



Introduction
Inadequate sanitation facilities within households represent a severe public health crisis, particularly in developing countries, where the impact is most profoundly felt. The World Health Organization (WHO) estimates that 2.3 billion people globally lack access to basic sanitation, with 892 million individuals resorting to open defecation. This issue is acutely pronounced in India, where nearly half of the population – 564 million people – are deprived of basic sanitation services, and 230 million practice open defecation (UNICEF, 2017). This stark sanitation infrastructure deficit contributes significantly to the spread of diarrhoeal diseases, parasitic infections, and other waterborne illnesses (Prüss-Ustün et al., Reference Prüss-Ustün, Wolf, Bartram, Clasen, Cumming, Freeman, Gordon, Hunter, Medlicott and Johnston2019). The consequences of inadequate sanitation extend far beyond immediate health impacts, creating a vicious cycle of disease and poverty that affects human capital development through multiple channels. Diarrhoeal diseases, closely linked to poor sanitation, are among the leading causes of child mortality and morbidity (Bitew et al., Reference Bitew, Woldu and Gizaw2017; Prüss-Ustün et al., Reference Prüss-Ustün, Bartram, Clasen, Colford, Cumming, Curtis, Bonjour, Dangour, De France and Fewtrell2014; Njuguna, Reference Njuguna2016). Children suffering from recurrent diarrhoea often face malnutrition and impaired cognitive development, significantly hindering their educational performance (Jasper et al., Reference Jasper, Le and Bartram2012), while adults experience reduced work capacity and diminished income potential, perpetuating intergenerational cycles of poverty (Belay et al., Reference Belay, Asratie, Aragaw, Tsega, Endalew and Gashaw2022). This situation not only strains healthcare systems but also imposes substantial economic costs through lost productivity and increased medical expenses, creating an economic burden that developing countries can ill afford (Cairncross and Valdmanis, Reference Cairncross and Valdmanis2006).
The existing literature has identified a complex web of barriers to sanitation adoption, encompassing cultural, economic, and social dimensions. Deep-rooted social norms and cultural beliefs, particularly those that associate toilets with impurity, present significant obstacles to the acceptance of improved sanitation practices (Routray et al., Reference Routray, Schmidt, Boisson, Clasen and Jenkins2015; Biswas et al., Reference Biswas, De, Mudra and Gupta2024). These cultural impediments are further reinforced by the belief that open defecation is healthier, stemming from its perceived connection to the natural environment (Roy et al., Reference Roy, Rahaman and Chouhan2024). Social identities, including caste and religious affiliations, significantly influence access to sanitation facilities, with empirical evidence highlighting systematic disparities across different groups (Balasubramanya et al., Reference Balasubramanya, Stifel, Alvi and Ringler2022; Mishra, Reference Mishra2023). Lower caste households frequently encounter disproportionate barriers to accessing sanitation facilities, reflecting broader patterns of social inequality that persist in many parts of India (Alexander et al., Reference Alexander, Allton, Felsman, Hahn, Okegbe, Palmer, Taglieri and Thibert2016; Coffey et al., Reference Coffey, Gupta, Hathi, Khurana, Spears, Srivastav and Vyas2014). From an economic standpoint, household decisions regarding toilet adoption follow a cost–benefit framework, where the likelihood of adoption increases when perceived benefits – such as improved health outcomes, enhanced privacy, and elevated social status – outweigh the associated costs (Coffey et al., Reference Coffey, Spears and Vyas2017; Duflo et al., Reference Duflo2015).
Gender inequalities are particularly exacerbated by inadequate sanitation infrastructure, adding another critical dimension to the challenge (Adukia, Reference Adukia2017; Kayser et al., Reference Kayser2021). Women and girls are disproportionately affected by the absence of safe and private facilities, often being compelled to seek secluded locations for defecation, which exposes them to harassment and sexual violence (Purkayastha, Reference Purkayastha2023). These risks severely limit their ability to participate in education and economic activities, reinforcing cycles of inequality (Jalali, Reference Jalali2021; UNICEF, 2023; Sahoo et al., Reference Sahoo, Hulland, Caruso, Swain, Freeman, Panigrahi and Dreibelbis2015; Saleem et al., Reference Saleem, Burdett and Heaslip2019). The gravity of these concerns is amplified when women must relieve themselves during less visible hours, increasing their vulnerability to assault (O’Reilly, Reference O’Reilly2016; Khanna and Das, Reference Khanna and Das2016). Cultural norms in many rural areas further intensify these safety concerns, as traditional practices often dictate that women and girls must conceal their sanitation activities, stifling open discussions about their specific needs (Saleem et al., Reference Saleem, Burdett and Heaslip2019; Pearson and McPhedran, Reference Pearson and McPhedran2008).
