction
Aneurysms are thought to have first been described more than 2000 years ago in Egyptian antiquity.Reference Al-Shatoury, Raja and Ausman1 For much of their history, aneurysms, especially intracranial aneurysms (IAs), have been poorly understood and had limited treatment options. Proximal ligation of the cartotid artery was the first mainstream surgery for IA used by pioneers like Cooper in the 1800s to variable success.Reference Cooper2, Reference Cooper3 Over the years, gradual improvements were made to the proximal ligation method although it was still held back by a high risk of complications.Reference Schorstein4 Modern surgery for IA can be described in four periods: the Pre-Microsurgical era (pre-1960); the Early Microsurgical era (1960–1980); the Late Microsurgical era (1980–2000); and the Continuing Innovations era (2000–present).Reference Lai and O’Neill5 The predominant treatment for IA during each of these periods was defined by their contemporary technology.
Surgical approaches for IA dominated the Pre-Microsurgical and Early Microsurgical eras. Clipping of IAs was introduced in the early 1930s and soon became the standard approach. Throughout the mid-to-late 20th century, clipping benefited from a number of innovations such as improvements in clip design, diagnostic imaging, and the introduction of the surgical microscope. For many years, clipping was regarded as the definitive treatment for IAs; however in the Late Microsurgical era (1980–2000) and the Continuing Innovations era (2000–present), the advent of endovascular approaches emerged. These minimally invasive procedures could avoid some of the adverse effects of open surgery while being capable of producing good results.Reference Molyneux, Kerr and Yu6 Various methods were tried over the years but the introduction of the detachable coil by Guglielmi in 1991Reference Guglielmi, Viñuela, Sepetka and Macellari7 is arguably the most important tool used in endovascular approaches to date. Since the 1990s, detachable coils have continued to evolve to the benefit of patient safety and reductions in cost.Reference Hui, Fiorella, Masaryk, Rasmussen and Dion8 There has also been the introduction of novel endovascular technologies including flow-diverting stents and liquid embolization materials which are currently under active development.
It is evident that the landscape of treatment for IAs has changed dramatically over the past 100 years, especially during the 1990s. The purpose of the present study is to compile and analyze publications to appraise how academic interest in various procedures has changed with improvements in technology over time. The number of publications in various topics will be used as a proxy measure of this academic interest.
Methods
We performed a generic search for all publications related to the treatment of IAs. We then compiled a list of keywords related to both surgical and endovascular repair of IAs. Based on these keywords, we performed a series of searches to find publications within these specific subtopics. The surgery keywords we used included aneurysm clipping, extracranial-to-intracranial (EC–IC) bypass, and intracranial-to-intracranial (IC–IC) bypass. Endovascular keywords included aneurysm coiling, balloon-assisted coiling, stent-assisted coiling, flow diversion, and liquid material embolization. These terms were combined with the terms intracranial or cerebral aneurysm (exact search strings can be found in Table 1 footnotes). Our searches identified articles that contained these phrases within their titles, abstracts, or keywords.
Table 1: Summary of publications on the treatment of intracranial aneurysms. The numbers represent publications cataloged in Scopus up to 2017. Search terms used are provided in the table footnote

a TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (surgery OR repair OR treatment) AND DOCTYPE (ar OR re).
b TITLE-ABS-KEY (Intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (craniotomy OR endoscopic OR clip OR bypass) AND NOT KEY (endovascular OR transluminal) AND DOCTYPE(ar OR re).
c TITLE-ABS-KEY (Intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (endovascular OR transluminal OR coil OR embolization OR embolisation) AND NOT KEY (clip OR bypass) AND DOCTYPE (ar OR re).
d TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (“Extracranial-to-intracranial” or “EC–IC” AND bypass) AND DOCTYPE (ar OR re).
e TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (“intracranial-to-intracranial” OR “IC–IC” AND bypass) AND DOCTYPE(ar OR re).
f TITLE-ABS-KEY (Intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (endovascular OR transluminal OR coil OR embolization OR embolisation) AND NOT KEY (clip OR bypass) AND DOCTYPE (ar OR re).
g TITLE-ABS-KEY (Intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (coil OR coiling AND (endovascular OR embolization OR embolisation OR repair) AND DOCTYPE (ar OR re).
h TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (“balloon-assisted coiling”) AND DOCTYPE (ar OR re).
i TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (“Stent-Assisted Coiling”) AND DOCTYPE (ar OR re).
j TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (“Flow Diversion”) AND DOCTYPE(ar OR re).
k TITLE-ABS-KEY (intracranial OR cerebral AND aneurysm) AND TITLE-ABS-KEY (“liquid embolization” OR “liquid embolisation” OR “liquid embolic material”) AND DOCTYPE (ar OR re).
