Isolated bilateral pedicle fractures in the spine are rare, and an extremely uncommon etiology for spondylolisthesis.Reference Kim, Kim and Lee 1 – Reference Hajjioui, Khazzani and Sbihi 3 We report a case of bilateral pedicle stress fractures accompanying spondylolisthesis in a patient taking Risedronate for 10 years. This is the first reported case of spondylolisthesis accompanying spontaneous bilateral pedicle stress fractures involving one vertebra in a patient on bisphosphonate therapy for osteoporosis. Informed consent to write up this case report was obtained from the patient.
A 79-year-old woman presented with progressively worsening low back pain (LBP) for 6 weeks without any traumatic episodes or previous spinal surgery. Her LBP was mechanical in nature; worse with activities but relieved by sitting or lying down. Past medical history showed she suffered from severe osteoporosis and had been taking a bisphosphonate drug (Risedronate; 35 mg once per week) for 10 years. She also had chondrosarcoma of the chest wall with required resection in 2013 and colon cancer with bowel resection in 2009, both with free margins and no signs or symptoms of local or distant recurrence.
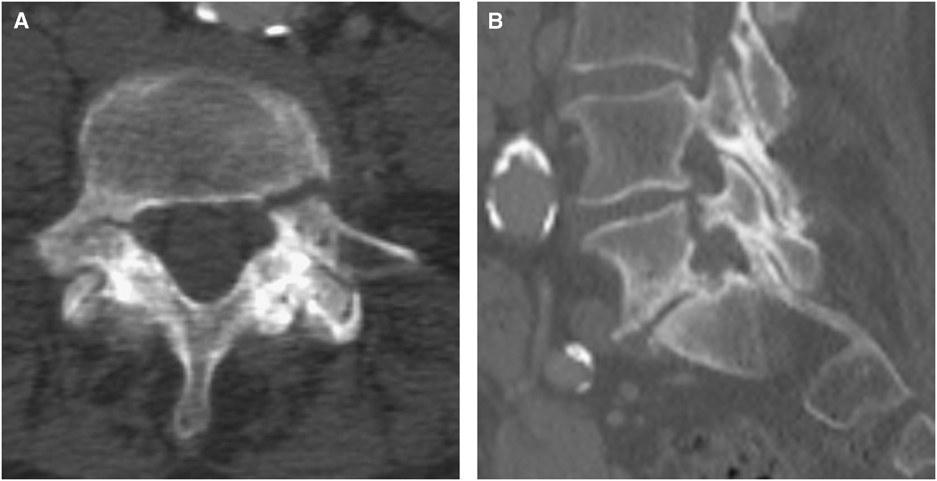
A CT scan 6 months before presentation, to follow-up on benign cystic lesions in her liver, demonstrated no significant vertebrae abnormalities (Figure 1). A further CT scan to investigate a 6-week history of atraumatic mechanical back and flank pain demonstrated new bilateral L5 pedicle fractures (Figure 2), which prompted her referral for consultation with a spine surgeon.
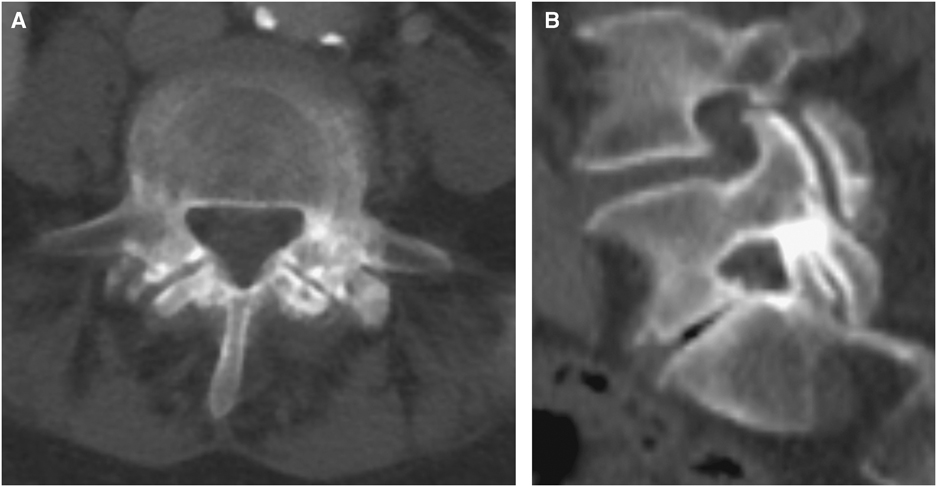
Figure 1 (A,B) Axial and sagittal CT scan of the abdomen performed 6 months before presentation. No fractures or spondylolisthesis noted.
