



Introduction
The human nervous system needs a long time of environmental and social inputs in early life to achieve adult levels of maturity. This slow pace of development allows offspring to grow refined cognitive, social, and behavioral skills to effectively adapt to the external environment (Del Giudice et al., Reference Del Giudice, Ellis and Shirtcliff2011; Kolacz et al., Reference Kolacz, Kovacic and Porges2019). In this scenario, childhood maltreatment (CM) represents a violation of the expectable environment able to increase the risk for atypical variations in brain development that in turn are associated with a variety of psychological, behavioral, and physical health sequelae (Nelson & Gabard-Durnam, Reference Nelson and Gabard-Durnam2020), demonstrated also among social, long-lived nonhuman mammals (Dettmer & Chusyd, Reference Dettmer and Chusyd2023). Amid various concerning consequences, recent studies have directed attention to the influence of CM on individuals’ social functioning (Maercker et al., Reference Maercker, Cloitre, Bachem, Schlumpf, Khoury, Hitchcock and Bohus2022; McCrory et al., Reference McCrory, Foulkes and Viding2022; Holz et al., Reference Holz, Berhe, Sacu, Schwarz, Tesarz, Heim and Tost2023). People exposed to CM report increased social isolation, less adaptive social relationships and impaired emotional intelligence (Pfaltz et al., Reference Pfaltz, Halligan, Haim-Nachum, Sopp, Åhs, Bachem, Bartoli, Belete, Belete, Berzengi, Dukes, Essadek, Iqbal, Jobson, Langevin, Levy-Gigi, Lüönd, Martin-Soelch, Michael, Oe, Olff, Ceylan, Raghavan, Ramakrishnan, Sar, Spies, Wadji, Wamser-Nanney, Fares-Otero, Schnyder and Seedat2022). More specifically, children and adolescents exposed to CM present altered behavioral and physiological responses to others’ emotions. At a behavioral level, several studies demonstrated the presence of a systematic recognition bias, according to which people exposed to CM are more inclined to erroneously identify others’ negative and neutral facial expressions as anger (Ardizzi et al., Reference Ardizzi, Martini, Umiltà, Sestito, Ravera and Gallese2013, Reference Ardizzi, Martini, Umiltà, Evangelista, Ravera and Gallese2015, Reference Ardizzi, Evangelista, Ferroni, Umiltà, Ravera and Gallese2017; Pollak et al., Reference Pollak, Cicchetti, Hornung and Reed2000; Pollak & Kistler, Reference Pollak and Kistler2002; Pollak & Sinha, Reference Pollak and Sinha2002; Pfaltz et al., Reference Pfaltz, Passardi, Auschra, Fares-Otero, Schnyder and Peyk2019). At a physiological level, reduced spontaneous facial mimicry – defined as the automatic, rapid, and congruent electromyographic muscular reaction to others’ facial expressions supporting empathic processes – was found in children and adolescents exposed to CM (Ardizzi et al., Reference Ardizzi, Martini, Umiltà, Sestito, Ravera and Gallese2013, Reference Ardizzi, Umiltà, Evangelista, Di Liscia, Ravera and Gallese2016). Moreover, both sympathetic and parasympathetic responses to emotional signals seemed maladaptive among maltreated kids (Ardizzi et al., Reference Ardizzi, Martini, Umiltà, Sestito, Ravera and Gallese2013, Reference Ardizzi, Umiltà, Evangelista, Di Liscia, Ravera and Gallese2016; McLaughlin et al., Reference McLaughlin, Sheridan and Lambert2014; Reference McLaughlin, Sheridan and Nelson2017). Overall, these studies show that CM profoundly interferes with victims’ affective and social development by placing them at a severe disadvantage in mature the physiological substrates of a full empathic automatic understanding of others’ emotions and self-regulation abilities in social contexts.
Considering the established protective advantages associated with proficient social skills for those who have undergone CM (Pfaltz et al., Reference Pfaltz, Halligan, Haim-Nachum, Sopp, Åhs, Bachem, Bartoli, Belete, Belete, Berzengi, Dukes, Essadek, Iqbal, Jobson, Langevin, Levy-Gigi, Lüönd, Martin-Soelch, Michael, Oe, Olff, Ceylan, Raghavan, Ramakrishnan, Sar, Spies, Wadji, Wamser-Nanney, Fares-Otero, Schnyder and Seedat2022), it is imperative to swiftly grasp the role played by specific moderating factors in the connection between CM and victims’ social functioning.
Generally, the extremely heterogeneous impact that CM exerts on social development has been associated to the influence of specific factors, namely: type of maltreatment (distinct sub-categories of maltreatment induce differential effects), timing (the effect of maltreatment depends on the developmental time period of the exposure), duration of exposure (every additional year of exposure to CM is associated with increased risk) and severity (the effect varies according to the severity of the stressor).
A recent conceptual framework distinguishes between experiences of deprivation (i.e., lacking anticipated environmental inputs and complexity, like neglect) and threat (i.e., encountering experiences that pose a threat to one’s physical integrity, like physical or sexual abuses), indicating a discernible impact of these two on social development (McLaughlin et al., Reference McLaughlin, Sheridan and Lambert2014; Machlin et al., Reference Machlin, Miller, Snyder, McLaughlin and Sheridan2019; Peterson et al., Reference Peterson, Zhu, Germine and Dunn2022; Sheridan & McLaughlin, Reference Sheridan and McLaughlin2014). On the one hand, deprivation may limit opportunities for a child to learn to navigate social encounters through observing the behavior and reactions of others, thus reducing cognitive stimulation and social nurturing. On the other hand, physical or sexual abuse may lead to a hypersensitive response to aversive stimuli, thereby altering neural circuits, similar to findings associated with fear learning. Importantly, this model does not propose that deprivation and threat occur independently for children rather, they are dimensions co-occurring in CM experiences which impact can be, in some cases, measured separately. Numerous studies have explored the influence of temporal factors related to CM (i.e., timing and duration) on the social development of the victims. Consistently, there is a prevailing emphasis on the significance of duration (Crawford et al., Reference Crawford, Choi, Davis, Zhu, Soare, Smith, Germine and Dunn2022; Moss et al., Reference Moss, Loxton and Mishra2023; Peterson et al., Reference Peterson, Zhu, Germine and Dunn2022; Ross et al., Reference Ross, Handley, Toth and Cicchetti2023), aligning with the “accumulation of risk model”. This model suggests that each additional year of exposure to CM is consistently linked to an increased risk of poor health (Dunn et al., Reference Dunn, Soare, Raffeld, Busso, Crawford, Davis, Fisher, Slopen, Smith, Tiemeier and Susser2018). Lastly, the severity factor is seldom examined in isolation from the others, given its inherent connection to the number of episodes, the diversity of exposure types, the duration, and early occurrence of the stressors.
In line with this framework, the present study endeavors to scrutinize the specific trajectory of the influence exerted by the duration of CM on social development. While prior studies have underscored the pivotal role of CM duration in shaping victims’ social development, they have primarily concentrated on linear trajectories without considering the potential existence of diverse patterns. Uncovering the configuration of the impact trajectory associated with CM duration will unveil natural patterns of resilience, improvement, deterioration, and chronicity. This insight will offer valuable cues for designing and implementing coherent evidence-based rehabilitative interventions.