Searches were performed in June and July 2018 using the Scopus database (www.scopus.com). The publications found were restricted to articles or reviews in scholarly journals. Articles published up until December 31st, 2017, were included in our analysis. The search results returned included the article name, author list, year published, and number of citations. This information was extracted into a spreadsheet which was screened for duplicate entries. The number of publications in each topic was tallied by year and displayed in graphical form.
In order to provide some indication of influence of the open-surgical versus endovascular literature in the recent past, we calculated the 10-year h-index of these two fields. In this case, the h-index is equal to a number, h, where a particular field has h number of publications with at least h number of citations. This was originally proposed by Hirsch as a metric to compare the research output of individual authors.Reference Hirsch9 In this case, we used all the surgical IA articles in the last 10 years (2008–2017) yielded by our search to calculate a field-specific h-index. We did the same for all the endovascular articles published in the last 10 years. We also found the most highly cited articles among our results and compiled a list of “citation classics” (articles that have been cited over 400 times) in order to help ascertain the most impactful topics over time. We surveyed their abstracts to classify their primary focus as either surgical, endovascular, medical, or a combination.
Results
The number of papers published varied with each procedure (Table 1). A search for all treatment of IAs yielded 21,255 publications between the years of 1938 and 2017. The annual number of publications on IA treatment was modest throughout most of the 20th century but then accelerated in the 1970s. The average annual number of publications was 95 in the 1970s, 150 in the 1980s, 330 in the 1990s, 636 in the 2000s, and 1077 in the 2010s. A peak of 1241 annual publications was reached in 2016.
Our search identified 24 articles with over 400 citations, which earned them the designation of citation classic (Table 2). Only four articles were exclusively surgical in nature while nine were exclusively on endovascular approaches. The remaining articles consisted of trials and reviews that focused on both endovascular and surgical approaches or medical treatment topics. The 10-year (2008–2017) h-index was 51 for open-surgical articles (51 surgical articles published in the last 10 years that received 51 or more citations) and 86 for endovascular articles (86 endovascular articles published in the last 10 years that have 86 or more citations).
Table 2: The most highly cited publications on cerebral aneurysm treatment derived from Scopus up to 2017. Papers with over 400 citations (citation classics) are listed
Surgical Approaches
A generic search for surgical treatment of IA found 5956 articles. The first publication found was a 1947 article by Jefferson titled “Isolated oculomotor palsy caused by intracranial aneurysm,”Reference Jefferson10 which discussed proximal artery ligature and clipping as treatments for IA. There was very little growth in the number of annual publications around mid-century. This period of low activity was followed by steady growth beginning in the 1970s toward a peak of 299 publications in 2015. The number of annual publications on surgical approaches was maintained or declined slightly year-over-year from 2015–2017. Figure 1 shows a comparison of annual publications in surgical and endovascular topics over time, as returned by our searches.
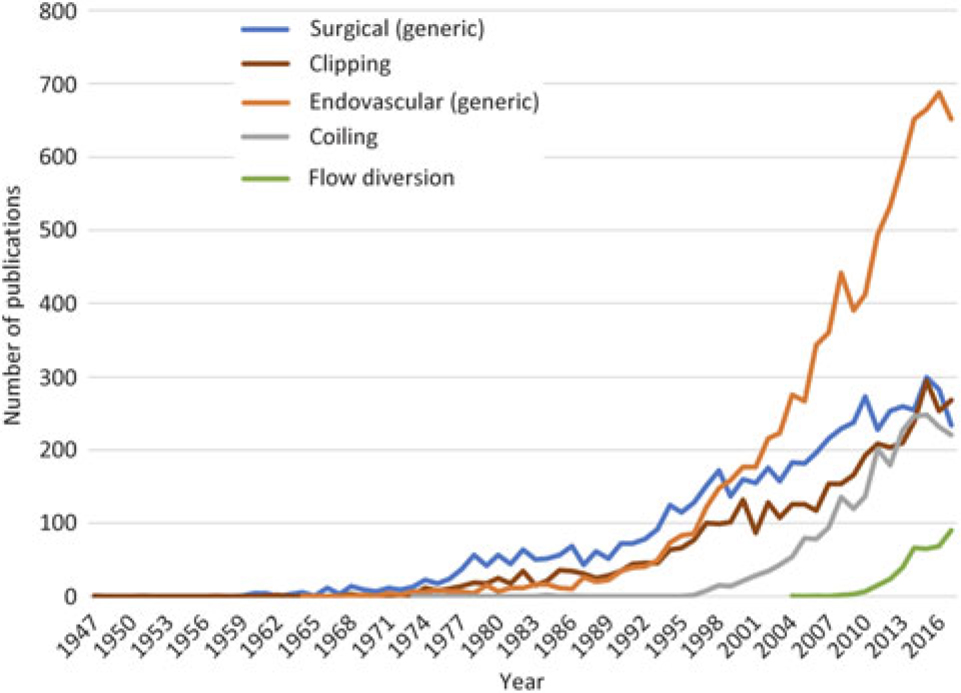
Figure 1: Annual counts of papers published on surgical and endovascular IA treatments until 2017. Data were derived from the Scopus database as described in methods.
