

Greenough, Black, and Wallace (Reference Greenough, Black and Wallace1987) argued that a critical expected input for the developing brain is contact with a responsive caregiver. Positive dyadic social and emotional exchanges between caregiver and child help the brain organize its neural circuitry and these exchanges contribute to the early development of brain structure. Infants raised in institutional care experience very few individual interactions with caregivers (Smyke et al., Reference Smyke, Koga, Johnson, Fox, Marshall, Nelson and Group2007). Even when basic food and shelter needs are met, these infants are not able to form relationships with responsive adults who consistently meet their needs for social, emotional, and cognitive stimulation (Zeanah, Smyke, Koga, & Carlson, Reference Zeanah, Smyke, Koga and Carlson2005). Because these critical early caregiving experiences are not present, brain architecture may be altered in ways that result in atypical biological and behavioral development (Nelson, Zeanah, & Fox, Reference Nelson, Zeanah, Fox, Romer and Walker2007).
Biologically, empirical work demonstrates that early institutional care alters the hypothalamic–pituitary–adrenal (HPA) axis’ cortisol stress response (Koss, Mliner, Donzella, & Gunnar, Reference Koss, Mliner, Donzella and Gunnar2016; McLaughlin et al., Reference McLaughlin, Sheridan, Tibu, Fox, Zeanah and Nelson2015). Because infants rely solely on caregivers to provide safety, comfort, and meet basic needs, the lack of a consistently responsive and sensitive caregiver is highly stressful for young children in institutional care and triggers frequent activation of the HPA axis. While acute HPA axis responses are necessary for adaptive functioning, prolonged or repeated cortisol elevations can have deleterious effects on the body (Fries, Hesse, Hellhammer, & Hellhammer, Reference Fries, Hesse, Hellhammer and Hellhammer2005). Thus, in response to chronic activation, the body alters HPA axis activity in ways that result in a lower cortisol stress response. Empirical work has provided evidence of this and shown that maltreated children with higher cortisol at an initial assessment show suppression of cortisol over time (Doom, Cicchetti, & Rogosch, Reference Doom, Cicchetti and Rogosch2014). Given this association, it is not surprising that the majority of empirical work finds blunted cortisol reactivity to stress, or hypocortisolism, following early institutional care (however, see also Gunnar, Frenn, Wewerka, & Van Ryzin, Reference Gunnar, Frenn, Wewerka and Van Ryzin2009; Strüber, Strüber, & Roth, Reference Strüber, Strüber and Roth2014). For example, during early childhood, the Koss et al. (Reference Koss, Mliner, Donzella and Gunnar2016) longitudinal study of previously institutionalized (PI) children shows blunted cortisol responses to a laboratory visit across multiple time points. In middle childhood, researchers found PI children ages 8–10 years old to have a blunted cortisol response to a social stressor when compared to nonadopted (NA) youth (Hostinar, Johnson, & Gunnar, Reference Hostinar, Johnson and Gunnar2015). In an experimental study, McLaughlin et al. (Reference McLaughlin, Sheridan, Tibu, Fox, Zeanah and Nelson2015) provide evidence of a causal link between early adversity and blunted HPA axis reactivity at age 12; children aged 2 years or younger that were randomly assigned to be removed from the institutions showed larger cortisol responses to a social stressor than children who were assigned to institutional care as usual and children who were older than age 2 when assigned to removal from institutional care. Together, these studies provide strong evidence for the association between early institutionalization and underactivity of the HPA axis to a stressor, especially prior to adolescence.
In addition to often showing blunted cortisol reactivity to stress, children who experience early institutional care are shown to have poorer mental health, greater emotional problems, and psychopathology, including both internalizing (Bos et al., Reference Bos, Zeanah, Fox, Drury, McLaughlin and Nelson2011; Colvert et al., Reference Colvert, Rutter, Beckett, Castle, Groothues, Hawkins and Sonuga-Barke2008; Ellis, Fisher, & Zaharie, Reference Ellis, Fisher and Zaharie2004; Wiik et al., Reference Wiik, Loman, Van Ryzin, Armstrong, Essex, Pollak and Gunnar2011; Zeanah et al., Reference Zeanah, Egger, Smyke, Nelson, Fox, Marshall and Guthrie2009) and externalizing symptoms (Bos et al., Reference Bos, Zeanah, Fox, Drury, McLaughlin and Nelson2011; Hawk & McCall, Reference Hawk and McCall2010; Merz & McCall, Reference Merz and McCall2010; Wiik et al., Reference Wiik, Loman, Van Ryzin, Armstrong, Essex, Pollak and Gunnar2011). In general, empirical work provides evidence of direct associations between blunted cortisol reactivity and behavioral and mental health problems (e.g., Ayer et al., Reference Ayer, Greaves-Lord, Althoff, Hudziak, Dieleman, Verhulst and van der Ende2013; Ouellet-Morin et al., Reference Ouellet-Morin, Odgers, Danese, Bowes, Shakoor, Papadopoulos and Arseneault2011), though some evidence suggests that blunted cortisol reactivity relates specifically to externalizing problems while hyper-reactivity relates to internalizing problems (see Strüber et al., Reference Strüber, Strüber and Roth2014 for a review). This association may be partially explained by the U shape relation between glucocorticoids (i.e., cortisol) and behavioral functioning that results from differential activation of mineralocorticoid (MR) and glucocorticoid receptors (GR), especially in the hippocampus and the amygdala (Herbert et al., Reference Herbert, Goodyer, Grossman, Hastings, de Kloet and Lightman2006). Because of the U shape, it would be expected that under activity or over activity of the HPA axis during times of stress is associated with suboptimal outcomes. To our knowledge, no study has examined the direct and unique association between cortisol reactivity to stress and concurrent or future behavior problems in PI youth. Previous work from our laboratory, however, provides some support for a potential link. Specifically, Koss et al. (Reference Koss, Mliner, Donzella and Gunnar2016) found that a hypocortisolism latent factor (representing relatively lower diurnal intercept, shallower diurnal slope, and smaller increase in cortisol reactivity across a laboratory visit) during toddlerhood served as a mediator between early adversity and teacher-reported attention and externalizing problems during kindergarten. Thus, prior to adolescence, it appears that lower levels of cortisol and less of a cortisol stress response in PI youth are directly associated with more externalizing problems.