In a cross-sectional design covering 5–18 years of age, the affective and social development of maltreated children and adolescents has been investigated. Three different impact trajectories of CM duration have been tested: (i) a linear trajectory, describing a proportional additive effect; (ii) a logarithmic trajectory, defining a habituation or a charging effect according to which some years have greater or lower impact than others and (iii) a quadratic trajectory, describing an inversion trend in which the first years have a different impact than the last years.
Affective and social development was operationalized by drawing on prior research, with emphasis placed on both behavioral indicators (the percentage of anger false alarms in a forced-choice facial expressions identification task) and physiological markers (facial mimicry and autonomic regulation of the heart).
The study was conducted on a group of maltreated Sierra Leonean youths all abandoned at the age of 4, who still homeless at the time of the study. This group of youths was highly homogeneous in terms of CM timing (onset at 4 years of age) and type. Their affective and social development was compared with that of matched control participants. If CM duration shifts the typical pattern of social and affective development, we expect to highlight distinct trajectories exerted by Duration between the 2 groups. The trajectories’ type will be interpreted considering the specific quality of CM duration.
Method
Participants
The present study was conducted in Sierra Leone. Sierra Leone is one of the poorest countries in the world - ranking 181 out of 191 in the UN Human Development Index (Human Development Report 2021-2022) – and sadly known for the Sierra Leone Civil War (1991–2002) and the Ebola outbreak (2014). In Sierra Leone the 52% of people live below the poverty line, this percentage increases to 77% when considering children (Sierra Leone Child Poverty Report, 2016). Although an official census is not available, a recent survey (“Homelessness Situation in Freetown” by Social Workers Sierra Leone) declares that in 2023 the 19% of the homeless population in Sierra Leone are unaccompanied children. People get homeless mainly because of neglect or lack of support by family members and the larger community. The 54% of the unsheltered population became homeless before they were 15 years old, illustrating the significant social issue of child homelessness.
In this scenario, a total of 73 Sierra Leonean underage participants (age range 5–17 years), all males, were involved in the study (Table 1). All participants and their legal guardians or local mediators filled a written informed consent after oral explanation of the study general purposes and procedures. The local mediators were social workers or healthcare professionals who acted as facilitators and supervisors of the homeless children who did not have a legal guardian. The total sample size exceeded the minimum amount required (N = 61) estimated with statistical a priori sample size calculation, obtained for repeated-measures MANOVA considering both within and between interactions (1-ß = 0.90, α = 0.05 and effect size f = 0.50). Participants’ demographic and health information, together with their maltreatment history were collected through systematic interviews and further completed and checked thanks to sanitary, educational, and forensic local institutions.
Table 1. Sociodemographic characteristics of maltreated (Mal) and control (Con) groups
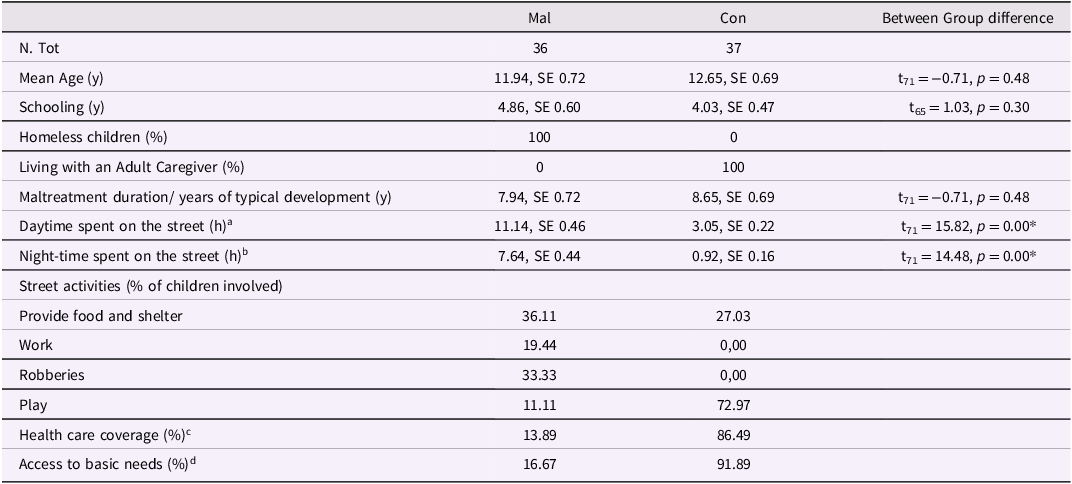
a Day-time: from 5:00 a.m. to 6:59 p.m.
b Night-time: from 7:00 p.m. to 4:59 a.m.
c Health care coverage was defined as participants’ access to preventive healthcare (i.e., vaccination, disease screening, malaria protection) and basic disease treatments (i.e., treatment of malaria, fever and diarrhea).
d Access of basic needs was defined as participants’ possibility to obtain adequate food, clean water, clothes and shelter.
Thirty-six homeless children, all abandoned at the age of 4, constituted the Maltreated Group (Mal, Appendix S1, Table S1). Familial abandonment at the age of 4 is notably prevalent, particularly within the most impoverished communities, as children at this age start to exhibit significant albeit rudimentary autonomy. Hence, our experimental sample comprises individuals hailing from backgrounds marked by specific adversity and impoverishment, with their circumstances exacerbated at the age of 4 due to complete abandonment by their primary household.
All Mal participants were recruited among Kroo Bay population. The last settlement profile report dates back to 2015 (Slum Dwellers International, https://sdinet.org/) and to date there are no official government reports. Kroo Bay, situated along the coastline is an informal housing settlement characterized by overcrowded and informal housing, often constructed from makeshift materials. Basic amenities such as clean water, sewerage service and electricity are missing. The community has only one health facility and four traditional pit latrines. There is no recycling and reuse of waste in the community and waste separation is not practiced in the entire settlement. Malnutrition and infectious diseases are prevalent and environmental hazards, such as flooding and wildfires, are very common.
In this adverse context, Mal participants have experienced conditions of both severe deprivation and threat. They have faced extraordinary circumstances of neglect and poverty, periods of institutionalization or detention, and the absence of an attachment figure. Concurrently, they have encountered multiple episodes of threat, with all participants being subjected to physical and emotional abuses, and in some cases even documenting instances of sexual assault.
To compare the affective and social development occurring in CM condition with a typical pattern of development, 37 healthy participants who continuously lived with parents or close relatives from the age of 4 until the time of the study formed the Control Group (Con). All Con participants were recruited among families residing in Lakka and followed by the Ravera Children Rehabilitation Centre. Lakka is a coastal village around the peninsular in the Western Area Rural District of Sierra Leone. The Centre aids families and children by offering social, educative, and health safeguarding services. Consequently, the Control Group comprises young individuals from the same cultural background as the Maltreated Group, but who have not undergone severe experiences of deprivation and threat. None of the participants in the Control Group experienced incidents of physical, sexual, or emotional abuse.
