



Introduction
Reading is a complex process that requires the implementation of various skills simultaneously. To begin with, it requires recognition of the visual information necessary to extract the information from text [Reference Aghababian and Nazir1]. The core reading skill is phonological processing, which involves recognition of the sound structure of the language, the decoding of written symbols into sounds (phonological awareness), and then their maintenance in working memory (phonological memory) [Reference Wagner and Torgesen2]. Phonological processing facilitates the decoding of written information, which leads to word identification and subsequent extraction of meaning [Reference Pollatsek, Rayner and Lee3]. A failure to read each word correctly leads to problems with comprehension [Reference Perfetti4] as comprehension involves the processing of individual letters and words, and then putting them together to form meaning [Reference Judd and Gray5]. When one or more of these reading skills are impaired, and this impairment cannot be explained by general cognitive dysfunction or intelligence, this is referred to as dyslexia [Reference Lyon, Shaywitz and Shaywitz6]. Overlaps between dyslexia and schizophrenia (SZ) have been suggested, based on previous findings of disruption in the processes that support skilled reading (e.g., deficits in language, auditory and visual perception, oculomotor control) in both disorders [Reference Whitford, O’Driscoll and Titone7] but the nature and severity of reading skills deficits in SZ and other severe mental illnesses (MIs) remain unclear at present.
Reading skills are of enormous significance for a range of socioeconomic outcomes in modern societies, including academic performance, occupational achievement, and family and social relationships [Reference Ritchie and Bates8,Reference Duncan, Dowsett, Claessens, Magnuson, Huston and Klebanov9]. Furthermore, poor reading skills in children have been associated with increased antisocial behavior [Reference Maughan, Pickles, Hagell, Rutter and Yule10,Reference Trzesniewski, Moffitt, Caspi, Taylor and Maughan11]. Likewise, in forensic populations, poor reading skills and dyslexia traits have been associated with increased anxiety and poor socialization, which, in turn, might explain their antisocial behavior [Reference Jensen, Lindgren, Meurling, Ingvar and Levander12,Reference Baker and Ireland13]. In people with various MIs, undiagnosed reading problems, and dyslexia result in scholastic failure, in turn raising the risk for mood problems [Reference Maughan, Rowe, Loeber and Stouthamer-Loeber14] and future criminal behavior [Reference Daderman, Lindgren and Lidberg15]. Poor reading skills also pose a challenge for accessibility of mental health interventions [Reference Sentell and Shumway16] and predict poor psychosocial outcomes [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Dondé, Martinez, Sehatpour, Patel, Kraut and Kantrowitz18]. There is thus a need to consider reading deficits as a therapeutic target and address them, for example, with interventions used for dyslexia [Reference Whitford, O’Driscoll and Titone7,Reference Law, Wouters and Ghesquière19]. A thorough understanding of the pattern and magnitude of reading deficits in people with specific MIs is an important first step toward this goal.
The main aim of this systematic and meta-analytic review was to conduct a comprehensive analysis to delineate the nature and magnitude of reading impairments based on data from studies that employed standardized tools to assess reading skills in people with SZ, bipolar disorder, affective disorders (major depression, anxiety, mania), personality disorders (PDs; borderline personality disorder [BPD], antisocial personality disorder [ASPD], psychopathy), and general MIs (across diagnoses/not-specified). Our secondary aims were to examine whether (a) particular reading skill deficits were more strongly present when assessed with some tests compared to others, given that reading skills in different studies have been quantified using a variety of tests and batteries, and (b) groups with MIs and a forensic history show more pronounced deficits relative to those from nonforensic settings.
Methods
This systematic literature review and meta-analysis followed PRISMA guidelines [Reference Liberati, Altman, Tetzlaff, Mulrow, Gøtzsche and Ioannidis20]. Search terms and key articles were identified based on an exploratory search of databases and an internet search engine (Google Scholar). We then searched Academic Search Complete, CINAHL Plus, PsycINFO, PsycARTICLES, SocINDEX, MEDLINE via EBSCO Host and PubMed (up to Feb 2020) for all studies including reading assessment(s) in MIs (see Table 1 for the full search strategy and eligibility criteria). Manual searches were conducted using the relevant literature [Reference Whitford, O’Driscoll and Titone7,Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21].
Table 1. Full search strategy per database and eligibility criteria.

Abbreviations: MI, Mental Illness; Intelligence Quotient, IQ
Two independent reviewers selected the studies (MV, BJ), and extracted and reviewed data for inconsistencies to reach a consensus (MV, LAW). Extracted data included tests and measures (Table 2), as well as participant characteristics, main findings, the language of assessment, and country (Table 3).
Table 2. Tests and measures used in the selected studies (k = 34) and diagnoses assessed. Studies involving forensic populations are in italics.
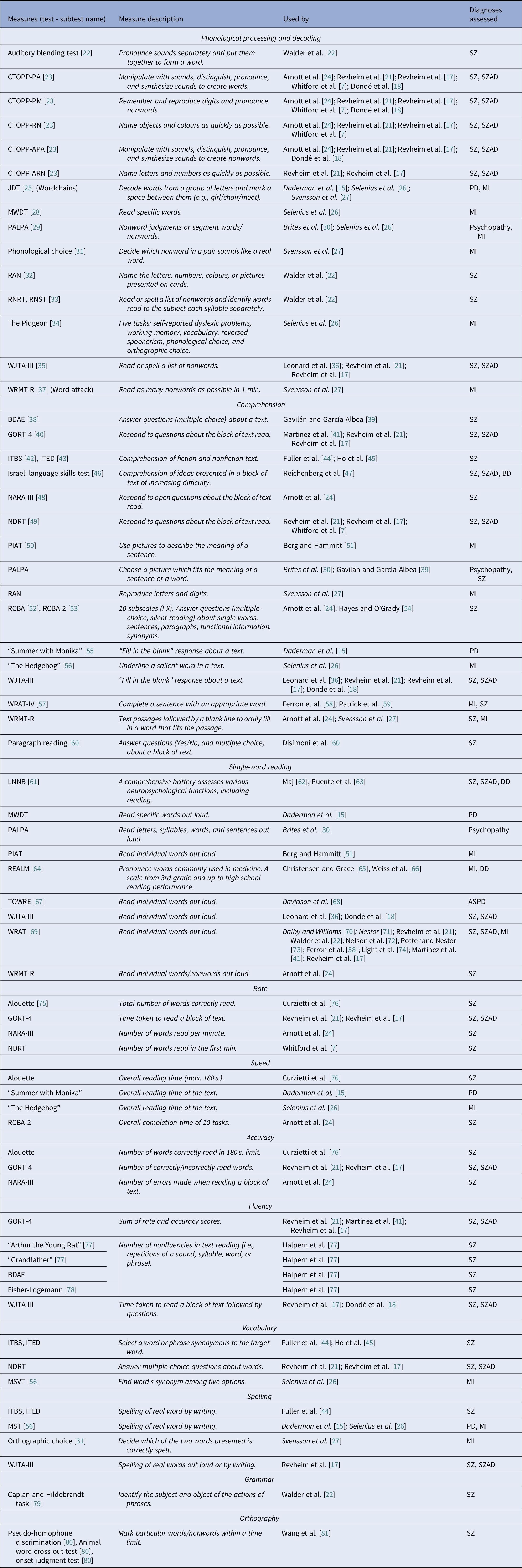
Abbreviations: BD, Bipolar Disorder; BDAE, Boston Diagnostic Aphasia Examination; CTOPP, Comprehensive Test of Phonological Processing (PA, Phonological Awareness; PM, Phonological Memory; RN, Rapid Naming; APA, Alternative Phonological Awareness; ARN, Alternative Rapid Naming); DD, Depressive Disorder; GORT, Gray Oral Reading Test; HC, Healthy Controls; ITBS, Iowa Test of Basic Skills; ITED, Iowa Test of Educational Development; JDT, Jacobson’s Decoding Test; LNNB, Luria-Nebraska Neuropsychological Battery; MI, Mental Illness; MST, Madison’s Spelling Test; MSVT, Madison’s Standardized Vocabulary Test; MWDT, Madison’s Word Decoding Test; NARA, Neale Analysis of Reading Ability; NDRT, Nelson–Denny Reading Test; PALPA, Psycholinguistic Assessments of Language Processing in Aphasia; PD, Personality Disorder; PIAT, Peabody Individual Achievement Test; RAN, Rapid Automatised Naming; RCBA, Reading Comprehension Battery for Aphasia; REALM, Rapid Estimate of Adult Literacy in Medicine; RNRT, Roentgen’s Nonwords Reading Test; RNST, Roeltgen’s Nonwords Spelling Test; SZ, Schizophrenia; SZAD, Schizoaffective Disorder; TOWRE, Test of Word Reading Efficiency; WJTA-III, Woodcock–Johnson III Tests of Achievement (BR, Broad Reading; BRS, Basic Reading Skills; RC, Reading Comprehension; PKG, Phoneme-Grapheme Knowledge); WRAT, Wide Range Achievement Test; WRMT-R, Woodcock Reading Mastery Test—Revised (BS, Basic Skills; PC, Passage Comprehension; PKG, Phoneme-Grapheme Knowledge).
Table 3 Summary of key data extracted from selected studies (k = 34).

