


Introduction
Decades of research have established the enduring effects of childhood experiences on adaptation and maladaptation across the lifespan (Cicchetti & Toth, Reference Cicchetti and Toth2009; Masten, Reference Masten2006; Sroufe, Reference Sroufe1979). Childhood adversity, including abuse, neglect, and exposure to family dysfunction, often measured using the Adverse Childhood Experiences (ACEs) questionnaire and hereafter referred to as “ACEs),” is associated with adulthood mental and physical health problems, such as higher levels of depression, anxiety, and post-traumatic stress disorder (PTSD) symptoms, and greater risk for cardio-metabolic problems, obesity, and earlier morbidity (Anda et al., Reference Anda, Whitfield, Felitti, Chapman, Edwards, Dube and Williamson2002; Brockie et. al, Reference Brockie, Dana-Sacco, Wallen, Wilcox and Campbell2015; CDC, 2020; Chapman et al., Reference Chapman, Whitfield, Felitti, Dube, Edwards and Anda2004; Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998; Widom, Reference Widom1999; Yehuda et al., Reference Yehuda, Spertus, Golier and Eth2001). These childhood adversities are also associated with romantic relationship difficulties during adulthood and parenting problems in the next generation (Belsky et al., Reference Belsky, Conger and Capaldi2009; Labella et al., Reference Labella, Raby, Martin and Roisman2019; Narayan et al., 2013, 2014).
A separate but accumulating body of research has considered the role of positive or benevolent childhood experiences (BCEs) on more favorable outcomes into adulthood (Han et al., Reference Han, Dieujuste, Doom and Narayan2023). BCEs include safe and supportive childhood relationships with caregivers and other social counterparts and a positive and predictable quality of life (Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018). Higher levels of these positive childhood experiences do not necessarily reflect the absence of ACEs, nor do higher levels of ACEs simply signal the absence of positive childhood experiences (Karatzias et al., Reference Karatzias, Shevlin, Fyvie, Grandison, Garozi, Latham, Sinclair, Ho, McAnee, Ford and Hyland2020; Narayan et al., Reference Narayan, Lieberman and Masten2021). In fact, previous research has indicated that ACEs and BCEs are only moderately inversely correlated and often co-occur, with many individuals experiencing high levels of both (Han et al., Reference Han, Dieujuste, Doom and Narayan2023; Merrick et al., Reference Merrick, Narayan, DePasquale and Masten2019; Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018). Reflecting promotive factors, BCEs are often directly associated with more desirable outcomes, including lower levels of adulthood mental health problems, such as lower depression and PTSD symptoms (e.g., Bellis et al., Reference Bellis, Hardcastle, Ford, Hughes, Ashton, Quigg and Butler2017; Bethell et al., Reference Bethell, Jones, Gombojav, Linkenbach and Sege2019; Crandall et al., Reference Crandall, Miller, Cheung, Novilla, Glade, Novilla, Magnusson, Leavitt, Barnes and Hanson2019; Merrick & Narayan, Reference Merrick and Narayan2020). Higher levels of positive childhood experiences are also associated with adults’ higher ratings of social and emotional health, healthy lifestyles, and resources within their families, broadly defined, as well as higher levels of social support and more nurturing parenting attitudes (Daines et al., Reference Daines, Hansen, Novilla and Crandall2021; Morris et al., Reference Morris, Hays-Grudo, Zapata, Treat and Kerr2021). Despite an accumulating body of research on the promotive effects of positive childhood experiences, and especially BCEs, on multiple long-term outcomes (Han et al., Reference Han, Dieujuste, Doom and Narayan2023), few studies have examined whether the favorable effects of BCEs extend into the next generation.
Adverse versus benevolent childhood experiences and perinatal mental health problems
The perinatal period is a particularly salient time when pregnant individuals’ wellbeing may echo the quality of experiences and resources present during childhood. As individuals experience the multitude of changes that occur during pregnancy, they are also increasingly likely to reflect on their own childhood experiences as they anticipate giving a new baby the best possible life (Lieberman et al., Reference Lieberman, Diaz and Van Horn2009; Narayan et al., Reference Narayan, Oliver, Rivera and Lieberman2016; Slade et al., Reference Slade, Cohen, Sadler, Miller and Zeanah2009). While a history of childhood adversity may be associated with prenatal mental health problems, complications during pregnancy, and early parenting difficulties (Osofsky et al., Reference Osofsky, Osofsky, Frazer, Fields-Olivieri, Many, Selby, Holman and Conrad2021; Seng et al., Reference Seng, Low, Sperlich, Ronis and Liberzon2009; Slade et al., Reference Slade, Cohen, Sadler, Miller and Zeanah2009), experiences with one’s own caregivers that were positive may be especially beneficial as pregnant individuals consider the type of parents that they hope to be (Lieberman et al., Reference Lieberman, Diaz and Van Horn2009; Narayan et al., Reference Narayan, Atzl, Merrick, River and Peña2019). Given the strong links between childhood, pregnancy, and future generations of children (Narayan et al., Reference Narayan, Oliver, Rivera and Lieberman2016, Reference Narayan, Lieberman and Masten2021), it is essential for research to continue examining the associations between childhood experiences, both adverse and positive, and perinatal mental health.
Childhood adversity
Research on childhood adversity and perinatal mental health problems has largely focused on the effects of ACEs on physical or reproductive health outcomes during pregnancy, including teenage pregnancies, unintended pregnancies, and substance abuse during pregnancy, as well as negative birth outcomes (e.g., Chung et al., Reference Chung, Nurmohamed, Mathew, Elo, Coyne and Culhane2010; Dietz et al., Reference Dietz, Spitz, Anda, Williamson, McMahon, Santelli, Nordenberg, Felitti and Kendrick1999; Frankenberger et al., Reference Frankenberger, Clements-Nolle and Yang2015; Hillis et al., Reference Hillis, Anda, Dube, Felitti, Marchbanks and Marks2004). A growing body of research has also begun to examine childhood adversity and mental health during pregnancy (e.g., Osofsky et al., Reference Osofsky, Osofsky, Frazer, Fields-Olivieri, Many, Selby, Holman and Conrad2021; Racine et al., 2020, 2021; Seng et al., Reference Seng, Kohn-Wood, McPherson and Sperlich2011, Reference Seng, Sperlich, Low, Ronis, Muzik and Liberzon2013; Wajid et al., Reference Wajid, van Zanten, Mughal, Biringer, Austin, Vermeyden and Kingston2020). For instance, a recent study indicated that total ACEs predicted depressive and PTSD symptoms during pregnancy, which were driven by experiences reflecting childhood maltreatment (i.e., abuse and neglect) rather than exposure to family/household dysfunction (Atzl, Narayan et al., Reference Atzl, Narayan, Rivera and Lieberman2019). Total ACEs were also related to higher levels of depression and PTSD symptoms during pregnancy in another study (Osofsky et al., Reference Osofsky, Osofsky, Frazer, Fields-Olivieri, Many, Selby, Holman and Conrad2021). When ACEs were further unpacked into experiences reflecting maltreatment versus family dysfunction in this sample, however, higher levels of maltreatment were associated with higher levels of depression and PTSD, while higher levels of family dysfunction were only associated with higher levels of PTSD (Osofsky et al., Reference Osofsky, Osofsky, Frazer, Fields-Olivieri, Many, Selby, Holman and Conrad2021). These studies, as well as others that have examined the differential effects of unique dimensions of ACEs on mental health outcomes outside the perinatal period, point to possible nuances in how specific dimensions of childhood adversity might distinctly relate to specific mental health outcomes (Narayan et al., Reference Narayan, Merrick, Lane and Larson2023; Sayyah et al., Reference Sayyah, Merrick, Larson and Narayan2022).