Procedure and measures
Because of the absence of an ethics committee covering studies conducted in Sierra Leone at the time of the study, the present experimental protocol was approved by an ad-hoc local ethical committee composed of three health professionals (one physician and two nurses), one religious member, three social workers, and one anthropologist. None of the member has any formal or informal conflict of interest with the evaluated study and the researchers. Then, the ethical evaluation of the committee was transmitted to the Ministry of Health and Sanitation of the Republic of Sierra Leone. The protocol was in line with the Declaration of Helsinki (Holm, Reference Holm2013).
The study took place in the morning, 2 hours after participants’ food intake, at the presence of a local social worker. After arrival at the experimental location, participants responded to the systematic interview.
Maltreatment measures
Participants’ maltreatment history was derived from sanitary and forensic reports. We preferred to rely on official records because of both the absence of validated scales on the population under study and the presence of very detailed records. Both groups, in fact, are followed by local institutions and have medical and legal records. From these reports, two main variables were extracted: maltreatment duration and maltreatment severity.
Maltreatment duration
Maltreatment duration was computed as the number of consecutive years each child had spent as homeless child without a consistent primary caregiver from the age of 4. For the Con group, the years of typical development were then computed as the number of consecutive years each child had spent with his family from the age of 4. Kolmogorov–Smirnov test for independent samples revealed that maltreatment duration and years of typical development have the same distribution (p = .973).
Maltreatment severity
Maltreatment severity was calculated as the mean severity scores obtained at Kaufman scale at Physical Abuse rating scale, Neglect rating scale and Emotional Maltreatment rating scale (Kaufman et al., Reference Kaufman, Jones, Stieglitz, Vitulano and Mannarino1994). The Kaufman Scale was selected because it enables an evaluation of maltreatment severity based on official descriptions, such as those within our possession, without necessitating victim’s self-assessment or witnesses’ report. The scale characterizes each category of abuse using a few indices and descriptions and each category is rated from 0 to 4. In the face of exceptionally harsh and extreme circumstances, accurately gauging the severity of the deprivation and threat CM components becomes challenging. Consequently, an index of overall CM severity was obtained as the mean severity scores. Considering the absence of maltreatment incidents verified by health or legal documents as the criterion for inclusion of control participants, the severity index was calculated only for the Maltreated group.
Affective and social development measures
Affective and social development was measured though both behavioral and physiological measures recorded in response to dynamic facial expressions (Ardizzi et al., Reference Ardizzi, Martini, Umiltà, Sestito, Ravera and Gallese2013, Reference Ardizzi, Martini, Umiltà, Evangelista, Ravera and Gallese2015, Reference Ardizzi, Umiltà, Evangelista, Di Liscia, Ravera and Gallese2016, Reference Ardizzi, Evangelista, Ferroni, Umiltà, Ravera and Gallese2017). Stimuli were 64 video-morphing depicting the transition from a neutral facial expression to an emotional one (i.e., anger, fear, joy, or sadness). Each stimulus lasted 3 sec (15 fps; 800x560 pixels). Stimuli were presented using E-Prime 2.0 software (Psychology Software Tools, Inc.).
Behavioral measure: anger false alarms rate
Anger false alarms (Afa) rate were calculated as a ratio of participants’ incorrect use of anger label to the total number of erroneous facial expression identifications at a forced-choice facial expressions identification task. Afa rates were subjected to variance-stabilizing procedure for a binomial proportion through arcsin-square-root transformation.
During a forced-choice facial expressions identification task (Figure 1, panel a), participants had to verbally identify, with no time limit, which of the four alternative labels (i.e., anger, fear, joy, and sadness) best described the emotional content of the facial expression just shown. The four alternative labels, written in English and in participants’ primary language, were always visible. Stimulus presentation was preceded by the question “you able du am?” (“Are you ready?”) on the monitor. After participant’s affirmative answer, the experimenter pressed the spacebar to show the following stimulus. Stimuli were presented once (64 trials) in a random order. The forced-choice facial expressions identification task lasted approximately 15 minutes, depending on participants’ response time.
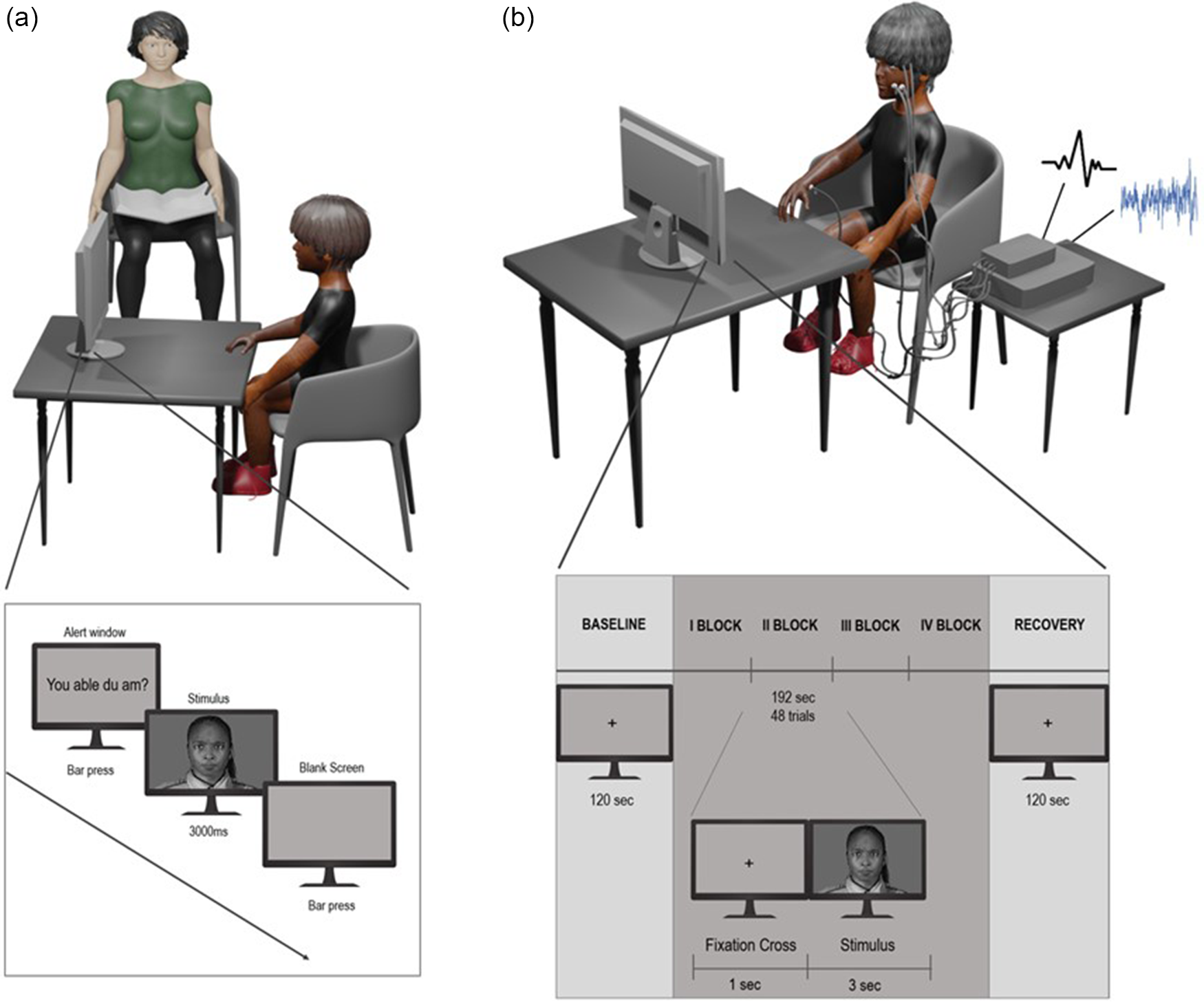
Figure 1. Experimental settings and protocols of behavioral (panel a) and physiological (panel b) tasks.
