



Background
The relationship between ethnicity and reproductive health outcomes has been contested. This is because the variations in youth sexual behaviours by ethnic affiliations may be confounded by factors such as socio-economic characteristic of the young adult and that of their community. In addition, religion and culture are usually seen as characteristics of ethnic groups which may also influence sexual behaviours. Therefore, this paper posits that it is important to consider the associations between the ethnic affiliations of young adults and their sexual behaviours. This is because studying the sexual behaviour of young adults with different ethnic backgrounds but similar individual characteristics may contribute to our understanding of how different ethnic affiliations influence youth sexual behaviours.
Nigeria is a diverse nation with more than 250 ethnic groups, but the Hausa, Igbo, and Yoruba are the three major ethnic groups, making up about 70% of the entire population (Okolie et al., Reference Okolie, Cisana, Schanfield, Adekoya, Oyedeji and Podini2018). The Hausa and Fulani make up a large percentage of the northern population, while the Yoruba and Igbo ethnic groups can be found in some parts of the South of Nigeria. There are documented differences in the traditions of these groups despite their socio-economic status (Adebowale, Reference Adebowale2019). For instance, school enrolment among girls and the use of modern contraceptives are higher in the southern part of Nigeria compared with the northern part of the country (National Population Commission ICF, 2019). In addition, the North consists largely of Muslims and is more patriarchal than the South dominated by Christians (Doctor et al., Reference Doctor, Findley, Ager, Cometto, Afenyadu, Adamu and Green2012).
Extant literature has also shown that youth belonging to each ethnic group have a distinct behavioural pattern that represents different levels of sexual risk in Nigeria (Odimegwu and Somefun, Reference Odimegwu and Somefun2017; Somefun and Olamijuwon, Reference Somefun and Olamijuwon2022). For instance, the most recent Nigerian demographic and health survey has shown a higher percentage of early childbearing among Hausa women compared with their Igbo and Yoruba counterparts (National Population Commission ICF, 2019). Similarly, results from a study conducted in Nigeria among young adults aged 15–24 revealed that Yoruba and Igbo male youth were more likely to use condoms at last sex and engage in multiple sexual partnerships compared with their Hausa counterparts (Odimegwu and Somefun, Reference Odimegwu and Somefun2017). Based on the noted differences among the three major ethnic groups, there is reason to believe that they may differ in sexual behaviours.
However, the majority of the existing studies on ethnicity and demographic outcomes in Nigeria have focused on fertility (Adebowale, Reference Adebowale2019), mortality (Adedini et al., Reference Adedini, Odimegwu, Imasiku and Ononokpono2015), and child marriage (Mobolaji et al., Reference Mobolaji, Fatusi and Adedini2020). The available studies showing the relationship between ethnicity and sexual behaviours have used a quantitative approach (Odimegwu and Somefun, Reference Odimegwu and Somefun2017). This paper contributes to the existing body of knowledge by using a mixed-method approach to understand why young adults with different ethnic affiliations engage in protective sexual behaviours. Young adults belonging to a particular ethnic group may engage in sexual behaviours based on the traditions in their family environment or in their communities. Highlighting ethnic differences in youth sexual behaviours will inform the promotion of sustainable sexual health education among each ethnic group.
Several theories have been used to explain the relationship between ethnic affiliation and sexual behaviours, but this paper uses the primary socialization theory which posits that all or major components of human behaviours are learned (Oetting et al., Reference Oetting, Donnermeyer, Trimble and Beauvais1998). Diverse ethnic groups often maintain distinct cultural norms and values concerning sexuality. According to socialization theory, individuals are typically introduced to these norms and values within their specific ethnic communities during their formative years. These cultural norms and values can significantly shape the perceptions and behaviours related to sexuality in young people from various ethnic backgrounds.
This suggests that the sexual behaviours of young adults might be influenced by their affiliation with a particular ethnic group and the ethnic composition of their social surroundings. When surrounded by members of the same ethnic group who are presumed to both practice and endorse these cultural norms, young adults are more likely to engage in sexual behaviours associated with their own ethnic background, regardless of their socio-economic characteristics.
Socialization into ethnic norms and values typically commences within the family unit. Families frequently pass down cultural beliefs and attitudes regarding sexuality to their offspring. Additionally, peer groups can play a role in reinforcing these values or introducing alternative perspectives. For instance, some ethnic communities may place a strong emphasis on abstinence until marriage, while others may adopt more lenient stances towards premarital sex. Parents and peers both wield significant influence as socialization agents in the lives of young adults, shaping their ethnic attitudes and sexual behaviours. Moreover, young adults establish a sense of ethnic identity through a process of exploration and commitment, which encompasses self-identification with their ethnic group, experiencing a sense of belonging, and cultivating positive attitudes towards this group.
