


1. Introduction
Schizophrenia is a serious psychiatric disorder with a heterogeneous genetic and neurobiological background that alters early brain development and maturation, ultimately affecting information processing, motivation and cognition Reference Kahn, Sommer, Murray, Meyer-Lindenberg, Weinberger and Cannon[1]. The neurodevelopmental model posits that the phenomenological diagnosis of schizophrenia based on the expression of hallucinations, delusions and disorganization typically around late adolescence-early adulthood, is the end stage of abnormal neurodevelopmental processes that began years before Reference Rapoport, Giedd and Gogtay[2]. Stable epidemiological risk factors for schizophrenia, such as being winter-born Reference Davies, Welham, Chant, Torrey and McGrath[3], urbanicity Reference van Os, Kenis and Rutten[4] and immigration Reference Bourque, van der Ven and Malla[5] have been identified, with the vast majority of this research focusing on adult psychosis. Yet, urban residency from birth to adolescence, rather than during adulthood, appears to be more strongly associated with adult psychosis Reference Pedersen and Mortensen[6–Reference Mortensen, Pedersen and Westergaard8]] and it is the post-migratory family-social context interactions rather than pre- or peri-migrational factors that mediate the risk for psychosis Reference Bourque, van der Ven and Malla[5]. Consistent with the neurodevelopmental model of schizophrenia, the above suggest that the processes leading from urban exposure or immigration to psychosis begin in adolescence, childhood or earlier.
Schizotypy is a subclinical construct tapping normative dispositions toward characteristics that are associated with schizophrenia Reference Mason Claridge[9] and indeed, elevated schizotypy is considered a potential precursor to schizophrenia-spectrum disorders. Although longitudinal studies support the dimensional nature of psychosis and risk Reference Rapoport, Giedd and Gogtay[2] and despite the considerable interest in the pathogenesis of schizotypy in recent years, there are no studies examining the degree to which the aforementioned epidemiological risk factors for schizophrenia hold for schizotypy. There are no studies on urban exposure and immigration effects on adult or adolescence schizotypy and the few reports of winter-birth effects on schizotypy have yielded mixed results Reference Konrath, Beckius and Tran[10, Reference Córdova-Palomera, Calati, Arias, Ibáñez, Moya and Ortet11]] although the study of Konrath et al. Reference Konrath, Beckius and Tran[10] confirmed an effect using a very large sample of the adult population.
For the reasons described above, examination of season of birth, urbanicity and immigration on schizotypy in late adolescence is a key area of psychosis research given that:
around 10% of the general population presents with increased schizotypy Reference Lenzenweger, Rawlings, Williams, Haslam and Claridge[12] that increases their risk for developing schizophrenia-spectrum disorders Reference Debbané and Barrantes-Vidal[13];
adolescence is the critical period when positive schizotypy reaches a peak Reference Fonseca-Pedrero, Paíno, Lemos-Giráldez, García-Cueto, Campillo-Álvarez and Villazón-García[14, Reference Bora and BaysanArabaci15]] and positive schizophrenia symptoms typically begin;
over two-thirds of the world's population are predicted to live in cities by 2050 Reference Lederbogen, Kirsch and Haddad[16];
the immigrant population worldwide has been growing rapidly over the past fifteen years with an average 2% per year, reaching 244 million in 2015 [17].
In this study, we examined for the first time the association of season of birth, urbanicity and immigrant status with schizotypy, in nonclinical individuals in their late adolescence, controlling for a range of potentially confounding factors. We focused on positive rather than negative schizotypy, because the former taps to the “psychosis” syndrome that is unequivocally shared across genders and diagnoses of both affective and non-affective psychotic illness; psychosis also constitutes the cornerstone for the allocation of a diagnosis of schizophrenia, upon which most winter-birth, urbanicity and migration research was based Reference Davies, Welham, Chant, Torrey and McGrath[3–Reference Bourque, van der Ven and Malla5]].