Physiological measures: autonomic regulation of the heart and facial mimicry
Physiological measures were recorded at rest (i.e., baseline) and in response to emotional stimulations (Figure 1, panel b). During baseline, lasting 120 sec, participants were asked to relax and observe a fixation cross displayed on a screen. Facial expressions were then showed in a randomized block design. During each block (i.e., anger, fear, joy, and sadness blocks), lasting 192 sec, stimuli belonging to the same emotion (48 trials) were displayed in a random order preceded by a fixation cross lasting 1 s. For the entire duration of each facial expression block, participants were instructed to carefully observe the stimuli. Between blocks, a minimum of 2-minute interval was waited to avoid potential physiological cross-over between conditions. To maintain participants’ attention, at the end of each block a question about the videos just shown was asked. Participants’ faces were video recorded to ensure that they looked at the monitor during stimuli presentation. Overall, the procedure lasted approximately 22.8 min basing on the between-block intervals.
Physiological measurements were converted and amplified with an eight-channel amplifier (PowerLab8/30; ADInstruments UK) and displayed, stored, and reduced with LabChart 7.3.1 software package.
Heart rate variability (HRV), a measure of the variability in intervals between subsequent heart beats, is widely considered an index of emotion regulatory capacity and the ability to adapt flexibly to changing environmental demands (Heiss et al., Reference Heiss, Vaschillo, Vaschillo, Timko and Hormes2021). HRV is widely thought to reflect current activity of sympathetic and parasympathetic nervous systems as well the balance between them (Pham et al., Reference Pham, Lau, Chen and Makowski2021). HRV power spectrum can be meaningfully divided into different frequency bands. Broadly speaking, High Frequency (HF-HRV; 0.15–0.4 Hz) component is established as an index of the parasympathetic modulation of the heart and under controlled conditions, its derivative, the respiratory sinus arrhythmia (RSA) as an estimator of the vagal regulation of the heart. Differently, Low Frequency (LF-HRV; 0.04–0.15 Hz) component dominantly represents the sympathetic modulation of the heart. However, we must emphasize that the absence of a vagal influence on LF is not completely excluded (Thomas et al., Reference Thomas, Claassen, Becker and Viljoen2019). In the present study, the RSA and the LF components of the HRV were used to estimate the parasympathetic and the putative sympathetic regulation of the heart, respectively.
Participants’ electrocardiogram (ECG) was recorded using three 10 mm Ag/AgCl pre-gelled electrodes (ADInstruments, UK) placed in an Einthoven’s triangle configuration. The ECG was sampled at 1 kHz and filtered with an online Main Filter (adaptive 50 Hz filter). ECG R-wave peaks were detected from each sequential heartbeat. R-R intervals (lasting 120 sec for baseline and 192 sec for each facial expression block) were then extracted and, when necessary, edited for artifacts manually or by integer division or summation procedures (Berntson et al., Reference Berntson, Bigger, Eckberg, Grossman, Kaufmann, Malik, Nagaraja, Porges, Saul, Stone and van der Molen1997; Kaltwasser et al., Reference Kaltwasser, Rost, Ardizzi, Calbi, Settembrino, Fingerhut, Pauen, Gallese and Avenanti2019). Recordings with more than 30% of edited beats were excluded from analyses. CardioBatch+ software (Brain-Body Center for Psychophysiology and Bioengineering, University of North Carolina at Chapel Hill, 2016) was used to calculate RSA and LF-HRV from the ECG data using age-specific parameters that are sensitive to the shifts in the frequency of spontaneous breathing (Porges & Bohrer, Reference Porges, Bohrer, Cacioppo and Tassinary1990; Porges, Reference Porges1985). RSA and LF-HRV were computed detrending the time-based heartbeat series with a 21-point cubic moving polynomial stepped through the data to create a smoothed template, then subtracting the template from the original time-based series to generate a detrended residual series. The detrended time series was filtered to extract the variance in the heart period pattern associated with RSA or LF-HRV. Lastly, RSA values were transformed to their natural logarithmic values to address the distributional requirements for parametric analyses. These procedures (Lewis et al., Reference Lewis, Furman, McCool and Porges2012; Porges, Reference Porges1985) are statistically equivalent to frequency domain methods (i.e., spectral analyses) for the calculation of the amplitude of RSA and LF-HRV when heart period data are stationary.
RSA and LF-HRV were measured during baseline and facial expressions blocks. In both cases, heart metrices were calculated for 4 sequential 30-sec epochs and then averaged. RSA and LF-HRV values in response to facial expressions of emotions were measured as the change scores from the baseline values.
The ‘simulation theory’ posited that when individuals observe emotional expressions in others, it triggers an automatic inner simulation with them. This process manifests behaviorally as the automatic tendency to respond to emotional expressions with unobservable or mild facial changes, the so-called facial mimicry (Goldman & Sripada, Reference Goldman and Sripada2005; Dimberg, Reference Dimberg1982; Hess & Fischer, Reference Hess and Fischer2013).
Research suggests that facial mimicry supports a proficient recognition of facial expressions and empathy, underscoring the importance of this mechanism in social cognition (Borgomaneri et al., Reference Borgomaneri, Bolloni, Sessa and Avenanti2020; De Stefani et al., Reference De Stefani, Ardizzi, Nicolini, Belluardo, Barbot, Bertolini, Garofalo, Bianchi, Coudé, Murray and Ferrari2019; Japee et al., Reference Japee, Jordan, Licht, Lokey, Chen, Snow, Jabs, Webb, Engle, Manoli, Baker and Ungerleider2023; Oberman et al., Reference Oberman, Winkielman and Ramachandran2007; but see also Holland et al., Reference Holland, O’Connell and Dziobek2021).
In the present study, facial mimicry was acquired by facial electromyography (EMG).
Facial EMG was measured by means of 4 mm Ag/Ag-Cl electrodes bipolarly placed, following standard procedures, on the left side of participants’ face over Corrugator Supercilii and Zygomaticus Major muscular regions (Fridlund & Cacioppo, Reference Fridlund and Cacioppo1986). Facial EMG was sampled at 2 kHz and recorded with an online Main Filter (adaptive 50 Hz filter). A 20–500 Hz bandpass filter was applied offline on the raw EMG signal. EMG signal was screened for artifacts by 2 blind coders who firstly removed trials with artifacts due to electrical noise (less than 3.2% of removed trials), and subsequently, inspected participants’ face videos to remove trials affected by motion artifacts. Participants with more than 30% of discarded trials were excluded from analyses. The amplitude of the EMG signal was obtained, independently for the two muscles, via root-mean-square method applied on epochs of 0.5 sec then averaged (1 pre-stimulus onset epoch, and 6 post-stimulus onset epochs). Mean EMG responses (expressed in microvolts, µV) of the 2 muscles during the visualization of angry, fear, joy, and sadness facial expressions were obtained as mean change score between pre-stimulus epoch and post-stimulus epochs.