To address these multifaceted challenges, governments and organisations have implemented various social schemes that combine financial subsidies, community engagement, and educational campaigns. India’s Swachh Bharat Mission (Clean India Mission), launched in 2014, represents a landmark initiative to eliminate open defecation and promote toilet construction across both rural and urban areas. While the mission has achieved significant progress in infrastructure development, substantial challenges remain in ensuring sustained use of these facilities and reaching marginalised communities (Kedia, Reference Kedia2022; Behera et al., Reference Behera, Pradhan, Behera, Jena and Satpathy2021). Behaviour change campaigns have emerged as essential complements to economic incentives in tackling sociocultural barriers to toilet adoption (Surya et al., Reference Surya2017). These campaigns are particularly effective when they leverage community engagement strategies and actively involve local leaders and influencers (Novotný et al., Reference Novotný2024). Government subsidies and financial assistance programmes are pivotal in alleviating costs, making it possible for economically disadvantaged households to build and maintain essential sanitation facilities (Bishoge, Reference Bishoge2021; Evans et al., Reference Evans, Van der Voorden and Peal2009; Clasen et al., Reference Clasen, Boisson, Routray, Torondel, Bell, Cumming, Ensink, Freeman, Jenkins and Odagiri2014; Augsburg et al., Reference Augsburg2023). Environmental conditions, including water availability and physical terrain, further influence the feasibility of building and maintaining toilets, necessitating adaptations such as dry toilets or composting systems in water-scarce regions (Kithuki et al., Reference Kithuki2021; Shrestha et al., Reference Shrestha, Bhattarai, Acharya, Timalsina, Marks, Uprety and Paudel2023).
Despite extensive research on sanitation barriers and interventions, significant gaps remain in understanding how social scheme participation affects infrastructure adoption and associated behavioural changes. Previous studies have largely examined infrastructure development (Dandabathula et al., Reference Dandabathula, Bhardwaj, Burra, Rao and Rao2019) or behavioural aspects (Surya et al., Reference Surya2017) in isolation, but few have investigated their joint dynamics. While the literature acknowledges the role of social schemes in promoting sanitation (Curtis, Reference Curtis2019), rigorous evaluations of their impact on multiple sanitation outcomes remain scarce. Furthermore, existing research has not adequately explored how the effectiveness of these interventions varies across different socio-economic groups, particularly in contexts where social and cultural barriers intersect with economic constraints. The relationship between toilet adoption and complementary hygiene practices, such as soap usage, remains understudied despite its crucial importance for public health outcomes.
This study addresses these critical gaps by investigating how participation in social schemes influences both toilet adoption and soap usage in rural India. Using panel data from the India Human Development Survey (IHDS) (2004–05 and 2011–12), we employ a Linear Probability Model (LPM) with Propensity Score Matching (PSM) to address potential selection bias in scheme participation. The analysis specifically examines three key questions: First, how does participation in social schemes affect household decisions to adopt toilets? Second, do these interventions generate positive externalities in the form of improved hygiene practices, particularly increased soap usage? Third, how do these effects vary across different socio-economic and demographic groups? Examining these questions provides insights into the mechanisms through which social schemes can effectively promote both infrastructure adoption and sustainable behavioural change.
This research contributes to the literature in several significant ways. First, rigorous empirical evidence is provided on the effectiveness of social schemes in promoting both toilet adoption and improved hygiene practices, offering a more comprehensive understanding of intervention impacts than previous single-outcome studies. Second, the analysis of heterogeneous effects across social groups identifies which populations benefit most from these interventions and where additional support may be needed. Third, examining the relationship between toilet adoption and soap usage sheds light on potential complementarities in sanitation behaviours, informing the design of more holistic interventions. These findings have important policy implications, particularly when sanitation challenges are deeply entrenched and multifaceted. The results suggest that focusing simultaneously on infrastructure development and behavioural change while accounting for local social and cultural contexts can lead to more effective and sustainable sanitation improvement.
Data and methodology
Data
This study utilises two rounds of the IHDS panel data to analyse the impact of households’ access to social schemes on sanitation behaviours and outcomes. The IHDS is a comprehensive nationwide survey that captures detailed information across multiple household welfare and development dimensions. The survey’s extensive coverage includes data on health, employment, education, social networks, economic status, fertility, marriage, gender relations, and social capital, enabling a thorough examination of the various factors that influence household sanitation practices. The survey was conducted in two rounds (2004–05 and 2011–12), covering 215,754 individuals and 41,554 households across 1,503 villages and 971 urban neighbourhoods in 33 states and union territories of India ( Desai et al., Reference Desai and Vanneman2018a, Reference Desai and Vanneman2018b). The longitudinal design, with a robust re-contact rate of 84 per cent in Round II, allows us to track changes in sanitation practices over time, providing a unique opportunity to examine the impacts of social scheme participation on household behaviour.
The analysis focuses on understanding two key outcomes: toilet adoption and soap usage. For toilet adoption, the dependent variable is constructed by identifying households that did not have toilet access in 2004–05 but acquired one by 2011–12, coded as a binary indicator (1 for adoption, 0 otherwise). Similarly, changes in hygiene practices are tracked through soap usage, represented as a binary variable indicating whether households reported using soap in 2011–12. The primary explanatory variable of interest captures participation in social schemes for sanitary latrines, measured through the survey question: ‘During the past five years, did the household benefit from a government/private social scheme for sanitary latrine/toilet?’ This binary indicator identifies households participating in such schemes during the study period.
To account for the complex socio-economic factors that influence sanitation behaviours, a comprehensive set of control variables is incorporated. Economic status is captured through multiple measures: monthly per capita expenditure (logged) reflects short-term economic conditions, while a household assets index provides insight into long-term wealth accumulation. The analysis also includes below poverty line (BPL) status to identify economically vulnerable households. Educational attainment is measured through the highest years of schooling achieved by adult males and females within each household, recognising the potentially different impacts of male and female education on household decision-making. Demographic characteristics are captured through variables including the number of married females and elderly members (aged 60+ years) in the household, while social identity is reflected through caste status (Scheduled Caste/Scheduled Tribe) (SC/ST) and religious affiliation (Muslim/non-Muslim).