2. Materials and methods
2.1. Study design and participants
The sample consisted of 500 adolescent pupils (n=500) from the last two high school years (90%) or the first year of the Technological high school (10%), from 17 urban schools from nine municipalities, which were counterbalanced for urbanicity (inhabitants/km2) and Migrant Density Index (MDI), defined as the ratio of total number of immigrants/total inhabitants. Specifically, we choose 4 schools from Heraklion Crete and 5 schools from 4 municipalities of Attica Prefecture with low MDI (0,5–2,5%), and 8 schools from 4 municipalities of Attica with high MDI (5,3–9,6%).
The final sample with complete valid questionnaires was n=445 (192 men), born between 1990 and 1995 [age mean (SD): 18 (1.1), range: 17–22]. Of those, 287 were of Greek origin, 121 were of Albanian origin and 37 pupils came from other ethnic groups. Most non-Greek pupils were first generation Albanian immigrants who migrated in the country in their preschool years (1st/2nd generation: 124/34, Albanian/other ethnicities: 121/37). Descriptive characteristics from the sample are presented in Table 1. The study was approved by the University of Crete Ethics Committee and the Ministry of Education. Following contact with high schools administration and a presentation of the study's aims and procedures to staff and pupils, all pupils were given a written informed consent to be signed by themselves and their parents, prior to their participation to the study.
Table 1 Descriptive characteristics of study participants (n=445).

2.2. Questionnaires
The main outcome of the study was schizotypal personality traits as measured with the Schizotypal Traits Questionnaire (STQ) Reference Claridge and Broks[18]. This is a 37-item self-report questionnaire derived from the criteria for schizotypal personality disorder in the diagnostic and statistical manual of mental disorders (DSM-IV). It has been extensively used in adult, adolescent and children populations, with excellent face and predictive validity and test-retest reliability Reference Cyhlarova and Claridge[19] and is thought to provide the best measure of the underlying positive schizotypy dimension. Responses to each item have a dichotomous (yes/no) format. A total schizotypy and three subscale scores [“magical thinking”, “paranoid ideation” and “unusual perceptual experiences”] are derived by adding the positive answers. Higher scores indicate higher positive schizotypy.
Participants also completed the following personality questionnaires: Revised Eysenck Personality Questionnaire (EPQ-R) Reference Eysenck and Eysenck[20], Cloninger's Temperament and Character Inventory (TCI) Reference Cloninger, Svrakic and Przybeck[21], Spielberger's State-Trait Anxiety Inventory—Trait Scale (STAI-T) Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs[22] and Carver and White's Behavioural Inhibition/Behavioural Activation System (BIS/BAS) questionnaire Reference Carver and White[23]. Additionally, participants completed a modified version of the Health Behavior in School-aged Children (HBSC) [24] World Health Organization questionnaire which refers anonymously to their socio-demographic characteristics, health habits, and other important life-style parameters, family and school circumstances. A detailed description of all the above scales is included in the Supplementary Data.
2.3. Pre-analysis data reduction and processing
Prior analysis included a data reduction and variables classification procedure. The HSBC questionnaire data were subjected to principal component analysis (PCA), which reduces the data by forming linear combinations of the original observed variables, thereby grouping together correlated variables; this, in turn identifies any underlying dimensions in the data. Nonlinear principal components analysis with CATPCA was performed. For categorical variables, CATPCA uses a scaling process, which transforms categories into numerical values, while the variance accounted for is maximized Reference Linting and Van der Kooij[25]. Varimax rotation and the score-loadings were used to extract the standardized components using a regression-based method. The number of components that best represented the data was chosen on the basis of the scree plots and the Eigen values of the principal components, as well as the interpretability of the factor loadings. The extracted components, accounting for 72% of total variance, were:
drug use (times used cannabis, age of onset cannabis);
school cohesion (cohesion, solidarity and acceptance from schoolmates);
quality of life (QoL) & family relations (satisfaction from family relations scale, number of first degree relatives with history of mental illness, quality of life scale);
academic performance (teacher's opinion of academic performance, last year's academic performance) (Supplementary Table 1).