Abbreviations: AdjD, Adjustment Disorder; AfD, Affective Disorder; Alc, Alcoholism; BD, Bipolar Disorder; BDAE, Boston Diagnostic Aphasia Examination; BPRS, Brief Psychiatric Rating Scale; CPZE, Chlorpromazine equivalents; CTOPP, Comprehensive Test of Phonological Processing (PA, Phonological Awareness, PM, Phonological Memory, RN, Rapid Naming, APA, Alternative Phonological Awareness, ARN, Alternative Rapid Naming); DD, Depressive Disorder; FC, Forensic Controls (history of violence without MI); GORT, Gray Oral Reading Test; HC, Healthy Controls; ITBS, Iowa Test of Basic Skills; ITED, Iowa Test of Educational Development; JDT, Jacobson’s Decoding Test; LNNB, Luria-Nebraska Neuropsychological Battery; Mac-CAT-CR, MacArthur Treatment Competence Assessment Tool for Clinical Research; MCCB, MATRICS Consensus Cognitive Battery; MI, Mental Illness; MST, Madison’s Spelling Test; MSVT, Madison’s Standardized Vocabulary Test; MWDT, Madison’s Word Decoding Test; NARA, Neale Analysis of Reading Ability; NDRT, Nelson–Denny Reading Test; NE, Not Examined; NR, Not Reported; PALPA, Psycholinguistic Assessments of Language Processing in Aphasia; PANNS, Positive and Negative Syndrome Scale; PD, Personality Disorder; PIAT, Peabody Individual Achievement Test; RAN, Rapid Automatised Naming; RCBA, Reading Comprehension Battery for Aphasia; REALM, Rapid Estimate of Adult Literacy in Medicine; RNRT, Roentgen’s Nonwords Reading Test; RNST, Roeltgen’s Nonwords Spelling Test; SZ, Schizophrenia; SZAD, Schizo-Affective Disorder; TOWRE, Test of Word Reading Efficiency; WJCog, Woodcock–Johnson Test of Cognitive Ability; WJTA-III, Woodcock–Johnson III Tests of Achievement (BR, Broad Reading, BRS, Basic Reading Skills, RC, Reading Comprehension, PKG, Phoneme-Grapheme Knowledge); WRAT, Wide Range Achievement Test; WRMT-R, Woodcock Reading Mastery Test—Revised (BS, Basic Skills, PC, Passage Comprehension, PKG, Phoneme-Grapheme Knowledge).
Studies including forensic populations are marked *Forensic*.
Studies included in the meta-analysis are marked “Meta-analysis”.
Bold entries indicates Visual aid to distinguish studies using a control group as a reference
Studies that reported means and standard deviations (s.d.) for patient and healthy control (HC) groups to permit the calculation of effect sizes were included in the meta-analysis (effect sizes also presented where only one study available). The remaining studies contributed only to the narrative synthesis (see Table 3 for details). Studies assessing individuals with conditions primarily classified as neurodevelopmental (ADHD, autism, learning difficulties, and intellectual disabilities) [82] were excluded.
Statistical analysis
The meta-analysis was conducted using Review Manager 5.3 Software—RevMan [83]. For eligible studies, effect sizes were calculated as Hedge’s g (standardized mean difference). A random-effects model was used as a more conservative approach. Heterogeneity was calculated as the I2 measure of consistency for each meta-analytic calculation. Planned analyses included comparing each diagnosis (SZ, bipolar disorder, depression, anxiety, PDs, psychopathy), and unspecified general MI with healthy groups on specific reading skills (phonological processing and decoding; comprehension; single-word reading; rate, speed, accuracy, and fluency). For each reading skill, differences between tests to assess deficits in the patient group were calculated by investigating overlaps of confidence intervals of the summary effect sizes for each test. Risk of publication bias (none identified) was formally assessed via Egger’s and Begg’s tests and with funnel plots.
Results
Of 34 studies in total (Tables 2–3), 19 studies provided data for meta-analysis (Figure 1. PRISMA flowchart); five of these studies also presented composite scores (combining two or more measures) that are covered in the narrative synthesis. The remaining 15 studies contributed to the narrative synthesis only. The findings from the nonforensic and forensic samples are presented separately, followed by a direct comparison of forensic and nonforensic groups.
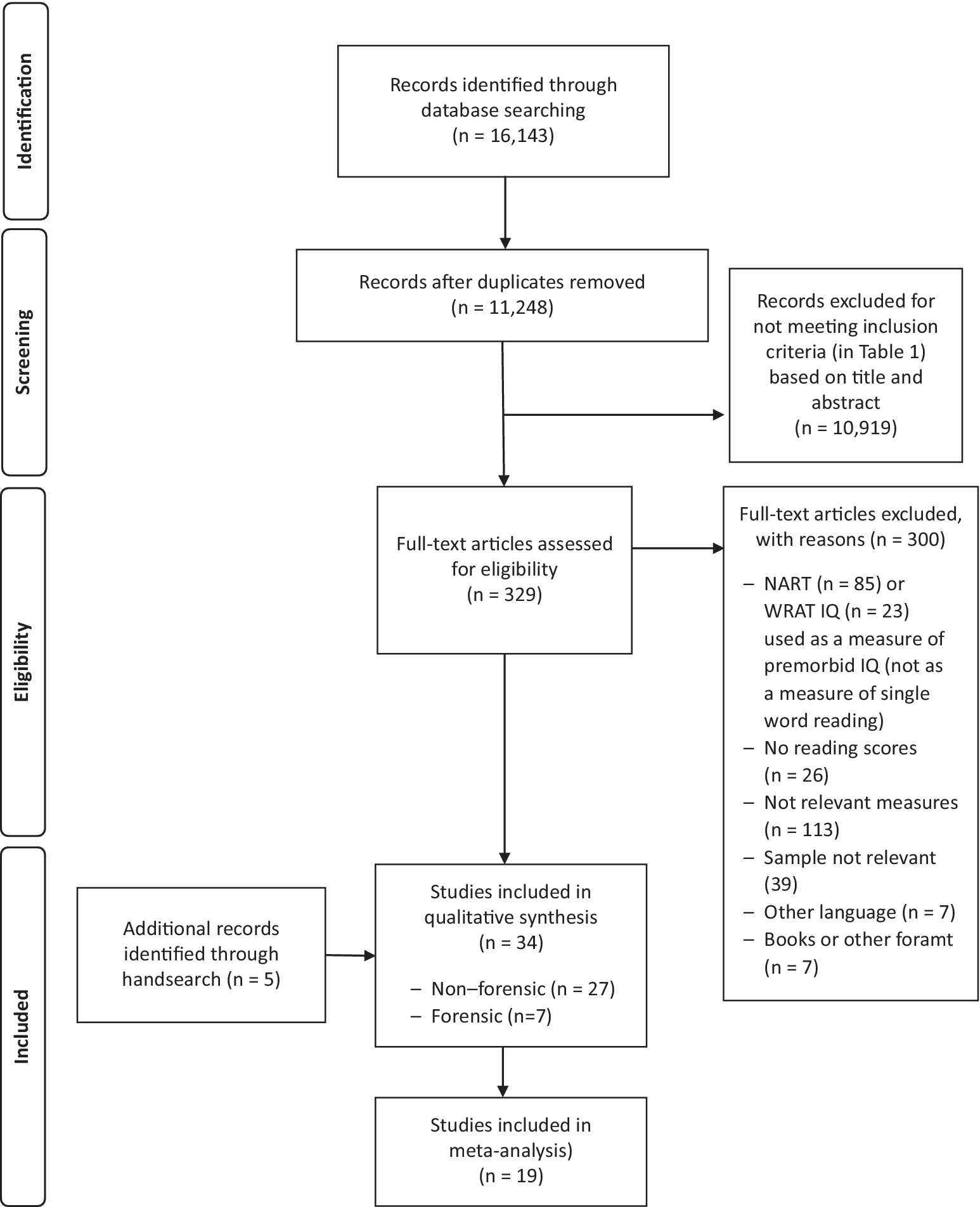
Figure 1. PRISMA flowchart.
Reading Skills in Nonforensic Populations
Schizophrenia
Phonological Processing and Decoding: Across seven studies (Figure 2(2.1)), SZ showed significantly poorer phonological processing compared to HC with a large effect size (Hedge’s g = −0.88, df = 24, p < 0.00001, CI = [−1.07, −0.70]). There was medium heterogeneity within the data (p = 0.001, I 2 = 53%), with nonsignificant differences between the tests (p = 0.15, I 2 = 32.3%).

