



The article by Hu et al. is very meaningful. Reference Hu, Yao and Qiu1 We agree that a series of Early Warning Scores, including Standardized Early Warning Score (SEWS), National Early Warning Score (NEWS), National Early Warning Score 2 (NEWS2), and Hamilton Early Warning Score (HEWS), have the potential to be used as screening tools for predicting the mortality risk of severe coronavirus disease 2019 (COVID-19) patients. However, the data collected in this study are only used to calculate the Early Warning Scores, actually, some studies have shown that other rapid scoring systems, such as Quick Sequential Organ Failure Assessment (qSOFA) Reference Liu, Yao and Qiu2 and Rapid Emergency Medicine Score (REMS), Reference Hu, Yao and Qiu3 can also be used to assist in predicting the risk of death in patients with severe COVID-19. What’s more, they are also used in clinical practice. Reference Miller, Nazir and McDonald4 Consequently, we collected some study subjects and their data through systematic records of the wards from March 7 to April 7 in 2020 to assess the value of the other 2 rapid scoring systems.
COVID-19 is responsible for the outbreak of severe respiratory illness, is now spreading rapidly throughout the world. Reference Chakraborty, Sharma and Sharma5 And it is necessary to evaluate COVID-19 with fast and accurate methods; hence, we collected the relevant population data from the medical records, which included 17 nonsurvivors, then we collected the hospitalization, clinical manifestations, and laboratory examination results to calculate the scores. Next, we drew the receiver operating characteristic (ROC) curve to analyze and compare the predictive effectiveness of REMS, qSOFA, and NEWS, HEWS by using the IBM Statistical Program for Social Sciences Statistics 25.0 (SPSS; IBM Corp). We collected 127 subjects, excluding 3 patients with missing data. Among them, there are 110 (86.6%) patients alive, and the average age of the survivor and nonsurvivor are 59.08 ± 14.87 and 75.29 ± 12.78 y. In addition, the data include 47 male survivors and 13 male nonsurvivors. The results of ROC curve analysis and areas under the curve (AUC) are showed in Table 1 and Figure 1. The AUCs of REMS, qSOFA, NEWS, and HES are 0.826, 0.700, 0.774, and 0.764, respectively (Table 1). It can be clearly seen that REMS was the most effective scoring system in this study. And its AUCs suggest that NEWS and NEWS2 are nearly identical for screening COVID-19 patients (Table 1).
Table 1. AUC of 6 scoring systems in predicting in-hospital mortality
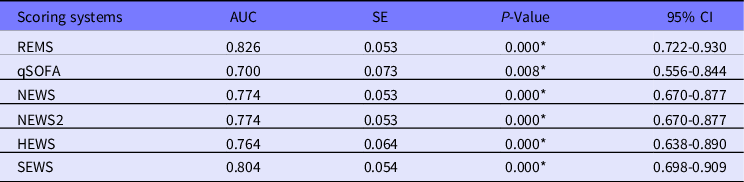
Abbreviations: AUC, area under the curve of the receiver operating characteristic; CI, confidence interval; HEWS, Hamilton Early Warning Score; NEWS, National Early Warning Score; NEWS2, National Early Warning Score2; qSOFA, Quick Sequential Organ Failure Assessment; REMS, Rapid Emergency Medicine Score; SE, standard error; SEWS, Standardized Early Warning Score.
*P < 0.05.