Parallel analysis with 1000 datasets was applied for the number of extracted components, which verified that exactly four components were above the 95th percentile Reference O’Connor[26].
The same procedure was followed for personality traits derived from subscales of the EPQ-R, TCI, STAI-T and BAS questionnaires. Bartlett's test of Sphericity (P<0.001), the Kaiser-Meyer-Olkin measure (KMO=0.677) and the correlation-matrix Determinant (determinant=0.059,) supported sampling adequacy for PCA. The resulting PCA factor dimensions, accounting for 73% of total variance, were:
anxiety/neuroticism (STAI-trait anxiety, EPQ-neuroticism, TCI-self directedness);
sensitivity to reward (BAS-Drive, BAS-reward responsiveness);
openness to experience (TCI-novelty seeking, EPQ-extraversion, BAS-fun seeking);
agreeableness (TCI-reward dependence, TCI-cooperativeness) (Supplementary Table 2).
Parallel analysis with 1000 datasets was again applied to check the number of extracted components, resulting at three components above the 95th percentile.
2.4. Selection of covariates
Independent variables of a priori interest include:
individual characteristics, such as sex, season of birth [May to Nov vs. Dec to Apr (winter-births)];
immigrant status (Greek/Non Greek);
family history of mental illness (yes/no), family financial status (bad/average/good);
area of living, such as urbanicity (<5000, 5000–10,000, 10,001–50,000, >50,000 inhabitants/km2) and MDI (low, high).
Standardized scores of the four life-style factor dimensions derived from PCA of the HSBC and standardized scores of the four personality dimensions derived from PCA of the personality questionnaires were also included in the analyses.
2.5. Data analysis
Descriptive analyses were performed for individual characteristics of participants. Normality of dependent variables was tested using appropriate statistics and by visual inspection of corresponding histograms. Bivariate associations between categorical independent and continuous dependent variables were studied using t-tests for independent samples or ANOVA. Bivariate associations between categorical independent and dependent variables were studied using Pearson's Chi-square test. Pearson's correlation coefficient was used to estimate the strength of the association between two continuous variables.
Separate multivariate linear regression models were implemented to estimate the associations of schizotypy traits (magical thinking, paranoid ideation and unusual experiences) and participant characteristics. Byproduct interaction terms of sex were introduced in the models, which revealed significant heterogeneity in associations (data not shown). Therefore, separate multivariate models were built for adolescent men and women participants by stratifying the sample. In order to assess the improvement of the models by adding more variables in the regression process, we applied hierarchical regression using the enter method. That is, blocks of variables were entered in three steps:
individual demographic characteristics with a priori interest, such as season of birth, immigrant status, area of living (population density and migration index), family financial status and family history of mental illness;
life-style factors from the PCA of the HBSC questionnaire;
personality dimensions from the PCA of the personality traits questionnaires.
R 2 change is an indicator of the improvement of the model and significance of F-change is reported. Estimated associations are described in terms of β-coefficients (beta) and their 95% confidence intervals (CI). The Benjaminni–Hochberg procedure was performed in order to control for multiple hypotheses testing, setting false discovery rate at 0.25. Results that survived the Benjaminni–Hochberg procedure were considered significant, while results with a p<0.05 are also shown as ‘suggested findings’ for future replication attempts. All statistical analyses were performed using SPSS Software (IBM, USA).
3. Results
As shown in Table 1, adolescent women scored significantly higher in all schizotypy traits, reported significantly less satisfaction from family relationships and more frequently a positive family history of mental illness, while they were living more frequently in less urbanized areas, compared to adolescent men.