The long-term effects of childhood adversity on perinatal mental health may continue even after the baby is born. In fact, metanalytic findings have documented associations between higher numbers of childhood adversities and higher reports of postpartum depression symptoms (Racine et al., Reference Racine, Devereaux, Cooke, Eirich, Zhu and Madigan2021), with prenatal depression symptoms continuing to influence postnatal depression symptoms (e.g., Bohne et al., Reference Bohne, Høifødt, Nordahl, Landsem, Moe, Wang and Pfuhl2022; Mersky & Janczewski, Reference Mersky and Janczewski2018). Though previous research on childhood adversity and postnatal PTSD symptoms has mostly examined these associations in the context of individuals who reported a traumatic childbirth, some studies have documented significant associations between childhood adversity and postnatal PTSD symptoms more generally (Menke et al., 2019; Morelen et al., Reference Morelen, Menke, Rosenblum, Beeghly and Muzik2016; Oh et al., Reference Oh, Muzik, McGinnis, Hamilton, Menke and Rosenblum2016; Sexton et al., Reference Sexton, Hamilton, McGinnis, Rosenblum and Muzik2015). Of note, these studies did not account for prenatal PTSD symptoms as predictors of postnatal PTSD symptoms. A history of mental health problems is a strong developmental predictor of future mental health problems, reflecting continuity in risk for psychopathology across the life course (Cicchetti and Toth, Reference Cicchetti and Toth2009; Masten, Reference Masten2006; Sroufe, Reference Sroufe1979). Research that accounts for the effects of prenatal symptoms along with the effects of childhood adversity is needed to clarify the salience of childhood experiences and contemporaneous influences on postnatal mental health problems.
Some research on postnatal symptomatology also points to the importance of separately examining the distinct effects of childhood maltreatment versus exposure to family dysfunction. For instance, one study found that higher levels of childhood maltreatment, but not exposure to family dysfunction, were significantly associated with individuals’ depression symptoms six months postpartum (McDonnell & Valentino, Reference McDonnell and Valentino2016). In another study, higher levels of maltreatment were associated with a higher likelihood of prenatal depression symptoms carrying into the postpartum period, although this study did not examine effects of childhood exposure to family/household dysfunction (Grote et al., Reference Grote, Spieker, Lohr, Geibel, Swartz, Frank, Houck and Katon2012). Although research supports the associations between childhood maltreatment and postnatal PTSD symptoms (Menke et al., Reference Menke, Morelen, Simon, Rosenblum and Muzik2018; Morelen et al., Reference Morelen, Menke, Rosenblum, Beeghly and Muzik2016; Sexton et al., Reference Sexton, Hamilton, McGinnis, Rosenblum and Muzik2015), no studies to our knowledge have directly compared childhood maltreatment versus exposure to family dysfunction as predictors of postnatal PTSD symptoms, Research outside of the perinatal period continues to emphasize the robust links between childhood maltreatment and adulthood PTSD symptoms specifically (Narayan et al., Reference Narayan, Lieberman and Masten2021), so clarifying links from maltreatment to PTSD in the prenatal and postpartum period would strengthen understanding about intergenerational pathways of traumatic stress. Research is also needed that examines the effects of childhood maltreatment versus exposure to family dysfunction as predictors for various types of postnatal mental health outcomes while also accounting for prenatal mental health symptoms.
Positive childhood experiences
Associations between positive childhood experiences and prenatal mental health have also been increasingly documented (Han et al., Reference Han, Dieujuste, Doom and Narayan2023). In the original psychometric study of the BCEs scale, which included an ethnically diverse sample of 101 low-income pregnant individuals with high levels of childhood adversity, higher levels of BCEs from birth to 18 years predicted lower levels of PTSD symptoms and exposure to stressful life events (SLEs) during pregnancy, above and beyond the effects of ACEs on outcomes (Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018). Furthermore, greater numbers of BCEs began to offset the long-term effects of ACEs on PTSD symptoms and SLEs during pregnancy in individuals who had both high levels of BCEs and heightened ACEs. In a follow-up study in the same sample that further examined the developmental timing of BCEs, higher levels of BCEs in early childhood and adolescence were associated with lower levels of sexual risk taking, including unwanted, unintended, and teenage pregnancies (Merrick et al., Reference Merrick, Narayan, Atzl, Harris and Lieberman2020). Both of these studies demonstrated unique associations of BCEs with outcomes after accounting for the effects of ACEs.
In a separate sample of low-income pregnant individuals, higher levels of positive childhood experiences, defined as various aspects of positive parent-child relationships, were associated with lower levels of depressive symptoms (Chung et al., Reference Chung, Mathew, Elo, Coyne and Culhane2008). Data from the original ACEs study also found that higher levels of family-specific strengths such as family closeness, support, and responsiveness were associated with lower rates of adolescent pregnancies in the presence of childhood adversity, showing evidence of a protective effect (Hillis et al., Reference Hillis, Anda, Dube, Felitti, Marchbanks, Macaluso and Marks2010). Overall, these findings and results from a recent systematic review demonstrate that positive childhood experiences often occur despite childhood adversity and promote more positive pregnancy-related outcomes (Han et al., Reference Han, Dieujuste, Doom and Narayan2023). While limited studies have examined how BCEs are related to postnatal outcomes, results from one study demonstrated a similar promotive pattern, such that higher levels of BCEs were related to lower levels of postnatal depression symptoms even after accounting for prenatal depression symptoms (Cárdenas et al., Reference Cárdenas, Kujawa and Humphreys2022).
Contemporaneous adulthood risk and promotive factors for perinatal mental health
Sociodemographic factors
A separate but related body of literature has examined the effects of risk and promotive factors in adulthood, including those that occur during the perinatal period, on mental health symptoms during pregnancy and after birth. For instance, sociodemographic factors, including educational attainment, current employment, and income, are strong predictors of mental health during the transition to parenthood. Higher levels of sociodemographic stress (e.g., lower educational attainment and income, as well as unemployment) are associated with higher levels of prenatal and postnatal depression and PTSD symptoms (Goyal et al., Reference Goyal, Gay and Lee2010; Martínez-Vazquez et al., Reference Martínez-Vazquez, Rodríguez-Almagro, Hernández-Martínez, Delgado-Rodríguez and Martínez-Galiano2021; Seng et al., Reference Seng, Low, Sperlich, Ronis and Liberzon2009). Given the adulthood sociodemographic factors often related to mental health during pregnancy, it seems particularly important to consider contemporaneous risk factors, such as sociodemographic stress, in pregnant individuals, especially those with histories of childhood adversity. Contemporaneous sociodemographic stress (e.g., having a lower educational attainment, being unemployed, living in severe poverty) may represent an additional set of risk factors that uniquely influence both prenatal and postnatal depression and PTSD symptoms.
Social support
Social support during the perinatal period may also be an important contemporaneous promotive factor associated with lower levels of perinatal mental health problems. Pregnant individuals with higher levels of social support, broadly defined, reported lower levels of prenatal depression (Westdahl et al., Reference Westdahl, Milan, Magriples, Kershaw, Rising and Ickovics2007), and new mothers with higher levels of social support reported lower levels of depression and PTSD symptoms (Sumner et al., Reference Sumner, Valentine, Eisenman, Ahmed, Myers, Wyatt, Liu, Zhang and Rodriguez2011; Surkan et al., Reference Surkan, Peterson, Hughes and Gottlieb2006). The promotive effects of social support have also been studied among pregnant individuals with histories of childhood adversity, with results indicating similar patterns for better perinatal mental health (Atzl, Grande et al., Reference Atzl, Grande, Davis and Narayan2019; Racine et al., Reference Racine, Zumwalt, McDonald, Tough and Madigan2020).