2.1. Phonological processing and decoding

2.2. Comprehension

2.3 Single-word reading

2.4. Rate

2.5 Accuracy

2.6 Fluency

2.7 Speed
Figure 2. Reading deficits in schizophrenia (non-forensic population). Within each specific reading skill, the results are presented for each of the test(s)/measures used, followed by the analysis of differences between tests (last row). Negative values represent a poorer performance of people with schizophrenia in comparison to HC.
References: Arnott et al. [Reference Arnott, Sali and Copland24]; Curzietti et al. [Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76]; Dondé et al. [Reference Dondé, Martinez, Sehatpour, Patel, Kraut and Kantrowitz18]; Gavilán and García-Albea [Reference Gavilán and García-Albea39]; Hayes and O’Grady [Reference Hayes and O’Grady54]; Ho et al. [Reference Ho, Andreasen, Nopoulos, Fuller, Arndt and Cadoret45]; Leonard et al. [Reference Leonard, Kuldau, Maron, Ricciuti, Mahoney and Bengtson36]; Light et al. [Reference Light, Swerdlow, Rissling, Radant, Sugar and Sprock74]; Maj [Reference Maj62]; Martinez et al. [Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41]; Patrick et al. [Reference Patrick, Rastogi and Christensen59]; Potter and Nestor [Reference Potter and Nestor73]; Revheim et al. [Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21]; Revheim et al. [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17]; Walder et al. [Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22]; Whitford et al. [Reference Whitford, O’Driscoll and Titone7]. Abbreviations: BDAE, Boston Diagnostic Aphasia Examination; CTOPP, Comprehensive Test of Phonological Processing (PA, Phonological Awareness, PM, Phonological Memory, RN, Rapid Naming, APA, Alternative Phonological Awareness, ARN, Alternative Rapid Naming); GORT, Gray Oral Reading Test; ITBS, Iowa Test of Basic Skills; ITED, Iowa Test of Educational Development; LNNB, Luria-Nebraska Neuropsychological Battery; NARA, Neale Analysis of Reading Ability; NDRT, Nelson–Denny Reading Test; PALPA, Psycholinguistic Assessments of Language Processing in Aphasia; RAN, Rapid Automatised Naming; RCBA, Reading Comprehension Battery for Aphasia; RNRT, Roentgen’s Nonwords Reading Test; RNST, Roeltgen’s Nonwords Spelling Test; WJTA-III, Woodcock-Johnson III Tests of Achievement Knowledge); WRAT, Wide Range Achievement Test; WRMT-R, Woodcock Reading Mastery Test-Revised. White circle ![]() —effect size for a particular study determining the difference between patients and controls. Black diamond
—effect size for a particular study determining the difference between patients and controls. Black diamond ![]() —pooled effect size for particular test/subtest. Red diamond
—pooled effect size for particular test/subtest. Red diamond ![]() —overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
—overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
Comprehension: Across 11 studies (Figure 2(2.2)), SZ showed poorer comprehension than HC with a large overall effect size (Hedge’s g = −0.96, df = 34, p < 0.00001, CI = [−1.15, −0.78]) and medium heterogeneity (p < 0.00001, I 2 = 69%). The test differences were significant (p < 0.0001, I 2 = 74.5%) with NDRT [Reference Brown, Fishco and Hanna49] and GORT-4 [Reference Wiederholt and Bryant40] showing the largest effect sizes for a comprehension deficit in SZ. In addition, three studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41] reported lower Oral Reading Quotient from GORT-4 [Reference Wiederholt and Bryant40]. In other studies, retrospective assessment revealed that those with a current diagnosis were below the norm during 4th to 11th grade of school [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44], with the most prominent deficit in the 11th grade, indicating a gradual decline [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44,Reference Ho, Andreasen, Nopoulos, Fuller, Arndt and Cadoret45]. A similar study on adolescents, who later developed psychosis, displayed a premorbid deficit in comprehension and sentence reading relative to HC [Reference Reichenberg, Weiser, Rabinowitz, Caspi, Schmeidler and Mark47].
Single-Word Reading: Across 10 studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Dondé, Martinez, Sehatpour, Patel, Kraut and Kantrowitz18,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22,Reference Arnott, Sali and Copland24, Reference Leonard, Kuldau, Maron, Ricciuti, Mahoney and Bengtson36,Reference Patrick, Rastogi and Christensen59,Reference Maj62,Reference Potter and Nestor73,Reference Light, Swerdlow, Rissling, Radant, Sugar and Sprock74], there was a significant medium-size deficit (Figure 2(2.3)) in SZ relative to HC (Hedge’s g = −0.70, df = 9, p < 0.00001, CI = [−0.94, −0.46]). There was significant heterogeneity within the results (p = 0.01, I 2 = 58%) but no test performed better than others (p = 0.20, I 2 = 35.6%). Moreover, in two studies [Reference Maj62,Reference Puente, Rodenbough and Orrell63], both using LNNB—Reading subtest (see Table 2 for test descriptions) [Reference Christensen61]—SZ showed a deficit compared to HC (data for meta-analysis not provided). In a third study [Reference Nelson, Combs, Penn and Basso72], SZ scored markedly lower (M = 78.00, SD = 21.01) than the norm (M = 100) on WRAT-III [Reference Wilkinson84].