Tables 2–4 show the association of schizotypal dimensions with individual, life-style and personality characteristics in adolescent men. Magical thinking (Table 2) was significantly predicted by winter-birth and high anxiety/neuroticism in the fully adjusted model but only the latter survived correction for multiple testing. Paranoid ideation (Table 3) was predicted by winter-birth and a personality profile of high anxiety/neuroticism and reduced agreeableness in the fully adjusted model. Immigrant status, reduced school cohesion and quality of life-family relationships were significant before entering personality traits in the model. Unusual experiences (Table 4) were predicted by immigrant status and high anxiety/neuroticism in the fully adjusted model. Total schizotypy in the fully adjusted model in males was predicted by winter-birth, a personality profile of high neuroticism and reduced agreeableness and we observed trends for positive family history of mental illness; immigrant status was significant before entering personality in the model (Supplementary Table 3).
Table 2 Associations of individual characteristics, personal factors, and personality traits with STQ- Magical Thinking subscale for male pupils.
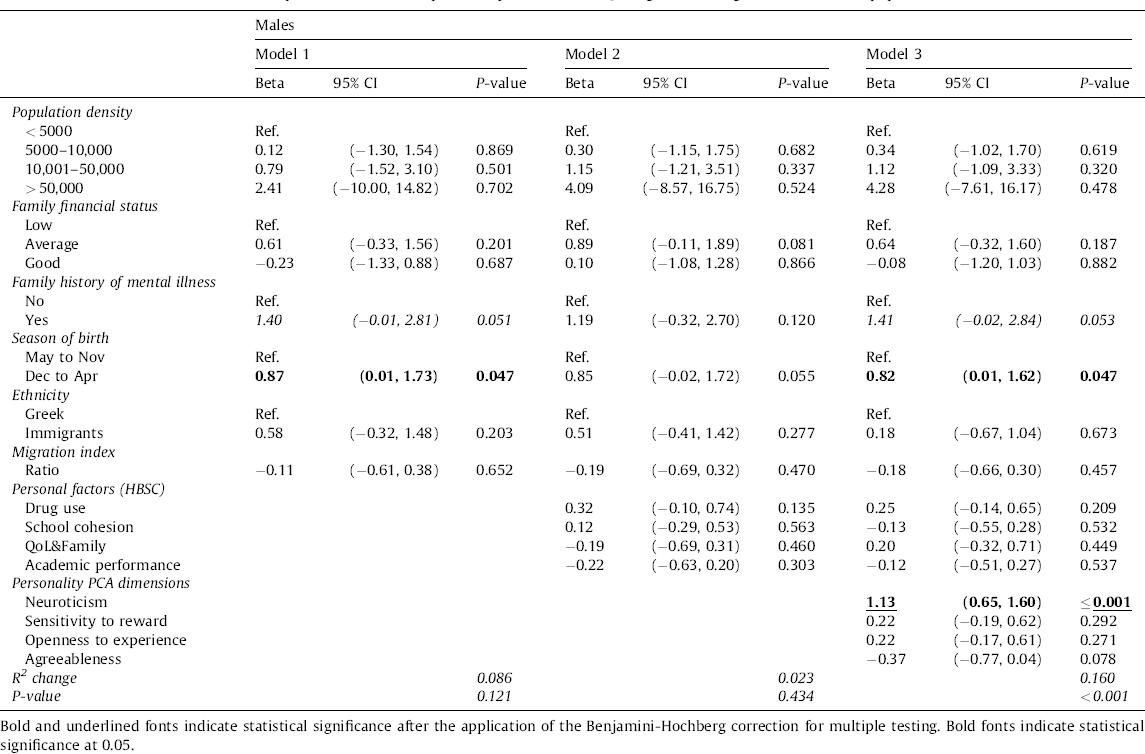
Table 3 Associations of individual characteristics, personal factors, and personality traits with STQ-Paranoid Ideation subscale for male pupils.