A search for publications relating specifically to IA clipping found a similar pattern to the generic search for surgical articles. In total, 4204 publications were found spanning 1947–2017. The first publication in 1947 was the one described above.
We also searched for publications regarding EC–IC bypass and IC–IC bypass techniques yielding 23 and 16 publications, respectively. The first instance of EC–IC bypass in our search was titled “The role of EC–IC in the treatment of giant intracranial aneurysms” by Speztler etal., in 1980.Reference Spetzler, Roski, Schuster and Takaoka11 Most of the publications for EC–IC bypass, however, occurred in the 2010s. The first instance of IC–IC bypass was by Streefkerk etal., in 2004.Reference Streefkerk, Wolfs, Sorteberg, Sorteberg and Tulleken12 Similar to EC–IC bypass, most of the activity occurred in the 2010s.
Endovascular Approaches
A generic search for endovascular treatment of IA found 8602 articles spanning 1964–2017. The first article was in 1964 by Brizzi. It was an Italian article with a translated title: “2 cases of congenital arteriovenous aneurysm of the brain treated by means of embolization with lipiodol-wax.”.Reference Brizzi13 However, we were unable to locate a copy or abstract of this paper to verify that it was truly an endovascular approach and suspect that it was not. The timeline of endovascular approaches shows minimal growth between the initial publication in 1964 and the 1980s. It was only in the 1990s–2000s that substantial growth was seen. The maximum number of 688 publications was reached in 2016 and has since leveled off. A particular point of interest is 1999, which was the year where the number of endovascular publications surpassed surgical ones and continued to remain more numerous ever since.
Our search for publications relating to endovascular coiling of IAs found 5436 results beginning in 1985. This 1985 article was a case series by Braun etal.,Reference Braun, Hoffman, Casarella and Davis14 describing the use of Gianturco coils for internal carotid aneurysms. The time course of annual coiling publications is similar to that of the generic endovascular search.
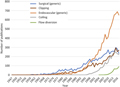
We also examined several other emerging endovascular techniques such as balloon-assisted coiling, stent-assisted coiling, flow diversion, and liquid embolization. The time course of publications for these procedures is shown in Figure 2. Of note is stent-assisted coiling which had the largest body of literature of all these techniques with 522 publications. Both stent-assisted coiling and flow diversion demonstrate steep upward trends although still only make up a small proportion of the total endovascular literature. Balloon-assisted coiling has also seen an upward trend although not to the same consistency and magnitude. The number of publications on liquid embolization has been low with sporadic activity over the past two decades with no obvious trend.