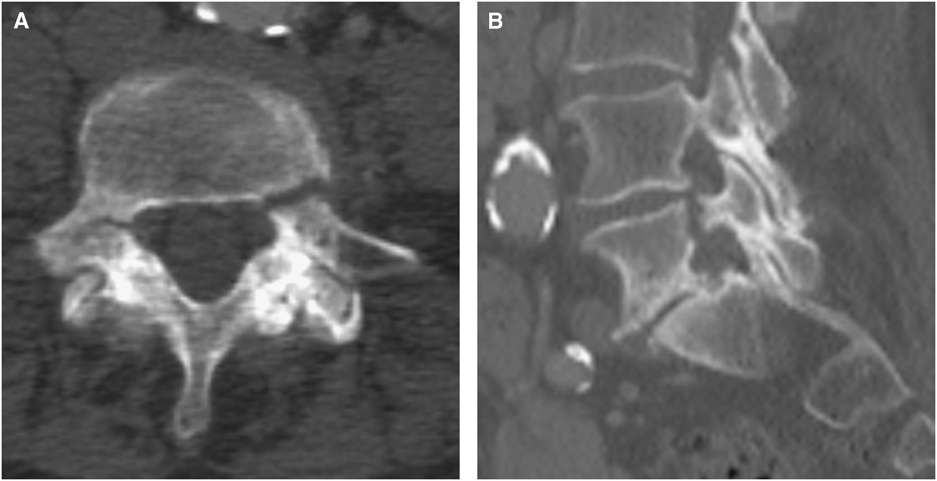
Figure 2 (A,B) Axial and sagittal CT scan of the abdomen performed before presentation. Demonstrating bilateral L5 pedicle fractures.
On physical examination, she was able to stand and walk without assistance, although her LBP increased gradually in the standing position. She was neurologically intact. At presentation, she rated her pain as 8/10 on a numerical pain rating scale and scored 43/50 on the Oswestry Disability Index (ODI).
Standard X-ray imaging of the lumbar spine (i.e., lateral, anterior–posterior, and flexion/extension views) showed stable grade 1 spondylolisthesis at L5-S1 and bilateral L5 pedicle fractures. There was mild degenerative scoliosis but we do not think this was relevant because of the bilateral nature of the injury. Subsequent MRI (Figure 3) confirmed these X-ray imaging findings and, together with a technetium-99m methyl diphosphonate bone scan, found no local or distant findings that would suggest tumor involvement. Dual-energy X-ray absorptiometry T-scores for bone mineral density of the femoral neck and lumbar spine were −2.5 and −2.7, respectively.
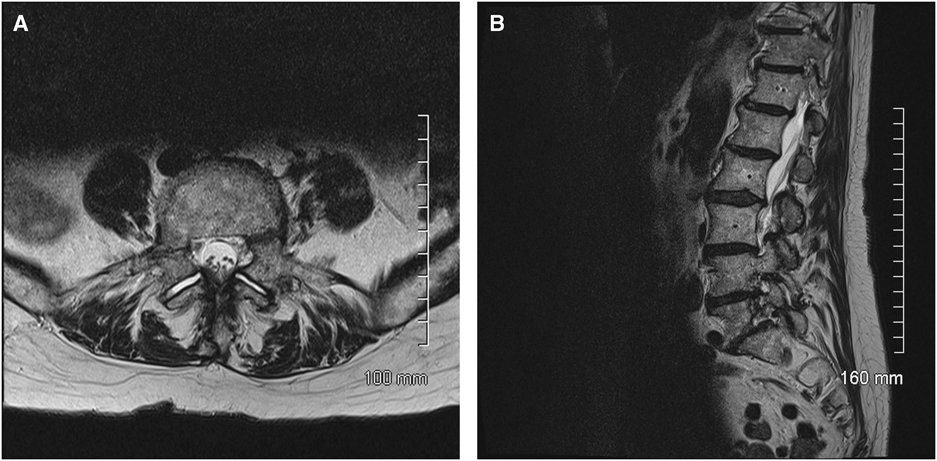
Figure 3 (A,B) Axial and sagittal T2 weight MRI scan of the lumbar spine performed at presentation. Demonstrating bilateral L5 pedicle fractures with grade 1 spondylolisthesis at L5-S1, and no findings suggestive of tumor involvement.
Options for treatment including surgery versus brace versus observation were discussed with the patient. After hearing the costs, risks, and benefits of each option, she chose conservative therapy.