It’s important to note that in certain contexts, such as Northern Nigeria, child marriage has been documented as being promoted by parents as a means of fostering family alliances or expressing gratitude to their sponsors (Adekola and Ogundipe, Reference Adekola and Ogundipe2017). This practice which is promoted by parents in the North may also influence youth sexual behaviours such as condom non-use and early initiation of sexual activity. Among the Igbo ethnic group, women are usually excluded financially as several privileges are entrusted in the hands of men and passed down to younger males (Nwabunike and Tenkorang, Reference Nwabunike and Tenkorang2015). This practice may influence the sexual behaviours of young Igbo adults where male domination may be seen as the norm and affect sexual negotiation among young adults. The Yoruba ethnic group has been reported to sanction premarital sexual activities and frowns against unplanned pregnancy especially among young women (Melvin and Uzoma, Reference Melvin and Uzoma2012). These norms among the different ethnic groups may be transmitted to young adults through parents, peers, and available mass media in their environment. In addition, religion often plays a vital role in socializing individuals regarding sexual behaviour. Different ethnic groups may have varying religious affiliations with distinct teachings on sexuality. These teachings can significantly impact youth sexual behaviour. Additionally, community and cultural institutions can reinforce or modify these religious teachings.
One limitation frequently encountered in past studies that have applied the socialization theory to explore the relationship between ethnic affiliation and sexual behaviours is a lack of comprehensive consideration for the broader societal and contextual influences that may interact with ethnic norms and values. Previous research has often focused primarily on the role of ethnic affiliation in shaping young adults’ sexual behaviours, overlooking external factors that can significantly impact these behaviours.
This current study addresses this limitation by recognizing and acknowledging the potential influence of broader contextual factors. By contextualizing the findings within specific regions of Nigeria, this study demonstrates an awareness of the complex interplay between ethnic norms and wider societal dynamics. It goes beyond attributing all variations in sexual behaviours solely to ethnic affiliations and recognizes that certain practices promoted by parents and communities may intersect with or even contradict ethnic norms, leading to nuanced outcomes.
In essence, this study takes a more comprehensive and nuanced approach, acknowledging the interplay of ethnic norms and contextual factors, thereby addressing a limitation observed in previous research that may have oversimplified the relationship between ethnic affiliation and sexual behaviours.
This study is timely because sexual and reproductive health (SRH) is essential for youth health and well-being. Due to the changes that occur from young adulthood into adulthood, SRH decisions made during the youth phase have implications for them now and in the future. Ethnic affiliations and health are interconnected and present through the values, norms, and beliefs of the people in the context. Knowledge about the relationship between ethnic affiliation and sexual behaviours will help inform the sustainability of existing youth SRH services, especially in a diverse country like Nigeria.
Methods
The setting
This study was a cross-sectional survey conducted in 2018 in Kano, Enugu, and Osun State. Kano is in northwest Nigeria, and the principal inhabitants of the state are the Hausa/Fulani people, with Islam being the prevalent religion in the state (Ehrhardt, Reference Ehrhardt2016). There is a widespread practice of early marriage in this setting, and the Islamic law allows the marriage of young girls who have not started menstruation (Ajuwon et al., Reference Ajuwon, Olaleye, Faromoju and Ladipo2006). Enugu is in Southeast Nigeria, primarily inhabited by the Igbo people and described as a Christian region (Uchendu, Reference Uchendu2010). Osun State, consisting of Yoruba people, is located in south-western Nigeria, and it has been reported that the state has an equal representation of Muslims and Christians (Sampson, Reference Sampson2014). These states were purposively selected for a cross-sectional study of protective sexual behaviour (PSB) among youth in Nigeria, based on data from the Nigeria Demographic and Health Surveys (NDHS). The rationale behind the choice of research sites is rooted in the examination of data from the (National Population Commission, 2013), which was a crucial component of my doctoral dissertation. The primary objective of my dissertation was to assess the levels and patterns of protective sexual behaviour among young people in Nigeria. This investigation was carried out in four states, with one state selected from four of the six geopolitical zones. The selection process was purposeful and based on the prevalence of protective sexual behaviours among Nigerian youth as indicated in the 2013 NDHS data. These behaviours encompassed aspects such as abstinence (both primary and secondary), condom usage during the most recent sexual encounter, Human immunodeficiency virus (HIV) testing, and engagement in single sexual partnerships. These variables were aggregated to create a composite score, categorized as ‘Yes’ or ‘No’. States were chosen for inclusion in the study based on having the highest prevalence of these behaviours within the three major ethnic groups (Hausa, Igbo, and Yoruba). Additionally, a control state was selected from a different ethnic group within the country to ensure diversity in the sample, but this was not included in this study.