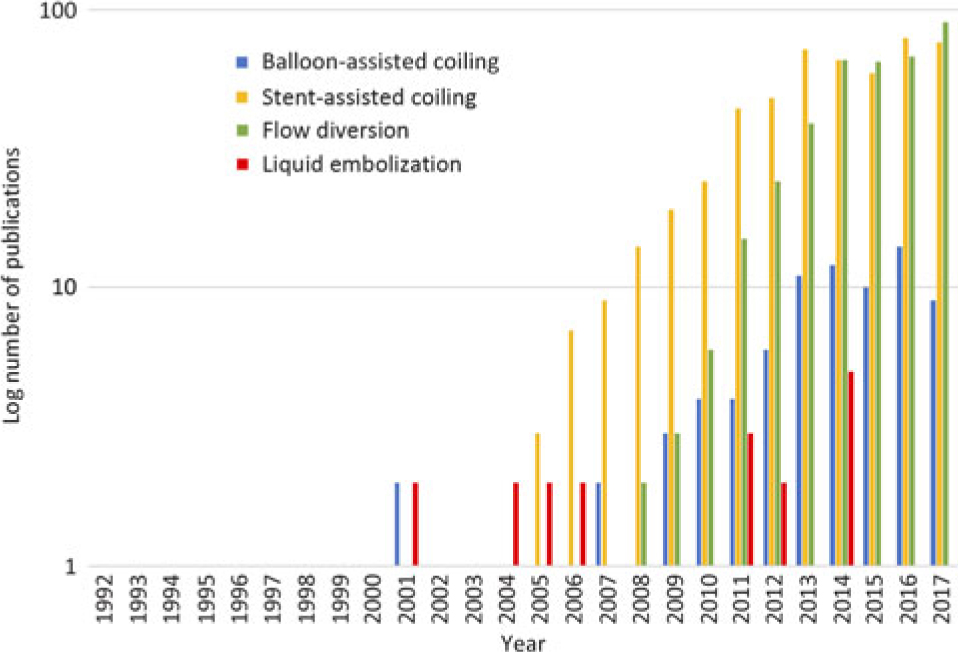
Figure 2: Annual counts of papers published on four different endovascular approaches for IA until 2017. Note the counts are displayed on a logarithmic scale. The four approaches are balloon-assisted coiling, stent-assisted coiling, flow diversion, and liquid material embolization.
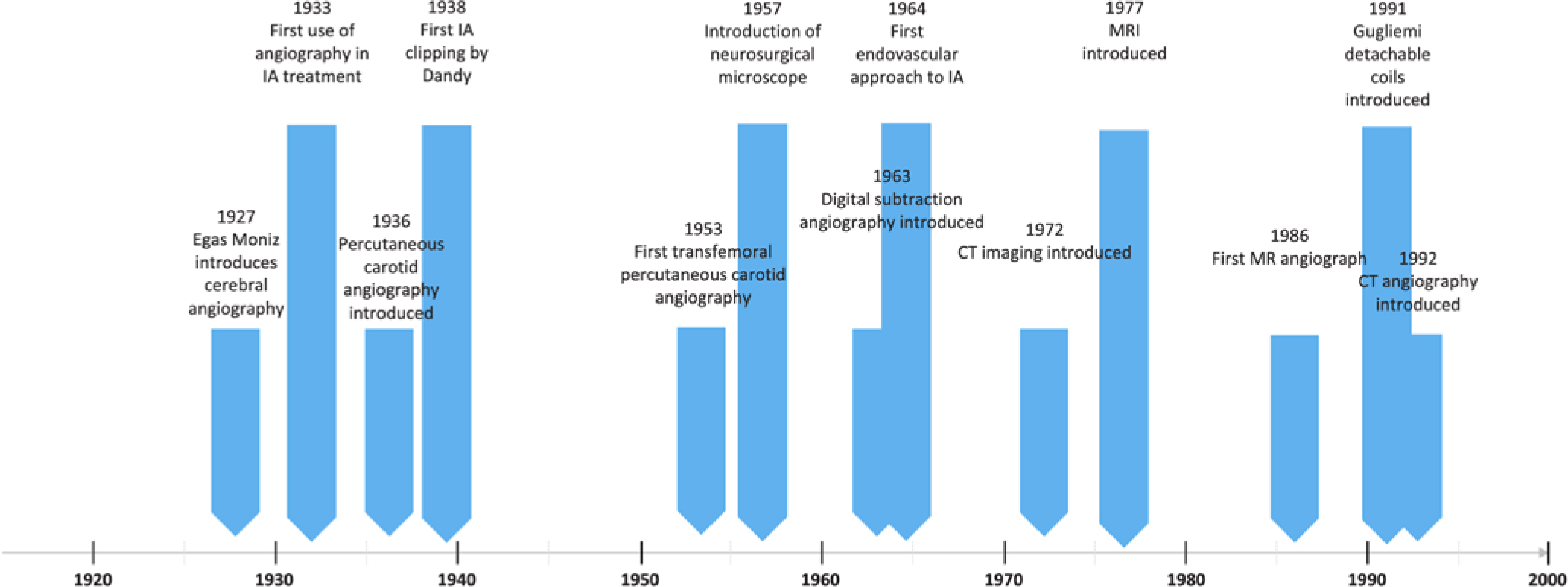
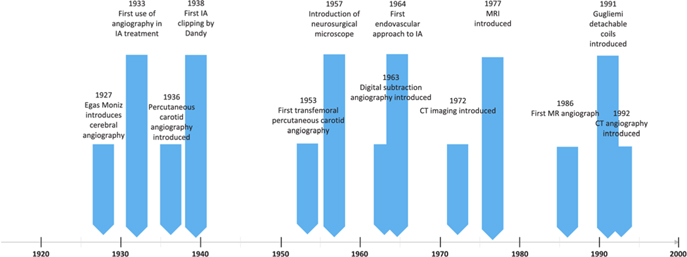
Figure 3: Timeline showing milestones and major innovations in treatment of IA.
