



Introduction
Adolescence is a critical period of human growth and development, contributing to attainment of more than 20% of adult height and up to 50% of adult weight during this period (Meier et al., Reference Meier, Nickerson, Olson, Berg and Meyer2003). The World Health Organization (WHO) defined the adolescent age group from 10 to 19 years, although the definition may vary from country to country (UN General Assembly,, 1989). Generally, the adolescent period is sub-divided into two stages: early adolescent age (10–14 years) and late adolescent age (15–19 years) (World Health Organization, 2017). Currently, approximately 1.2 billion adolescents live worldwide, and half of them are girls (Black et al., Reference Black, Victora, Walker, Bhutta, Christian, De Onis, Ezzati, Grantham-Mcgregor, Katz and Martorell2013; Engelman et al., 2014; Gielen & Roopnarine). Report shows that 86% of the world’s total adolescents live in low and middle-income countries, and half of the global adolescent population are residents of Asia (Gielen and Roopnarine, Reference Gielen and Roopnarine2016). Proper nourishment during adolescence is crucial to maintain a healthy and productive life (Roba et al., Reference Roba, Abdo and Wakayo2016). Nutritional impairment during adolescence may result in adverse physical and clinical outcomes in later life (Aguayo and Paintal, Reference Aguayo and Paintal2017; Christian and Smith, Reference Christian and Smith2018). Nutrition of adolescent girls is also important for optimum reproductive health and well-being of their offspring (World Health Organization, 2006). Studies confirm that adolescent mothers with malnutrition are more prone to unfavourable obstetric and neonatal outcomes (Black et al., Reference Black, Victora, Walker, Bhutta, Christian, De Onis, Ezzati, Grantham-Mcgregor, Katz and Martorell2013). Therefore, nutritional status of adolescent girls should get proper attention to ensure healthy lives of the next generation.
The term malnutrition comprises both undernutrition (BMI<18.5) and overnutrition (overweight/obesity) (Ahmed et al., Reference Ahmed, Mahfuz, Ireen, Ahmed, Rahman, Islam, Alam, Hossain, Rahman and Ali2012). However, both the spectrum of malnutrition is highly prevalent among the population living in low- and middle-income countries and adolescent girls are not an exception (Kelly et al., Reference Kelly, Yang, Chen, Reynolds and He2008). Globally, 9.7% of women and 8.4% of girls are underweight, while 14.9% of women and 5.6% of girls are obese (Aabdeen and NCD Risk Factor Collaboration, Reference Aabdeen2017). Prior reports showed that the prevalence of undernutrition is alarmingly higher among adolescent girls in Bangladesh (Alam et al., Reference Alam, Roy, Ahmed and Ahmed2010; Kurz, Reference Kurz1996). It was estimated that 26% of the adolescent girls living in rural areas had a low BMI, and 32% were stunted (Alam et al., Reference Alam, Roy, Ahmed and Ahmed2010). Evidence suggests that more women are overweight and obese compared to men in the South Asian countries which was 28% and 22%, respectively for women and men in 2013 (Kelly et al., Reference Kelly, Yang, Chen, Reynolds and He2008). Overweight/obesity is a major health concern for women and adolescent girls, particularly for those who are in reproductive age. This is not only for their potential health risks of developing gestational diabetes mellitus, type II diabetes, and cardiovascular diseases, but also for adverse perinatal, neonatal, infant, and childhood health outcomes (Catalano et al., Reference Catalano, Mcintyre, Cruickshank, Mccance, Dyer, Metzger, Lowe, Trimble, Coustan and Hadden2012). Besides, undernutrition is also a major concern for women of reproductive age (Fahim et al., Reference Fahim, Das, Gazi, Alam, Mahfuz and Ahmed2020). Undernutrition hinders physical and mental development (Brown and Pollitt, Reference Brown and Pollitt1996). Despite recent trends of increasing BMI, prevalence of underweight remains very high in the South Asian countries affecting nearly one in four women in this region (Collaboration, Reference Collaboration2016). Not only in Bangladesh, maternal undernutrition has also been identified as an event of silent emergency in India (Patel et al., Reference Patel, Prakash, Das, Gupta, Pusdekar and Hibberd2018). A study shows that, in Maharashtra women who were underweight during pregnancy were at increased risk of neonatal death and delivering a low birth weight baby (Young et al., Reference Young, Nguyen, Tran, Avula and Menon2020). It is also evident that maternal overweight and obesity increase the risk of maternal morbidity, preterm birth, infant mortality, gestational diabetes, hypertension, and caesarian section