



Task-specific movement disorders are triggered and ended with a task, such as writing or playing an instrument.Reference Rana and Vaid 1 Many of these conditions, failing medical therapy, may be amenable to neurosurgical treatment. Writer’s cramp, a focal dystonia, and task-specific writing tremor are such examples that affect the hand during writing. Their pathophysiology is unclear. Where writer’s cramp is characterized by uncontrollable opposing muscle contractions that result in abnormal repetitive movements or postures,Reference Albanese, Bhatia and Bressman 2 patients with task-specific writing tremor lack dystonic posturing and may have a family history of tremors.Reference Rana and Vaid 1 Nevertheless, these conditions share overlapping motor features such that task-specific writing tremor has been hypothesized to be a variant of writer’s cramp.Reference Rana and Vaid 1
Previous case series of patients with writer’s cramp describe improved symptoms after stereotactic radiosurgery (SRS) or deep brain stimulation (DBS) targeting of the globus pallidus interna (GPi),Reference Yianni, Bain and Gregory 3 the ventralis oralis (VO) nucleus, and/or the ventrointermediate (VIM) nucleusReference Asahi, Koh, Kashiwazaki and Kuroda 4 , Reference Fukaya, Katayama and Kano 5 of the thalamus. Magnetic resonance-guided focused ultrasound (MRgFUS) is an emerging transcranial technique to perform ablation surgeries incision-free.Reference Elias, Lipsman and Ondo 6 It is FDA-approved for treating essential tremor (ET). Magnetic resonance-guided focused ultrasound VIM lesion was described in one patient with writer’s cramp, with a 47% improvement.Reference Fasano, Llinas, Munhoz, Hlasny, Kucharczyk and Lozano 7 We approached our patient diagnosed with writer’s cramp with tandem MRgFUS ablation of the VIM and ventralis oralis posterior (VOP) nucleus, and saw incremental benefit after the VOP lesion.
A 60-year-old right-handed married businessman diagnosed with writer’s cramp by his neurologist was referred to us given his interest in the MRgFUS ablation. Hand tremors and spasms while writing started over 20 years ago and progressively worsened in the last 8 years. Once he learned how to write with his left hand, the left hand became worse. His symptoms did not respond to various medical treatments, namely botulinum toxin injections, primidone, propranolol, and topiramate. His past medical history and family history was otherwise unremarkable. While the patient’s symptoms did not significantly affect his daily activities—he was able to type and drive, the difficulties writing impaired his work as a businessman as he could not even sign his name.
On exam, the patient did not have a resting tremor. There was only a slight intermittent tremor of the right hand when holding his index fingers almost touching. He could raise a cup full of water to his mouth with either hand without difficulty. However, when writing and drawing a circle with his right hand, it was interrupted by spasms of tremor (Figure 1, Supplementary Video). The Clinical Rating Scale for Tremor (CRST), on which the patient scored 30, is part of the outcome measures in the MRgFUS for movement disorder study protocol. It was designed to assess the severity of various tremors in patients with ET, with a maximum score of 152, but may also provide an assessment of any improvements in handwriting or drawing. Finally, MR brain did not demonstrate acute intracranial processes.