She was initially managed with advice to remain active within pain tolerance, reassurance, and over-the-counter analgesia. She was referred to an endocrinologist with specialization in osteoporosis. Her Risedronate was stopped and she was started on Denosumab as well as calcium and vitamin D supplementation.
Thereafter, she was followed with serial X-rays which demonstrated stability of the listhesis, and she was prescribed physiotherapy. At 1-year follow-up, her pain score was lowered to 5/10 and her ODI score was improved to 31/50. X-rays demonstrated no progression of the listhesis (Figure 4). A CT scan performed 2 years after initial presentation demonstrated healing of the bilateral pedicle fractures (Figure 5).
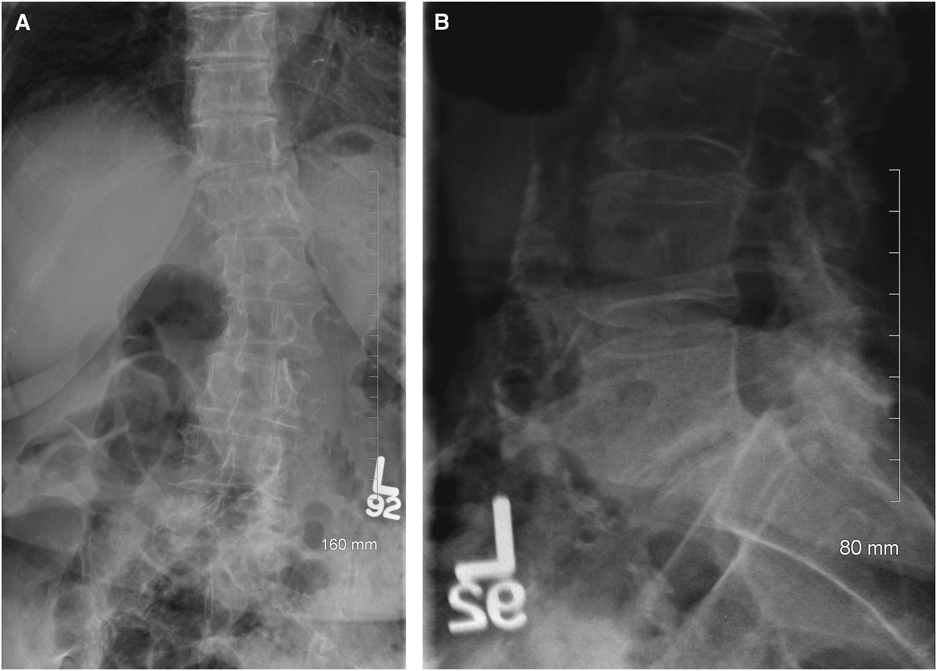
Figure 4 (A,B) Anterior–posterior and lateral X-rays of the lumbar spine performed 1 year after presentation. Demonstrating no progression of listhesis at L5-S1.
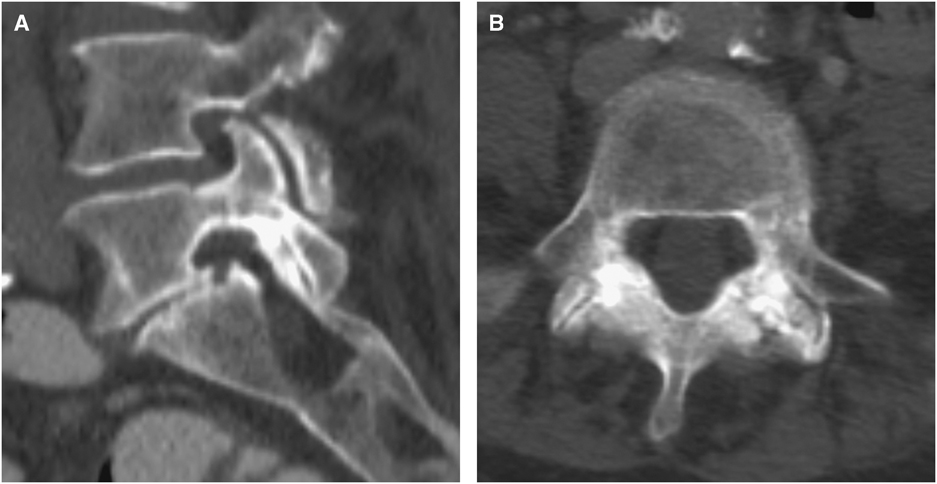
Figure 5 (A,B) Axial and sagittal CT scan of the spine performed 2 years after presentation. Demonstrating healed L5 pedicle fractures and residual grade 1 spondylolisthesis at L5-S1.