Support from the second biological parent may exert particularly salient promotive effects on pregnant individuals’ mental health (Narayan et al., Reference Narayan, Oliver, Rivera and Lieberman2016; River et al., Reference River, Narayan, Atzl, Rivera and Lieberman2020a, b; Slade et al., Reference Slade, Cohen, Sadler, Miller and Zeanah2009). Indeed, higher levels of both self-reported and coder-rated partner support from the second biological parent were related to pregnant individuals’ lower levels of prenatal depression and PTSD symptoms in another sample of individuals with high childhood adversity (River et al., Reference River, Narayan, Atzl, Rivera and Lieberman2020a, b). Other research has found that higher self-reported support from the partner was also related to individuals’ lower postpartum depression symptoms (Gremigni et al., Reference Gremigni, Mariani, Marracino, Tranquilli and Turi2011).
Despite extensive research on adulthood risk and promotive factors for perinatal mental health, little research has considered these factors alongside risk and promotive factors that occurred in childhood. Considering childhood and adulthood experiences together, both those that are adverse and positive, is essential to understand the full picture of experiences affecting pregnant individuals’ wellbeing throughout the perinatal period (Narayan et al., Reference Narayan, Atzl, Merrick, River and Peña2019, Reference Narayan, Lieberman and Masten2021). Understanding the ways that experiences across the lifespan additively influence perinatal mental health symptoms has immense potential to inform prenatal care and screening and provide tailored trauma-informed services to support pregnant individuals before babies are born.
The current study
This study examined the childhood experiences and contemporaneous factors that were associated with mental health problems during pregnancy and at three-to-four months postpartum. Mental health problems were operationalized as symptoms of depression and PTSD, given previous research on the associations between childhood and adulthood adversity and these two outcomes, particularly during the perinatal period, and because these were the two focal mental health outcomes of Narayan et al.’s (Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018) original validation study of the BCEs scale (hereinafter referred to as the original study). This study replicated and extended those findings in the following key ways.
Aim and hypothesis 1
Aim 1 sought to replicate the original findings on the effects of BCEs and ACEs for prenatal depression and PTSD symptoms (Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018), with the slight modification that this study examined childhood maltreatment and exposure to family dysfunction separately given accumulating evidence on distinct dimensions of adversity. We accounted for a similar set of sociodemographic covariates as those in the original study including maternal age, gestational age, and primiparous status, as well as an additional covariate, childhood income status. We hypothesized that BCEs would show a promotive effect (i.e., direct association) on outcomes, both dimensions of ACEs (i.e., childhood maltreatment and exposure to family/household dysfunction) would show risk effects (also direct associations) on outcomes, and all childhood experiences would each significantly predict both types of prenatal mental health problems after accounting for sociodemographic covariates.
Aim and hypothesis 2
Aim 2 extended findings from the original study by also accounting for effects of contemporaneous factors, including sociodemographic stress and prenatal social support from the second biological parent, on prenatal mental health problems. By including both childhood and contemporaneous predictors of prenatal mental health problems we provide a more stringent test of the effects of childhood experiences. We hypothesized that BCEs would continue to show a promotive effect and both dimensions of ACEs would continue to show risk effects on prenatal depression and PTSD symptoms after accounting for contemporaneous sociodemographic stress and social support and sociodemographic covariates.
Aim and hypothesis 3
Aim 3 built on Aims 1 and 2 to examine the promotive effects of BCEs and the risk effects of both dimensions of ACEs for postnatal depression and PTSD symptoms. We hypothesized that the promotive effects of BCEs and the risk effects of ACEs would be significant for postnatal mental health problems after accounting for the effects of prenatal mental health problems. We also expected that the effects of childhood experiences would hold after accounting for prenatal sociodemographic stress and prenatal and contemporaneous social support and sociodemographic covariates.
Methods
Participants
Participants were 175 low-income, ethnically diverse pregnant individuals (M age = 28.07 years, SD = 5.68, range = 18–40; 38.9% White, 25.7% Latina, 16.6% Black, 12.0% biracial/multiracial, 6.8% other) who participated in a longitudinal study on the intergenerational transmission of risk and resilience through the perinatal period. Across the sample, pregnant individuals reported high levels of previous and current sociodemographic stress (see below), and approximately half of the sample (51.7%) reported a lifetime history of homelessness. Eligible participants were a) at least 18 years old, b) spoke English, c) in their second (67.4%) or third (32.6%) trimester of pregnancy at the time of study recruitment (M gestational age = 23.71 weeks, SD = 7.29, range = 13–39), and d) planning to deliver their babies at the urban general hospital in a western U.S. metropolitan city. All individuals were recruited via fliers posted in the OB/GYN and Labor and Delivery Clinics at the hospital, by a hospital-based OB/GYN research manager/recruitment liaison during routine prenatal visits or childbirth classes, and via fliers posted online to the Craigslist forum. Second parents (the other biological parent and/or the pregnant individual’s partner who was planning to be involved in parenting) were recruited as well, although the current study solely focused on data from 175 pregnant individuals.
Pregnant individuals completed the first study assessment (Wave 1) during pregnancy and the second study assessment (Wave 2) when their babies were three-to-four months old (M age = 23.71 weeks, SD = 7.29, range = 13–39); 48.8% male; 51.2% female). Approximately 69.1% (n = 121) of pregnant participants who completed Wave 1 also completed Wave 2. Attrition rates were primarily due to research personnel not being able to reach participants from Wave 1 with any contact information provided. See attrition analyses below. All participants completed Wave 1 before the COVID-19 pandemic began, and 21 participants (17.4%) completed Wave 2 after the COVID-19 pandemic began.
Measures: independent variables
Benevolent childhood experiences
During Wave 1, all participants completed the BCEs scale (Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018), a culturally sensitive measure with excellent test-retest stability that assesses the presence of 10 favorable childhood experiences reflecting safety, support, and predictability from family, peers, teachers, and neighbors, and a positive quality of life. Positive items are summed to yield a total BCEs score (M = 8.19, SD = 1.66, range = 3–10). Approximately one fourth of the sample (25.7%) positively endorsed all 10 BCEs.
Adverse childhood experiences
During Wave 1, all participants completed the ACEs scale (CDC, 2020, Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards, Koss and Marks1998; Schmidt et al., Reference Schmidt, Narayan, Atzl, Rivera and Lieberman2020), a 10-item checklist of childhood adversity. Participants’ responses were used to measure the following two variables:
Childhood maltreatment
The first five items on the ACEs scale reflect childhood experiences of maltreatment (emotional abuse, physical abuse, sexual abuse, emotional neglect, physical neglect). All positively endorsed items were summed to create a total maltreatment score (M = 1.73, SD = 1.62, range = 0–5).
Childhood exposure to family dysfunction
The second five items on the ACEs scale include parental separation or divorce, domestic violence, and household member substance use, mental illness, or incarceration. A total score for exposure to family dysfunction was created by summing all positively endorsed items (M = 2.55, SD = 1.51, range = 0–5).