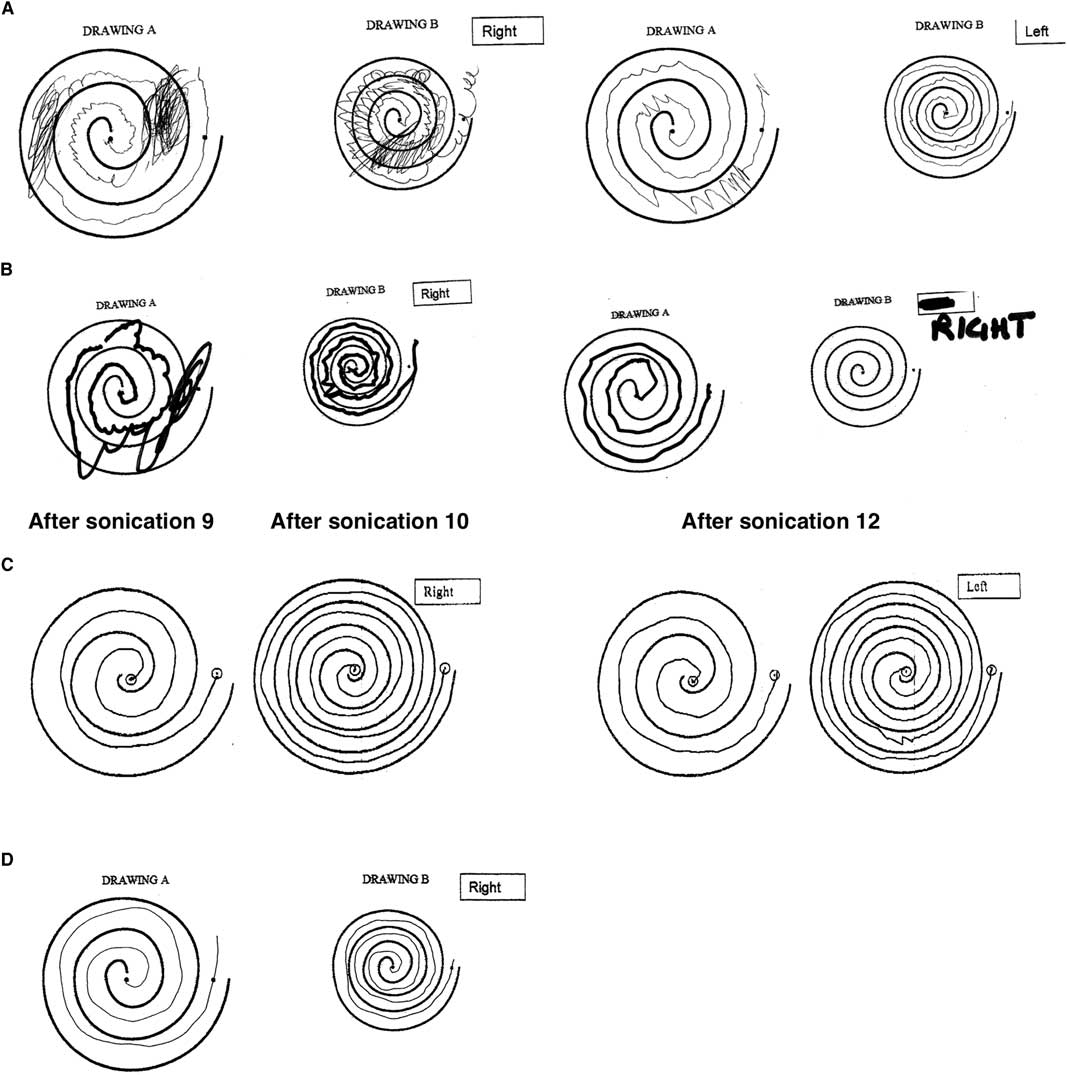
Figure 1 Spiral drawings within large and small spirals are part of the Clinical Rating Scale for Tremor (CRST) to measure the severity of tremor. The patient’s spiral drawings before treatment (A), during treatment after ventrointermediate (VIM) lesion (B left), after ventralis oralis posterior (VOP) lesion (B right), 1 month after (C), and 3 months after treatments (D) are presented. Note the progressive improvement in tracing the spiral as the lesion in VIM is enlarged (sonication 9 and 10) and then further improvement after the single sonication in VOP (sonication 12). Tracings 9, 10 and 12 are, in a sense, a worst case, as they are obtained with the patient immobilized supine just outside the bore of the MRI scanner. The serial comparison shows that the patient’s improvement is durable at 3 months after treatment.