There are two types of stress fractures: (1) fatigue fractures which occur in normal bone that is subjected to repetitive abnormal stress and (2) insufficiency fractures which are due to normal stress on a structurally defected bone. Pediculolysis is a fatigue-type stress fracture.Reference Sirvanci, Ulusoy and Duran 4 An in vitro study applying mechanical stress on vertebrae showed that pedicle is the second weakest part of the vertebra after pars interarticularis.Reference Cyron, Hutton and Troup 5
Defects within the pedicle of the lumbar spine may be congenital, traumatic, iatrogenic, or pathologic.Reference Robertson and Grobler 6 They can present as a unilateral pedicle fracture with contralateral pars lysis,Reference Sirvanci, Ulusoy and Duran 4 , Reference Gunzburg and Fraser 7 it can happen in one or more levels in the lumbar spine,Reference Smith, Goorman and Baron 8 , Reference Karabay, Ozer and Ada 9 or they may be associated with spondylolisthesis.Reference Kang, Hong, Park and Suh 2 , Reference Hajjioui, Khazzani and Sbihi 3 In younger adults the diagnosis is extremely rare and is nearly always associated with sports in which hyperextension is common (e.g., ballet), whereas in older adults it is usually due to non-diagnosis of a defect from adolescence presenting later with associated LBP.Reference Abel 10 , Reference Amari, Sakai and Katoh 11
Pedicle stress fractures may present as an acute traumatic fracture or have signs of established pseudoarthrosis.Reference Sadiq 12 Gunzburg and FraserReference Gunzburg and Fraser 7 introduced the term pediculolysis in the 1990s and presented a case of a unilateral stress fracture of the pedicle associated with a contralateral pre-existing spondylolysis. In contrast, we are presenting a case of isolated bilateral pedicle stress fractures that was not present on CT scan 6 months before presentation. Previous reports have presented similar cases, yet they have been in association with previous spine surgery,Reference Macdessi, Leong and Bentivoglio 13 or in the setting of previous osteoporotic vertebral body fractures.Reference Doita, Ando and Hirata 14
Although prolonged bisphosphonate therapy is generally considered safe, it does carry the potential risk of over-suppressing bone turnover, which may compromise the biomechanical bone properties in high stress areas. It also impairs stress fracture healing by blocking the osteoclastic remodeling of callus from woven to lamellar bone.Reference Li, Mori and Kaji 15 , Reference Molvik and Khan 16 This has led to, and has been reported to relate with, the so-called “atypical fractures.” Such atypical fractures associated with bisphosphonate use have been reported previously in the proximal femurReference Ayanaoglu, Atik, Tokgoz and Ucar 17 and other skeletal sites.Reference Marongiu and Capone 18 , Reference Erdem, Atbasi and Emre 19
El Rachkidi et alReference El Rachkidi, Sari-Leret and Wolff 20 suggested that the pedicles may be another site of atypical fracture not previously reported with long-term Risedronate therapy. Karabay et alReference Karabay, Ozer and Ada 9 reported a case of multi-level bilateral pedicle fractures with no other suggestive predisposing factor in which the patient was on a bisphosphonate. Like defects of the pars interarticularis, pedicle stress fractures may heal with bony sclerosis or progress to pseudoarthrosis.Reference Sadiq 12 , Reference Macdessi, Leong and Bentivoglio 13 To date, there is no confirmed method of treatment because of its rarity.Reference Kang, Hong, Park and Suh 2
This report represents one of the first cases of “de novo” atraumatic pedicle insufficiency bilateral fractures without any pre-existing biomechanical risk factors. We believe this type of fracture is easily overlooked on plain radiographs if undisplaced,Reference Lee, Jung, Kim and Kwon 21 thus justifying advanced modalities if suspected. It may be associated with subsequent development of lytic spondylolisthesis, though the strength of such an association is not clear. In our case, the patient had a known history of osteoporosis and prolonged Risedronate use. Thus, future surveillance for this diagnosis may demonstrate an association, especially as the incidence of bisphosphate therapy increases with the burgeoning older patient population.
Statement of Authorship
EKW conceived of the report and contributed to the interpretation of the case, and wrote the first draft. SS, AZS, MME, and DMR contributed further to the interpretation of the case and the writing of subsequent drafts. EKW obtained the necessary diagnostic images. All authors provided critical revisions of the manuscript and approved the final version.