The Adaptive Calibration Model (Del Giudice, Ellis, & Shirtcliff, Reference Del Giudice, Ellis and Shirtcliff2011) posits that stress responses develop as a result of environmental conditions. While in institutions, blunted cortisol reactivity may emerge as a result of chronic activation. When children are removed from institutional care and placed into well-resourced homes with responsive caregivers, we might expect to see an increase or “normalization” in cortisol stress responses as a result of a more enriching environment. Unfortunately, even years after adoption, empirical work finds hypocortisolism in PI children (Koss et al., Reference Koss, Mliner, Donzella and Gunnar2016; Pitula, DePasquale, Mliner, & Gunnar, Reference Pitula, DePasquale, Mliner and Gunnar2019). Moreover, studies have shown that sensitive parenting and adoptive home environments do not substantively alter HPA axis responses to stress or increase cortisol reactivity (Hostinar et al., Reference Hostinar, Johnson and Gunnar2015; Lawler, Koss, & Gunnar, Reference Lawler, Koss and Gunnar2017).
Recently, however, researchers have found evidence to suggest that a window of HPA axis recalibration might emerge across puberty. Endocrine changes that occur across the pubertal period, including increases in androgens and gonadotropins, as well as growth in breast tissue and external genitalia, are initiated and controlled by the same neural and endocrine systems that play a role in the release of cortisol (Dismukes, Shirtcliff, Hanson, & Pollak, Reference Dismukes, Shirtcliff, Hanson and Pollak2015). Thus, this time of great physical and hormonal change may allow the HPA axis to recalibrate, for better or worse, to reflect the degree of supportiveness of the current environment. In two cross-sectional studies involving the cortisol awakening response (CAR), researchers found blunted CAR in children at earlier stages of puberty and increased CAR at later stages (King et al., Reference King, Colich, LeMoult, Humphreys, Ordaz, Price and Gotlib2016; Quevedo, Johnson, Loman, Lafavor, & Gunnar, Reference Quevedo, Johnson, Loman, Lafavor and Gunnar2012). In a cross-sectional study from our laboratory using the same sample as in the current study, we were able to show that early pubertal PI children showed blunted HPA axis reactivity to a social stressor compared to NA children, but PI children who were categorized as being in mid to late puberty showed cortisol reactivity similar to that of their NA counterparts (DePasquale, Donzella, & Gunnar, Reference DePasquale, Donzella and Gunnar2019). Finally, in a follow-up longitudinal study with this sample, data showed within individual increases in pubertal stage were associated with increases in cortisol stress reactivity for PI youth but not NA youth (Gunnar, DePasquale, Reid, Donzella, & Miller, Reference Gunnar, DePasquale, Reid, Donzella and Miller2019). Because the HPA axis shows evidence of recalibration across puberty for PI youth, such that PI youth show increases in cortisol responses to stress, the logical next question is whether these increases are associated with behavioral functioning.
Though some work still finds evidence of hypocortisolism in adulthood (e.g., Kumsta et al., Reference Kumsta, Schlotz, Golm, Moser, Kennedy, Knights and Edmund2017), one possibility is that PI youth who show evidence of recalibration and increased cortisol response to stress also show fewer, or smaller increases in, behavioral problems post puberty. That is, if cortisol reactivity increases to more normative levels, we may not expect it to be associated with psychopathology symptoms. However, some empirical work suggests that internalizing and externalizing symptoms persist, or get more pronounced, as PI children enter adolescence and early adulthood (Fisher, Ames, Chisholm, & Savoie, Reference Fisher, Ames, Chisholm and Savoie1997; Groza & Ryan, Reference Groza and Ryan2002; Humphreys et al., Reference Humphreys, Gleason, Drury, Miron, Nelson, Fox and Zeanah2015). For example, the English and Romanian Adoptees study showed that PI children who experienced more than 6 months of deprivation began to display increases in emotional problems during mid-adolescence (Sonuga-Barke, Schlotz, & Kreppner, Reference Sonuga-Barke, Schlotz and Kreppner2010), and further increases between early adolescence and young adulthood relative to children who experienced little to no deprivation (Sonuga -Barke et al., Reference Sonuga -Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). Additional studies have found externalizing behaviors to increase from early to late adolescence (Verhulst, Reference Verhulst2000; Verhulst & Versluis-Den Bieman, Reference Verhulst and Versluis-Den Bieman1995). Finally, in a meta-analysis, Hawk and McCall (Reference Hawk and McCall2010) reported that several studies found that older children had higher reported rates of extreme behaviors on the Internalizing and Externalizing scales.