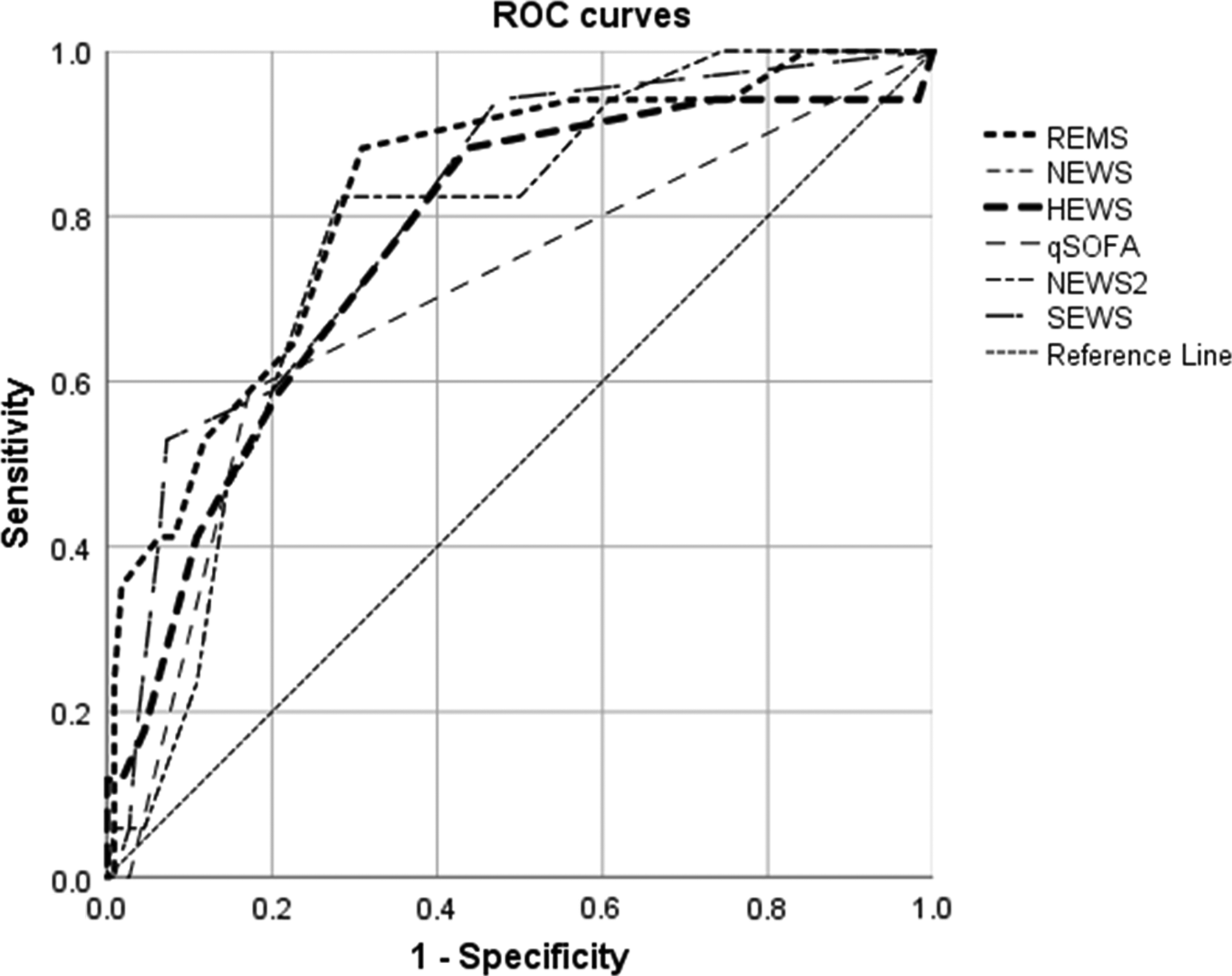
Figure 1. The ROC curves of scoring systems for predicting the mortality of COVID-19 patients. REMS, Rapid Emergency Medicine Score; qSOFA, Quick Sequential Organ Failure Assessment; NEWS, National Early Warning Score; NEWS2, National Early Warning Score2; HEWS, Hamilton Early Warning Score; SEWS, Standardized Early Warning Score.
As stated in the original, we agree quite well that SEWS, HEWS, NEWS, and NEWS2 have the potential to be used as tools for screening severely and critically ill COVID-19 patients. Reference Hu, Yao and Qiu1 Meanwhile, another conclusion can be drawn, that is, that REMS does well in predicting the mortality risk of COVID-19 patients and it is the most accurate in this research. Therefore, we hold the view that REMS also has great potential in COVID-19 evaluation. Moreover, the predictive performance of qSOFA is also acceptable.
Author’s Contribution
Longping Yan: Software, Methodology, Data analysis, Writing and editing. Wei Wang: Data collection. Ruijun Luo: Data collection
Conflict of Interests
All authors declare no competing interests.