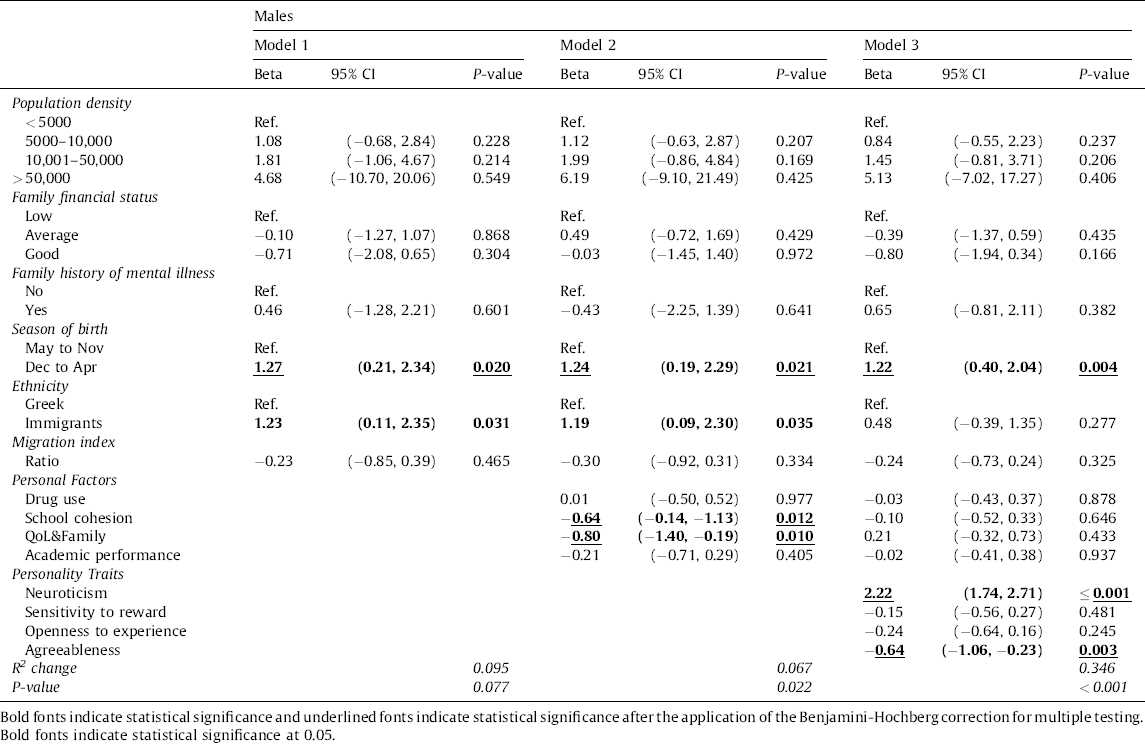
Table 4 Associations of individual characteristics, personal factors, and personality traits with STQ-Unusual Experiences subscale for male pupils.

Tables 5–7 show the predictors of schizotypal dimensions in adolescent women. Magical thinking (Table 5) in the fully adjusted model was significantly predicted by living in urban areas, high anxiety/neuroticism, sensitivity to reward and openness to experience. Paranoid ideation (Table 6) was associated with reduced school cohesion, QoL&Family relations and academic performance; however, these did not survive in the fully adjusted model where high anxiety/neuroticism and reduced agreeableness emerged as the only significant predictors. Unusual experiences were predicted by living in more urban areas, positive family history of mental illness and increased QoL&Family relations, even though above the boundary of multiple correction. Increased anxiety/neuroticism and openness to experience were the only significant predictors in the fully adjusted model (Table 7). Total schizotypy in the fully adjusted model was predicted by living in more urban areas and a personality profile of high anxiety/neuroticism, and sensitivity to reward while positive family history of mental illness just missed criterion (Supplementary Table 4). Multiplicative interaction terms of significant predictors and sex were introduced to fully adjusted models in order to examine the sex differences in the previously described analyses. In the fully adjusted models of total schizotypy, sex was found to interact significantly with season of birth (P=0.033), family relations (P=0.031) and a personality profile of high anxiety/neuroticism (P=0.011). Ethnicity and family relations’ interactions with sex were also significant in unusual experiences models (P=0.018 and P=0.039, respectively). For magical thinking and paranoid ideation, significant sex interactions were found with a personality profile of high anxiety/neuroticism and season of birth (P=0.019 and P=0.013 respectively).