Accessing young adults
The sample for this study was constructed through snowball sampling. Young adults who were known to the study team helped recruit other young adults for the study. We put up posters with our contact details in universities and higher education institutes inviting people for the study. Once they contacted the study team, we explained the study to them and confirmed if they were willing to partake in the study. On some days, the data collectors who were young adults in selected states approached other young adults in malls, lesson centres, garages, and markets. For people younger than 18, we took their contact details and visited them in their homes or addresses they provided to get parental consent for the study. Some of the respondents in the quantitative study were asked to participate in the qualitative arm of the study, and a similar approach was used to recruit other respondents for focus group discussions (FGD) and in-depth interviews (IDI). The aim of going to the universities and other places where youth congregate was to include both in and out of school youth. The sample size by state has been presented in Table 1.
Table 1. Percentage Distribution of Protective Sexual Behaviour by State

Sampling design
The main study adopted a three-stage cluster random sampling technique. Detailed information on sample size calculation has been reported elsewhere (Somefun, Reference Somefun2019). For this paper, we used a subset of the young adults recruited in the main study. Youth were recruited based on a three-stage cluster sampling technique. In Nigeria, each state has 3 senatorial districts with an average of 11 local government areas (LGAs) per district. The list of LGAs was stratified into urban, suburban, and rural. Using a simple random sampling technique, two LGAs were selected by balloting from each urban, suburban, and rural LGAs making a total of six districts per district. In each of the LGAs (rural or urban), two wards were selected by balloting from the list of wards obtained from the LGA commission. Wards were regarded as clusters. In each ward, youth locations where many congregate (markets, lesson centres, garages, and schools) were identified and young people (male or female) who were within the age group 15–24 were invited to participate in the study.
For the qualitative arm of the study, the states were stratified into three main strata: the urban, rural, and suburban. The sampling frame consisted of the list of all wards, the lowest geopolitical unit. Two wards were selected from each of the three LGA in each state (a total of six wards per state). Four focus groups were held per ward in each state (one male and one female). Therefore, 24 focus group discussions were held in each state. The FGDs were stratified by age (15–17 and 18–24) and by gender to capture variations among different subgroups and for homogeneity. Demographic data were collected before the discussions and interviews.
Measures
The outcome variable for this study is PSB which was measured as abstinence (primary) and condom use at last sex.
The key independent variable is ethnic affiliation. There are various conceptualizations of ethnicity in the literature, such as ethnic background; cultural, traditional, or religious background; and migration or immigration history. In this study, we focus on the ethnic origin which implies where the ethnic affiliation of the parent, where the respondent was born, and the number of years the respondent had stayed in the location. Respondents whose parents identified with a particular ethnic affiliation – for instance, Hausa – and had lived in Kano all their lives were categorized as ‘Hausa’. Similar categorizations were done for Igbo and Yoruba. Based on the age group of the respondents, there were not many migrants, but the few migrants and respondents who did not fall into any of the three ethnic affiliations were dropped for this analysis.
Other variables that have been considered include age (categorized as ‘15–17’ and ‘18–24’), place of residence (categorized as ‘urban’, ‘suburban’, and ‘rural’), education (categorized as ‘no education,’ ‘primary,’ ‘secondary’, and ‘tertiary’), self-efficacy (categorized as ‘low’ and ‘high’), family structure (presence of two parents), and presence of role models as independent variables in the analysis.
Self-efficacy has been defined as one’s confidence in their ability to handle a situation well. For the purposes of this study, the self-efficacy questions focused on a sexual context. This variable comprised of four questions: I feel confident I could purchase condoms without feeling embarrassed, I feel confident in my ability to use a condom, I am confident I could gracefully remove a condom after sexual intercourse, and I am confident I can insist on condom use every time I have sex. Cronbach alpha reliability estimate for the constructs provided evidence in support of a strong and acceptable internal reliability (α = 0.8443). Initial responses to these questions were rated on a three-point Likert scale with categories defined as Agree, Disagree, and Don’t Know. This was recoded into two categories such as low and high where ‘disagree’ and ‘don’t know’ were categorized into low.