Data analyses
Multiple regression models including Group (i.e., Mal and Con) and Duration (i.e., maltreatment duration/years of typical development) as predictors were conducted separately for baseline RSA, baseline LF-HRV, and Afa values. Three different regression models were tested to find the most fitting impact trajectory describing the relation between Duration and participants’ baseline autonomic parameters and explicit recognition bias. Among the models showing a significant Group*Duration interaction (p < 0.05), the one with the lowest Akaike Information Criterion (AIC) value was selected as best representative. The significant interaction was then assessed running univariate tests.
Then, multivariate multiple regressions were conducted separately for Corrugator EMG activity, Zygomaticus EMG activity, RSA, and LF-HRV including Group (i.e., Mal and Con) and Duration as predictors, and Emotion (i.e., Anger, Fear, Joy, and Sadness) as multivariate dependent measure. Also in this case, three different regression models were tested to find the most fitting impact trajectory describing the relation between Duration and participants’ physiological responses to facial expressions of emotions. Among the models showing a significant Group*Duration interaction (p < 0.05), of interest for our purposes, the one with the lowest Wilks’ lambda value (Λ) was selected as best representative. The significant interaction was then assessed running univariate tests.
To control for potential effects of other factors interacting with CM duration, control analyses were conducted considering the number of maltreatment episodes and maltreatment severity. These analyses are reported extensively in Appendix S2 and Table S2. Raw RSA and LF-HRV data organized by age and by group are shown in the Appendix S3, Table S3.
Results
Baseline RSA
The model selected as best representative based on the established statistical criteria was the quadratic one (AIC = 228.30). The quadratic multiple regression showed a significant Group*Duration interaction (F (2,67) = 3.9, p = 0.003). Post-hoc univariate quadratic regression models conducted independently for the 2 groups showed a significant effect of Duration for Mal group (F (2,33) = 6.45, p = 0.001, R 2 = 0.28, R 2 adj = 0.24; β = −4.28) and not for Con group (p = 0.11) (Figure 2, panel a).
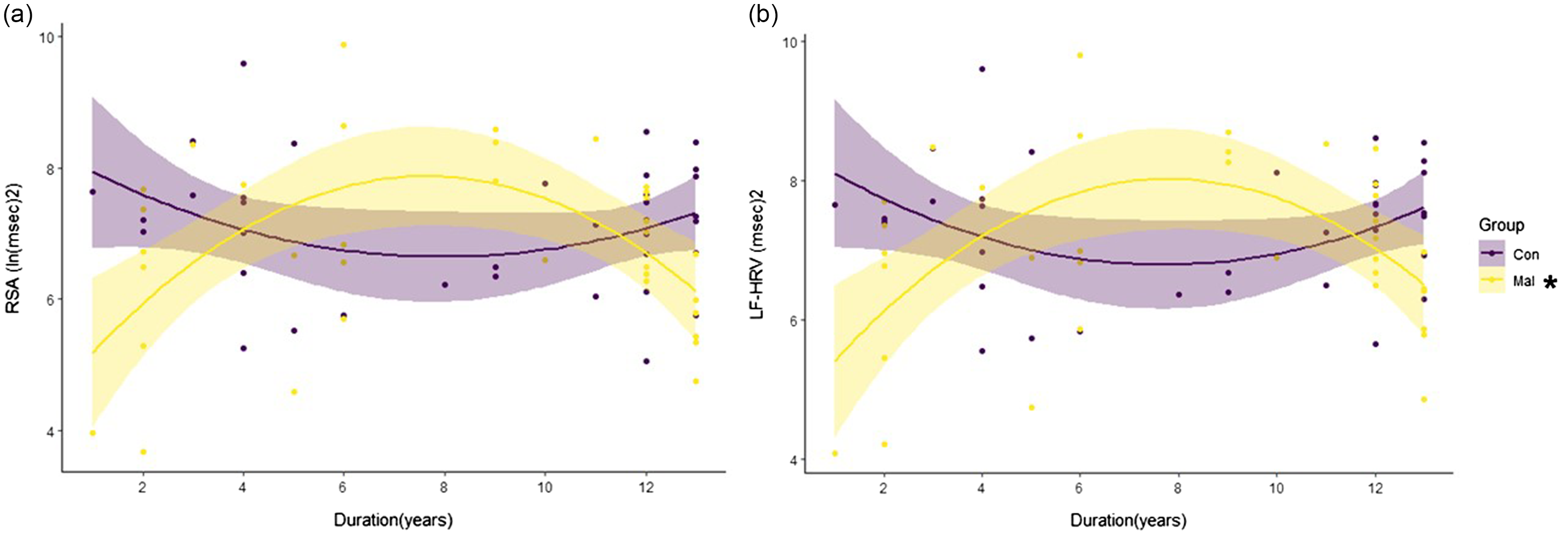
Figure 2. Effect of duration (Childhood maltreatment duration/years of typical development) displayed for maltreated (Mal) and control (Con) groups on respiratory sinus arrhythmia (RSA, panel a) and low frequency heart rate variability (LF-HRV, panel b) recorded at baseline * = p < 0.05.
Baseline LF-HRV
The model selected as best representative based on the established statistical criteria was again the quadratic one (AIC = 220.32). The quadratic multiple regression showed a significant Group*Duration interaction (F (2,67) = 7.68, p = 0.001). Post-hoc univariate quadratic regression models conducted independently for the 2 groups showed a significant effect of Duration for Mal group (F (2,33) = 6.18, p = 0.005, R 2 = 0.27, R 2 adj = 0.22; β = −3.96) and not for Con group (p = 0.17) (Figure 2, panel b).
Anger false alarms rate
The model selected as best representative based on the established statistical criteria was the quadratic one (AIC = 530.82) but it did not show a significant Group*Duration interaction (p = 0.11).
Corrugator EMG activity
The model selected as best representative based on the established statistical criteria was the linear one (Λ = 0.77) which showed a significant Group*Duration interaction (F (4,50) = 3.70, p = 0.01).
Univariate linear multiple regression model conducted for the Corrugator EMG activity in response to angry facial expressions was significant (F (3,58) = 11.54, p < 0.001; multiple R 2 = 0.37; multiple R 2 adj = 0.34) and revealed a significant Group* Duration interaction (p = 0.049). Post-hoc univariate linear regression models conducted independently for the 2 groups showed a significant effect of Time for Mal group (F (1,30) = 9.19, p = 0.005, R 2 = 0.23, R 2 adj = 0.21; β = −0.06) and not for Con group (p = 0.97) (Figure 3, panel a).