Prenatal sociodemographic stress
A cumulative sociodemographic stress variable was created to capture sociodemographic stress during pregnancy by summing the following three dichotomized variables collected at Wave 1: Participants having less than a high school education (or equivalent; 19.4%), being currently unemployed (52.6%), and living below the federal poverty line (42.3%). Total scores ranged from 0 to 3 (M = 1.14, SD = 1.01).
Social support from the second biological parent
During Waves 1 and 2, all participants completed the Five-Minute Speech Sample (FMSS) (Magaña et al., Reference Magaña, Goldstein, Karno, Miklowitz, Jenkins and Falloon1986), adapted to assess relationship quality with the second biological parent. All participants were asked to speak about the baby’s second biological parent, including “what kind of person they are” and “how the two of you get along together” for five minutes without interruption. Interviews were audio-recorded, transcribed, and later coded for emotional and instrumental support (River et al., Reference River, Narayan, Atzl, Rivera and Lieberman2020a; River et al., Reference River, Narayan, Atzl, Rivera and Lieberman2020b). Two trained raters coded all the data with good reliability (ICC = .85) and conferenced all disagreements. Total scores on this variable ranged from 0 (No support) to 5 (High support) on the prenatal FMSS (M = 2.94, SD = 1.35) and the postnatal FMSS (M = 2.85, SD = 1.30). Participants’ prenatal and postnatal FMSS scores were significantly correlated (r = .59, p = <.001).
Dependent variables
Prenatal and postnatal depression symptoms
During Wave 1 and Wave 2, all participants completed the Edinburgh Postnatal Depression Inventory (EPDS; Cox et al, Reference Cox, Holden and Sagovsky1987). All positively endorsed items were summed to yield a total score (prenatal depression symptoms M = 7.91, SD = 4.76, range = 0-24, α = .82; postnatal depression symptoms M = 5.74, SD = 4.63, range = 0-26, α = .85). Using the cutoff recommended by the American Academy of Pediatrics (total score ≥ 10; Earls, Reference Earls2010), 33.7% of the sample endorsed prenatal depression in the clinical range, and 18.2% of the sample endorsed postnatal depression in the clinical range.
Prenatal and postnatal PTSD symptoms
During Wave 1 and Wave 2, all participants completed the PTSD Checklist for the DSM-5 (PCL-5; Weathers et al., Reference Weathers, Litz, Keane, Palmieri, Marx and Schnurr2013). Of note, participants were not asked about specific criterion A events in relation to PTSD symptoms. Many adults in this study had experienced cumulative adversity [54.9% of participants endorsed four or more ACEs, a threshold associated with multiplicative risk for long-term health problems (Dube et al., Reference Dube, Felitti, Dong, Giles and Anda2003)], and many also had ongoing cumulative stress. Indeed, as noted above, over half of the sample also reported previous homelessness. Individuals with complex trauma, including multiple childhood adversities and cumulative stressors, typically cannot distinguish discrete Criterion A events that correspond symptoms, as symptoms of complex PTSD may themselves be incompatible with the ability to differentiate which traumatic events correspond to which PTSD symptoms (Courtois & Ford, Reference Courtois and Ford2013). Thus, study participants were instructed to respond to questions about symptoms without needing to keep only one previous traumatic experience in mind. All positively endorsed items were summed to yield a total score (prenatal PTSD symptoms M = 21.02, SD = 15.53, range = 0–67, α = .92; postnatal PTSD symptoms M = 19.69, SD = 14.95, range = 0–68, α = .93). Based on the cutoff recommended by the National Center of PTSD (total score ≥ 33; National Center for PTSD, 2017), 22.4% of the sample endorsed prenatal PTSD symptoms in the clinical range and 20.7% of the sample endorsed postnatal PTSD symptoms in the clinical range.
Covariates
Maternal age, primiparous status (22.9%), and childhood income status were included as covariates in all analyses. Childhood income status was assessed using a validated 1-5-point self-report scale assessing participant’s self-reported income status from their most formative childhood home environment: (1-Poor, 2-Low-income, 3-Middle-class, 4-Well-to-do, 5-Wealthy; M = 2.47, SD = .83, range = 1–5; Sayyah et al., Reference Sayyah, Merrick, Larson and Narayan2022). All analyses that examined prenatal depression or PTSD symptoms as the outcome variable also included maternal gestational age as an additional covariate, and all analyses that examined postnatal depression or PTSD symptoms as the outcome variable also included infant age as an additional covariate.
Data analytic plan, attrition analyses, and missing data
Data analytic plan
Aim 1 (i.e., replication the original BCEs study; Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018) was tested using two separate hierarchical regressions for prenatal depression and prenatal PTSD symptoms. For both regressions, covariates were entered in the first step, followed by the main effects of BCEs in the second step, and childhood maltreatment and exposure to family dysfunction in the third step.
Aim 2 (i.e., extension of the original BCEs study to also include effects of contemporaneous factors) was tested using two separate hierarchical regressions for prenatal depression and prenatal PTSD symptoms. For both regressions, covariates were entered in the first step, followed by the main effects of BCEs in the second step, childhood maltreatment and exposure to family dysfunction in the third step, and the contemporaneous sociodemographic stress and prenatal support variable in the fourth step.
Aim 3 (i.e., extension of the original BCEs study to predict postnatal mental health problems) was also tested using two separate hierarchical regressions for postnatal depression and postnatal and PTSD symptoms. All variables were entered in the same order that they had been entered in Aim 2 and prenatal symptomatology (i.e., either prenatal depression or PTSD symptoms) was also entered in the fourth step that included sociodemographic stress during pregnancy and prenatal support. The postnatal support variable was entered in the fifth step. All analyses were completed in SPSS version 28.
Attrition analyses
Independent t-tests and chi-square tests were conducted to examine whether the 121 participants who participated in Wave 2 differed on any of the predictors or covariates from the 54 participants who did not participate in Wave 2. There were no significant group differences between participants who did versus did not participate in Wave 2 on primiparous status, gestational age, childhood income status, total BCEs, childhood maltreatment, exposure to family dysfunction, prenatal mental health symptoms, prenatal sociodemographic stress, or prenatal support. Maternal age was the one variable that significantly differed between the two groups, t (133) = 2.58, p = .011, such that those who participated in Wave 2 were younger (M = 27.35, SD = 5.78) than those who did not participate in the Wave 2 interview (M = 29.70, SD = 5.12). Independent t-tests were also conducted to examine whether means on postnatal depression symptoms, PTSD symptoms, and social support differed for the 21 participants who completed Wave 2 after the COVID-19 pandemic began. There were no significant differences in mean levels of postnatal depression symptoms, PTSD symptoms, or social support between participants who completed the Wave 2 interview before versus after the COVID-19 pandemic began.
Missing data
Missing data on key variables in analyses for the 175 participants at Wave 1 and the 121 participants at Wave 2 were very minimal and were addressed using listwise deletion. Missingness for variables collected in Wave 1 ranged from 0% on most covariates to approximately 3% (n = 5) on the prenatal support variable. No participants were missing data for childhood maltreatment or BCEs, and only one participant was missing data for exposure to family dysfunction. No participants were missing data for prenatal depression symptoms, and one participant was missing data for prenatal PTSD symptoms. Two participants were missing data on sociodemographic stress. Only approximately 3% of participants (n = 4) who completed the Wave 2 (postnatal) interview were missing data for the postnatal support variable. No participants who completed Wave 2 were missing data for postnatal depression or PTSD symptoms. The total amount of missing data across the entire dataset was less than 1%, so analyses for missing data were not deemed necessary.