Analysis
We presented the distribution of protective sexual behaviours by ethnic affiliation and other variables. Logistic regression was also used to examine the unadjusted and adjusted associations between ethnic affiliation and protective sexual behaviours. The multivariate analyses allowed us to examine the unique predictive contribution of ethnicity while controlling for other predictors that may be contributing to the relationship between ethnicity and PSB.
Data transcription
Interviews were recorded using audio recorders. Nonverbal communication during discussions was also noted. Each recording was appropriately labelled with the category of young adult (e.g. urban male youth, Kano, rural female youth Osun, etc.), date of interview, and type of interview (FGD or IDI). The interview data was analysed for content and themes using deductive and inductive approaches. A codebook was developed based on the interview guide and research questions. Transcripts were uploaded into NVivo for coding.
Ethical considerations
Study procedures were approved by the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (H17/11/54) and the National Health Research Ethics Committee of Nigeria (NHREC/01/01/2007–16/10/2018). Each participant signed an informed consent form. Respondents were guaranteed utmost confidentiality, privacy, and anonymity. Based on the age of some of the participants, permission from parents and guardians was sought and obtained to interview the participants less than 18 years. The voluntary nature of participation was stressed to both participants and parents.
Results
Descriptive statistics
The total number of respondents was 1,393. Igbo respondents made up about 44% of the sample followed by Yoruba (34%) and Hausa (22%) respondents. The descriptive statistics in Table 1 shows the percentage distribution of young adults by primary abstinence and condom use at last sex. Primary abstinence ranged from 72%, 68%, and 80% for Yoruba, Igbo, and Hausa young adults, respectively. Condom use at last sex was 56% among Hausa young adults and 80% among the Igbo and Yoruba young adults. In short, the Yoruba youth were the most likely to be sexually active but also had high rates of condom use. Igbo youth were somewhat less likely to be sexually active but still used condoms at high rates when they were having sex. Hausa youth were least likely to be sexually active but also least likely to use condoms.
Overall, there was an equal distribution of females and males, but 55% of the Igbo youth were females compared to 45% of their male counterparts. More than three-quarters of the young adults were aged between 18 and 24 years. There was a larger sample of Yoruba (87%) young adults in rural areas compared with the Hausa (66%) and Igbo (25%) youth sampled. More than half of the young adults sampled had some form of secondary level education, and more than half of the young adults were living with both parents. The presence of role models was highest among Igbo (60%) young adults compared with Yoruba (48%) and Hausa (46%) young adults (See Table 2).
Bivariate analysis
The unadjusted results in Table 3a and 3b show the independent effect of selected variables on abstinence and condom use at last sex. Young adults who belonged to the Hausa ethnic group had significantly higher odds of abstinence compared with their Yoruba counterparts.
Table 2. Variable Distribution by State

Table 3a. Unadjusted Association Between Characteristics and Abstinence in the States

***p < 0.01; **p < 0.05; *p < 0.1.
Table 3b. Unadjusted Association Between Characteristics and Condom Use in the States

***p < 0.01; **p < 0.05; *p < 0.1.
Males with Yoruba and Igbo ethnic affiliation had lower odds of abstinence compared with their female counterparts, but this association was only significant for Igbo males. By age, Igbo and Yoruba youth aged 18–24 had lower odds of abstaining than their counterparts aged 15–17. Igbo youth living in suburban and rural areas had significantly higher odds of abstaining compared with their counterparts living in urban areas. Similarly, Hausa living in suburban had significantly higher odds of abstaining compared with their counterparts living in urban areas. Muslim Yoruba and Hausa youth had higher odds of abstaining, but this association was only significant for Yoruba Muslims.
Yoruba young adults with secondary and higher level of education had lower odds of abstaining compared with their counterparts with less than secondary level education. On the contrary, Hausa young adults with secondary and higher level of education had higher odds of abstaining compared with their counterparts with less than secondary level education.
All the youth living with neither parent were significantly less likely to abstain than their counterparts living with both parents. This relationship was the same for youth living with their mother and father alone. Igbo youth who had role models in the community had significantly higher odds of abstinence compared with their counterparts with no role models. By condom use, Hausa young adults had significantly lower odds of condom use compared with their Yoruba counterparts.