Taken together, these studies suggest an alternative possibility; recalibration of the HPA axis during puberty for PI youth initiates a change from hyporeactivity to more normative reactivity (i.e., an increase) which may be subsequently associated with increased psychopathology. If the brain shows alterations in neuro-cognitive systems as a result of early life chronic stress, it may not be equipped to handle the influx of cortisol produced by the body postpuberty, contributing to increased behavioral and emotional difficulties. This may be especially true for internalizing symptoms given the link between hyper HPA reactivity and increased internalizing behaviors in the broader literature (see Strüber et al., Reference Strüber, Strüber and Roth2014). Specifically, the neurocognitive alternations resulting from chronic HPA activation may serve an adaptive role in early adverse settings, but function to increase vulnerability to stress when the body is no longer experiencing adversity. In support of this hypothesis, researchers have demonstrated that children exposed to severe early life neglect show alterations in limbic (Gee et al., Reference Gee, Gabard-Durnam, Flannery, Goff, Humphreys, Telzer and Tottenham2013; Tottenham et al., Reference Tottenham, Hare, Quinn, McCarry, Nurse, Gilhooly and Casey2010; Tottenham et al., Reference Tottenham, Hare, Millner, Gilhooly, Zevin and Casey2011) and fronto-striatal (Behen et al., Reference Behen, Muzik, Saporta, Wilson, Pai and Hua2009; Mehta et al., Reference Mehta, Golembo, Nosarti, Colvert, Mota and Williams2009) circuitry. These neurodevelopmental changes have been posited as potential mechanisms underlying risk for increased anxiety and poorer emotional and behavioral control, which may contribute to risk for internalizing and externalizing disorders.
Finally, we know very little about whether the behaviors PI youth engage in, or their mental state, predicts changes in their cortisol stress reactivity. However, research conducted with typically developing youth provides some evidence of this association. When looking at diurnal cortisol, some research has suggested that youth with externalizing behaviors in childhood had a flatter diurnal cortisol slope by adolescence, but there was no relation with internalizing behaviors (Ruttle et al., Reference Ruttle, Shirtcliff, Serbin, Fisher, Stack and Schwartzman2011). With regard to stress reactivity, Mackrell et al. (Reference Mackrell, Sheikh, Kotelnikova, Kryski, Jordan, Singh and Hayden2014) showed that increased fear and behavioral inhibition at age 7 was associated with greater cortisol stress reactivity at age 9, suggesting longitudinal associations between early emotional problems and increased cortisol reactivity as children approach adolescence. Mindfulness work has shown that reappraising stress-induced arousal is predictive of more adaptive cardiovascular stress responses (Jamieson, Nock, & Mendes, Reference Jamieson, Nock and Mendes2012). Thus, it is possible that children's cognition and behavior may play also play a role in subsequent HPA responses to stress.
The goal of the current study was to longitudinally examine the association between HPA recalibration, or increases in cortisol reactivity, and both internalizing and externalizing symptoms across the pubertal period. This work will help to elucidate whether recalibration of the HPA axis is associated with increases in adaptive functioning or whether increases in HPA activity underlie potential links to developmental psychopathology. We did not focus our investigation on NA children in this analysis, as they did not “recalibrate” or show change in cortisol reactivity across puberty (Gunnar et al., Reference Gunnar, DePasquale, Reid, Donzella and Miller2019). However, to be thorough, those nonsignificant results can be found in supplemental materials, and a description of the NA sample can be found in DePasquale et al., Reference DePasquale, Donzella and Gunnar2019. Because we are the first to investigate the links between cortisol reactivity to stress and behavioral functioning beyond early childhood PI youth, we do not have explicit hypotheses regarding the direction of these associations.
Method
Participants
The participants were 132 children (83 female) who were adopted internationally from institutional (i.e., orphanage) care (previously institutionalized, PI). Children spent at least 50% of their preadoption life in institutionalized care, versus foster care or other arrangements (M = 95%, range 50–100%). Age at adoption ranged from 5.5 to 59 months (M = 19.30 months, SD = 12.47). The children ranged from 7.08 to 15.12 years at the time of testing. As reported in $25,000 increments, the mean income was $100,000–$150,000 per year for adoptive families. Over 75% of the parents had a four-year college degree or higher. Adoptive parents reported that 39% of the children were White, 42% were Asian, 10% indigenous to the Americas, 5% Black or African, 3% were of more than one race, and 1% Other/Unknown. Regarding country of birth, 39% of youth were adopted from Russia, 22% from China, 11% from India, and 6% from Guatemala, 4% from Ukraine, 4% from Colombia, 3% from Vietnam, 2% from Kazakhstan, and 9 from other countries including: Ecuador, Ethiopia, Haiti, Nepal, Philippines, and Slovakia.
Procedures
The children were part of a short-term longitudinal accelerated design examining the association between puberty and stress responding in children with adverse early life histories. All measures were obtained at each visit, and three visits occurred over the span of 2 years, with approximately 1 year between visits (M = 12.23 months, SD = .90 months).
Trier social stress test
Children participated in a modified version of the Trier social stress test for children (TSST-C; Yim, Quas, Rush, Granger, & Skoluda, Reference Yim, Quas, Rush, Granger and Skoluda2015), a commonly used laboratory procedure to induce psychological stress and changes in cortisol concentration (Kirschbaum, Pirke, & Hellhammer, Reference Kirschbaum, Pirke and Hellhammer1993). In this social evaluative task, participants give a 5-min speech, pretending to introduce themselves to an imaginary classroom. Participants were given 5 min to prepare for their speech and write notes but could not use the notes during the speech period. The speech was given in a small room with a one-way mirror and visible camera. The experimenter stood behind the mirror, gave instructions through a speaker, and rated the speech for quality and effectiveness. Participants were told that the experimenter was behind the mirror with a teacher who would also be watching and judging their speech. Instructions before the speech were played from a recording of a male's voice (the teacher) to ensure that all participants heard the same instructions and perceived someone else was behind the mirror to judge their speech. The recording also told children that they were being videotaped so that other students could rate them, adding to the social-evaluative stress of the task. If participants stopped their speech before 5 min, they were told to “continue” by the experimenter over the speaker. The experimenters remained neutral which should increase the uncertainty about one's performance. After the speech section, participants performed a verbal arithmetic task aloud for an additional 5 min, a standard part of the TSST-C.