Results
Descriptive statistics
Bivariate correlations between all variables are presented in Table 1. Higher levels of BCEs were significantly associated with lower levels of prenatal and postnatal mental health problems (prenatal depression r = −.19, p = .010, prenatal PTSD r = −.24, p = .001, postnatal depression r = −.21, p = .023, postnatal PTSD r = −.23, p = .012). Higher BCEs were also associated with lower levels of prenatal sociodemographic stress (r = −.26, p < .001), though they were not significantly associated with higher levels of prenatal social support (r = .09, p = .259) or postnatal social support (r = .04, p = .691).
Table 1. Bivariate correlations and descriptive statistics for all study variables
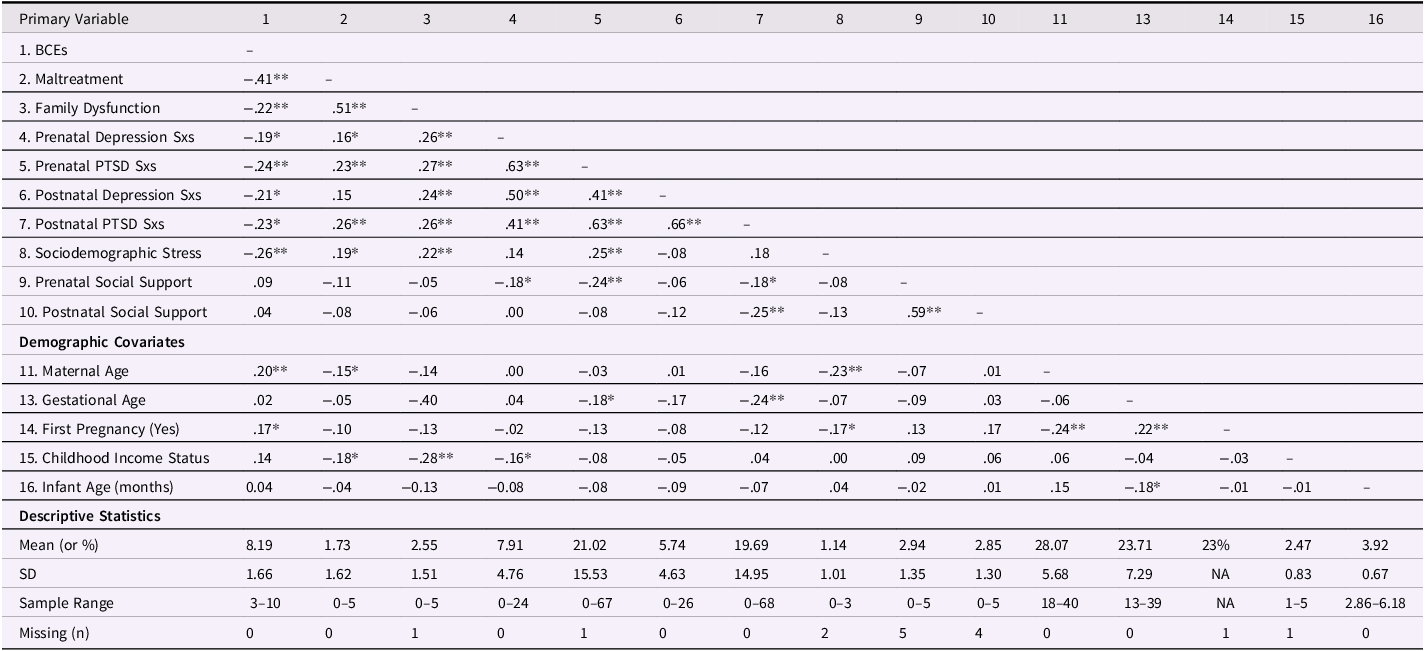
Note. Sxs. = Symptoms. * p < .05. ** p < .01.
Higher levels of maltreatment were significantly associated with higher levels of prenatal depression symptoms (r = .16, p = .031), prenatal PTSD symptoms (r = .23, p = .002), and postnatal PTSD symptoms (r = .26, p = .004). They were not significantly associated with higher levels of postnatal depression symptoms (r = .15 p = .100), lower levels of prenatal social support (r = −.11, p = .172), or lower levels of postnatal social support (r = −.08, p = .407) Higher levels of family dysfunction were significantly associated with higher levels of prenatal and postnatal depression symptoms (r = .26, p < .001, r = .24, p = .007, respectively) and prenatal and postnatal PTSD (r = .27, p < .001, r = .26, p = .004, respectively). Higher levels of family dysfunction were not significantly associated with lower levels of prenatal social support (r = −.05, p = .501) or postnatal social support (r = −.06, p = .551).
Higher levels of maltreatment and family dysfunction were also both significantly associated with higher levels of sociodemographic stress (r = .19, p = .012, r = .22, p = .003, respectively). Finally, higher levels of BCES were significantly but only moderately associated with lower levels of maltreatment (r = −.41, p < .001) and family dysfunction (r = −.22, p = .003).
Aim 1: childhood experiences as predictors of prenatal mental health
Prenatal depression symptoms
In the final step of this regression (Table 2), higher levels of family dysfunction (β = .23, p = .010) significantly predicted higher levels of prenatal PTSD symptoms. This model accounted for 10.3% of the variance (R 2 ) in prenatal depression symptoms (p = .012).
Table 2. Regressions examining the risk and promotive effects of childhood experiences for prenatal depression and post-traumatic stress disorder (PTSD) symptoms with all covariates and predictors included in the models (Aim 1)
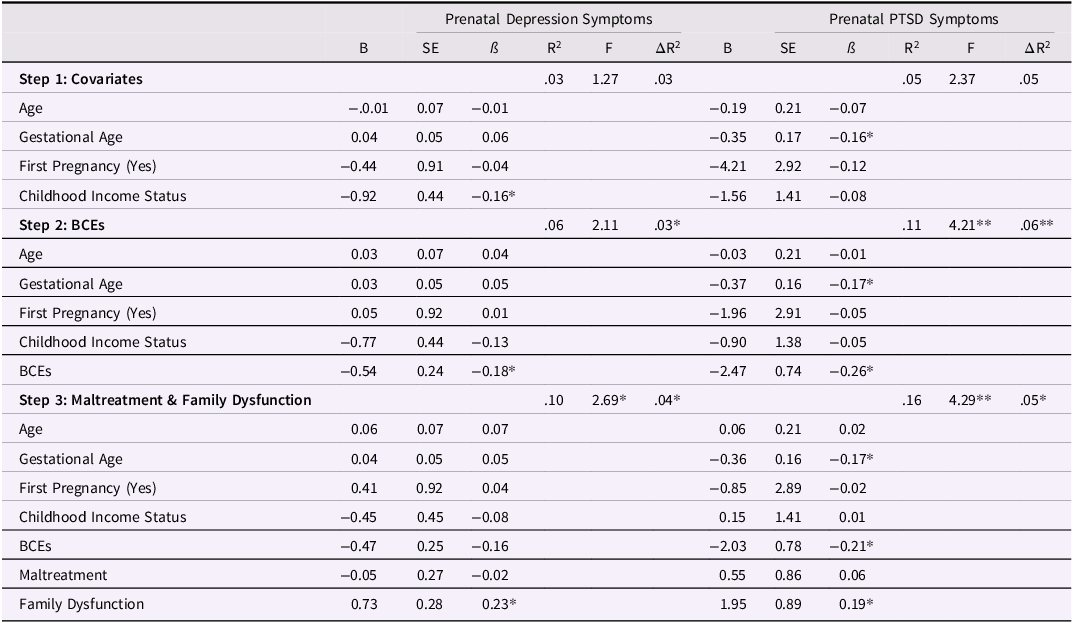
*p < .05. ** p < .01.