Multivariate analysis
The adjusted panel in Table 4a shows that Hausa youth were significantly more likely (OR 3.82; CI 1.92–7.59) to abstain compared with their Yoruba counterparts. Place of residence, educational attainment, and family structure were factors associated with abstinence among youth. For instance, Hausa youth in suburban areas were significantly more likely (OR 7.48; CI 1.75–31.84) to abstain compared with their counterparts in urban areas.
Table 4a Adjusted Association Between Characteristics and Abstinence in the States
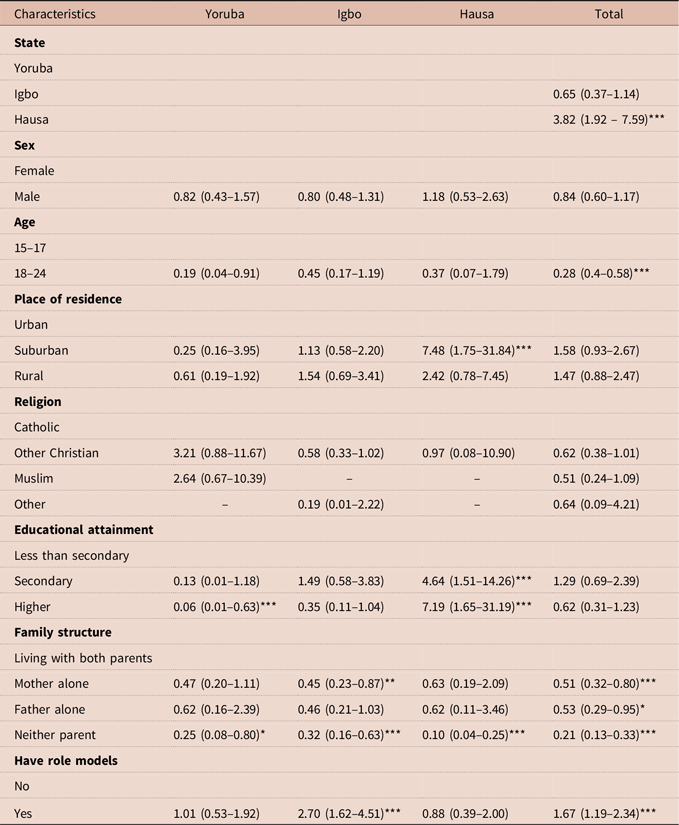
***p < 0.01; **p < 0.05; *p < 0.1.
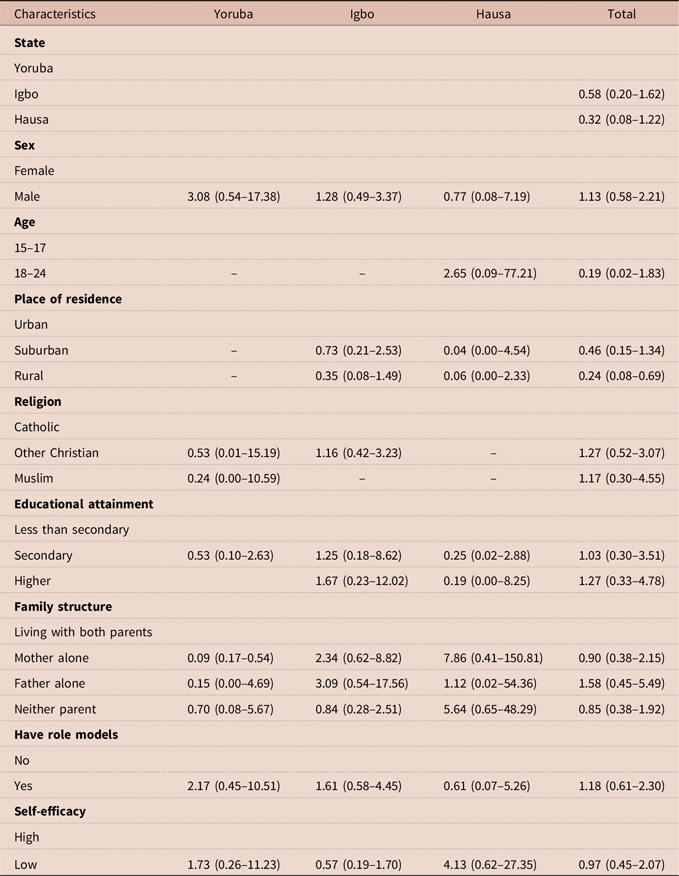
Table 4b. Adjusted Association Between Characteristics and Condom Use in the States
The influence of education on abstinence differed by ethnic affiliation. For instance, among Hausa young adults, higher education was significantly associated with higher odds (OR 7.19; CI 1.65–31.19) of abstinence, but higher education was associated with lower odds of abstinence among Yoruba young adults (OR 0.06; CI 0.01–0.63). Living with neither parent was significantly associated with lower odds of abstinence among the Yoruba (OR 0.25; CI 0.08–0.80), Igbo (OR 0.32; CI 0.16–0.63), and Hausa (OR 0.10; CI 0.04–0.25) young adults. Igbo young adults (OR 2.70; CI 1.62–4.51) who had role models in the community had significantly higher odds of abstinence compared with their counterparts with no role models.