Cortisol collection
Salivary cortisol was collected four times during the TSST-C (0, +5, +20, and +40 min surrounding the TSST-C). These samples were selected to reflect cortisol reactivity to the task (see DePasquale et al., Reference DePasquale, Donzella and Gunnar2019 for description of all samples), given the lag between when the adrenal secrets cortisol and when it appears in saliva. Sample 0 was collected 40 min after arrival to the lab, prior to the start of the TSST-C, and is considered a baseline or ground from which cortisol may rise in response to the TSST-C. Sample +5 is taken following the speech instructions and speech preparation period and may capture some anticipatory stress; +20 is taken following the speech delivery and math performance; +40 is taken following the completion of the TSST-C. Together, samples +5, +20, and +40 are intended to capture the cortisol reactivity to the TSST-C. The samples were kept frozen at −20°C until being shipped to the University of Trier, Germany to be assayed using a time-resolved fluorescence immunoassay (dissociation-enhanced lanthanide fluorescent immunoassay, DELFIA), with intra- and inter- assay coefficient of variance (CV) < 10%. All of the samples from each participant for a given assessment were included in the same assay batch. Samples were assayed in duplicate, duplicates were correlated > .99 and thus averaged. Because the HPA axis has a strong diurnal rhythm, all TSST-C sessions began between 3.00 and 4.30 p.m. Participants were asked to refrain from eating and drinking (including water and especially caffeine) during the visit. One participant had biologically implausible values (>2 μg/dL at Session 3) and that session was excluded for that participant. Across the three sessions, a total of 10 samples (0.04%) had values greater than 4SD from the mean. It was decided to allow those values to enter the calculation of area under the curve (AUC) to allow natural variation to occur.
Child report
Youth filled out the MacArthur Health and Behavior Questionnaire (HBQ-C 2.l; Essex et al., Reference Essex, Boyce, Goldstein, Armstrong, Kraemer and Kupfer2002), which measures mental health/psychological symptoms, following the completion of the TSST-C. From this, we used the Internalizing scale. We relied on child report of their own internalizing symptoms given that empirical work has shown child self-report of their own mental health to be superior to that of their parent's reports (Rey, Schrader, & Morris-Yates, Reference Rey, Schrader and Morris-Yates1992), and parent report is marginally correlated with child report and associated with parents’ own depression (Choudhury, Pimentel, & Kendall, Reference Choudhury, Pimentel and Kendall2003; Krain & Kendall, Reference Krain and Kendall2000; Wiik et al., Reference Wiik, Loman, Van Ryzin, Armstrong, Essex, Pollak and Gunnar2011).
Parent report
Parents filled out the MacArthur Health and Behavior Questionnaire (HBQ-P 2.1l; Essex et al., Reference Essex, Boyce, Goldstein, Armstrong, Kraemer and Kupfer2002), which measures mental health/psychological symptoms, while the participants were completing the TSST-C. From this, we used the Externalizing scale. Here, we used parent report of externalizing symptoms because we believed parents would be better reporters of children's problem behaviors than children themselves, as children with externalizing behaviors might not recognize them as such. Moreover, by choosing one reporter for externalizing and another for internalizing, we avoid shared-method variance we would have from relying on one reporter for both metrics.
Measures
Cortisol reactivity (AUCi)
Area under the curve with respect to increase (AUCi) is a formula used to capture a cortisol change. Specifically, AUCi emphasizes changes over time and is related to the sensitivity of the hormonal system, as the formula takes into account sensitivity and intensity. Thus, the AUCi formula is useful to derive a stress response over an event period (Fekedulegn et al., Reference Fekedulegn, Andrew, Burchfiel, Violanti, Hartley, Charles and Miller2007) and can be thought of as an index of sensitivity of the system in response to a stressor, in this case, the TSST-C (Morris, Rao, Wang, & Garber, Reference Morris, Rao, Wang and Garber2014). Formulas for the calculation of AUCi are derived from the trapezoid formula, using simple additions of areas of triangles and rectangles (Fekedulegn et al., Reference Fekedulegn, Andrew, Burchfiel, Violanti, Hartley, Charles and Miller2007; Pruessner, Kirschbaum, Meinlschmid, & Hellhammer, Reference Pruessner, Kirschbaum, Meinlschmid and Hellhammer2003). AUCi is calculated from the AUC across samples minus the AUC below the baseline. In the present study, AUCi was calculated from participants’ salivary cortisol from the four timepoints relevant to the TSST, using the initial (prestress) sample as a baseline. To preserve power, any missing samples were imputed as follows: cortisol was taken as the mean of the nearest neighbor samples for a subject, and the modal time across the study for that sample was used. Imputations were only performed if a person was missing a single sample. This resulted in four imputations across all three sessions, or 0.01%. Thus, AUCi was included to examine participants’ cortisol response sensitivity to the speech and math task, with higher scores representing greater cortisol reactivity during the TSST-C.