Prenatal PTSD symptoms
In the final step of this regression (Table 2), lower levels of BCEs (β = −.21, p = .010), higher levels of family dysfunction (β = .19, p = .029), and lower gestational age (β = −.17, p = .025) significantly predicted lower levels of prenatal PTSD symptoms. This model accounted for 15.5% of the variance (R 2 ) in prenatal depression symptoms (p < .001).
Aim 2: childhood experiences and contemporaneous stress and social support as predictors of prenatal mental health
Prenatal depression symptoms
In the final step of the regression (Table 3), higher levels of family dysfunction significantly predicted higher levels of prenatal depression symptoms (β = .23, p = .012). This model accounted for 12.6% of the variance (R 2 ) in prenatal depression symptoms (p = .011). The final step of the regression, which included contemporaneous stress and social support, accounted for 2.7% of the variance (R 2 ) in prenatal depression symptoms (p = .095).
Table 3. Final step of the regressions examining the risk and promotive effects of childhood and contemporaneous experiences for prenatal depression and post-traumatic stress disorder (PTSD) symptoms with all covariates and predictors included in the models (Aim 2)
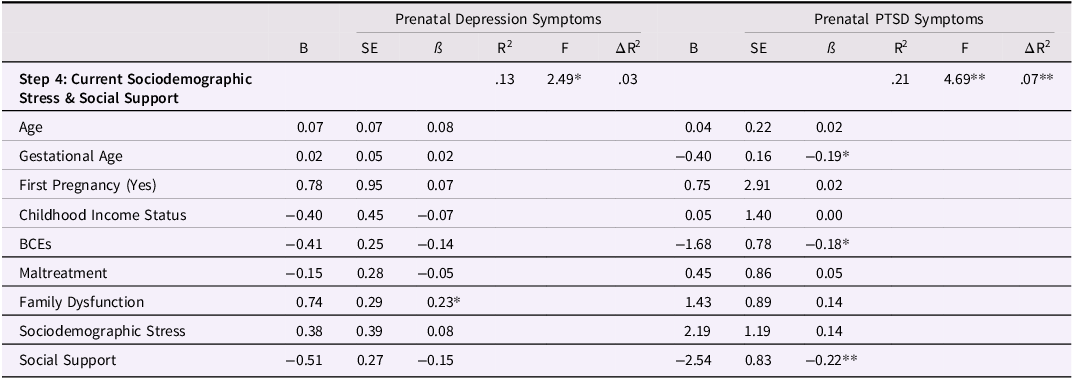
*p < .05. ** p < .01.
Prenatal PTSD symptoms
In the final step of this regression (Table 3), higher levels of BCEs (β = −.18, p = .033) and higher levels of social support (β = −.22, p = .003) significantly predicted lower levels of prenatal PTSD symptoms. Greater gestational age also significantly predicted lower levels of prenatal PTSD symptoms (β = −.19, p = .012). This model accounted for 21.3% of the variance (R 2 ) in prenatal PTSD symptoms (p < .001). The final step of the regression, which included contemporaneous stress and social support, accounted for 6.8% of the variance (R 2 ) in prenatal depression symptoms (p = .002).
Aim 3: childhood experiences, prenatal stress, social support, and mental health problems, and postnatal social support as predictors of postnatal mental health problems
Postnatal depression symptoms
In the final step of the regression (Table 4), higher levels of prenatal depression symptoms significantly predicted higher levels of postnatal depression symptoms (β = .46, p < .001). This model accounted for 33.4% of the variance (R 2 ) in postnatal depression symptoms (p < .001). The fourth step of the regression, which included prenatal stress, social support, and depression symptoms, accounted for 19.5% of the variance (R 2 ) in prenatal depression symptoms (p < .001). The final step of the regression, which included postnatal support, accounted for 1.5% of the variance (R 2 ) in prenatal depression symptoms (p = .173).
Table 4. Regressions examining the risk and promotive effects of childhood and contemporaneous experiences for postnatal depression and post-traumatic stress disorder (PTSD) symptoms with all covariates and predictors included in the models (Aim 3)
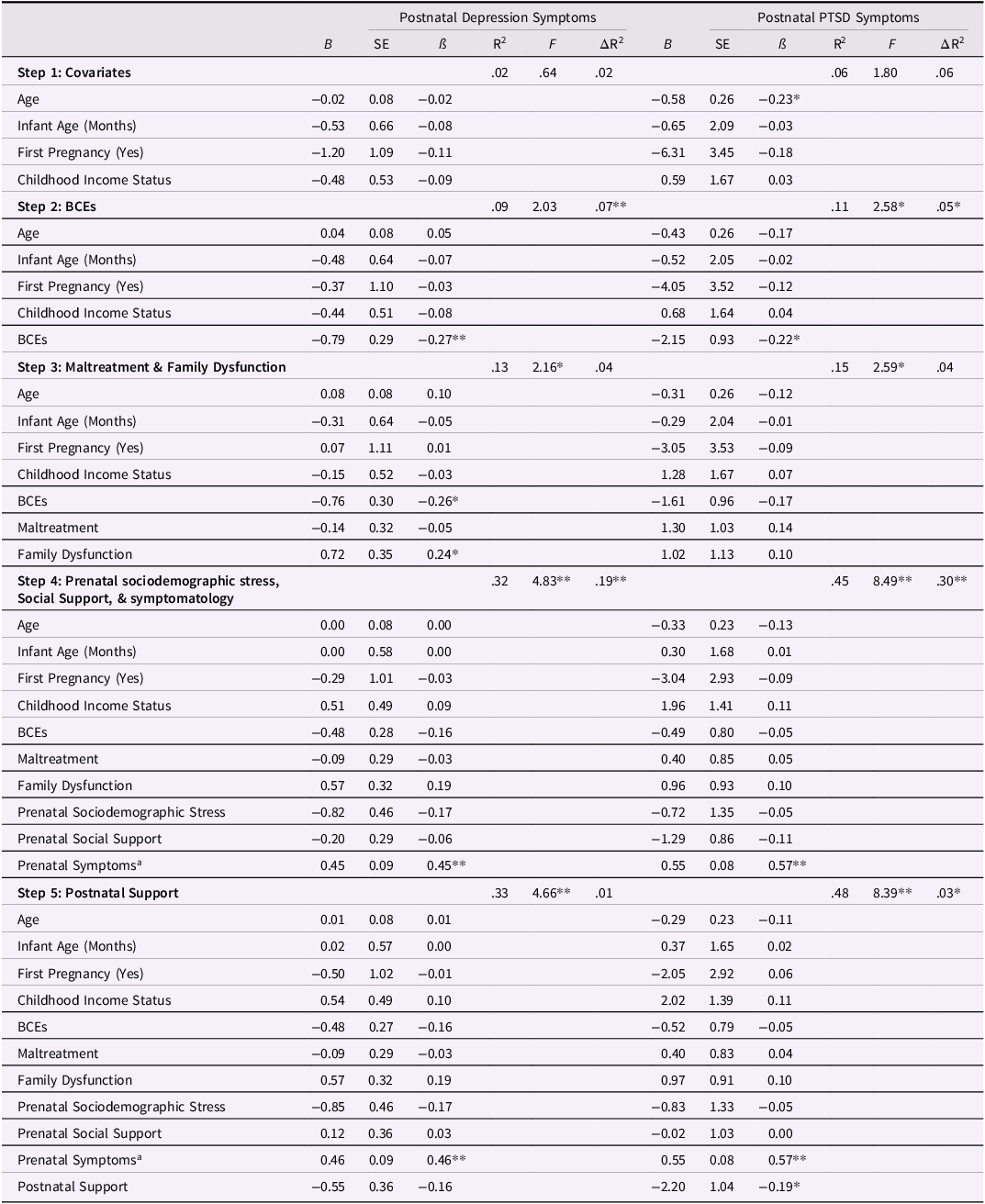
Note. a indicates that prenatal depression symptoms were examined in the regression for postnatal depression symptoms and prenatal PTSD symptoms were examined in the regression for postnatal PTSD symptoms. * p < .05. ** p < .01.