By condom use, Igbo and Hausa youth had lower odds of using condoms, but the association was not significant (See Table 4b).
Other findings
Participants in the study were unmarried males and females aged 15–24 years. The total number of FGDs and IDIs for each ethnic affiliation is shown in Appendix 1. For this analysis, all the young adults presented in Kano were Hausas, in Enugu were Igbos, and in Osun were Yorubas. To explore the reasons for engaging in protective sexual behaviours, some thematic headings emerged such as pull, push, coercive, and restrictive factors. Some findings from the FGDs complement the quantitative results. For instance, quantitative results showed that Igbo male young adults have lower odds of abstinence. One of the Igbo females in an FGD explained this in noting that ‘It is not easy for men to be faithful because of their dynamic nature.’ (Female FGD, Urban, Enugu). In an IDI, one of the young Hausa males stated that premarital sex was a sin in the Quran, and he only wanted to have sex in a marital union. Fear, parental communication, lack of opportunity, and personal readiness were some of the prominent concurrent themes in narratives surrounding protective sexual behaviours across all ethnic affiliations. Each of these themes will be described individually.
Fear
Fear as a reason for abstinence and condom use was a prominent theme among young adults interviewed, although the reasons for their concerns varied. Some young men were afraid of early fatherhood, and some young women were worried about unplanned pregnancy and contracting Sexually transmitted infections (STIs). For instance, a 22-year-old female attending tertiary school in urban Enugu mentioned that she was afraid of getting pregnant, as pregnancy would mean dropping out of school and being laughed at by her friends. A young male aged 19 in Osun said he did not want to risk having sex without condoms – ‘I’ve never had sex, because I am not ready to be a father or be in a relationship with anyone’. Female and male young adults belonging to the Hausa ethnic group appeared to be more conservative and expressed fear of their parents as reasons for abstinence. For instance, ‘I decided to wait because I don’t want trouble for myself as I am still living with my parents. Which means I am afraid of impregnating any lady now’ (Male, IDI, rural educated).
Parental engagement
Parental engagement was only prominent among young adults who belonged to the Igbo and Yoruba ethnic affiliation. However, the type of engagement differed. For instance, some parents were more supportive, while some parents used alternative techniques.
In-depth interview with a Yoruba young adult,
‘Yes. Personally, my own experience. When I was eighteen on the day of my birthday my dad gave me a pack of condoms. He was like, keep it…’. (Male IDI, urban educated)
FGD with Yoruba young adult,
‘My mother beats me when I bring home what is not mine or sees me spending money she did not give me, she tells me that I shouldn’t accept that money…she also beats me when I come home late…She says I was late because I was with a boyfriend’. (Female, FGD, rural educated)
Another Igbo young adult in an FGD mentioned that they preferred to talk to their mothers about issues related to their sexual behaviours.
‘My sisters and I prefer to talk to our mother because we spend most of our time with her. She told me about condoms and not allowing any man to come near me. My father comes home late and always too serious. We only discuss schoolwork with him’. (Female, FGD, rural)
‘Unlike men, mothers know more about pregnancy cycle … so it is easier to talk to them’. (Female, FGD, suburban)
Lack of opportunity
This emerged from the sample of male Igbo youth only. The male youth interviewed reported that they had never had the chance to have sex and they were aged 16, 19, and 21, respectively. However, they had not gotten into tertiary institutions. One of them, who was 16 years old, was in a relationship but was currently living with his parents. He complained of close supervision and said he could not invite female friends over to his house. His girlfriend was also in the same circumstance; he however noted that they would have had sex if the perfect opportunity and space had presented itself.