Infrastructure and community-level factors are represented through several variables: access to piped water supply, proximity to panchayat members or officials, and household confidence in the panchayat’s ability to implement public projects. Measures of media exposure are included through variables capturing television viewing and newspaper reading habits among male household members. At the village level, sanitation infrastructure is accounted for through the presence of cemented drainage systems (pucca), and existing sanitation norms are captured through the percentage of households practicing open defecation. This rich set of covariates enables us to control the various socio-economic, demographic, and infrastructural factors that might influence a household’s transition to improved sanitation facilities, thereby helping to isolate the specific impact of social scheme participation.
Methodology
The empirical evaluation of social schemes’ impact on sanitation outcomes presents significant methodological challenges, primarily due to self-selection bias in programme participation. Households that choose to participate in social schemes may systematically differ from non-participating households in ways that influence their sanitation behaviours. These differences could stem from unobservable factors such as health awareness, environmental consciousness, or general receptiveness to government initiatives. Consequently, standard regression approaches might yield biased estimates of the causal relationship between scheme participation and sanitation outcomes. To address these challenges, a dual methodological approach is employed, combining LPMs with PSM.
The primary empirical strategy begins with a LPM that estimates the relationship between social scheme participation and sanitation outcomes while controlling for an extensive set of household and community characteristics. The baseline specification is
 $$Y\; = \;\alpha \; + \;\beta \left( {Social\;Scheme} \right)\; + \;\delta \left( X \right)\; + \varepsilon \;$$
$$Y\; = \;\alpha \; + \;\beta \left( {Social\;Scheme} \right)\; + \;\delta \left( X \right)\; + \varepsilon \;$$
where Y represents the binary outcomes of interest (toilet adoption and soap usage) measured in 2011–12, Social Scheme indicates household participation in sanitation-related social schemes during the preceding five years, and X comprises a comprehensive vector of control variables capturing household socio-economic status, demographic composition, and community characteristics. The coefficient β represents the coefficient of interest, measuring the effect of scheme participation on sanitation outcomes. While this approach allows us to control for observable characteristics that might influence both participation and outcomes, it may not fully address selection bias arising from unobservable factors.
To strengthen the empirical analysis, the LPM approach is complemented by PSM. PSM creates a quasi-experimental framework by constructing treatment and control groups that are balanced across observable characteristics, thereby approximating the conditions of a randomised controlled trial. PSM is implemented through a three-step process. Propensity scores are first estimated to represent each household’s probability of participating in social schemes, conditional on observed characteristics. These scores are calculated using a logistic regression model that incorporates a full set of covariates, including economic indicators (per capita consumption expenditure, assets index, and poverty status), human capital measures (educational attainment of adult males and females), social identity markers (caste and religious affiliation), household composition (size and number of elderly members and married females), community connections (proximity to panchayat officials), and village-level infrastructure (drainage systems and water access).
Following propensity score estimation, Radius Matching with a caliper of 0.01 is employed as the primary matching algorithm, following methodological precedents established in prior impact evaluation studies (Kumar and Vollmer, Reference Kumar and Vollmer2013). This approach matches each treated household with all control households falling within a specified radius of its propensity score, offering advantages in terms of both precision and bias reduction compared to simpler matching methods. To assess the robustness of the results, Nearest Neighbor (NN) Matching is also implemented as an alternative specification, comparing outcomes between treated households and their closest matches in the control group based on propensity scores.
While PSM offers substantial advantages in addressing selection bias, its limitations are acknowledged. The method’s validity rests on two key assumptions: first, that all relevant covariates affecting both participation and outcomes (selection on observables) have been adequately captured, and second, that there exists sufficient overlap in propensity scores between treated and untreated households (common support). Extensive diagnostic tests are also conducted to verify these assumptions, examining covariate balance and common support conditions. Additionally, it is recognised that PSM cannot account for the selection of unobservables, though the rich set of control variables helps mitigate this concern.
Results
The LPM analysis reveals substantive impacts of social scheme participation on sanitation outcomes in rural India (Table 1). Participation in social schemes increases the probability of toilet adoption by 45.5% and soap usage by 13.8%, with both effects statistically significant. These magnitudes are particularly noteworthy given the historically low rates of sanitation adoption in rural areas and suggest that well-designed interventions can effectively overcome traditional barriers to improved sanitation practices. The empirical analysis identifies several key household characteristics that systematically influence sanitation behaviours. Economic indicators demonstrate strong predictive power: a one-unit increase in the household assets index corresponds to a 0.99% increase in toilet adoption probability and a 1.43% increase in soap usage probability. The educational attainment of adult household members shows similarly robust positive associations with both outcomes. These relationships persist after controlling for a comprehensive set of socio-economic and demographic variables, suggesting that human capital accumulation plays a crucial independent role in facilitating sanitation improvements.