Children's internalizing symptoms
Children's internalizing symptoms were assessed from self-report using the Internalizing scale of the HBQ-C. Internalizing comprised three subscales: depression, separation anxiety, and overanxious. For each item, children selected “sort of like me,” “mostly like me,” or “really like me” to one of two contrasting statements; for example, “When I meet new kids, I am shy” or “When I meet new kids, I am not shy”. The internalizing subscale had good internal reliability within our sample (38 items, α ranged across three assessments = .90–.93). Using the clinical cutoff of 3.55 for the Internalizing scale of the HBQ-C that was reported in the study by Wiik et al., Reference Wiik, Loman, Van Ryzin, Armstrong, Essex, Pollak and Gunnar2011, only 4–5% of PI youth at each session could be classified at a clinical level.
Children's externalizing symptoms
Children's externalizing symptoms were assessed from parent report using the Externalizing scale of the HBQ-P. Externalizing comprised four subscales: opposition/defiance, conduct problems, overt hostility, and relational aggression. Parents selected “never or not true,” “sometimes or somewhat true,” or “often or very true” to each question. The externalizing subscale had good internal reliability within our sample (38 items, α ranged across three assessments = .89–.93). Using the clinical cutoff of .68 for the Externalizing scale of the HBQ-P that was reported by Lemery-Chalfant et al. (Reference Lemery-Chalfant, Schreiber, Schmidt, Van Hulle, Essex and Goldsmith2007), only 1%–4% of PI youth at each session could be classified at a clinical level.
Data analytic plan
Autoregressive cross-lagged panel models with structured residuals (Berry & Wiloughby, Reference Berry and Wiloughby2017; Curran, Howard, Bainter, Lane, & McGinley, Reference Curran, Howard, Bainter, Lane and McGinley2014) were used to examine concurrent and cross-lagged associations between (a) cortisol reactivity and child-reported internalizing symptoms and (b) cortisol reactivity and parent-reported externalizing symptoms across three time points during the pubertal transition. Data were analyzed using the ‘lavaan’ package in R (R Core Team, 2016; Rosseel, Reference Rosseel2012). Missing data were handled using full-information maximum likelihood.
First, univariate models were built through the systematic addition of paths. Comparison of model fit was used to determine whether adding additional paths better explained associations among model variables. Good model fit was determined by comparative fit index (CFI) and Tucker–Lewis index (TLI) > .95 (Bentler, Reference Bentler1990; Tucker & Lewis, Reference Tucker and Lewis1973), and root mean squared error of approximation (RMSEA) and standardized root mean squared residual (SRMR) < .08 (Hu & Bentler, Reference Hu and Bentler1999; MacCallum, Browne, & Sugawara, Reference MacCallum, Browne and Sugawara1996). Model fit was compared using the chi-square test of difference using the ‘analysis of variance’ (ANOVA) base R function. The more complex model was chosen only if it resulted in a significant improvement in model fit. For each univariate model (cortisol reactivity, internalizing symptoms, and externalizing symptoms) a latent slope was fit on its own to demonstrate whether there is linear change in sample means over time. For each model, a latent slope did not provide a good fit to the data. Thus, a latent intercept model with autoregressive paths over time (autoregressive paths held constant) was compared to a model with a latent intercept and the best fitting model (favoring parsimony) was accepted.
Once univariate models were determined, two bivariate models were created: one assessing the associations between cortisol reactivity and child-reported internalizing symptoms and the other assessing the associations between cortisol reactivity and parent-reported externalizing symptoms. In both models, latent intercepts were allowed to correlate. Then, correlations among variable residuals within timepoint (i.e., concurrent associations, held constant over time) and all cross-lagged paths capturing bidirectional associations (cortisol to internalizing/externalizing and internalizing/externalizing to cortisol) were included. This model was compared to the bivariate model without concurrent and cross-lagged paths. The best fitting model (favoring parsimony) was accepted.
A time-variant covariate of child age and a time-invariant covariate of child sex were included in both bivariate models. To account for the correlation between internalizing and externalizing symptoms, mean parent-reported externalizing was included as a time-invariant covariate of child-reported internalizing for the cortisol/internalizing model. Similarly, mean child-reported internalizing was included as a time-invariant covariate of parent-reported externalizing for the cortisol/externalizing model. An index of daily medication use, scored using methods described by Granger, Hibel, Fortunato, and Kapelewski (Reference Granger, Hibel, Fortunato and Kapelewski2009), was examined as a potential time-variant covariate of cortisol reactivity. However, it did not significantly predict cortisol reactivity at any time point, so it was not included in the model.
Results
Descriptive statistics
Means, standard deviations, and intercorrelations among focal variables are displayed in Table 1. Child-reported child internalizing symptoms were highly correlated over time, as were parent-reported child externalizing symptoms. Internalizing symptoms and externalizing symptoms were modestly interrelated. Session 1 and 2, but not Session 3, cortisol AUCi were significantly associated. Notably, Session 2 cortisol AUCi was negatively associated with internalizing symptoms at Sessions 2 and 3, but Session 3 cortisol AUCi was positively associated with Sessions 2 and 3 internalizing. Cortisol AUCi was not significantly associated with externalizing symptoms.
Table 1. Descriptives and intercorrelations among all focal variables (N = 132).

* p < .05, **p < .01, ***p < .001.
AUCi = area under the curve with respect to increase
Univariate model building
When modeling cortisol reactivity, the latent intercept model with autoregressive paths (CFI = .96, TLI = .96, RMSEA = .03, SRMR = .06) fit significantly better than the latent intercept model without autoregressive paths (χ2 (1, N = 132) = 9.71, p = .002). Thus, both were included when modeling cortisol reactivity in the bivariate models described below. With regard to externalizing behaviors, the latent intercept model with autoregressive paths did not fit significantly better than the latent intercept model without autoregressive paths (CFI = .95, TLI = .90, RMSEA = .11, SRMR = .04; χ2 (1, N = 132) = 2.40, p = .12). Thus, only a latent intercept was included when modeling parent-reported externalizing symptoms in the bivariate models. For internalizing symptoms, the latent intercept model with autoregressive paths (CFI = 1.00, TLI = 1.00, RMSEA = .00, SRMR = .04) fit significantly better than the latent intercept model without autoregressive paths (χ2 (1, N = 132) = 8.56, p = .003). Thus, both were included when modeling child-reported internalizing symptoms in the bivariate models.