as well (Catalano et al., Reference Catalano, Mcintyre, Cruickshank, Mccance, Dyer, Metzger, Lowe, Trimble, Coustan and Hadden2012). Therefore, attention should be given on the nutritional status of the ever-married adolescent girls for their individual health as well as for the sufficient growth and development of their offspring. However, considering the co-existence of both under nutrition – and overweight/obesity in the country, it is important to explore the prevalence of both underweight and overweight/obesity among ever-married Bangladeshi adolescent girls who are at the outset of reproductive age. Hence, the objective of this study was to investigate the prevalence of underweight and overweight/obesity among ever-married adolescent girls in Bangladesh using the national representative data of Bangladesh Demographic and Health Surveys (BDHS) conducted from 2004 to 2014. This study also identified the socio-demographic factors associated with underweight and overweight/obesity among those girls using the same dataset.
Methodology
This study analysed BDHS data from 2004 to 2017 by the National Institute of Population Research and Training, ICF International (USA), and Mitra and Associates. Four surveys were conducted during this period, and the years are as follows: 2004, 2007, 2011, 2014, and 2017. In the BDHS, the participants were selected using a probability-proportional-to-size sampling technique based on a two-stage cluster sample of households and stratified by rural and urban areas in the seven administrative regions of Bangladesh. Data collected from the ever-married adolescent girls with age between 15 and19 years were analysed in this study. Data for never-married adolescent girls were not available in the survey data. Adolescent girls who were pregnant on the survey visit or had given birth during the preceding two months were excluded. Participants with missing data of height and weight were also excluded from the analysis. A total number of 7040 respondents were included in the final analysis, where 1281 adolescents from BDHS 2004, 1058 from BDHS 2007, 1497 from BDHS 2011, 1615 from BDHS 2014, and 1589 from 2017 has been selected for final analysis.
Ethical statement
Ethical approval for the BDHS programme was received from the Institutional Review Board of the Medical Research Council of Bangladesh. Informed consent was obtained from all the participants after notifying them about the purpose of the survey.
Data collection
Data on socio-demographic characteristics were collected at the household level by trained interviewers. Indicators including educational status, involvement in work, region (administrative division of the country) and place of residence (urban or rural), household asset status, and ownership of assets were collected through a face-to-face interview. Household wealth index was calculated using household’s ownership of selected assets including electricity, televisions, and bicycles; materials used for construction of houses; types of water access and sanitation facilities; and use of health and other services, and health outcomes.
Anthropometric measurement
Trained fieldworkers visited the households and measured the height and weight. They collected data twice from each participant and recorded the mean value. We considered the BMI cut-off value set by the WHO for the Asian region to assess the nutritional status. Having a BMI ≥ 23 kg/m2 was considered as overweight, ≥27.5 kg/m2 as obese, and BMI <18.5 kg/m2 as underweight (Tan, Reference Tan2004).
Statistical analysis
Socio-demographic characteristics of the participants were presented using frequencies with percentages. In our study, nutritional status of the adolescent girls based on BMI was the dependent variable. This variable includes three categories: underweight, normal weight, and overweight/obese. Prevalence of overweight/obesity and underweight in different BDHS years were calculated and reported the prevalence with 95% confidence intervals (CI). Pearson’s chi-square (χ2) test was applied to compare between the groups. Multinomial logistic regression analysis was done and odds ratio (OR) was calculated to identify the socio-demographic factors associated with the overweight/obesity and underweight among the adolescent girls. We considered the normal weight group as reference in the regression analysis. At first, we did perform bivariate analyses to select the variables for multivariable analysis. The variables found to be statistically significant (p < 0.05) in the bivariate analyses were considered for the multivariable analysis. A p-value less than 0.05 was considered statistically significant. All the data analyses were done using STATA 14 (Stata Corp. TX. USA).