Rate, Speed, Accuracy, and Fluency: Across five studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Arnott, Sali and Copland24,Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76,Reference Whitford, O’Driscoll, Pack, Joober, Malla and Titone85], there was a significant large effect of SZ diagnosis on reading rate (Hedge’s g = −1.22, df = 4, p = 0.002, CI = [−1.98, −0.46]) (Figure 2(2.4)). The effect of diagnosis [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Arnott, Sali and Copland24,Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76] in accuracy failed to reach significance (Hedge’s g = −0.73, df = 3, p = 0.09, CI = [−1.56, 0.10]) (Figure 2(2.5)). There were, however, significant test differences for both rate (p = 0.04, I 2 = 64.9%) and accuracy (p = 0.01, I 2 = 77.1%), with the GORT-4 revealing large deficits [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21], and the Alouette [Reference Lefavrais75] showing no deficit [Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76] (Figures 2(2.4–2.5)). In fluency [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Dondé, Martinez, Sehatpour, Patel, Kraut and Kantrowitz18,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41,Reference Halpern, McCartin-Clark and Wallack77], there was a highly significant deficit in SZ (Hedge’s g = −2.03, df = 4, p < 0.00001, CI = [−2.82, −1.24]), but with large heterogeneity within results (84%) (Figure 2(2.6)). In reading speed (time taken to read certain content) [Reference Arnott, Sali and Copland24,Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76], the effect of diagnosis was nonsignificant (Hedge’s g = −0.50, df = 1, p = 0.11, CI = [−1.11, −0.11]) (Figure 2(2.7)). In an additional study [Reference Halpern, McCartin-Clark and Wallack77], 10–11% of SZ demonstrated nonfluencies (e.g., sound repetitions at beginning of word) in sentence and paragraph reading during the BDAE [Reference Goodglass and Kaplan38].
Composite Scores: Two studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21] that examined Basic Reading Skills (phonological processing and single-word reading) and Phoneme-Grapheme Knowledge (phonological processing and orthography) composite scores from WJTA-III [Reference Mather and Wendling35] showed different results, with only one of these showing a significant deficit in SZ [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17]. Both studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21] found significantly lower WJTA-III Broad Reading (phonological processing, comprehension, speed) scores in SZ, relative to HC. The study [Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22] that created a phonology composite score by combining the RNRT [Reference Roeltgen33], RNST [Reference Roeltgen33], WRAT-R [Reference Jastek and Wilkinson86], and the Controlled Oral Word Association Test (COWAT) [Reference Benton87] also reported a significant deficit in SZ relative to HC.
Reading-related skills
Vocabulary: Six studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22,Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44,Reference Ho, Andreasen, Nopoulos, Fuller, Arndt and Cadoret45,Reference Wang, Wang, Xia, Liu, Quan and Tian81] assessed reading-related skills in SZ. There was evidence of impaired vocabulary from an early age [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44,Reference Ho, Andreasen, Nopoulos, Fuller, Arndt and Cadoret45] and those with prodromal illness scored significantly below grade-norms when assessed by the ITBS [Reference Hoover, Hieronymus, Dunbar and Frisbie42] and ITED [Reference Forsyth, Ansley, Feldt and Alnot43] as a part of their school performance. Vocabulary, assessed using the NDRT [Reference Brown, Fishco and Hanna49], was also impaired in two studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21].
Spelling and Grammar: Spelling in RNST [Reference Roeltgen33] was found to be adversely affected in male patients, while female patients scored similarly to HC [Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22]. Another study [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44], which longitudinally assessed spelling together with grammar and other language-related skills by ITBS [Reference Hoover, Hieronymus, Dunbar and Frisbie42], found a significant decline in abilities at 11th grade in SZ. Similarly, SZ scored significantly lower in the WJTA-III [Reference Mather and Wendling35] spelling subtest compared to HC [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17]. Grammar was assessed exclusively in one study [Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22], using Caplan and Hildebrandt’s task [Reference Caplan and Hildebrandt79], showing a stronger and significant deficit in male, relative to female, patients [Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22].
Orthography: Orthography processes are not reading abilities. However, in languages such as Chinese, orthography and semantics play an important role in reading, in contrast to alphabetical languages such as English where phonological processing plays a key role [Reference Wang, Wang, Xia, Liu, Quan and Tian81]. One study [Reference Wang, Wang, Xia, Liu, Quan and Tian81] that investigated orthography processes found significant deficits in orthography-phonology, but not in vocabulary when distinguishing real words from nonwords, in SZ compared to HC.
Affective disorders (depression, anxiety or mania)
Two studies [Reference Maj62,Reference Weiss, Francis, Senf, Heist and Hargraves66] assessed single-word reading in depression, both using the REALM [Reference Davis, Crouch, Long, Jackson, Bates and George64]. Of these, one study [Reference Maj62] showed a nonsignificant small deficit in people with depression (Hedge’s g = −0.30, df = 0, p = 0.37, CI = [−0.96, 0.36]) and, in the other study [Reference Weiss, Francis, Senf, Heist and Hargraves66], all participants performed at 7–8th grade reading level.
Bipolar disorder
The earlier-mentioned study on adolescents [Reference Reichenberg, Weiser, Rabinowitz, Caspi, Schmeidler and Mark47] had also assessed comprehension premorbidly in a group who later developed nonpsychotic bipolar disorder and found them to have no deficit in comparison to HC.
Personality disorders/psychopathy
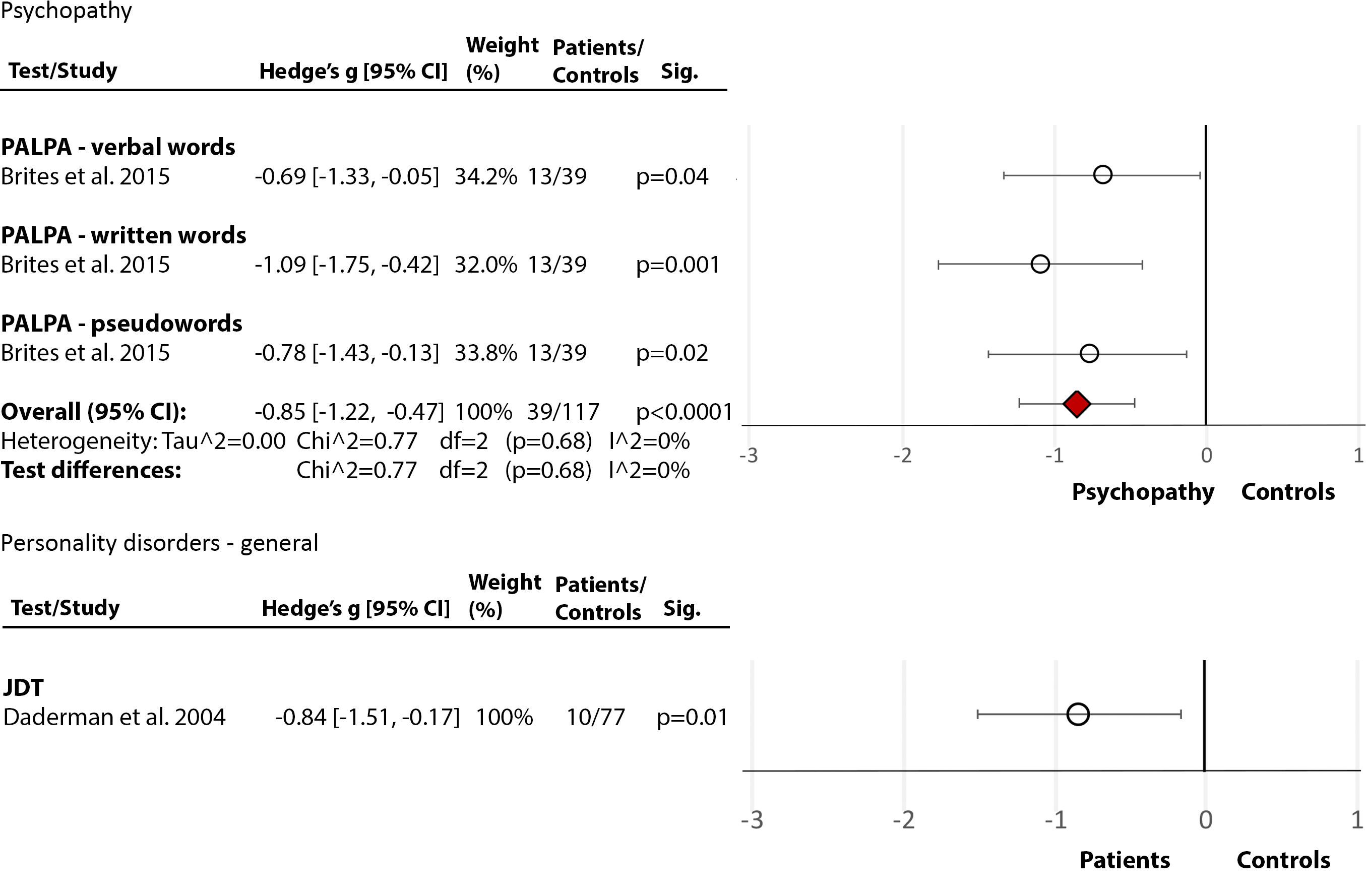
One study [Reference Brites, Ladera, Perea and García30] assessed phonological processing and comprehension, using the Portuguese version of the PALPA [Reference Castro, Caló and Gomes29], and showed medium-size deficits in both phonological processing (Hedge’s g = −0.55, df = 2, p = 0.004, CI = [−0.92, −0.18]) (Figure 3(3.1)) and comprehension (Hedge’s g = −0.47, df = 0, p = 0.05, CI = [−0.87, 0.39]) (Figure 3(3.2)) in people with diagnosed psychopathy (from community settings), compared with nonpsychopathic nonforensic controls.