Cortisol reactivity and parent-reported externalizing symptoms
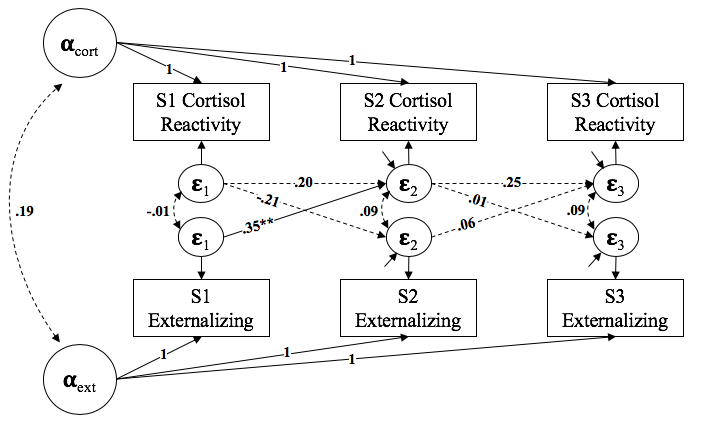
The bivariate model of cortisol reactivity and externalizing symptoms that included concurrent and cross-lagged paths did not provide significantly improved model fit compared to the model that did not include concurrent and cross-lagged paths (CFI = .97, TLI = .96, RMSEA = .07, SRMR = .06; χ2 (6, N = 132) = 3.32, p = .77) (See Figure 1). Thus, the cross-lagged bivariate model was not interpreted. This finding suggests no association between cortisol reactivity and externalizing symptoms across puberty for PI youth. Instead, the majority of the variance in externalizing symptoms was accounted for by the latent intercept, indicating strong stability in parent-reported externalizing symptoms over time.

Figure 1. Final autoregressive cross-lagged panel model results for cortisol reactivity-externalizing symptom associations. Comparative fit index (CFI) = .97, Tucker–Lewis index (TLI) = .96, root mean squared error of approximation (RMSEA) = .07, standardized root mean squared residual (SRMR) = .06. Standardized estimates are shown. Covariates of child age, sex, and mean child-reported internalizing symptoms are not shown here for clarity but are accounted for in the model. Significant paths are shown with solid lines, while nonsignificant paths are shown with dotted lines. **p < .01.
Cortisol reactivity and child-reported internalizing symptoms
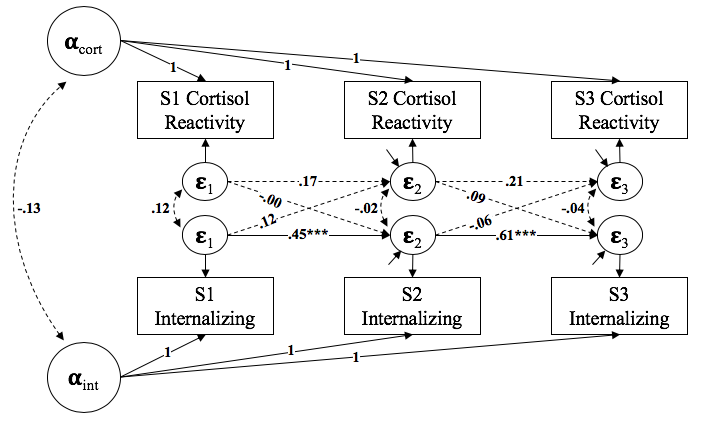
The bivariate model of cortisol reactivity and internalizing symptoms that included concurrent and cross-lagged paths (CFI = .99, TLI = .99, RMSEA = .05, SRMR = .05) showed a significant improvement in model fit compared to the bivariate model without concurrent and cross-lagged paths (χ2 (6, N = 132) = 29.35, p < .001). Thus, the cross-lagged model was interpreted. Model fit statistics and standardized coefficients can be found in Figure 2.

Figure 2. Final autoregressive cross-lagged panel model results for cortisol reactivity–internalizing symptom associations. Comparative fit index (CFI) = .99, Tucker–Lewis index (TLI) = .99, root mean squared error of approximation (RMSEA) = .05, standardized root mean squared residual (SRMR) = .05. Standardized estimates are shown. Covariates of child age, sex, and mean parent-reported externalizing symptoms are not shown here for clarity, but are accounted for in the model. Significant paths are shown with solid lines, while nonsignificant paths are shown with dotted lines. *p < .05, **p < .01, ***p < .001.
Results show evidence for bidirectional associations between cortisol reactivity and internalizing symptoms across puberty such that increases in cortisol reactivity predicted increases in internalizing behaviors and increases in internalizing behaviors predicted increases in cortisol reactivity. Specifically, greater cortisol reactivity at Session 1 significantly predicted internalizing symptoms at Session 2, accounting for previous levels of internalizing symptoms at Session 1 (see Figure 2). The same pattern emerged when looking at cortisol reactivity at Session 2; cortisol reactivity at Session 2, controlling for cortisol reactivity at Session 1, predicted greater internalizing symptoms at Session 3 after controlling for previous levels of internalizing symptoms at Session 1 and Session 2.