Table 5 Associations of individual characteristics, personal factors, and personality traits with STQ-Magical Thinking subscale for female pupils.

Table 6 Associations of individual characteristics, personal factors, and personality traits with STQ-Paranoid Ideation subscale for female pupils.

Table 7 Associations of individual characteristics, personal factors, and personality traits with STQ-Unusual Experiences subscale for female pupils.

4. Discussion
This is the first report that examined the relationship of winter-birth, urbanicity and immigrant status, with positive schizotypy in late adolescence. We found that adolescent women scored higher than adolescent men in all positive schizotypy dimensions replicating previous findings in this age group Reference Fonseca-Pedrero, Paíno, Lemos-Giráldez, García-Cueto, Campillo-Álvarez and Villazón-García[14, Reference Bora and BaysanArabaci15, Reference Raine27, Reference Rawlings and Goldberg28] but also in adults Reference Bentall, Claridge and Slade[29, Reference Venables and Bailes30]] and children Reference Cyhlarova and Claridge[19]. Interestingly, we found sex-specific patterns of relationships between the risk factors of interest and positive schizotypy dimensions. In adolescent men, winter-birth predicted paranoid ideation and total schizotypy, while immigrant status was more relevant to unusual experiences. In adolescent women, urbanicity was the main predictor for magical thinking, unusual experiences and total schizotypy. We controlled for a range of potential and established confounding factors, including family history of mental illness, low SES, drug use, reduced subjective quality of life, school and family relations, objective academic performance and the strong influence of personality traits. Therefore, while these associations need replication, they seem robust and, given the potential for over-adjustment in our models, they should be regarded as conservative in the least. Moreover, meaningful associations between schizotypy and other personality traits increase confidence that the reported associations above were not spurious findings.
Only a handful of studies have examined the relationship between winter-birth and adult psychometric schizotypy, with mixed results, which did not generate a signal in a meta-analysis Reference Córdova-Palomera, Calati, Arias, Ibáñez, Moya and Ortet[11]. The most likely reason was the strong influence of age on schizotypy Reference Mata, Marguerat and Bahler[31], which, in the small sample sizes used in those studies, rendered practically undetectable the small effect of winter-birth Reference Córdova-Palomera, Calati, Arias, Ibáñez, Moya and Ortet[11]. Winter-birth effects require either very large adult samples Reference Konrath, Beckius and Tran[10] or they can be more readily revealed in younger-aged samples Reference Córdova-Palomera, Calati, Arias, Ibáñez, Moya and Ortet[11], as we confirmed in the present sample of 17–18 year old adolescents. There are no previous studies on the relationship between urbanicity or immigrant status and psychometric schizotypy in adult or younger age samples. Meta-analyses of adult studies show a consistent association of psychosis risk and urbanicity in a dose–response manner in many settings Reference van Os, Kenis and Rutten[4] after controlling for a range of possible confounders, such as urban drift and minority status Reference March, Hatch, Morgan, Kirkbride, Bresnahan and Fearon[32], suggesting aetiological underpinnings. However, the factors driving the association remains unknown with speculations for a non-specific stress processing factor Reference Lederbogen, Kirsch and Haddad[16], as mood and anxiety disorders are also elevated in the urban environment Reference Peen, Schoevers, Beekman and Dekker[33]. Here, we showed for the first time that urbanicity is important for the expression of positive schizotypy in adolescent women. The prediction of unusual perceptual experiences by immigrant status in adolescent men is interesting and could be mediated by childhood trauma and dissociation Reference Giesbrecht, Merckelbach, Kater and Sluis[34], both of which are highly prevalent among immigrants Reference Kang, Razzouk, Mari and Shirakawa[35, Reference Finklestein and Solomon36]], especially adolescents Reference Ratzoni, Ben Amo, Weizman, Weizman, Modai and Apter[37, Reference Finklestein38]], in various host societies and migrant populations. This relationship was limited to adolescent men only but this finding requires replication before we can conclude that it is gender specific.