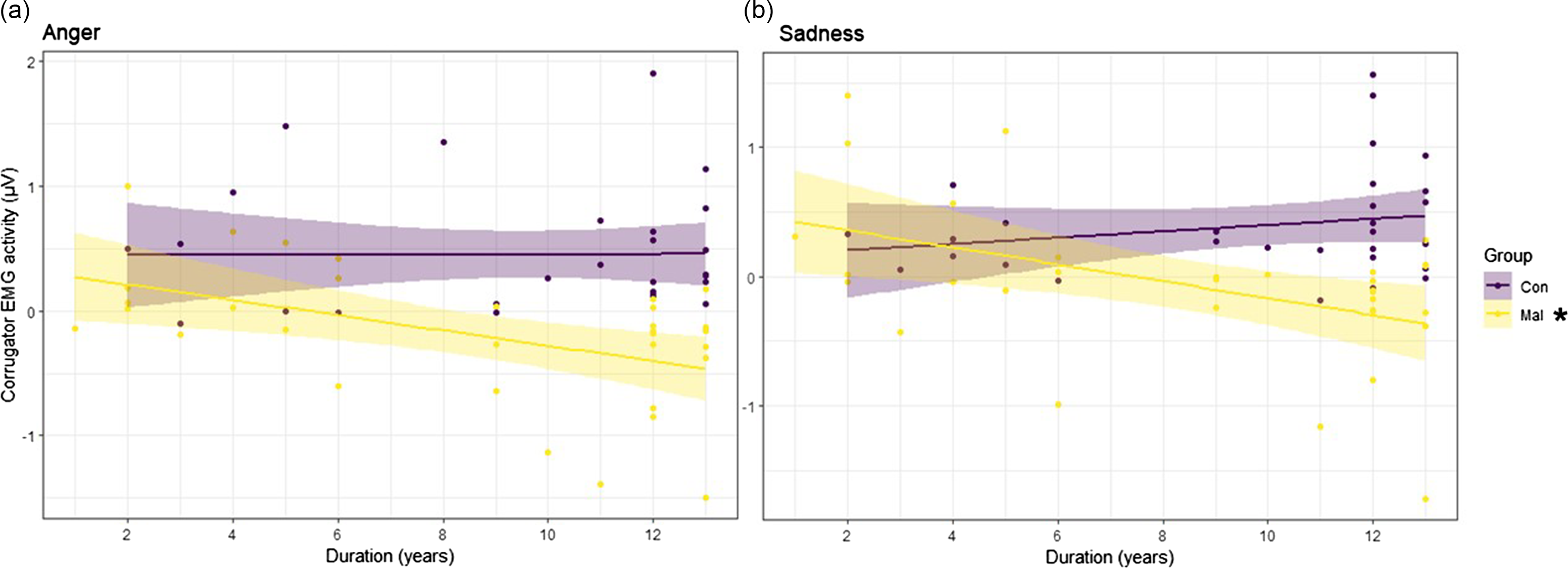
Figure 3. Effect of duration (Childhood maltreatment duration/years of typical development) displayed for maltreated (Mal) and control (Con) groups on corrugator EMG activity in response to angry (panel a) and sad (panel b) facial expressions. * = p < 0.05.
Univariate linear multiple regression model conducted for the Corrugator EMG activity in response to fearful facial expressions was significant (F (3,60) = 14.61, p < 0.001; multiple R 2 = 0.42; multiple R 2 adj = 0.39) but revealed a non-significant Group* Duration interaction (p = 0.14).
Univariate linear multiple regression model conducted for the Corrugator EMG activity in response to joyful facial expressions was not significant (p = 0.16).
Univariate linear multiple regression model conducted for the Corrugator EMG activity in response to sadness facial expressions was significant (F (3,58) = 8.35, p < 0.001; multiple R 2 = 0.30; multiple R 2 adj = 0.26) and revealed a significant Group* Duration interaction (p = 0.006). Post-hoc univariate linear regression models conducted independently for the 2 groups showed a significant effect of Duration for Mal group (F (1,30) = 8.28, p = 0.007, R 2 = 0.22, R 2 adj = 0.19; β = −0.06) and not for Con group (p = 0.25) (Figure 3, panel b).
Zygomaticus EMG activity
The model selected as best representative based on the established statistical criteria was the linear one (Λ = 0.78) but it did not show a significant Group* Duration interaction (p = 0.71).
RSA response
The model selected as best representative based on the established statistical criteria was the linear one (Λ = 0.81) which showed a significant Group* Duration interaction (F (4,50) = 2.84, p = 0.03).
Univariate linear multiple regression model conducted for the RSA response to angry facial expressions was significant (F (3,58) = 4.23, p = 0.007; multiple R 2 = 0.19; multiple R 2 adj = 0.14) and revealed a significant Group* Duration interaction (p < 0.001). Post-hoc univariate linear regression models conducted independently for the 2 groups showed a significant effect of Duration both for Mal group (F (1,29) = 7.56, p = 0.01, R 2 = 0.21, R 2 adj = 0.18; β = −0.06) and Con group (F (1,28) = 5.30; p = 0.03; R 2 = 0.15, R 2 adj = 0.12; β = 0.04) (Figure 4, panel a).
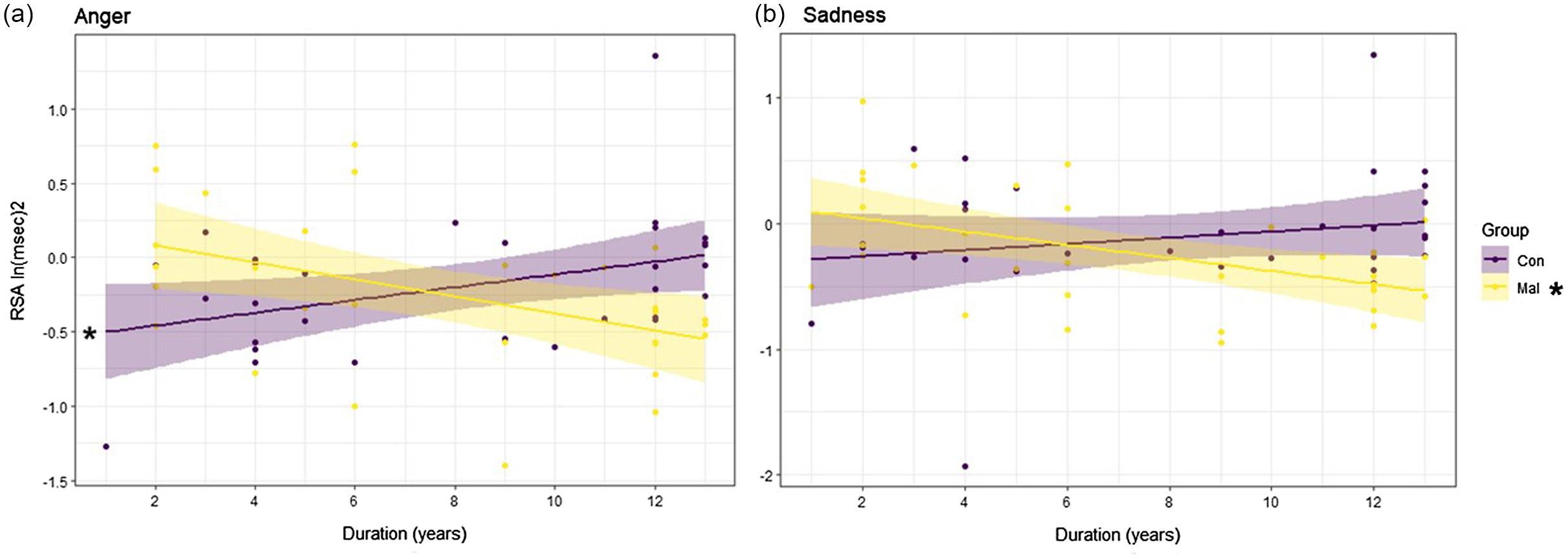
Figure 4. Effect of duration (Childhood maltreatment duration/years of typical development) displayed for maltreated (Mal) and control (Con) groups on respiratory sinus arrhythmia (RSA) in response to angry (panel a) and sad (panel b) facial expressions. * = p < 0.05.