Postnatal PTSD symptoms
In the final step of this regression (Table 4), higher levels of prenatal PTSD symptoms significantly predicted higher levels of postnatal PTSD symptoms (β = .57, p < .001). In addition, higher levels of postnatal social support significantly predicted lower levels of postnatal PTSD symptoms (β = −.19, p = .036). This model accounted for 47.5% of the variance (R 2 ) in postnatal PTSD symptoms (p < .001). The fourth step of the regression, which included prenatal stress, social support, and PTSD symptoms, accounted for 30.6% of the variance (R 2 ) in prenatal depression symptoms (p < .001). The final step of the regression, which included postnatal support, accounted for 2.3% of the variance (R 2 ) in prenatal depression symptoms (p = .036).
Discussion
Findings highlight the associations between both childhood and contemporaneous experiences and mental health symptoms during the perinatal period in a sample of 175 low-income, ethnically diverse pregnant individuals. Results replicated the original BCEs study and highlighted the role of childhood experiences for pregnancy-related outcomes (Aim 1). Findings also showed that higher levels of family dysfunction were associated with higher levels of prenatal depression symptoms, while higher levels of BCEs and prenatal social support were associated with lower levels of prenatal PTSD symptoms when childhood and contemporaneous experiences were both included in the model (Aim 2). Prenatal depression and prenatal PTSD symptoms were significantly associated with postnatal depression and PTSD symptoms, respectively, and higher postnatal social support was also associated with lower postnatal PTSD symptoms (Aim 3).
Replication of original study
Results from the first aim partially supported the first hypothesis. Findings regarding higher levels of childhood family dysfunction and higher prenatal depression symptoms demonstrate robust associations between discord and dysfunction in the childhood family-of-origin and depression symptoms during pregnancy, over and above the effects of childhood maltreatment and BCEs. These results are consistent with the original BCEs study, which indicated that the effects of BCEs on prenatal depression symptoms did not hold above and beyond the effects of ACEs (Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018). Our results provide further insight into antecedents of prenatal depression, indicating that they seem to stem from childhood exposure to family dysfunction. These findings also highlight the importance of examining different dimensions of childhood adversity rather than considering total ACEs all together as one indicator of cumulative risk (e.g., Merrick et al., Reference Merrick, Narayan, Atzl, Harris and Lieberman2020; Narayan et al., Reference Narayan, Kalstabakken, Labella, Nerenberg, Monn and Masten2017; Sayyah et al., Reference Sayyah, Merrick, Larson and Narayan2022).
Significant associations between higher levels of BCEs, lower levels of family dysfunction, and lower levels of prenatal PTSD symptoms also replicated findings from the original BCEs study. These results demonstrate the role of BCEs for prenatal symptoms of PTSD even after accounting for the effects of maltreatment and family dysfunction. Of note, childhood maltreatment and exposure family dysfunction were examined separately in the current study, whereas in the original study they were examined together total ACEs. These results suggest that at least in the current sample, the significant effects of ACEs on prenatal PTSD symptoms were driven by childhood exposure to family dysfunction. Taken together, these findings support the replicable association of higher BCEs and lower ACEs with lower prenatal PTSD symptoms and point to the need to continue to examine the role of PTSD symptoms in the transmission of ACEs and BCEs and across generations (Narayan et al., Reference Narayan, Lieberman and Masten2021).
Risk and promotive factors for prenatal mental health
Findings from the second aim also partially supported the second hypothesis. Higher levels of childhood family dysfunction continued to be associated with higher levels of prenatal depression symptoms even after contemporaneous experiences were included. Exposure to family dysfunction remained significantly associated with prenatal depression symptoms not only above and beyond the other childhood experiences, but also above and beyond other contemporaneous influences - pregnant individuals’ social support and sociodemographic stress. Past research has documented significant associations between childhood maltreatment, as opposed to family dysfunction (even when both are accounted for together in the same models), and prenatal depression symptoms in other samples of pregnant individuals (e.g., Atzl, Narayan et al., Reference Atzl, Narayan, Rivera and Lieberman2019; Osofsky et al., Reference Osofsky, Osofsky, Frazer, Fields-Olivieri, Many, Selby, Holman and Conrad2021). These previous studies have not accounted for the role of BCEs as counterparts to multiple dimensions of ACEs in predicting prenatal mental health problems, nor have they accounted for the role of contemporaneous influences.
In terms of prenatal PTSD symptoms, higher levels of BCEs and higher levels of contemporaneous support were significantly associated with lower levels of prenatal PTSD symptoms when childhood and contemporaneous factors were both included in the model. Findings on the role of BCEs and contemporaneous support demonstrate the effects of positive experiences above and beyond childhood adversity for prenatal PTSD symptoms (but not prenatal depression symptoms). These findings are consistent with research on cumulative positive influences as predictors of more resilient outcomes (Masten, Reference Masten2001) and indicate that positive experiences in childhood and support during pregnancy may relate to lower risk for prenatal PTSD even in the context of childhood and contemporaneous adversity and stress. Taken together, findings highlight that research examining childhood and contemporaneous influences, including those that are both positive and negative, provides a more nuanced and comprehensive set of predictors for prenatal mental health problems.
Risk and promotive factors for postnatal mental health
Results from the third aim also partially supported our hypotheses. First, prenatal depression symptoms were the one and only variable that was significantly associated with postnatal depression symptoms in the final step of the regression. Findings are consistent with previous research documenting symptoms of depression during pregnancy as one of the most robust predictors of postnatal depression symptoms (Schaffir, Reference Schaffir2018). These results indicate that identifying and addressing symptoms of depression during the prenatal period has immense potential to not only impact individuals’ wellbeing during pregnancy, but also after the baby is born. By providing pregnant individuals with the tools, resources, and referrals to decrease their symptoms of depression while they are pregnant, providers may be able to help to decrease symptoms of depression postnatally as well, a topic that could be explored in future clinical research.
Higher levels of prenatal PTSD symptoms and lower levels of current support from the second biological parent were significantly associated with higher levels of postnatal PTSD symptoms. Just as prenatal depression symptoms have been documented as robustly associated with postnatal symptoms of depression, prenatal PTSD symptoms have been documented as a robustly associated with postnatal symptoms of PTSD (Onoye et al., Reference Onoye, Goebert, Morland, Matsu and Wright2009), and current results further supported this pattern. Providers may therefore wish to approach prenatal symptoms of PTSD in a manner similar to the suggested approach to prenatal depression symptoms above, addressing these mental health difficulties during pregnancy to decrease postnatal symptoms in turn. Results on the significant role of postnatal support also indicate that in the early postpartum period, relationships with the babies’ other biological parent may be another important target for screening, especially for individuals who are at risk for heightened PTSD symptoms given their prenatal symptomatology. These findings point to the need for more intervention-based research focused on helping new parents understand how they can best provide support one another during the postnatal period, which may also strengthen their mental health.