Table 1. LPM analysis: social scheme on sanitation and household’s toilet adoption and soap usage in India
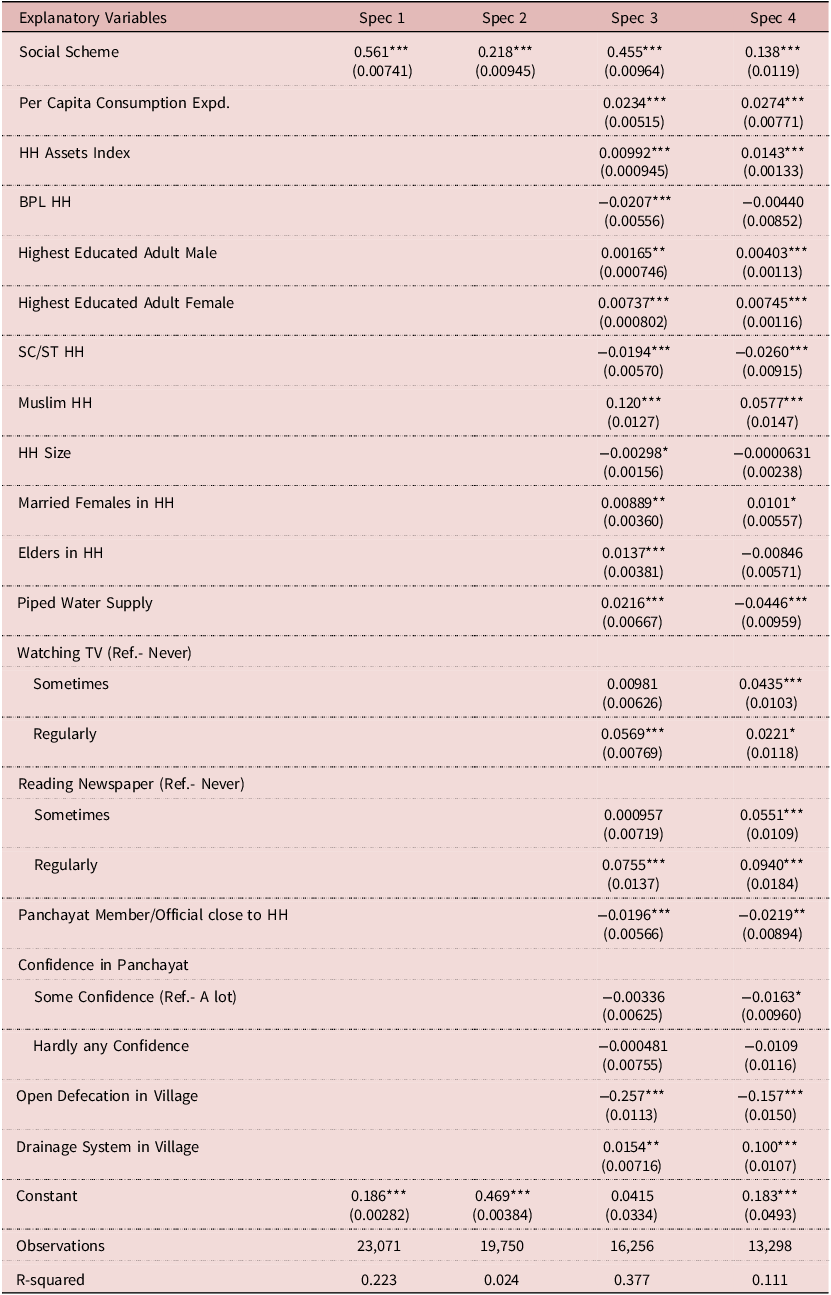
Note: Robust standard errors are in parentheses. For Spec 1 and Spec 3, the dependent variable is toilet adoption. For Spec 2 and Spec 4, the dependent variable is soap usage.
***p < 0.01, **p < 0.05, *p < 0.1.
Social identity markers emerge as significant determinants of sanitation outcomes, revealing persistent structural inequalities in access and adoption patterns. BPL status reduces toilet adoption probability by 2.07%, while SC/ST households show systematically lower probabilities of both toilet adoption and soap usage. These patterns suggest that socio-economic disadvantages continue to constrain sanitation improvements despite targeted intervention efforts. Religious affiliation also influences outcomes, with Muslim households demonstrating higher probabilities of soap usage compared to non-Muslim households, suggesting that cultural practices may meaningfully shape hygiene behaviours. Infrastructure accessibility exhibits complex relationships with sanitation outcomes, revealing unexpected patterns in household behaviour. Piped water supply increases toilet adoption probability by 2.6% but is associated with a 4.46% decrease in soap usage. This seemingly paradoxical relationship may reflect substitution effects in hygiene practices where households rely on water alone for cleanliness. Household media exposure, measured through television viewership and newspaper readership, shows consistent positive associations with soap usage, suggesting that information access through mass media channels may effectively promote behavioural change.
Local governance structures and community-level characteristics significantly influence household sanitation decisions, highlighting the importance of institutional and social context in shaping individual behaviours. Interestingly, households with panchayat members or officials close to them are less likely to adopt toilets and use soap, potentially reflecting complex political or social dynamics at play. This counterintuitive finding suggests that proximity to local governance does not always translate into better sanitation outcomes, possibly due to issues like political patronage or social pressures that discourage change. High levels of open defecation within a village are strongly negatively associated with both toilet adoption and soap usage, indicating that community norms heavily influence individual behaviours. Conversely, the presence of a proper drainage system in the village positively correlates with soap usage, highlighting the role of infrastructure in supporting better hygiene practices.