These sex differences in the relationship between environmental risk factors and positive schizotypy suggest sex differences in thought and perception processes captured by the STQ in the critical stage of adolescence, which may resonate sex differences in illness trajectory and severity; indeed, female patients have a generally milder presentation and course than male patients and their positive symptoms are often comorbid or reinforced by the presence of affective symptoms but not the negative/deficit syndrome more typical of male schizophrenia Reference McGlashan and Bardenstein[39–Reference Mueser, Bellack, Morrison and Wade42]. Urbanicity may include social stressors of an affective nature Reference Lederbogen, Kirsch and Haddad[16, Reference Peen, Schoevers, Beekman and Dekker33, Reference Lederbogen, Haddad and Meyer-Lindenberg43] and we observe an analogy between the female-specific relationship between urbanicity and positive schizotypy in our study and the higher affective comorbidity and affective presentation of female schizophrenia patients Reference Goldstein and Link[40]. In contrast, the male-specific prediction of positive schizotypy by winter-birth (an early hit in the course of neurodevelopment) appears analogous to the earlier onset, more severe and less affective forms of schizophrenia seen in males and is consistent with evidence for:
greater vulnerability of the male brain to prenatal stress Reference Tavassoli, Saboory, Teshfam, Rasmi, Roshan-MilaniS and Ilkhanizadeh[44];
winter-birth, being a “second hit” that is related to expression of psychopathology onset in vulnerable individuals Reference Cohen and Najolia[45].
In both sexes, personality was the most significant predictor accounting for the greatest proportion of variance in all schizotypy subscales scores (range of additional variance explained by personality: 9.9-34.6%). High anxiety/neuroticism in particular was the single most consistent significant predictor for all schizotypal dimensions and total schizotypy score in both sexes. This is consistent with previously shown strong associations between neuroticism and positive schizotypy Reference Gooding, Davidson, Putnam and Tallent[46–Reference Ross, Lutz and Bailley51], suggestive of aetiological underpinnings [52–Reference Barrantes-Vidal, Ros-Morente and Kwapil55] with shared genetic etiology Reference Macare, Bates, Heath, Martin and Ettinger[56] and not solely a ‘secondary effect’ of schizophrenia-spectrum psychopathology. High openness to experience has also been repeatedly associated with positive schizotypy Reference Ross, Lutz and Bailley[51, Reference Barrantes-Vidal, Lewandowski and Kwapil57, Reference Asai, Sugimori, Bando and Tanno58] and its influence extends to the domain of perception Reference Kreitz, Schnuerch, Gibbons and Memmert[59]. It is interesting that, consistent with the latter, we confirmed this relationship for the “unusual experiences” and “magical thinking” schizotypy dimensions. This association was limited to the adolescent women but not the adolescent men of our study, possibly due to power and variance issues. High sensitivity to reward is implicated in bipolar spectrum affective psychoses Reference Depue and Iacono[60–Reference Urošević, Abramsona, Harmon-Jones and Alloy62]], normative development in adolescents Reference Urosevic, Collins, Muetzel and Luciana[63] and may be linked with cognitive control deficiencies during reward processing in affected adolescents Reference Urošević, Luciana, Jensen, Youngstrom and Thomas[64]. Given that women generally present with higher positive schizotypy and more affective symptoms than men and the multiple-level overlap between affective and non-affective psychoses, it may not be surprising that high sensitivity to reward predicted “magical thinking” in adolescent women. Reduced agreeableness, a construct related to a persons’ ability and desire to cooperate, adjust their behavior to a social context and reduce social conflict Reference Keller[65], also contributed meaningfully to the “paranoid ideation” dimension in both sexes confirming previous results Reference Tavassoli, Saboory, Teshfam, Rasmi, Roshan-MilaniS and Ilkhanizadeh[44, Reference Fridberg, Vollmer, O’Donnell and Skosnik66]]. Our results on personality predictors of late adolescence schizotypy confirm and extend previous findings in adults and fit with general evidence indicating that temperament and personality may reflect the vulnerability to particular types of pathological functioning Reference Barrantes, Colom, Claridge and Vieta[67]. Furthermore, they increase confidence in the results presented herein, implying that the reported associations could not be attributed to trivial phenotype assessment bias (i.e. self-ratings of schizotypal traits) or analytical errors that could have led to spurious associations.