Conversely, internalizing symptoms at Session 1 significantly predicted cortisol reactivity at Session 2, accounting for previous levels of cortisol reactivity at Session 1 (see Figure 2). Again, the same pattern emerged when looking at internalizing symptoms at Session 2; internalizing symptoms at Session 2, controlling for internalizing symptoms at session 1, predicted greater cortisol reactivity at Session 3 after controlling for previous levels of cortisol reactivity at Session 1 and Session 2.
Discussion
In the current study, we examined the relation between recalibration of the HPA axis in PI youth and changes in both internalizing and externalizing symptoms. The focus was on youth adopted from institutions as these youth demonstrated hypocortisolism that did not normalize in the initial years postadoption (Koss et al., Reference Koss, Mliner, Donzella and Gunnar2016) but, as a group, did show HPA axis recalibration during puberty. Recalibration involved a shift from hyporeactivity to reactivity more closely resembling that of same-aged never-institutionalized peers, resulting in an increase in cortisol reactivity with increasing pubertal stage (Gunnar et al., Reference Gunnar, DePasquale, Reid, Donzella and Miller2019).
Given that PI youth shift from hyporeactivity to more normative levels of cortisol reactivity during puberty, we might expect the association between cortisol reactivity and behaviors problems to weaken or diminish throughout the pubertal period. Our findings regarding externalizing problems supported this hypothesis such that we found no significant cross-lagged effects in either direction. Previous work has not examined the direct association between externalizing behaviors and cortisol reactivity in PI youth, though Koss et al. (Reference Koss, Mliner, Donzella and Gunnar2016) did include cortisol reactivity to a laboratory visit in their hypocortisolism latent factor. However, the broader literature suggests that blunted cortisol responses to stress are more strongly associated with externalizing rather than internalizing symptoms (Strüber et al., Reference Strüber, Strüber and Roth2014), especially in early and middle childhood. Thus, if PI youth no longer show blunted HPA reactivity due to recalibration of the HPA axis, then this may explain the lack of association between externalizing behaviors and cortisol reactivity we find as children transition to adolescence. It should also be noted, however, that the significant stability in externalizing behaviors in our sample across the three sessions (see Table 1) also plays a role in these null findings such that there may be too little within-individual variability in externalizing symptoms over time to detect significant associations with cortisol reactivity. Moreover, very few young people had externalizing symptoms that reached clinical levels.
An alternative hypothesis is that HPA axis recalibration, and subsequent increases in cortisol reactivity, may be associated with increased psychopathology if neuro-cognitive systems are not equipped to handle the influx of glucocorticoids postpuberty. Our findings also provide support for this hypothesis. We found longitudinal bidirectional associations indicating that increases in cortisol reactivity were associated with increases in internalizing symptoms and increases in internalizing symptoms were associated with increases in cortisol reactivity. These associations emerged across the three sessions and held over and above the stability in cortisol reactivity and internalizing symptoms over time.
Importantly, though, our results must be interpreted in the context of the normative level of internalizing symptoms reported by PI youth in our sample. Using the clinical cutoff that was reported in the study by Wiik et al., Reference Wiik, Loman, Van Ryzin, Armstrong, Essex, Pollak and Gunnar2011, only 4%–5% of PI youth at each session could be classified at a clinical level. Thus, although associations between these constructs emerged such that increases in one domain predicted increases in the other, the majority of this movement was still within a normative range. Nonetheless, the findings from the current study are noteworthy and provide valuable insight into the links between biological and behavioral stress responses in PI youth across the pubertal period, an area that has received no investigation.
Because previous work demonstrates that internalizing symptoms can persist or increase in mid-adolescence and early adulthood for PI youth (Hawk & McCall, Reference Hawk and McCall2010; Sonuga -Barke et al., Reference Sonuga -Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017; Sonuga-Barke et al., Reference Sonuga-Barke, Schlotz and Kreppner2010), it is not entirely surprising that one predictor of these increases is the change in cortisol reactivity that can occur as the HPA axis recalibrates across puberty. However, the mechanisms that underlie this association are unclear.
One possible explanation is that alterations in brain structure that develop in response to early life adversity are incompatible with more normative biological responses that emerge when the HPA axis recalibrates. For example, glucocorticoids bind to MRs and GRs in the brain but have a higher affinity to bind to MRs (De Kloet, Reul, & Sutanto, Reference De Kloet, Reul and Sutanto1990). Under nonstress conditions, when glucocorticoid levels are lower, glucocorticoids bind more readily to MRs, which serves to regulate basal functions such as circadian rhythm. When acute stress is experienced and glucocorticoid levels rise, GR binding increases, which contributes to the body's stress response, memory storage, and negative feedback regulation (De Kloet, Reference De Kloet2013). Rodent studies have shown that chronically elevated glucocorticoid levels due to early life stress (low maternal licking and grooming) can ultimately downregulate expression of MR and GR receptors in the hippocampus (Champagne et al., Reference Champagne, Bagot, van Hasselt, Ramakers, Meaney, De Kloet and Krugers2008; Liu et al., Reference Liu, Diorio, Tannenbaum, Caldji, Francis, Freedman and Meaney1997; Sapolsky, Krey, & McEwen, Reference Sapolsky, Krey and McEwen1986). In line with rodent models, it is possible that early institutional care and chronic elevation of glucocorticoids in early infancy impact the neural structures of the developing forebrain, resulting in reduced MR/GR receptor expression and altered MR/GR binding. Eventual downregulation of the HPA axis under chronic stress, as we see in PI youth, may be an adaptive response to avoid glucocorticoid toxicity (Fries et al., Reference Fries, Hesse, Hellhammer and Hellhammer2005), but it may be additionally adaptive such that it maintains a similar MR/GR binding ratio as when both glucocorticoid production and MR/GR receptor expression was higher. However, as the HPA axis recalibrates across puberty, and cortisol reactivity increases, the influx of cortisol may bind to more GRs, resulting in increased internalizing symptoms (De Kloet, Reference De Kloet2014). In other words, the structure of the brain may have adapted to hypocortisolism early on such that increases to more typical levels may be considered “too much,” exacerbating internalizing, but not necessarily externalizing, symptoms (Strüber et al., Reference Strüber, Strüber and Roth2014).