Univariate linear multiple regression model conducted for the RSA response to fearful facial expressions was not significant (p = 0.28) nor was the one conducted for the RSA response to joyful facial expressions (p = 0.74).
Univariate linear multiple regression model conducted for the RSA response to sadness facial expressions was significant (F (3,61) = 3.29, p = 0.03; multiple R 2 = 0.14; multiple R 2 adj = 0.09) and revealed a significant Group* Duration interaction (p = 0.007). Post-hoc univariate linear regression models conducted independently for the 2 groups showed a significant effect of Duration for Mal group (F (1,30) = 8.92, p = 0.005, R 2 = 0.23, R 2 adj = 0.20; β = −0.05) and not for Con group (p = 0.26) (Figure 4, panel b).
LF-HRV response
The model selected as best representative based on the established statistical criteria was the linear one (Λ = 0.68) but it did not show a significant Group* Duration interaction (p = 0.83).
Discussion
To date there is a broad consensus regarding the severe cognitive, emotional, and behavioral deficits following maltreatment exposure during childhood (Jaffee & Maikovich-Fong, Reference Jaffee and Maikovich-Fong2011). CM has been, indeed, consistently linked to alterations in social cognition, competence which in turn serves as a buffer against the negative consequences of maltreatment (Pfaltz et al., Reference Pfaltz, Halligan, Haim-Nachum, Sopp, Åhs, Bachem, Bartoli, Belete, Belete, Berzengi, Dukes, Essadek, Iqbal, Jobson, Langevin, Levy-Gigi, Lüönd, Martin-Soelch, Michael, Oe, Olff, Ceylan, Raghavan, Ramakrishnan, Sar, Spies, Wadji, Wamser-Nanney, Fares-Otero, Schnyder and Seedat2022). Worsening this picture, epidemiological data reveals that maltreatment is an extremely common condition: worldwide 1 in 4 adults has been abused as child (WHO, 2017). In non-WEIRD countries (Western, Educated, Industrialized, Rich, and Developed), the percentages of boys experiencing maltreatment prior to age 18 consistently exceed the 50% (e.g., Tanzania: 53%; Zimbawe: 76%; Haiti: 57%; ©WHO, 2017). The current study contributes to the ongoing research agenda in the field by exploring the impact trajectories of maltreatment duration on the development of social cognition.
We focused on specific behavioral (anger false alarm rate) and physiological (facial mimicry and autonomic regulation of the heart) markers of affective and social development already found altered in child populations exposed to maltreatment, and we tested the influence of maltreatment duration along three different impact trajectories (i.e., linear, logarithmic, and quadratic).
The initial conclusion to be drawn from the present results is that the duration of maltreatment exerts varying effects on both behavioral and physiological markers of social cognition development.
While at the physiological level maltreatment duration had a severe influence, the opposite was evident for the behavioral measure. Indeed, Afa rate was not influenced by maltreatment duration. This result is coherent with other studies demonstrating the presence of this biased emotional identification even after a single acute traumatic episode (Bick & Nelson, Reference Bick and Nelson2017; Nelson et al., Reference Nelson, Westerlund, McDermott, Zeanah and Fox2013; Scrimin et al., Reference Scrimin, Moscardino, Capello, Altoè, Steinberg and Pynoos2011; Troller-Renfree et al., Reference Troller-Renfree, McDermott, Nelson, Zeanah and Fox2015). This bias is apparently not restricted to a deficit in selective attention but may instead reflect a broader bias pattern whereby anger and hostility are perceived in ambiguous and even unambiguous non-hostile expressions (Mellentin et al., Reference Mellentin, Dervisevic, Stenager, Pilegaard and Kirk2015). The behavioral adaptation to maltreatment occurs as an “all-or-nothing” phenomenon shifting and biasing victims’ facial expression recognition independently from maltreatment duration. The observation of this behavioral adaptation across various forms of abuse, diverse age groups, and both chronic and acute instances suggests it as a broad, swift, and non-specific adaptation strategy (Bérubé et al., Reference Bérubé, Turgeon, Blais and Fiset2023).
Seeing threat in others’ faces could be yet a cognitive pathway that mediates reactive, oppositive, and instrumental aggression in victims of maltreatment. The phenomenon resilience to variations in maltreatment characteristics and its early onset highlight its significance for the affective and social development of the victims.
The second conclusion to be drawn pertains to the differential impact of maltreatment duration on sympathetic and parasympathetic regulation of the heart. Specifically, in this study, both components are influenced by the duration of maltreatment when assessed at rest (i.e., baseline). They indicate an increasing physiological compensation of both sympathetic and parasympathetic branches of the autonomous nervous system (first 6 years of exposure) that begins to decrease over time, turning into a progressive autonomic withdrawal. This pattern of adaptation is coherent with the “sleeper effect” (Maurer et al., Reference Maurer, Mondloch and Lewis2007) detected both for behavioral and anatomo-functional sequelae of chronic maltreatment (Hanson et al., Reference Hanson, Chung, Avants, Shirtcliff, Gee, Davidson and Pollak2010; Zeanah et al., Reference Zeanah, Gunnar, McCall, Kreppner and Fox2011). Our data highlight a long-term pattern of adaptation to maltreatment resulting in opposing outcomes basing on maltreatment duration (e.g, hyper- and hypo-arousal) and support the necessity to explore different impact trajectory after CM exposure. It’s not unexpected that these 2 autonomic components exhibit similar modulation patterns. LF- and HF-HRV share indeed functional components that are pertinent to our study (Thomas et al., Reference Thomas, Claassen, Becker and Viljoen2019). In contrast, the sympathetic and parasympathetic regulation of the heart demonstrate divergent responses to emotional expressions, with only the parasympathetic component being affected by the maltreatment duration. Specifically, while Con showed the anticipated linear maturational adjustment toward a coherent vagal recruitment in response to threatening facial expressions (see also Dollar et al., Reference Dollar, Calkins, Berry, Perry, Keane, Shanahan and Wideman2020), the Mal group evidenced a linear increase in the suppression of the vagal brake toward anger and sadness. An exaggerated and progressive vagal suppression in response to angry facial expression may lock victims in a physiological state supporting defensive strategies and reactions (Porges, Reference Porges2021). Similarly, too low or too high autonomic responses to others’ negative emotions could be maladaptive because it underlies a lack of empathetic reaction or a highly distressed response (Truzzi & Ripoli, Reference Truzzi and Ripoli2019).