These findings collectively emphasise the multifaceted nature of sanitation behaviours, where economic status, social identity, cultural influences, infrastructure, and media exposure all interplay to shape outcomes. The demonstrated positive impact of social schemes on toilet adoption and soap usage suggests that targeted, well-designed interventions can significantly enhance sanitation outcomes in developing countries. However, the varying effects across different social and economic groups indicate that policymakers must consider individual and collective sanitation behaviour dimensions to design effective strategies to drive sustainable change across diverse communities. The strong influence of community-level factors, particularly the negative association with open defecation practices and positive correlation with infrastructure availability, underscores the importance of addressing both behavioural and structural barriers to improved sanitation.
Results from PSM analysis
Table 2 presents the descriptive statistics for covariates before and after matching, along with the logit regression results for participation in the social scheme. The table is divided into three sections: (1) covariates, (2) matching status, and (3) logit regression results. The covariates included are per capita consumption expenditure, household assets index, BPL status, highest education level of adults in the household, SC/ST status, Muslim status, household size, married females in the household, elders in the household, piped water supply, proximity to a panchayat member or official, level of open defecation in the village, presence of a proper drainage system in the village, and television and newspaper watching habits of men.
Table 2. Descriptive statistics of covariates (pre- and post-matching) and logit result of participation/treatment assignment
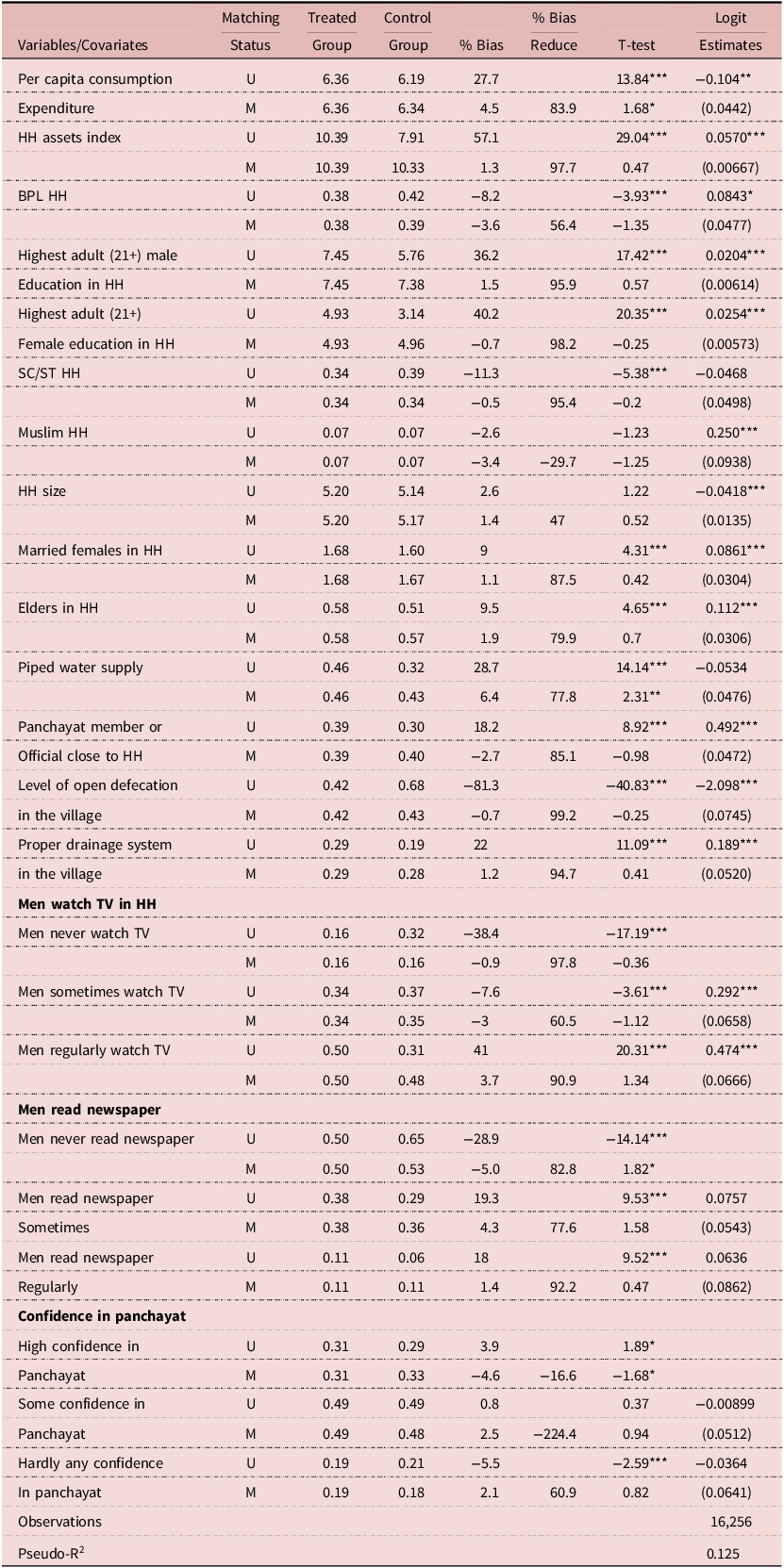
Note: This table presents the descriptive statistics of covariates before and after matching and the logistic regression results for participation or treatment assignment. The covariates include household characteristics such as logged per capita expenditure, asset index, education levels, sanitation access, and participation in social schemes. Pre-matching statistics provide an overview of the covariates’ distribution before applying the matching procedure, while post-matching statistics show the distribution after matching to ensure comparability between treated and control groups. The logistic regression results indicate the likelihood of households participating in or being assigned to the treatment, with coefficients and standard errors displayed. Significance levels are denoted by ***, **, and * for 1%, 5%, and 10%, respectively.