3.1 Phonological processing and decoding.

3.2 Comprehension.
Figure 3. Reading deficits in community/nonforensic samples of people with psychopathy. Within each specific reading skill, the results are presented for each of the test(s)/measures used, followed by the analysis of differences between tests (last row). Negative values represent a poorer performance of people with personality disorder in comparison to healthy control.
Brites et al. [Reference Brites, Ladera, Perea and García30]. Abbreviations: PALPA, Psycholinguistic Assessments of Language Processing in Aphasia. White circle ![]() —effect size for a particular study determining the difference between patients and controls. Red diamond
—effect size for a particular study determining the difference between patients and controls. Red diamond ![]() —overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
—overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
General mental illnesses (nonspecified/mixed)
Two studies [Reference Berg and Hammitt51,Reference Ferron, Brunette, McGurk, Xie, Frounfelker and Cook58] assessed comprehension and single-word reading while the third study [Reference Christensen and Grace65] assessed single-word reading only. The first study [Reference Ferron, Brunette, McGurk, Xie, Frounfelker and Cook58] reported 9th-grade level comprehension as well as 9th-grade level single-word reading when assessed by WRAT-IV [Reference Robertson and Wilkinson88] in people with unspecific MIs. The second study [Reference Berg and Hammitt51], using the PIAT-comprehension subtest [Reference Dunn and Markwardt50], reported 7th-grade comprehension, despite 9–10th grade for single-word reading, in psychiatric patients (majority with alcoholism or nonorganic psychoses). In the third study [Reference Christensen and Grace65], 75% of the sample with MIs (mainly SZ and affective disorders) read below 7th grade when assessed by REALM [Reference Davis, Crouch, Long, Jackson, Bates and George64].
Summary of Deficits in Nonforensic Populations
Overall, SZ was associated with pronounced deficits in phonological processing, comprehension, reading rate, and fluency (Figure 4), with deficits also present in reading-related skills. These deficits appear to be present often from an early age, with reading skills of SZ adults remaining below their achieved education levels. The single-word reading and speed were less impacted. There were few data in affective disorders, and only for single-word reading, showing a mild/nonsignificant deficit. Individuals with PDs/high psychopathy showed mild deficits in both phonological processing and comprehension (Figure 4). Comprehension and single-word reading skills of people with unspecified MIs from nonforensic settings were at secondary school levels, which, although below the norm, were better than those in SZ (Figure 4).