The spontaneous facial EMG responses mimic the autonomic ones. A progressive linear decrement of facial mimicry in response to anger and sadness was indeed found among maltreated youths and not among controls. Being facial mimicry a spontaneous physiological response supporting empathic access to others’ emotions (Drimalla et al., Reference Drimalla, Landwehr, Hess and Dziobek2019), maltreatment appears to affect more and more negatively victims’ implicit empathic ability, jeopardizing their possibility to automatically and bodily simulate others’ affective states (Gallese, Reference Gallese2003, Reference Gallese2007, Reference Gallese2014; Niedenthal, Reference Niedenthal2007; Uddin et al., Reference Uddin, Kaplan, Molnar-Szakacs, Zaidel and Iacoboni2005). We posit that the reduced facial mimicry in response to negative emotions of others works as a protective mechanism useful to better adapt to and survive in a highly hostile and competitive social environment (Seibt et al., Reference Seibt, Mühlberger, Likowski and Weyers2015) where empathically engaging with other people’s anger or sadness would turn out not to be emotionally feasible.
Another observation arising from this study is the specific effect of maltreatment duration on the physiological responses to angry and sad facial expressions and not to happy and fearful ones. This result does not imply that exposure to maltreatment fails to modify physiological reactions to the latter two emotions, a conclusion previously shown by Ardizzi et al., (Reference Ardizzi, Martini, Umiltà, Sestito, Ravera and Gallese2013, Reference Ardizzi, Martini, Umiltà, Evangelista, Ravera and Gallese2015). Rather, it suggests that the duration of maltreatment does not significantly affect RSA and facial mimicry adaptations in response to happy and fearful faces. Although CM has been seen to affect responses to both positive and negative emotions, some studies have shown specific alterations in the processing of anger and sadness. For example, Bodenschatz et al. (Reference Bodenschatz, Skopinceva, Ruß and Suslow2019) demonstrated that CM was associated with reduced attention for angry and sad facial expressions in the depressed sample. The authors argued considering CM as a potential factor able to decrease attendance to social stimuli asking for substantial empathic engagement and emotion regulation strategies. Whereas encountering other people expressing joy or fear might trigger swift adaptive reactions (i.e., engaging or fly, respectively), managing the anger or sadness of others necessitates enhanced self-regulation abilities, especially in adverse and competitive contexts. Though preliminary, our findings may support this interpretation, highlighting how prolonged maltreatment duration correlates with deteriorating empathic responses and self-regulation, especially in response to emotions that demand heightened engagement.
The last conclusion that could be drawn from the present study is about the impact trajectory followed by CM duration on victims’ affective and social development. It would seem that CM may influence social development along similar trajectories regardless of the physiological variable of interest. In the present study, indeed, both vagal and electromyographic responses linearly correlate with increased duration of maltreatment. However, the effect differs when considering these parameters in a context where social stimuli are present or not. Again, in the present study, heart rate autonomic regulation follows a linear trend when measured in response to emotions and a quadratic trajectory when measured at rest. This result suggests the importance of considering different impact trajectories and also confirms the progressively additive effect of each year of CM exposure on physiological markers of social and affective development (Dunn et al., Reference Dunn, Soare, Raffeld, Busso, Crawford, Davis, Fisher, Slopen, Smith, Tiemeier and Susser2018).
Conclusion
Taken together, the present evidence demonstrates that CM penetrates under victims’ skin (Holochwost et al., Reference Holochwost, Wang, Kolacz, Mills-Koonce, Klika and Jaffee2021; Lupien et al., Reference Lupien, King, Meaney and McEwen2001) to become physiologically embedded (Berens et al., Reference Berens, Jensen and Nelson2017), preventing them the possibility to automatically resonate with other individuals and effectively self-regulate in social contexts. This failure can promote the development of antisocial behaviors, self-concept disturbances and ineffective coping strategies, delineating a maladaptive profile coherent with the one described in the complex-PTSD nosographic category. The trajectories here outlined allow a deeper comprehension of the developmental pathways through which early life adversities place youths on a track of lifelong health disparities (Kuhlman et al., Reference Kuhlman, Horn, Chiang and Bower2020), providing some relevant suggestions. First, the progressive damage to the physiological markers of affective and social development indicates that, for victims of CM, a somatically oriented therapy should be favored. Second, the presence of compensatory autonomic recruitment during the first years of CM exposure suggests that interventions targeting this time window may be the most impactful in shifting negative developmental cascades (Koss, Reference Koss2019). Third, considering both the peculiarity and the CM trajectory, attention should be paid to the existence of this precedent background in clinical population groups through ad-hoc anamneses. Focusing on a non-WEIRD (western, educated, industrialized, rich, and democratic) country and on a sample of youths exposed to severe form of CM, the present study contributes to the generalizability of research results and of the above-mentioned considerations.
It is however critical to make explicit some limitations of the study. Although we have enrolled a homogeneous group of homeless kids, it is almost impossible to surgically isolate CM duration from other influencing factors. For this reason, it was impossible to independently test the effect of CM severity and CM duration, as well as the effect of deprivation and threat. Staying within the framework of the last mentioned dichotomy, our data may suggest that CM duration influences the impairments typically associated with deprivation (i.e., poor empathic engagement due to lack of social stimulation, here measured by the reduction of EMG responses) and threat (i.e., hyper-reactivity to non-threatening stimuli, here measured by vagal suppression) in a similar way (i.e., linear trajectory). Further investigation into these dimensions is still necessary, particularly in samples experiencing less severe forms of maltreatment and for which validated scales are available.
Furthermore, other relevant moderators, such as individual psychobiological vulnerability, could not be measured mainly due to the absence of validated assessment instruments for this experimental population. Thus, potential interactive effects of CM duration with other moderators are not considered in the present study. Lastly, it is noteworthy to consider that we had the opportunity to focus only on male participants.
In conclusion, the present study identifies the specific impact trajectory that CM duration exerts on the psychophysiological mechanisms involved in empathic recognition of others’ emotions and self-regulation in social context. Nevertheless, much remains to be learnt about the complex mechanisms through which adversity becomes biologically embedded in children’s mind and body and on how these mechanisms vary across their development. Considering the inherently social nature of human beings and the pervasive long-lasting mental and physical health disruptions brought by CM, the present findings highlight the urgency of promptly taking charge of this enduring, silent and, so far, too neglected epidemic (Kaffman, Reference Kaffman2009).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579424001214.
Acknowledgments
The authors would like to acknowledge all the members and the staff of FHM Sierra Leone, FHM Italia and R.C.R.C. whose help was essential for the realization of this study. The authors would also like to thank the directors and the staff of Approved School Correctional Centre, Remand Home Correctional Centre and Holy Family School. The biggest thanks go to the youngsters who agreed to participate in the research giving their time and telling us their stories.
Funding statement
None.
Competing interests
None.








 Open access
Open access