The second section shows the matching status of the covariates, including the matching method (M or U) and the percentage bias reduction for each variable. The percentage bias reduction measures the improvement in balance between the treatment and control groups regarding the covariate distributions. The third section presents the logit regression results examining factors associated with participation in the social scheme on sanitation. The dependent variable is a binary indicator of participation in the scheme. The logit coefficients reflect changes in the log odds of participation for a one-unit increase in each covariate, holding all other covariates constant. The coefficients are accompanied by their standard errors (in parentheses).
For instance, the logit estimate for ‘Per Capita Consumption Expenditure’ is −0.104. This indicates that a one-unit increase in per capita consumption expenditure decreases the log odds of participation by 0.104, corresponding to an odds ratio of approximately 0.901. This means that higher per capita consumption expenditure reduces the odds of participation by about 9.9%, holding all else constant. Similarly, the logit estimate for the ‘Household Assets Index’ is 0.0570, meaning that a one-unit increase in the household assets index increases the log odds of participation by 0.0570, corresponding to an odds ratio of 1.059 or about a 5.9% increase in the odds of participation.
Several covariates are statistically significant predictors of participation. Positive predictors include being below the poverty line, being in a Muslim household, higher education levels of male and female adults (aged 21+), greater household assets, more elders and married females in the household, regular or occasional TV watching by men, proximity to a panchayat member or official, and the presence of a proper drainage system in the village. In contrast, negative predictors of participation include higher per capita consumption expenditure, larger household size, and higher levels of open defecation in the village.
Post matching quality and post-matching diagnostics
Table 3 presents summary measures assessing covariate balance before and after matching. The table demonstrates that, prior to matching, there were substantial imbalances in covariates between the treated and control groups. This is shown by a high
 $Pseudo - {R^2}$
value (0.134), a large LR-
$Pseudo - {R^2}$
value (0.134), a large LR-
 ${\chi ^2}$
statistic (1997.48), and a highly significant
${\chi ^2}$
statistic (1997.48), and a highly significant
 $P - value\;(P \lt 0.001)$
, indicating that the covariates collectively explained significant variation in treatment assignment and the groups were not comparable.
$P - value\;(P \lt 0.001)$
, indicating that the covariates collectively explained significant variation in treatment assignment and the groups were not comparable.
Table 3. Summary measures of matching quality

Note: ***p < 0.01, **p < 0.05, *p < 0.1.
After matching, these measures show dramatic improvements. The
 $Pseudo - {R^2}$
value decreases to 0.003, and the LR-
$Pseudo - {R^2}$
value decreases to 0.003, and the LR-
 ${\chi ^2}$
statistic drops to 21.85 with a non-significant P-value (
${\chi ^2}$
statistic drops to 21.85 with a non-significant P-value (
 $P = 0.349$
). These results indicate that the covariates no longer explain significant variation in treatment assignment after matching, suggesting that the treated and control groups are now well balanced.
$P = 0.349$
). These results indicate that the covariates no longer explain significant variation in treatment assignment after matching, suggesting that the treated and control groups are now well balanced.
The reduction in mean and median standardised biases further confirms the improvement in covariate balance. Before matching, the mean bias was 22.3%, and the median bias was 18.1%. After matching, these biases were reduced to 2.4% and 2%, respectively. These values fall below commonly accepted thresholds (5%), which strengthens confidence in the comparability of the groups. Overall, the results suggest that the matching procedure successfully improved the covariate balance between the treated and control groups, leading to more comparable groups and increased confidence in the estimated treatment effect. Post-matching diagnostics reinforce these findings. Additionally, Figure 1 illustrates the density distribution of propensity scores for treated and control groups, showing sufficient overlap between the groups and satisfying the common support condition.