Figure 4. Interpretation of observed reading deficits in included diagnoses.
No deficit = nonsignificant differences between patients and healthy control (HC); Very mild deficit = Hedge’s g up to −0.30 and/or mixed results with the majority of samples scoring within the norm; Mild deficit = Hedge’s g up to −0.50 and/or reading skill at 9–10th-grade level; Moderate deficit = Hedge’s g up to −0.75 and/or reading skill at 7–8th grade level; Severe deficit = Hedge’s g over −0.75 and/or reading skill below 7th grade level. This interpretation considers whether the results were consistent or mixed. Empty circle ![]() = Mixed evidence.
= Mixed evidence.
Reading Skills in Forensic Populations
Seven studies [Reference Daderman, Lindgren and Lidberg15,Reference Selenius and Strand26,Reference Svensson, Fälth and Persson27,Reference Brites, Ladera, Perea and García30,Reference Davidson, Espie, Lammie, D, E and Lammie68,Reference Dalby and Williams70,Reference Nestor71], all in PDs/psychopathy or general MIs, were found.
Personality disorders/psychopathy
Phonological Processing and Decoding: In the first study [Reference Brites, Ladera, Perea and García30], the PALPA [Reference Castro, Caló and Gomes29] phonological processing test showed a large deficit in the incarcerated group with diagnosed psychopathy relative to HC (Hedge’s g = −0.85, df = 2, p = 0.0001, CI = [−1.22, −0.47]) (Figure 5(5.1)). The second study [Reference Daderman, Lindgren and Lidberg15], using the JDT [Reference Jacobson25] to examine decoding, showed marked impairment (Hedge’s g = −0.84, df = 0, p = 0.01, CI = [−1.51, −0.17]) in people with nonspecific PDs (and comorbid MIs), relative to HC.
5.1. Phonological processing and decoding

5.2. Comprehension. Psychopathy.
Figure 5. Reading deficits in forensic patients with psychopathy or personality disorders. Within each specific reading skill, the results are presented for each of the test(s)/measures used, followed by the analysis of differences between tests (last row). Negative values represent a poorer performance of people with psychopathy or personality disorder in comparison to healthy control.
Brites et al. [Reference Brites, Ladera, Perea and García30]; Daderman et al. [Reference Daderman, Lindgren and Lidberg15]. Abbreviations: JDT, Jacobson’s Decoding Test; PALPA, Psycholinguistic Assessments of Language Processing in Aphasia. White circle ![]() —effect size for a particular study determining the difference between patients and controls. Red diamond
—effect size for a particular study determining the difference between patients and controls. Red diamond ![]() —overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
—overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
Comprehension: One study [Reference Brites, Ladera, Perea and García30] used the PALPA [Reference Castro, Caló and Gomes29] and showed a large deficit in comprehension in incarcerated people with diagnosed psychopathy, compared to HC (Hedge’s g = −0.95, df = 0, p = 0.0003, CI = [−1.48, −0.43]) (Figure 5(5.2)). The other study [Reference Daderman, Lindgren and Lidberg15] used a Swedish prose text [Reference Madison55] and found no deficit in PDs.
Single-word Reading: The first study [Reference Daderman, Lindgren and Lidberg15] used a Swedish single-word reading test [Reference Madison28] and found significant impairment in PD inmates with comorbid MI and dyslexia, as well as in dyslexic inmates, in comparison to inmates without a PD diagnosis. In the second study [Reference Brites, Ladera, Perea and García30], a diagnosis of psychopathy did not influence single-word reading as assessed by PALPA [Reference Castro, Caló and Gomes29]. The third study [Reference Davidson, Espie, Lammie, D, E and Lammie68] found literacy scores, as assessed by the TOWRE [Reference Torgesen, Wagner and Rashotte67], to be below the norm in PD. None of these studies [Reference Daderman, Lindgren and Lidberg15,Reference Brites, Ladera, Perea and García30,Reference Davidson, Espie, Lammie, D, E and Lammie68] provided data for effect size calculation.
Rate, Speed, Accuracy, and Fluency: Only one study [Reference Daderman, Lindgren and Lidberg15] was found, showing that reading speed was negatively affected in 7 of 10 forensic PD participants, especially in those with comorbid dyslexia.
Reading-related skills
One study [Reference Daderman, Lindgren and Lidberg15] showed that spelling was poorer in inmates with PD and dyslexia, as opposed to those with no comorbidities.
General mental illnesses (nonspecified/mixed)
Phonological Processing and Decoding: One study [Reference Svensson, Fälth and Persson27] used the JDT–Wordchains [Reference Jacobson25], the Word Attack test [Reference Svensson and Jacobson89], and Phonological Choice [Reference Olofsson31], and revealed severely impaired phonological skills (below the 6th grade) in people with various MIs. The second study [Reference Selenius and Strand26] examined correlations between psychopathic traits and phonological and decoding skills in forensic psychiatric patients, assessed with the “Pidgeon” test [Reference Lundberg and Wolff34], the MWDT [Reference Madison28], and the JDT [Reference Jacobson25], and found positive correlations between the superficial item of the Psychopathy Checklist: Screening Version (PCL:SV) [Reference Hart, Cox and Hare90] and phonological processing and decoding of sentences (but not words). However, as the study did not include HCs or test normative scores, the findings are difficult to understand in terms of quantifying the deficit.
Comprehension: In one study [Reference Svensson, Fälth and Persson27] that used the Oral Close subtest of the WRMT-R [Reference Woodcock37], comprehension in inmates with MI was below 4th grade in 23% of Swedish native and in over 50% of non-native speakers. In another study [Reference Selenius and Strand26] that used a silent paragraph reading test [Reference Madison56], no significant correlations between psychopathic traits and comprehension scores in people with nonspecified MIs were found.
Single-word Reading: There were two studies [Reference Dalby and Williams70,Reference Nestor71], both using the WRAT [Reference Jastak and Jastak69]. The first study [Reference Dalby and Williams70] assessed people with various diagnoses (psychosis, mania, alcoholism, and ASPD). It found no significant differences between HC and psychosis (Hedge’s g = 1.42, df = 0, p = 0.68, CI = [−5.40, 8.24]), mania (Hedge’s g = 0.53, df = 0, p = 0.13, CI = [−0.15, 1.20]), or alcohol abuse (Hedge’s g = −0.49, df = 0, p = 0.10, CI = [−1.06, 0.09]) but single-word reading was significantly impaired in ASPD (Hedge’s g = −1.01, df = 0, p = 0.004, CI = [−1.69, −0.33]. The second study [Reference Nestor71] found age-moderated differences in people with MIs and a history of violence, with people aged above 45 years scoring significantly better than those below 20 years.
Rate, Speed, Accuracy, and Fluency: One earlier-described study [Reference Selenius and Strand26] found that, within those with MIs, reading speed [Reference Madison56] was positively correlated with affective and interpersonal traits (Factor 1, PCL:SV [Reference Hart, Cox and Hare90]).
Reading-related skills
In a study [Reference Selenius and Strand26] involving Swedish inmates with MIs, neither spelling nor vocabulary scores significantly correlated with psychopathic traits.
Summary of Deficits in Forensic Populations
Overall, there was evidence of severe impairment in phonological processing and decoding in forensic populations with PDs/psychopathy (Figures 4 and 5), similar to that seen in SZ. There was also evidence of deficits in comprehension, single-word reading, and speed in this population (Figures 4 and 5). Studies on forensic patients with various MIs yielded mixed findings although one study [Reference Svensson, Fälth and Persson27] that examined inmates did show phonological processing and comprehension to be well below the norm.
Nonforensic versus Forensic Populations: Direct Comparison
Only one study [Reference Brites, Ladera, Perea and García30] directly compared forensic and nonforensic groups. It used PALPA [Reference Castro, Caló and Gomes29] and revealed a significant medium-size deficit in incarcerated individuals with psychopathy compared to nonincarcerated (community) sample with psychopathy in phonological processing and decoding (Hedge’s g = −0.49, df = 2, p = 0.03, CI = [−0.94, −0.04] (Figure 6(6.1)), and a large deficit in comprehension (Hedge’s g = −0.85, df = 1, p = 0.003, CI = [−1.43, −0.28]) (Figure 6(6.2)). These results support the findings from individual studies indicating severe reading deficits in incarcerated individuals with MI.