Discussion
Surgical IA Publications
Surgery for IAs has been around for more than 100 years. Some early approaches included proximal carotid artery ligation by Horsley in the late 1800sReference Drake15 and Dott’s muscle tissue wrapping of IAs in the early 1930s.Reference Moniz16 Interestingly, some of these early articles escaped detection in our searches despite containing several keywords in their titles.
The earliest articles returned by our search were published in the 1930s onward, coinciding with the introduction of IA clipping surgery. The first record of IA clipping came from Dandy, who in 1938 published an account of using Cushing—McKenzie silver clip to treat an internal carotid artery aneurysm.Reference Dandy17 According to our search results, activity in the IA literature remained low early on, despite the introduction of clipping. This lack of activity was perhaps a consequence of high mortality and morbidity associated with surgical treatment of IAs during this time.Reference Norlén and Olivecrona18 There was a notable uptick in the number of publications around the 1960s, and this coincided with the introduction of the neurosurgical microscope. Under the microscope, aneurysm surgery was able to see a dramatic improvement in outcomes.Reference Krayenbühl, Yaşargil, Flamm and Tew19 This uptick in publications is also likely associated with improvements in clip design by Drake, Sugita, and Yasargil in the 1960s and 1970s.Reference Dujovny, Agner, Ibe and Perlin20 It is clear from our results that clipping is the dominant surgical approach for IA as it produced the largest proportion of surgical publications. We also examined other surgical approaches such as EC–IC and IC–IC bypass techniques which made a contribution, albeit small, to the tally of surgical articles in the 2000s.
Endovascular IA Publications
According to our searches, endovascular approaches to IA treatment emerged largely in the 1990s, despite some early outliers. The first published account of the suggestion of using an endovascular approach for IA came in 1964 by Luessenhop etal.,Reference Luessenhop and Velasquez21 who were early explorers in cerebral artery catheterization. Publications on endovascular approach began to emerge in the 1970s and 1980s as catheter design and endovascular techniques were improved. Still, activity in the field remained low perhaps because surgical clipping was now well established and endovascular approaches were still prone to high rates of complications.Reference Guglielmi22 The field only really started to accelerate in the late 1990s after the introduction of detachable coils for embolization by Guglielmi in 1991.Reference Guglielmi, Viñuela, Sepetka and Macellari7 This new technique was able to avoid many of the shortcomings of the older balloon-based approaches. This period of rapid growth was also likely facilitated by MR angiography in 1986Reference Dumoulin and Hart23 and CT angiography in 1992.Reference Napel, Marks and Rubin24 Coiling has become the dominant endovascular approach. Publications on balloon- and stent-assisted coiling both had similar patterns to coiling, showing rapid growth during the 2000s, but their overall volume was much lower. From a bibliometric perspective, flow diversion appears to an up-and-coming technique, with most of its growth occurring in the last 5 years. Conversely, annual publications in coiling have plateaued, indicating that the field has matured.
The Current and Future Landscape of IA Treatment
It comes as no surprise that there has been a paradigm shift in the IA field. Historically, surgical clipping has been the dominant approach to treatment (Figure 3); however over the past three decades, our results indicate that endovascular approaches have begun to garner more interest. Two of the top three most cited articles in IA treatment, the International Subarachnoid Aneurysm Trial (ISAT) in 2002Reference Molyneux, Kerr and Stratton25 and the International Study of Unruptured Intracranial Aneurysms (ISUIA) in 2003,Reference Wiebers, Whisnant and Huston26 compared these two approaches, signaling a field-wide debate. Despite its rising popularity, coiling still faces its own barriers such as having a reported greater risk of rebleeding compared to clipping.Reference Li, Pan and Wang27 In addition, in certain cases, for example, those associated with large mass effect from a hematoma secondary to acute rupture or individuals where aneurysm anatomy and the ratio of the neck to the fundus are unfavorable, open procedures with clipping may be preferred. Despite these limitations, endovascular publications have surpassed open-surgical ones.