Given the patient’s history of non-response to conventional treatment, we proposed MRgFUS ablation of both the VIM and VOP nuclei of the thalamus with institutional research ethics board approval. We prepared for the procedure as previously described.Reference Elias, Lipsman and Ondo 6 On planning MR, the VIM was estimated to be at 14.3 mm from the midline and 6.4 mm anterior to the posterior commissural line. After the 10th sonication, his ability to draw a spiral moderately improved (Figure 1), but he also reported tingling sensation to the right side of his tongue. Accordingly, a further sonication was made 3 mm anterior to the VIM for the VOP lesion (Figures 1 and 2). Note the progressive improvement as the lesion in VIM is enlarged (sonications 9 and 10) and then further improvement after the single sonication of maximum power of 550 W for 21 seconds in the VOP (sonication 12). The maximum temperature was 58°C. A lesion measuring 7.7 mm in its longest diameter (anteroposterior) was visible on the T2-weighted MRI immediately after sonication and on follow-up studies (Figure 3).
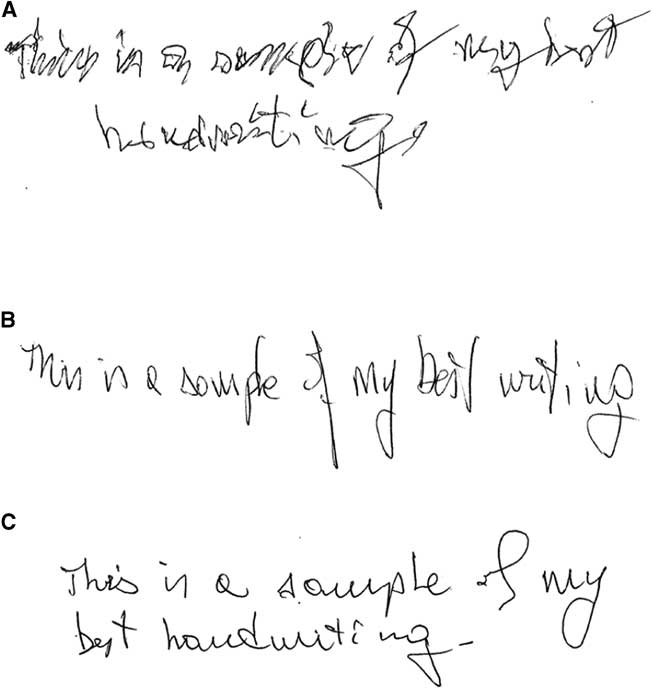
Figure 2 Serial comparisons of the patient’s best handwriting before magnetic resonance-guided focused ultrasound thalamotomy (A), immediately after (B), and 3 months after (C).
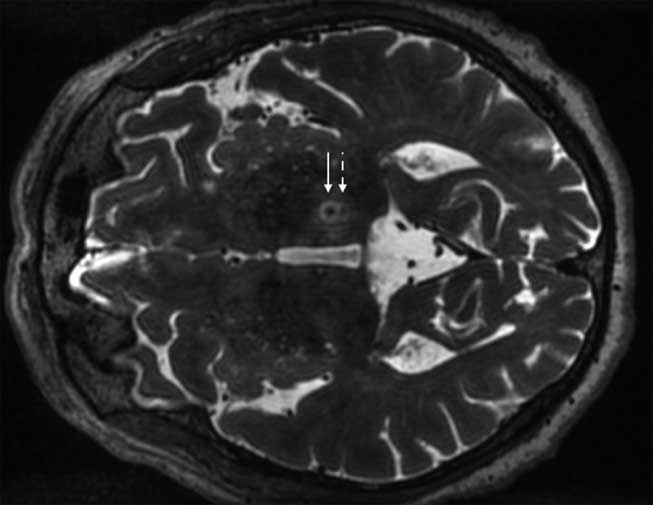
Figure 3 Axial T2 weight magnetic resonance (MR) image shows ventralis oralis posterior (VOP) (full arrow) and ventrointermediate (VIM) (dashed arrow) lesions at 1 month after MR-guided focused ultrasound treatment.
At one month after treatment, the patient reported a complete improvement of his writer’s cramp. On exam, he wrote without any observable difficulties with a total CRST score of 1. However, the tingling to his right tongue persisted along with an “aluminum taste” in his mouth. In addition, he reported a slight clumsiness of his right hand and his gait. We did not observe this objectively, but dysmetria is a known side effect that typically improves with time. His clinical improvement was durable at 3 months (Supplementary Video) and 6 months after treatment with total CRST score of 2 and 2, respectively. Furthermore, the patient reported improvement in the clumsiness, but persistent abnormal taste.