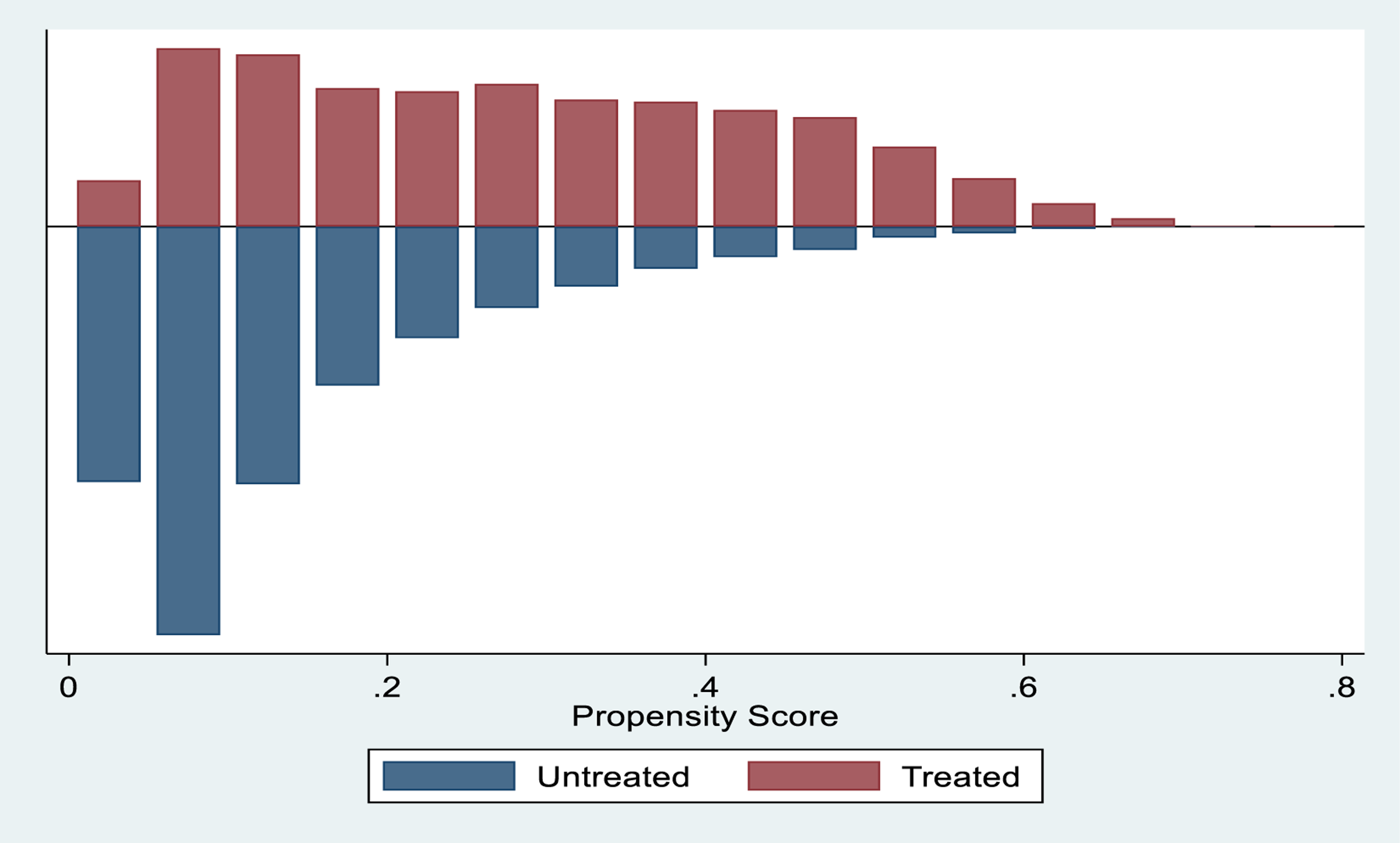
Figure 1. Graph of common support.
Treatment effects: results from PSM
Table 4A presents the results of a PSM estimation to assess the impact of the social scheme treatment on household toilet adoption and soap usage. The findings indicate that households that received the social scheme treatment exhibited significantly higher rates of both toilet adoption and soap usage compared to the control group. Specifically, the mean difference in toilet adoption between treated and control households was 43.5 percentage points (0.734 vs. 0.299). This result is statistically significant at the 1% level, suggesting that the social scheme treatment had a substantial positive effect on toilet adoption. Similarly, the mean difference in soap usage between treated and control households was 13.3 percentage points (0.660 vs. 0.527). While the effect on soap usage was statistically significant at the 1% level, it was less pronounced compared to the impact on toilet adoption.
Table 4A. PSM estimation: impact of social scheme treatment on household’s toilet adoption and soap usage in India

Note: ***p < 0.01, **p < 0.05, *p < 0.1
Table 4B further evaluates the robustness of the treatment effects using Radius Matching with a caliper of 0.01. The results reaffirm the positive impact of the social scheme treatment on both outcomes. The mean difference in toilet adoption increased slightly to 44.0 percentage points (0.734 vs. 0.294). Similarly, the mean difference in soap usage was 13.5 percentage points. These findings confirm that the treatment effects are robust to the propensity score model and estimation technique choice. Moreover, the larger mean difference in toilet adoption compared to soap usage is consistent with the results from Table 4A, indicating that the treatment had a stronger impact on toilet adoption.
Table 4B. PSM estimation: Radius Matching (Caliper 0.01)

Note: ***p < 0.01, **p < 0.05, *p < 0.1.
Table 5 presents results using NN Matching, another common PSM technique. These results corroborate the findings in Tables 4A and 4B. The mean difference in toilet adoption was 43.5 percentage points (0.734 vs. 0.299). For soap usage, the mean difference was 13.2 percentage points (0.660 vs. 0.528). Both outcomes remain statistically significant at the 1% level, confirming the robustness of the treatment effects across different matching techniques.
Table 5. Nearest Neighbor (NN) Matching

Note: ***p < 0.01, **p < 0.05, *p < 0.1.
The consistent findings across Tables 4A, 4B, and 5 provide strong evidence of the positive impact of the social scheme treatment on improving sanitation and hygiene outcomes in India. The larger effect size observed for toilet adoption compared to soap usage suggests that the treatment was particularly effective in promoting structural changes, such as building or using toilets, which may have required greater behavioural and infrastructural shifts. However, the positive but smaller effect on soap usage highlights the need for further behavioural interventions to enhance hygiene practices.