6.1 Phonological processing and decoding.

6.2 Comprehension.
Figure 6. Reading deficits in incarcerated vs community samples of people with a diagnosis of psychopathy. Within each specific reading skill, the results are presented for each of the test(s)/measures used, followed by the analysis of differences between tests (last row). Negative values represent a poorer performance of the forensic sample, compared to the nonforensic sample.
Brites et al. [Reference Brites, Ladera, Perea and García30]. Abbreviations: PALPA, Psycholinguistic Assessments of Language Processing in Aphasia. White circle ![]() —effect size for a particular study determining the difference between patients and controls. Red diamond
—effect size for a particular study determining the difference between patients and controls. Red diamond ![]() —overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
—overall effect size for diagnosis for a certain reading skill (e.g., comprehension) including all partial effect sizes.
Reading Skills Deficits in Mental Illness: Influencing Factors
Symptoms and medication
Of six studies in SZ [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Arnott, Sali and Copland24,Reference Nelson, Combs, Penn and Basso72,Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76,Reference Wang, Wang, Xia, Liu, Quan and Tian81] that examined the relationship between psychotic symptoms and reading skills, three [Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Arnott, Sali and Copland24,Reference Wang, Wang, Xia, Liu, Quan and Tian81] found a negative influence of positive and negative symptoms on phonological processing, comprehension, and orthography; and hallucinations negatively affected reading efficiency and speed in one study [Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76]. Five studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22,Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41,Reference Puente, Rodenbough and Orrell63,Reference Whitford, O’Driscoll, Pack, Joober, Malla and Titone85] examined the effect of antipsychotic dose as chlorpromazine equivalents; four [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22,Reference Puente, Rodenbough and Orrell63,Reference Whitford, O’Driscoll, Pack, Joober, Malla and Titone85] found no relationship with single-word reading, phonological processing, or comprehension, and one [Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41] found a negative influence of high dosage on fluency and comprehension. No significant association occurred between depressive symptoms and single-word reading [Reference Weiss, Francis, Senf, Heist and Hargraves66].
Cognitive function
Six studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41,Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44,Reference Hayes and O’Grady54,Reference Dalby and Williams70] examined the relationship between reading skills and general cognition in SZ. Verbal IQ significantly correlated with comprehension and vocabulary [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44]. Lower premorbid IQ (single-word reading) predicted reading comprehension [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Hayes and O’Grady54]. However, general IQ did not significantly predict any of the reading skills [Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41]. Similarly, working memory did not correlate with comprehension or reading rate in SZ and HC [Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21]. In forensic populations, full-scale IQ was significantly lower than single-word reading in individuals with SZ and bipolar disorder [Reference Dalby and Williams70]. These results suggest that general verbal skills may influence comprehension but no marked impact of other cognitive abilities was found.
Education
In SZ, three studies [Reference Revheim, Corcoran, Dias, Hellmann, Martinez and Butler17,Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21,Reference Martínez, Revheim, Butler, Guilfoyle, Dias and Javitt41] examined the influence of education and all found reading skills significantly below achieved academic levels. Six studies [Reference Dondé, Martinez, Sehatpour, Patel, Kraut and Kantrowitz18,Reference Arnott, Sali and Copland24,Reference Gavilán and García-Albea39,Reference Maj62,Reference Curzietti, Chaillou, Bonnefond, Vidailhet and Doignon-Camus76,Reference Wang, Wang, Xia, Liu, Quan and Tian81] matched their groups on education or entered it as a covariate [Reference Whitford, O’Driscoll, Pack, Joober, Malla and Titone85], and all found significant impairments in various reading skills. Nonforensic populations with general MIs had single-word reading equivalent to their achieved education but their comprehension was lower [Reference Berg and Hammitt51]. Forensic PD also had comprehension below their education level [Reference Daderman, Lindgren and Lidberg15].
Discussion
This systematic review and meta-analysis evaluated existing evidence to identify the type and degree of reading impairments in different MIs, the reading assessment tools that might most consistently detect them, and possible differences in the pattern of reading skills deficits in people with different MIs in forensic and nonforensic settings. Most of the reviewed studies (27/34) included people with SZ. There were seven studies of reading skills deficits in people with different MIs (PD or general MI) in forensic settings. Our findings are discussed below.
Effect of diagnosis in nonforensic samples
We observed significant deficits in multiple reading skills in SZ, resembling the pattern typically seen in dyslexia [Reference Lyon, Shaywitz and Shaywitz6], and consistent with previous evidence for shared genetic and psychophysiological traits in SZ and dyslexia [Reference Whitford, O’Driscoll and Titone7]. In our meta-analysis, both phonological processing and comprehension were greatly impaired. These impairments may be associated with ineffective use of contextual information [Reference Niznikiewicz, Friedman, Shenton, Voglmaier, Nestor and Frumin91] and contribute to poor speech in SZ, especially in close association with thought disorder [Reference Corcoran, Mittal, Bearden, Gur, Hitczenko and Bilgrami92]. Reading rate was low but the deficit in reading accuracy was lower. This indicates relatively preserved single-word reading skills, most likely because they are usually acquired before illness onset and remain intact [Reference Reichenberg, Weiser, Rabinowitz, Caspi, Schmeidler and Mark47]. In contrast, there was evidence for impairments in vocabulary and spelling, presumably as a result of disrupted scholastic experience. Disrupted scholastic experience during adolescence can affect complex skills