Personal life-style factors explained small and non-significant amounts of variance with the exception of “paranoid ideation” where the additional variance explained was significant (men: 6.7%; women: 9.8%). Low reported school cohesion and subjective quality of life/family relations were the important predictors of paranoid ideation in both sexes confirming a putative role for social stressors/lack of support in the emergence of paranoia. However, the relationship was probably attributable to high neuroticism and reduced agreeableness as it did not survive in the fully adjusted model. In contrast, low “academic performance”, an objective measure and a proxy for cognitive ability, predicted paranoid ideation only in adolescent women but not men. This is reminiscent of previously noted dysjunctions between subjective and objective cognitive performance Reference Chun, Minor and Cohen[68] and subjective-objective quality of life and family relations Reference Cohen, Auster, MacAulay and McGovern[69] in high schizotypy college students, which altogether provide evidence for potential metacognition deficits in schizotypy Reference Kwapil, Brown, Silvia, Myin-Germeys and Barrantes-Vidal[70].
Limitations of our study include the use of self-reports and that our findings cannot generalize to other age bands or to other schizotypy dimensions e.g. negative or disorganized. Also, the study was not powered enough to test immigrant generation (1st vs. 2nd generation) or ethnicity effects, due to the majority being 1st generation immigrants of Albanian origin who migrated in the country in their preschool years.
5. Conclusions
It is necessary to systematically study nonclinical schizotypy in young populations, both as a dimension of normal personality and as a means of understanding developmental processes foreshadowing schizophrenia-spectrum disorders and possibly other serious mental illnesses. This will ultimately require longitudinal follow up of these traits from childhood through to adolescence to adulthood. Here, we present novel cross-sectional findings of shared environmental risk factors between adolescent schizotypy and schizophrenia, which support the continuum hypothesis and offer potential insights in the nature of risk conferred by winter-birth, urbanicity and immigration as well as the nature of important gender differences.
Funding
This work was supported by the University of Crete Research Account (ELKE 1348). The funding source had no involvement in the study design, the collection, analysis and interpretation of data, the writing of the report and in the decision to submit the article for publication.
Authors and contributors
PB and DM designed the study, PB obtained the funding, DM recruited the participants and collected the data, PB and TR designed the data analyses, TR carried out the analyses with contributions from DM, SG and PR. DM wrote the first draft of the manuscript under the supervision of PB, with other authors contributing to data interpretation and final manuscript preparation. DM and PB had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of data analysis. All authors take final responsibility for the decision to submit the manuscript for publication.
Disclosure of interest
The authors declare that they have no competing interest.
Acknowledgments
The authors wish to thank the participants for their help.
Appendix A Supplementary data
Supplementary data associated with this article can be found, in the online version, at doi:http://dx.doi.org/10.1016/j.eurpsy.2017.07.014.










Comments
No Comments have been published for this article.