Results
Socio-demographic characteristics
A total of 7040 ever-married adolescent girls aged between 15 and 19 were interviewed in the last five BDHS. Socio-demographic characteristics of the participants from 2004 to 2017 have been described in Table 1. We observed an increase in the rate of education among the adolescent girls over the survey years from 2004 to 2017 (84.52% vs. 97.73%). The proportion of involvement in paid work increased from 11.09% to 25.28% during the same period. The proportion of adolescent girls from the poorest wealth index remained unchanged (20.05% in 2004 vs. 19.71% in 2017). A similar trend was found for adolescent girls from the richest wealth quintile (15.74% in 2004 to 14.78% in 2017). The provision of contraceptive use increased from 49.21% to 57.26% during the survey years. In addition, the proportion of delivering a child at an early age (12–15 years) decreased from 28.83% to 16.32%. The proportion of more than one childbirth during the adolescent period also decreased from 13.94% in 2004 to 6.48% in 2017.
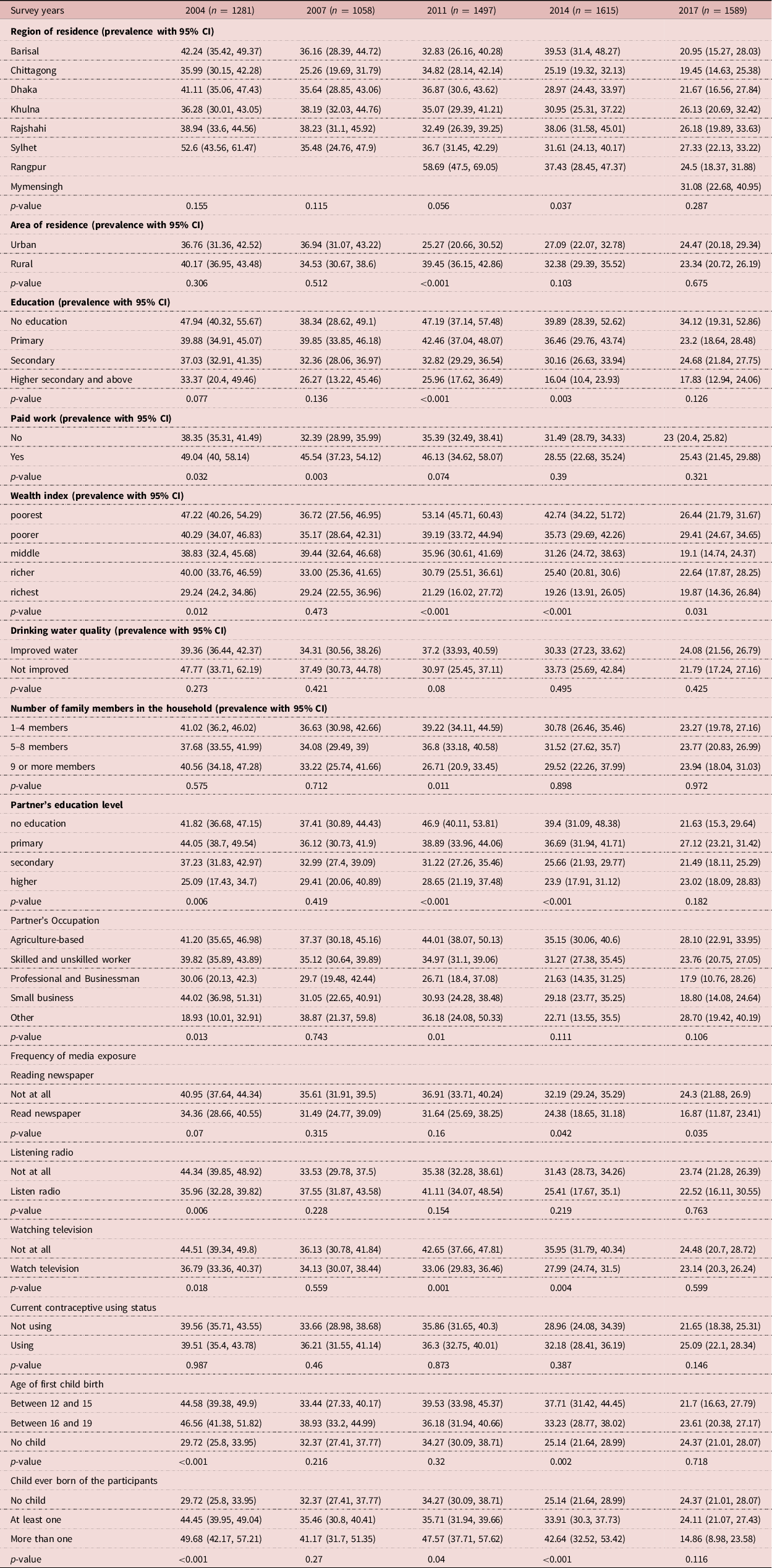
Table 1. Socio-Demographic Characteristics of the Participants in Survey Years From 2004 to 2017

* Rangpur division was officially formed in 2010 as the 7th administrative division; and