An overview of writer’s cramp literature recorded 25 SRS cases and six DBS cases targeting the GPi, VIM, or VOP, with one case of symptom recurrence and four complications (e.g., mild hemiparesis, dysarthria, and central facial nerve palsy due to thalamic hemorrhage).Reference Asahi, Koh, Kashiwazaki and Kuroda 4 These nuclei are implicated in the motor cortex-basal ganglia-thalamus-cortex loop and thalamo-cerebellum pathway, suspected to be dysfunctional in task-specific movement disorders.Reference Fukaya, Katayama and Kano 5 , Reference Hu, Wang, Liu and Zhang 8
The single optimal target for medically refractory writer’s cramp is debated. Ventrointermediate lesions are thought to provide greater benefit for hyperkinesia, while VO for hypertonia. In a case where two electrodes were implanted to cover both GPi and VO/VIM, disruption of the latter was shown to result in greater improvement in writing.Reference Fukaya, Katayama and Kano 5 Case series published by Goto et alReference Goto, Tsuiki and Soyama 9 suggests that the VO lesion resulted in greater durability of the improvement in task-specific dystonia. Furthermore, VIM in addition to VO may be more effective than VO alone.Reference Fukaya, Katayama and Kano 5 Unfortunately, there is no randomized control trial to compare the effect of surgery to placebo, nor the optimal target or neurosurgical technique.
Magnetic resonance-guided focused ultrasound is an emerging transcranial thermoablation technique. Evidence to support MRgFUS over other neurosurgical approaches (or vice versa) for treatment of movement disorders is sparse, with no prospective comparison studies. One retrospective study suggests equivalent effectiveness of unilateral DBS and MRgFUS thalamotomy to treat patients with medically refractory ET.Reference Huss, Dallapiazza, Shah, Harrison, Diamond and Elias 10 We further allude to the surgical advantages of MRgFUS. First, over SRS, the effect of the MRgFUS lesion is immediate and therefore allows the surgeon to make real-time adjustments. Second, with MRgFUS, the clinician can assess the potential effect of a lesion at sub-lesioning temperature. Lastly, compared with DBS, MRgFUS is transcranial and incision less, thereby obviating the risk of infection, intracranial hemorrhage, hardware malfunction, and maintenance.
There are several disadvantages to MRgFUS thermoablation. First, lesions are permanent and may be associated with a higher rate of disequilibrium and sensory disturbances, at approximately 9% and 14% at 12 months.Reference Elias, Lipsman and Ondo 6 Deep brain stimulation related side effects are potentially reversible with parameter adjustments. Second, the long-term durability of the clinical benefit of MRgFUS thermoablation has not been established, as compared with existing techniques. In the multi-centered study of MRgFUS thalamotomy for ET, the mean CRST score trended upwards at 1 year, although still clinical significantly improved from baseline.Reference Elias, Lipsman and Ondo 6 Outcome studies beyond 1 year after MRgFUS is an area of active research for this emerging technology, and may reasonably improve with accumulating surgeon experience.
We report tandem unilateral MRgFUS VIM and VOP lesioning for writer’s cramp resulting in significant clinical improvement. With the comfort of an awake patient in mind, we began with the VIM nucleus based on our previous experience with MRgFUS lesioning of the VIM for ET, and progressed to the VOP. With the immediate effect of MRgFUS thermoablation, we observed additional benefit from a single sonication of the VOP after VIM. While these observations in addition to a lack of family history of tremor favor writer’s cramp, minimal evidence of dystonic posturing suggests that a diagnosis of task-specific writing tremor is possible. Nevertheless, our case illustrates a potential new neurological indication for MRgFUS thermoablation that is worth further investigation.
Disclosures
YM, SS, NS, and MLS have nothing to disclose. NL reports personal fees from Focused Ultrasound Foundation, outside the submitted work.
Statement of Authorship
All authors contributed to writing and critically revising this manuscript.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/cjn.2018.19