Discussion and policy implications
This empirical investigation reveals several critical insights regarding the effectiveness of social schemes in improving sanitation outcomes in developing contexts. The substantial effects on both toilet adoption (45.5%) and soap usage (13.8%) demonstrate that well-designed interventions can successfully promote sanitation improvements. However, the analysis uncovers significant heterogeneity in programme effectiveness across different population segments, pointing to important policy design and implementation considerations.
The systematic variation in programme participation across socio-economic groups emerges as a central concern for policy development. Households characterised by lower educational attainment, limited assets, and BPL status demonstrate significantly lower participation rates in existing sanitation programmes. This finding suggests that current implementation approaches may inadvertently exclude the most vulnerable populations, particularly those who benefit most from improved sanitation. Addressing this participation gap requires developing specialised outreach strategies that explicitly account for disadvantaged communities’ unique constraints. Drawing on established behavioural change literature (Routray et al., Reference Routray, Schmidt, Boisson, Clasen and Jenkins2015; Coffey et al., Reference Coffey, Spears and Vyas2017), such strategies should incorporate culturally sensitive communication campaigns and community-based participatory approaches that foster local ownership and engagement.
Infrastructure complementarities emerge as another crucial determinant of programme effectiveness. The finding that community drainage systems positively correlate with improved sanitation outcomes suggests strong synergies between household-level interventions and community infrastructure. This relationship aligns with recent empirical work emphasising the importance of coordinating physical infrastructure development with behavioural interventions (Augsburg et al., Reference Augsburg2023). The significant positive association between piped water access and toilet adoption (2.6%), coupled with the counterintuitive negative relationship with soap usage (-4.46%), further underscores the complex interplay between infrastructure availability and sanitation behaviours.
The role of information dissemination through media channels warrants particular attention. The results demonstrate that regular exposure to television and newspapers correlates positively with improved hygiene practices, suggesting that mass media can effectively promote behavioural change. However, the literature emphasises the importance of careful message design and delivery to ensure cultural relevance and avoid unintended consequences (Scott et al., Reference Scott, Schmidt, Aunger, Garbrah-Aidoo and Animashaun2008). The negative association between proximity to Panchayat officials and sanitation outcomes raises important questions about local governance effectiveness. This finding, contrary to theoretical expectations, suggests a need to strengthen institutional capacity at the grassroots level, aligning with established research on decentralised service delivery in the WASH sector (Kumar and Vollmer, Reference Kumar and Vollmer2013).
These findings collectively point to the necessity of an integrated policy approach that simultaneously addresses multiple barriers to improved sanitation. Such an approach must combine targeted economic support, infrastructure development, and behavioural interventions while accounting for local social and cultural contexts. The strong negative association between village-level open defecation and individual adoption rates highlights the importance of achieving critical mass in behavioural change to overcome existing social norms. Similarly, the effect of household assets (0.99%) on adoption patterns, alongside other economic indicators, suggests that both long-term wealth and short-term liquidity constraints influence sanitation decisions.
The empirical evidence suggests that improving sanitation outcomes requires careful attention to both individual and community-level factors. Policy interventions should explicitly address the barriers faced by marginalised communities while leveraging the positive spillover effects of community infrastructure and social learning. The significant variation in programme effectiveness across different population segments indicates that a one-size-fits-all approach is unlikely to achieve universal sanitation coverage. Instead, policies must be tailored to local contexts while maintaining sufficient flexibility to address the specific needs of different community segments.
Conclusion
This empirical investigation provides robust evidence that participation in targeted social schemes significantly influences sanitation behaviours among households in rural India. The analysis demonstrates that scheme participation increases toilet adoption probability by 45.5% and soap usage by 13.8%. These substantial effects, identified through PSM to address selection bias, underscore the potential of well-designed interventions to improve sanitation outcomes in resource-constrained settings.
The findings establish social schemes as effective policy instruments for enhancing sanitation practices in regions with inadequate infrastructure. However, the analysis reveals that programme success depends critically on complementary investments in both physical infrastructure and local institutional capacity. The significant role of community-level factors and governance structures, evidenced by the relationships between sanitation outcomes and local infrastructure, village-level practices, and institutional proximity, points to the importance of multi-stakeholder approaches in programme implementation.
Several limitations of the current analysis suggest directions for future research. The durability of behavioural changes requires investigation through longitudinal studies that track outcomes over extended periods. While the present analysis identifies heterogeneous effects across socio-economic groups, a deeper examination of impact variation across demographic and institutional contexts could enhance understanding programme effectiveness. Additionally, expanding the analytical scope beyond toilet adoption and soap usage to include waste management, facility maintenance, and sustained behavioural change would provide a more comprehensive assessment of sanitation interventions.
The empirical evidence demonstrates that carefully designed social schemes can effectively improve sanitation and hygiene outcomes. These findings offer concrete guidance for evidence-based policy development while highlighting the complexity of achieving universal sanitation access. Future research should continue evaluating policy innovations and implementation strategies, building the evidence base for developing more effective and equitable sanitation initiatives. Such work remains crucial for advancing public health outcomes and promoting inclusive development across local and global contexts.
Funding statement
This research work was not supported by any funding from any institution.
Competing interests
No financial or non-financial interests that may have influenced the research findings or their interpretation. There are no conflicts of interest to disclose.
Ethical standard
This research is based entirely on analysis of publicly available data from the India Human Development Survey (IHDS). No primary data collection was undertaken.
Disclaimer
The views expressed herein are personal and do not necessarily reflect the views of the institutions the authors represent.








 Open access
Open access