Strengths and limitations
The current study was one of the first to examine how childhood and adulthood risk and promotive factors are together associated with functioning during the perinatal period. By examining experiences that occur both during and after childhood, this study considers a more extensive range of factors that may influence mental health symptoms during and shortly after pregnancy. Aside from the novel and unique approach to examining risk and resilience, this study was strengthened by the ability to examine pregnant individuals’ mental health symptoms at two timepoints, with the second time point measured prospectively into the early postpartum period. The current study also utilized a combination of self-reported data (e.g., for both types of childhood experiences and mental health symptoms and stress) and coder-rated data (for prenatal and postnatal social support). Relatedly, the use of the FMSS as a coder-rated assessment of support extended previous research that found significant effects of positive childhood experiences on mental health problems when using self-reported measures of social support (Bethell et al., Reference Bethell, Jones, Gombojav, Linkenbach and Sege2019; Doom et al., Reference Doom, Seok, Narayan and Fox2021).
The current study was limited by the retrospective nature by which childhood experiences were assessed. While some research has indicated potential limitations of retrospective reporting, including potentially inflated associations between childhood experiences and contemporaneous outcomes if the same informant is used for all variables (Reuben et al., Reference Reuben, Moffitt, Caspi, Belsky, Harrington, Schroeder, Hogan, Ramrakha, Poulton and Danese2016), other research has shown that many findings (e.g., linking childhood experiences to adulthood PTSD symptoms) still hold when accounting for current depression symptoms (Narayan et al., Reference Narayan, Merrick, Lane and Larson2023). Here, we found that mostly different predictor variables were associated with the outcome variables of depression versus PTSD symptoms, suggesting unique risk and promotive factors that vary for different mental health outcomes during the perinatal period. However, future research utilizing a design that includes both retrospective and prospective reporting formats for childhood experiences would be ideal, as recent research indicates that each type of format likely provides unique information on childhood adversity (Baldwin et al., Reference Baldwin, Reuben, Newbury and Danese2019).
The current study is also limited by the fact that it only assessed symptoms of depression and PTSD during and after pregnancy. There are other mental health difficulties that may influence individuals’ wellbeing during the perinatal period, such as symptoms of perinatal anxiety (Racine et al., Reference Racine, Devereaux, Cooke, Eirich, Zhu and Madigan2021). Of note, depression and anxiety are the most common mental health problems that pregnant people experience (e.g., Chauhan & Potdar, Reference Chauhan and Potdar2022), and both of these mental health problems are highly prevalent during the postpartum period (Field, Reference Field2018). These findings underscore the importance of further understanding the risk and promotive factors for perinatal anxiety symptoms alongside the risk and promotive factors for perinatal depression and PTSD symptoms examined in the current study.
While these results are likely to be especially relevant for samples of pregnant and postpartum individuals and/or those who have experienced high levels of adversity, it should be noted that they may have less generalizability to community samples that have higher income or are not recruited during the perinatal period. Finally, this study is limited by the fact that approximately one quarter of the current sample endorsed all 10 BCEs items, limiting the variability of total BCEs scores. It is important to note that while these data were collected using the original BCEs scale (Narayan et al., Reference Narayan, Rivera, Bernstein, Harris and Lieberman2018), which was the only BCEs instrument available at the time, an expanded version of the BCEs scale with 20 items is now available (Narayan et al., Reference Narayan, Merrick, Lane and Larson2023). The BCEs-20 includes a more comprehensive list of positive childhood experiences with more variability across items and total scores.
Clinical implications and conclusions
These findings can have key clinical implications for perinatal health services. They underscore that regardless of current stressors or supports during pregnancy, pregnant individuals may be at a heightened risk for prenatal PTSD symptoms due to a low level of positive experiences in their own childhood. Since the pregnancy period is a time when individuals may reflect back on how they were cared for as children in preparation for caring for a new child (Slade et al., Reference Slade, Cohen, Sadler, Miller and Zeanah2009), individuals who had a scarcity of positive childhood experiences might be at particular risk for elevated PTSD symptoms during pregnancy, whether or not they also experienced heightened childhood adversity (Narayan et al., Reference Narayan, Lieberman and Masten2021). Pregnant individuals with higher levels of BCEs, on the other hand, may benefit from opportunities to reflect on their own positive childhood experiences and the ways in which they plan to incorporate them into their babies’ lives.
Results highlight the importance of asking pregnant individuals about their BCEs, or lack thereof, during prenatal care visits. Specific advantages of the BCEs scale over the ACEs scale as a screening tool about childhood experiences are that the presence of BCEs signals a favorable set of childhood experiences, and the absence of BCEs also signals important information: a childhood lacking in these favorable experiences, which itself signals the presence of risk. Alternatively, while the presence of ACEs signals the presence of risk, the absence of ACEs doesn’t provide information on what was present and positive (Merrick & Narayan, Reference Merrick and Narayan2020). Given the ways that the presence or absence of certain childhood experiences can relate to perinatal mental health, providers may consider integrating this measure into their practice as a supplement to (or even a replacement for) screening for ACEs.
Given the significant associations between higher levels of support from the second biological parent and lower levels of prenatal PTSD symptoms documented here and in other studies (e.g., River et al., Reference River, Narayan, Atzl, Rivera and Lieberman2020a, b), providers could also inquire about pregnant individuals’ relationships with the second biological parent. For instance, providers could ask pregnant individuals about the support, or lack thereof, that they are experiencing to identify those who are most at risk for prenatal PTSD symptoms, most isolated without support, or most in need of resources to strengthen their relationships.
In conclusion, the current results demonstrate that specific types of childhood and adulthood experiences, both adverse and positive, uniquely contribute to mental health symptoms during the perinatal period. Consistent with the results of the original BCEs study, both childhood adversity and positive childhood experiences were related to prenatal mental health symptoms. In terms of postnatal symptomatology, when prenatal depression and PTSD symptoms were included in the models, they were the most robust predictors of postnatal depression and PTSD symptoms, respectively. These findings suggest that while childhood experiences likely have a far reach on functioning into adulthood, their reach may not be as strong for postpartum mental health problems as the effects that prenatal mental health problems have on postnatal mental health problems.
Social support from the baby’s second biological parent, however, may be another important factor that influences aspects of both prenatal and postnatal mental health. Therefore, a complete understanding of an individual’s early and contemporaneous experiences is essential to fully understanding the wide array of factors that may contribute to mental health difficulties during the pregnancy and postpartum periods.
By screening for both childhood and adulthood adversities and stressors, as well as asking pregnant individuals about their positive childhood experiences and current support, there is a higher likelihood of identifying individuals’ risk and promotive factors that may be best addressed and leveraged with tailored preventive perinatal interventions. Findings indicate that it is important to conduct screenings of childhood experiences during pregnancy and also assess more contemporaneous factors such as support both during and after pregnancy. Furthermore, given the robust associations between prenatal and postnatal symptoms, preventive interventions that lower symptomatology during pregnancy may indirectly lower postnatal symptomatology as well. These future research and clinical endeavors are key to better understanding the intergenerational transmission of risk and resilience from parents’ own adverse and positive experiences to those of their children.
Competing interests
None.





 Open access
Open access