Though a plausible theory, the MR/GR balance hypothesis is difficult to directly test in humans and little research has examined how neural programming of glucocorticoid receptors impacts changes in psychopathology across pubertal development. Future research is needed to replicate and extend the findings of the current study. Rodent models have shown that the downregulation of MR and GR receptors in the hippocampus can be rescued by the administration of antidepressants (Park et al., Reference Park, Lee, Seo, Ly, Lee, Cho and Kim2017), suggesting a potential intervention for PI youth whose internalizing symptoms reach clinical severity.
Although a significant amount of empirical work investigates the association between HPA functioning and concurrent or subsequent problem behaviors, relatively little work considers the opposite hypothesis. Our work is unique in that we were able to consider both directions simultaneously, thereby accounting for one while investigating the other. Thus, in addition to cortisol reactivity predicting increases in internalizing behaviors, we were able to show that increases in internalizing behaviors predicted increases in cortisol over time. As previously mentioned, there is some evidence to suggest that cognition can alter biological responses to stress (e.g., Jamieson et al., Reference Jamieson, Nock and Mendes2012). For example, one study found that telling participants to actively think about and reappraise a laboratory stressor resulted in increased cortisol reactivity (Denson, Creswell, Terides, & Blundell, Reference Denson, Creswell, Terides and Blundell2014). If adolescents report increased internalizing symptoms more generally, they may also be more likely to anticipate or ruminate over participating in the stressor in the laboratory. Therefore, if participants are ruminating or are focused on their experienced anxiety while engaging in the social stress task, this could help to explain why increases internalizing symptoms are associated with increases in cortisol reactivity.
Taken together, these findings show the importance of looking at bidirectional effects of biobehavioral associations in order to better understand how cortisol reactivity and mental health are associated over time, even when concurrent associations are not present. Our findings suggest that current feelings of anxiety may not always be associated with current cortisol levels, especially when removing variance associated with individual's trait-like anxiety. However, increased internalizing symptoms may predict a stronger biological response next time youth encounter a social stressor if they can recall their previous feelings of anxiety and are prone to more anxious behavior. In addition, it is also possible that increases in cortisol reactivity to stress prime the body to experience increased anxious states across a variety of challenging situations, therefore leading to greater reports of internalizing symptoms over time.
Evidence also shows that there may be a cyclical association where increased cortisol and internalizing symptoms exacerbate one another across the puberty period. However, this is the first study to examine how pubertal recalibration of the HPA axis may be associated with youth's behavioral functioning so further evidence of this is needed. We might assume that recalibrating to normative cortisol reactivity levels would be associated with positive outcomes for PI youth, but the present study suggests that may not always be true. We do not know what happens beyond puberty. It could be that increases in cortisol reactivity level off or even drop back to their prepubertal levels. Moreover, it is unclear whether internalizing behaviors for PI youth continue to increase into adulthood, or if recalibration of behavioral symptoms merely lag behind biological recalibration. More work is needed to better understand whether these changes are limited to adolescence, a period of increased stress and biological change, or if they have implications into early adulthood such as more long-term or stable aspects of mental health and psychological functioning.
Although the current study provides valuable insight into the associations between cortisol and behavior during puberty, it is not without limitations. First, we did not directly assess pubertal change in the current analysis. However, previous work with this sample provides evidence of increases in cortisol for PI youth with increasing pubertal development during this period (Gunnar et al., Reference Gunnar, DePasquale, Reid, Donzella and Miller2019). Second, the relatively low levels of behavioral symptoms reduce the clinical relevance of our findings. Because most PI youth in the current study did not reach clinical levels of internalizing or externalizing behaviors, it is unclear how increases in internalizing symptomology over time impacts normal daily functioning and social interactions. Finally, PI youth are not representative of children experiencing other types of early adversity such as maltreatment or extremely poverty. Thus, additional work is needed to better understand whether changes in biological functioning occur for these individuals across puberty and how these potential changes relate to multiple aspects of psychopathology.
For decades, Megan Gunnar's work has laid the foundation for scientists to better understand the role of early adversity on stress biology and neurobehavioral development. Her work has provided a considerable amount of evidence suggesting that early institutional care has deleterious impacts on the development of the HPA axis and behavioral functioning. Recently, she has shown that puberty may open a window for the HPA axis to recalibrate to children's more resource-rich environments. However, whether changes in HPA stress reactivity that occur across the pubertal period are associated with changes in behavior is unknown. The current study adds to this rich literature and special issue by using a longitudinal approach to examine how changes in stress reactivity among children who experienced early life stress are associated with changes in neurobehavioral functioning. Findings suggest that although the HPA axis may recalibrate, resulting in more typical cortisol stress responses for PI youth, these biological changes may not always be associated with adaptive outcomes.
Supplementary Material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579420001297
Acknowledgments
The authors thank the families, who devoted many hours to the longitudinal study from which the current data were taken. Additional thanks go to all the staff and students who helped recruit participants and collect and process the data.
Funding Statement
This research was supported by a grant from the National Institute of Child Health and Human Development through the National Institutes of Health [5R01 HD075349] to the final author.
Conflicts of Interest
None





 Open access
Open access