Media
The use of mass media promoting protective sexual attitudes was revealed to be a reason why some of the young adults who were Igbo and Hausa engaged in protective sexual behaviours. For instance, in rural Enugu, female and male youth said there were programmes by the state government that promoted condom use and abstinence. In Kano also, some of the youth in the urban areas said there was a call-in programme where young people could ask questions regarding their SRH challenges. One of the young Igbo adult elaborated: ‘During some of the music festivals here, the government works with the artists to talk about using condoms… I believe that these activities help remind us to use condoms when we are in school’ (Female, FGD, urban).
Discussion and conclusion
Although studies have explored the relationship between ethnicity and various demographic outcomes in Nigeria, a qualitative perspective on the sexual behaviours of young adults is missing. This paper examines the association between ethnic affiliations and youth sexual behaviour measured as abstinence and condom use, using a mixed-method approach. This is timely because young adults make up a sizeable percentage of the Nigerian population which makes their SRH crucial to achieving the demographic dividend.
The results showed larger number of respondents among Igbo youth which was due to the higher population of youth surveyed in Enugu State. There were variations in the sexual behaviours of young adults with diverse ethnic affiliations. The descriptive findings of our study revealed an intriguing pattern regarding abstinence among young adults from various ethnic groups. The results of a higher rate of abstinence among Hausa youth may appear surprising, especially considering earlier literature that underscored the prevalence of early marriage among Hausa females (Mobolaji et al., Reference Mobolaji, Fatusi and Adedini2020). A recent study examining the association between ethnicity and child marriage reported that child marriage among the Hausa ethnic group was approximately 15–18 times more prevalent than among the Igbo and Yoruba ethnic groups (Mobolaji et al., Reference Mobolaji, Fatusi and Adedini2020). However, it is important to consider the specific focus of our sample, which comprised unmarried young adults. It is plausible that sexual initiation typically occurs within the context of marital unions, a notion supported by insights shared by several participants during focus FGDs and IDIs. This divergent finding contrasts with data from the most recent NDHS (National Population Commission ICF, 2019), which traditionally collects information through face-to-face interviews. In contrast, our survey utilized ODK Collect, a technology-based alternative that affords greater privacy and potentially reduces social desirability bias.
Moreover, our discussions with young adults corroborated these findings. For instance, a male Hausa youth articulated during the discussions that premarital sex was considered a sin in accordance with the Quran, and he expressed a preference for engaging in sexual activity within the confines of a marital union.
These findings collectively suggest that abstinence rates among young adults may be influenced by cultural, religious, and marital factors, which should be taken into consideration when interpreting and comparing these results to broader demographic trends. Further research is warranted to explore the interplay between cultural norms, religious beliefs, and sexual behaviours among young adults in different ethnic contexts.
On the other hand, condom use was lowest among Hausa young adults compared with their Igbo and Yoruba counterparts. The low use of contraceptives among the Hausa ethnic group has been well documented in the literature (Babalola and Oyenubi, Reference Babalola and Oyenubi2018; Odimegwu and Somefun, Reference Odimegwu and Somefun2017; Sinai et al., Reference Sinai, Omoluabi, Jimoh and Jurczynska2020). Polygamy has been stated as one reason for low contraceptive use among people in the North (Sinai et al., Reference Sinai, Nyenwa and Oguntunde2018). It is possible that young adults are being socialized to model the behaviours in the environment which may influence their sexual behaviours. Similarly, it is also possible that young Hausa women are not empowered enough to negotiate condom use due to the Islamic value system of purdah (Konje and Ladipo, Reference Konje and Ladipo1999).
Condom use among the Yoruba young adults was highest and this result was seen in the qualitative findings. Yoruba young adults expressed fear of unplanned pregnancy and early fatherhood as a major reason for using condoms and practising abstinence. Several studies have associated the socio-economic status of Yoruba young adults as a reason for condom use (Ayinmoro and Fayehun, Reference Ayinmoro and Fayehun2022; Somefun, Reference Somefun2019), but majority of our sample had attained secondary level of education; we believe that there may be other reasons beyond education allowing Yoruba youth to engage in protective sexual behaviours. We draw support from a study conducted in south-western Nigeria which focused on pregnancy stigmatization and of adolescent mothers. Although unplanned pregnancy is frowned upon in many Nigerian settings, the Yoruba culture particularly has denigrating words used to address young adults who have unplanned pregnancy. The stigma associated with unplanned pregnancy may be the reasons why young adults in use contexts use condoms (Agunbiade, Reference Agunbiade2014). In the FGDs, fear was also revealed as a reason young Igbo females abstained. Stigma can create some form of fear among young adults in the community, and the relationship between fear and protective sexual behaviour has also been shown in other studies in the United States (Long-Middleton et al., Reference Long-Middleton, Burke, Lawrence, Blanchard, Amudala and Rankin2013). In communities that frown against sexual practices outside unions, members of that ethnic group may feel monitored and decide to engage in practices that are seen as favourable to the community.