While the advantages of endovascular approaches over open surgery could be one source of the increased publications in the endovascular literature, there are other factors at play. For example, the number of incidental unruptured asymptomatic aneurysms that are being detected has increased over time due to improvements and increased accessibility to imaging technology.Reference Tummala, Başkaya and Heros28 These aneurysms which previously would have not been dealt with surgically are perhaps now being treated with endovascular methods, fueling more publications. Another source of increased publications in the endovascular literature could come from the fact that both neurosurgeons and interventional radiologists could be publishing papers on endovascular topics, causing a larger author pool. Finally, part of the dramatic increase seen in publications could also be due to a general trend toward more publishing over time.
Since the h-index relies on both quantity (the number of publications) and quality (the number of highly cited publications),Reference Costas and Bordons29 we used this measure as a broad indicator of academic interest and impact. The h-index has typically been used as an indicator of impact, especially to rank individual authors, journals, or institutions, but it also has been proposed as an indicator of “hot-topics” in a particular field.Reference Bornmann and Daniel30 In this case, we used it to compare surgical papers and endovascular papers. A higher h-index, as is the case for endovascular articles, indicates a greater number of highly cited articles and therefore a greater amount of high-impact activity in this topic.Reference Bornmann and Daniel30 The increased 10-year h-index of the endovascular versus surgical literature supports the notion that the IA field is transitioning away from surgical approaches in the recent past.
Limitations
The purpose of this study was to appraise the trends of publications on IA treatment over time in the context of technological innovations. Importantly, this was not a systematic review which would have necessitated a thorough review of individual articles. Our bibliometric approach is practical, but not without limitations. The most significant problem encountered was false positives and false negatives returned by our searches. We noted several important articles that did not appear in our search results. This can be attributed to a variety of factors including the lack of journal coverage in the Scopus database and problems with the search terms we used. If articles used synonyms or alternative phrasing to the terms used in our searches, they would have been missed. Conversely, we found many false positives within our search results due to common terminology across unrelated fields. Many of these false-positive articles were related to aneurysm, but not necessarily cerebral aneurysm. In designing search queries, there must be a fine balance between including relevant key words while not being too broad. Another issue we encountered was slight discrepancies in articles returned by different databases. For example, some articles were found on PubMed but not Scopus. We recognize that other databases are available but chose to use Scopus due to its robust citation information and ease of use for exporting search results into Excel spreadsheets to facilitate analysis. We feel that differences across the major publication databases are relatively minor and that they would have yielded largely similar results.
We used the number of publications in a topic as proxy for academic interest in a particular procedure over time. This is an inherently crude approach, although it does provide a practical and reproducible measure and has been used before for a similar investigation.Reference Lozano, Tam and Lozano31 Still, it does fail to take into consideration a variety of biases, such as centers that perform surgeries but do not publish results, the time lag between surgery and publication of results, as well as socioeconomic factors, e.g. the favoring of procedures based on local cost and accessibility. To circumvent some of these limitations, a future study could conduct direct counts of the number of procedures being done with each technique as obtained by surveying national databases. Our analysis of the 10-year h-index of endovascular versus surgical publications is also prone to these biases. Importantly, the h-index is highly discipline specific.Reference Costas and Bordons29 Perhaps having both neurosurgeons and interventional radiologist contributing to the endovascular literature versus neurosurgeons only in the surgical literature is skewing the results. Limitations aside, the h-index provides a simple and reproducible metric for comparison that is within the scope of our investigation.
Conclusion
The state of IA treatment is constantly evolving. Surgical approaches have benefited from technical improvements over time. The advent of new minimally invasive endovascular approaches in the 1990s was a major turning point in the IA field, bringing the once definitive role of clipping into question. Publications on endovascular techniques experienced a more rapid rise to prominence and have now surpassed the number of surgical articles.
Acknowledgements
We would like to acknowledge the Royal College of Surgeons in Ireland and the Keenan Summer Student Research Program for their support of this research.
Disclosures
The authors have no conflicts of interest to disclose.
Statement of Authorship
Conception and design: CS Lozano, J Spears. Acquisition of data: CS Lozano. Analysis and Interpretation of data: CS Lozano, J Spears. Drafting of article: CS Lozano. Critical revision of article: AM Lozano, J Spears. Review of submitted version of article: all authors. Study supervision: J Spears.