such as comprehension [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44,Reference Ho, Andreasen, Nopoulos, Fuller, Arndt and Cadoret45,Reference Reichenberg, Weiser, Rabinowitz, Caspi, Schmeidler and Mark47], which could precipitate difficulties with processing complex written information in SZ. People with SZ showed reading skills well below their achieved education level (see Education). Reading skills deficits in SZ also do not seem to be explained by other aspects of cognition (see Cognitive Function) although more comprehensive investigations are needed to substantiate this. Our findings (Symptoms and Medication) further indicated that while symptoms and high antipsychotic doses may worsen reading skills, they do not fully explain the profile of reading skills deficits in SZ. Impairment in comprehension and vocabulary was present even before the onset of symptoms [Reference Fuller, Nopoulos, Arndt, O’Leary, Ho and Andreasen44,Reference Ho, Andreasen, Nopoulos, Fuller, Arndt and Cadoret45] together with deficient phonological processing, which has been related to disrupted visual processing in SZ since early age [Reference Revheim, Butler, Schechter, Jalbrzikowski, Silipo and Javitt21]. The symptoms can, however, aggravate deficits in reading skills, such as comprehension, which are acquired with experience, and also depend on the earlier acquired skills [Reference Cunningham and Stanovich93]. Recent data [Reference de Boer, Voppel, Brederoo, Wijnen and Sommer94] suggest that some aspects of language production (e.g., slower articulation) that can affect reading skills assessments are particularly sensitive to dopamine-D2 receptor blocking antipsychotics. Furthermore, most studies in SZ included more men than women or men solely and also included people with schizoaffective disorder. Further studies need to comprehensively examine specific reading skills in both men and women with schizophrenia and schizoaffective disorder (separately) while taking medication, symptoms, cognition, education, and socioeconomic status into account.
Unlike in SZ and psychosis [Reference Berg and Hammitt51,Reference Ferron, Brunette, McGurk, Xie, Frounfelker and Cook58,Reference Christensen and Grace65], nonpsychotic bipolar disorder, and affective disorders, seemed to have comprehension and single-word reading skills comparable to HC [Reference Brites, Ladera, Perea and García30,Reference Reichenberg, Weiser, Rabinowitz, Caspi, Schmeidler and Mark47]. Although not all studies specified the type of PD, it seems that reading skill deficits may not be as prominent in nonforensic psychopathy as in SZ.
Effect of diagnosis in forensic samples
Our findings suggest only a weak or no deficit in nonforensic psychopathy but indicate a marked phonological processing and comprehension deficit in the incarcerated group. It is possible that PD/psychopathic individuals with good phonological processing and comprehension are more able to evade incarceration [Reference Brites, Ladera, Perea and García30,Reference Timor and Weiss95]. Nonetheless, marked reading deficits in the incarcerated group may have contributed to their poor adjustment within the community [Reference Svensson, Fälth and Persson27], which, in turn, increased the risk of incarceration. Men with MIs within forensic settings had significantly lower general reading abilities and spelling than women with MIs [Reference Svensson, Fälth and Persson27], consistent with the pattern seen in healthy samples [Reference Walder, Seidman, Cullen, Su, Tsuang and Goldstein22].
Clinical implications
Comprehension has a significant influence on decision-making capacity in SZ [Reference Palmer and Jeste96], and this is likely to be true also for people with other MIs, especially within forensic populations. Dyslexia is often underdiagnosed in people with MIs, and this might explain their inability to complete higher education and obtain jobs [Reference Daderman, Lindgren and Lidberg15], or the expression of socially unacceptable behaviors [Reference Svensson, Fälth and Persson27]. Furthermore, progression and engagement in therapeutic activities within mental health services often depend on good reading and language skills. This highlights a need to accurately identify reading deficits and develop specific programs to improve reading skills of people in psychiatric services. It may be possible to target reading deficits in SZ and other MIs by building on the less affected aspects, such as lexical knowledge (access to words) [Reference Tan, Yelland and Rossell97,Reference Moro, Bambini, Bosia, Anselmetti, Riccaboni and Cappa98], and access to familiar information that can compensate for some of the reading deficits [Reference Fernández, Guinjoan, Sapognikoff, Orozco, Agamennoni and Fernandez99], while implementing interventions to ameliorate reading skills [Reference Snowling100].
Effect of assessments
Significant between-test differences were found only in tests detecting deficits in comprehension, accuracy, and rate in SZ. In comprehension and rate, the NDRT and GORT-4, and in accuracy, the GORT solely, consistently detected large deficits while the Alouette (French) test detected no deficits (Figure 2). It is conceivable that certain deficits emerge more often/strongly in English compared to some other languages, as is the case in developmental dyslexia [Reference Ziegler, Perry, Ma-Wyatt, Ladner and Schulte-Körne101]. This possibility requires further study.
Conclusions
Our findings demonstrate pronounced deficits in phonological processing and comprehension in SZ and forensic PD/psychopathy. Reading skills in people with other MIs in nonforensic settings seem relatively unaffected. Among the tests, only the NDRT and GORT detected significantly stronger deficits in SZ than other measures. Considering the importance of good reading skills in everyday life, as well as for the clinical success of mental health services, there is a clear need to identify methods that can improve reading in SZ and forensic PD populations. These interventions could potentially build on relatively spared aspects of reading by implementing approaches already effective in dyslexia.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors. Martina Vanova and Luke Aldridge-Waddon are supported by Brunel University London College of Health, Medicine and Life Sciences Doctoral Scholarships.
Conflict of Interest
The authors report no conflicts of interest.
Data Availability Statement
All data supporting the meta-analysis reported in this article are available from Brunel University London research repository at 10.17633/rd.brunel.13123334.



















 Open access
Open access
Comments
No Comments have been published for this article.