On the contrary, some studies have revealed that fear could be the reason why young adults do not use condoms. For instance, the fear of losing condoms inside a woman was a reason young males and females did not use condoms in the Philippines (Lucea et al., Reference Lucea, Hindin, Gultiano, Kub and Rose2013). Our FGDs revealed that some of the young females feared getting pregnant and dropping out of school, and this allowed them to better negotiate condom use in their relationships. Most of the Yoruba women reported that they were afraid of being disowned by their parents if they got pregnant. Dropping out of school and losing friends were the key reasons associated with fear among the female Igbo youth.
Our results on family structure and abstinence showed that youth living with neither parent had lower odds of being abstainers than youth living with both parents for the young adults with the three different affiliations. This is not surprising as analysis of Demographic and Health Survey data (Somefun and Odimegwu, Reference Somefun and Odimegwu2018) and Violence Against Children Surveys (Neville et al., Reference Neville, Saran and Crea2022) has documented the protective effects of living with both parents. This may imply the availability of resources in the household relating to time and supervision. For instance, having both parents could allow them to pool resources that may support the youth. It could also mean that either or both parents may have time to engage the youth on sexual issues. Looking beyond the presence of parents in the household, our study also showed that youth valued the usefulness of parent-child communication. Results from the qualitative data showed that Igbo and Yoruba reported the importance of parent-child communication for youth sexual behaviour. Some of the youth said the decisions they made were because of being able to discuss some issues with their parents, and this did not differ by gender. It is possible that Hausa parents are too conservative to discuss such issues with their young adult children, which has implications for policy and practice.
Gender was significantly associated with abstinence among Igbo young adults and condom use among Yoruba young adults. Male Igbo youth had a lower likelihood of abstaining and a higher likelihood of using condoms. These results are not surprising as they reflect the patriarchal social norms in Nigeria.
Lack of opportunity was a reason cited by young adults for sexual abstinence. This shows that young adults must be consistently engaged to know the reasons behind their behaviours. This would help in the type of interventions for the different groups of young adults. Exposure to mass media has been touted as a predictor of risky sexual behaviour among youth, but qualitative results from our study revealed its protective effects for young adults in Enugu and Kano State. Their reports on the usefulness of radio programmes reveal the need to sustain such interventions. This is because youth are consumers of mass media and information on TV or radio can shape behaviours.
Our results have implications for the existing and new interventions in Nigeria. Some of the factors associated with protective sexual behaviours among youth differed by ethnicity which implies the need for context-based interventions. It is therefore important to continually document the experiences of youth that are engaging in protective sexual behaviours.
Policy implication
Sexually resilient youth have received minimal attention in programmes and policies that have been targeted to their peers engaging in risky behaviours. Based on the results from our study, it is important that programmes continue to support and design interventions that sustain the sexual resilience of these youth. While it is important to design programmes that are aimed at ensuring abstinence, it may be more worthwhile to combine this information with skills that help youth negotiate sex and condom use. These programmes should also consider context and local values. They should take note of cultural differences in designing SRH policies. These policies should be context specific based on the rural-urban differentials that are evident in each ethnic group. Our results also imply that youth have a misunderstanding about sexual behaviours. Messages targeted at youth must be particularly effective and informative such that youth can still engage in protective behaviours while they are away from their parents. The effectiveness of these messages will require the cooperation of communities to support the interventions that are beneficial to sexually resilient youth. Support could be in the form of mentoring and ethnic/faith-based recreational activities.
Limitations
We understand that differences may exist within each ethnic group which is a limitation in our study. However, our focus on differences between ethnic groups rather than within still makes an important contribution to the literature.
Funding statement
This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Centre and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No. G-19-57145), Sida (Grant No. 54100113), Uppsala Monitoring Centre, Norwegian Agency for Development Cooperation (Norad), and by the Wellcome Trust [reference no. 107768/Z/15/Z] and the UK Foreign, Commonwealth & Development Office, with support from the Developing Excellence in Leadership, Training, and Science in Africa (DELTAS Africa) programme. The statements made and views expressed are solely the responsibility of the Fellow. For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Competing interests
The authors declare no conflict of interest.
Appendix 1. Distribution of FGDs and IDIs for Females in Each State

Similar pattern was done for males.