** Mymensingh division was formed in 2015 as the 8th administrative division of the country.
Prevalence of underweight among adolescent girls
Figure 1 describes the changes in the prevalence of underweight and overweight/obesity among ever-married adolescent girls over the survey years according to the country’s administrative divisions. Overall, the prevalence of underweight significantly decreased from 39.71% (95% CI: 36.85, 42.65) to 23.62% (95% CI: 21.35, 26.05) from 2004 to 2017 (p < 0.001).
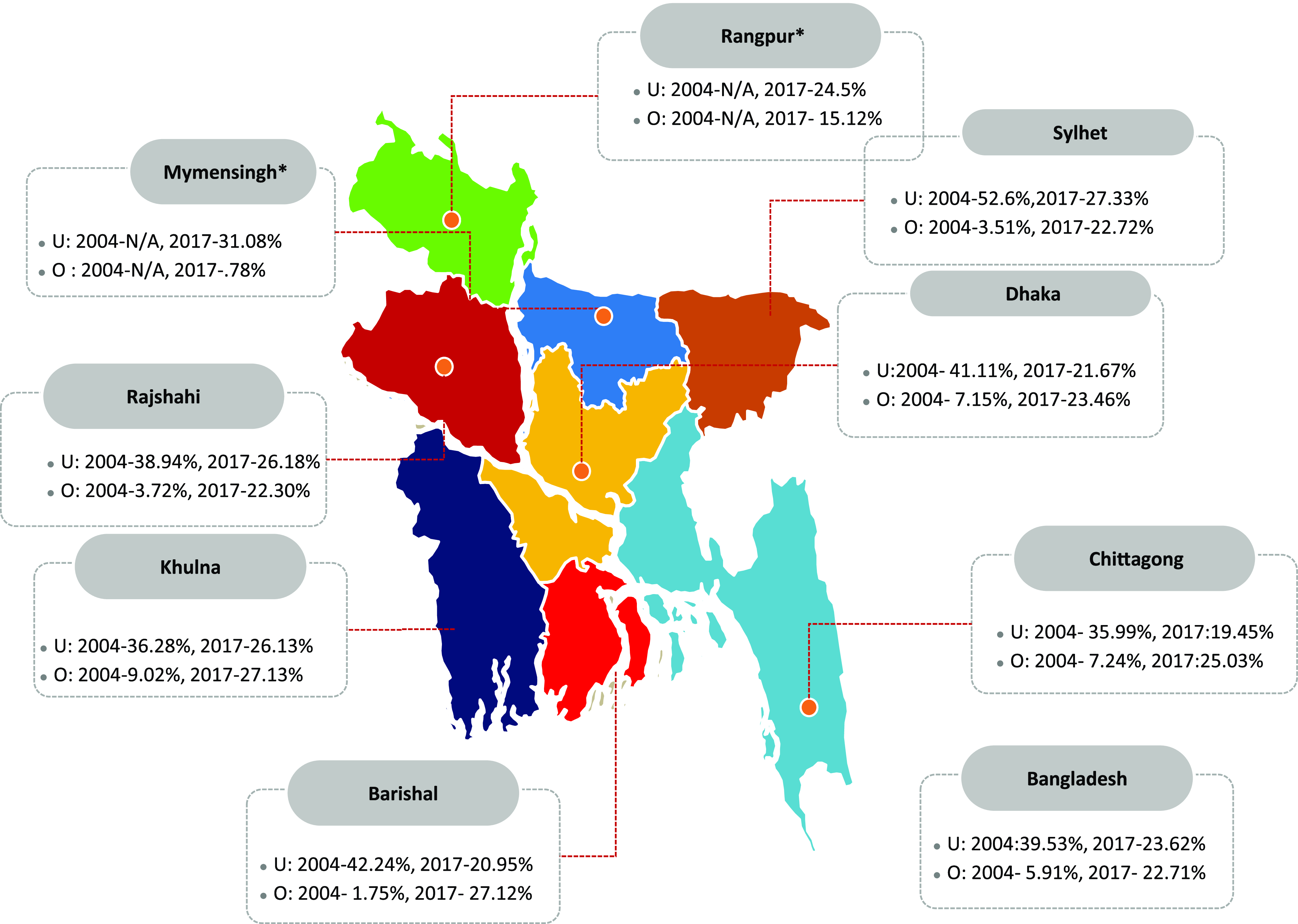
Figure 1. Prevalence of Underweight and Overweight/obesity Among Adolescent Girls.
Table 2 shows that the prevalence of underweight was significantly higher in Barisal division (39.53%, 95% CI: 31.4, 48.27) followed by Rajshahi (38.06%, 95% CI: 31.58, 45.01) division in 2014 (p = 0.037) and in 2017 this prevalence was higher in Mymensingh followed by Sylhet and Rajshahi, but this difference was not statistically significant. The prevalence of underweight was observed higher among the rural adolescents than those who lived in urban areas in 2004, 2011, 2014, and 2017, but only the differences in 2011 were found statistically significant (p < 0.001). Those who received no education had higher proportion of being underweight in 2004, 2011, 2014, and 2017, and the differences of 2011 and 2014 were statistically significant (p < 0.005). Similarly, the proportion was higher in 2011 and 2014 among the adolescent girls whose husbands received no education (p < 0.001). Adolescent girls who were not involved in any paid job had lower proportion of being underweight in 2004, 2007, 2011, and 2017 with significant differences in 2004 and 2011 (p < 0.05). Ever-married adolescent girls who came from the poorest wealth quintile had significantly higher prevalence of underweight in 2004, 2011, and 2014 (p < 0.05) and girls from poorer economic conditions had the highest prevalence of underweight in 2017 (p = 0.031). The prevalence of being underweight was significantly higher in adolescent girls married to agriculture-based professionals in 2011 (p = 0.01). Those who gave birth to their first child at 16–19 years of age had higher prevalence of being underweight in 2004, 2007, and 2017 whereas this prevalence was higher among the adolescent girls who gave birth to their first child at 12–15 years in 2011 and 2014. The differences between 2004 and 2014 were found statistically significant (p < 0.05).
Table 2. Prevalence of Underweight Among the Ever-Married Adolescent Girls in Survey Years From 2004 to 2014
Prevalence of overweight/obesity among adolescent girls
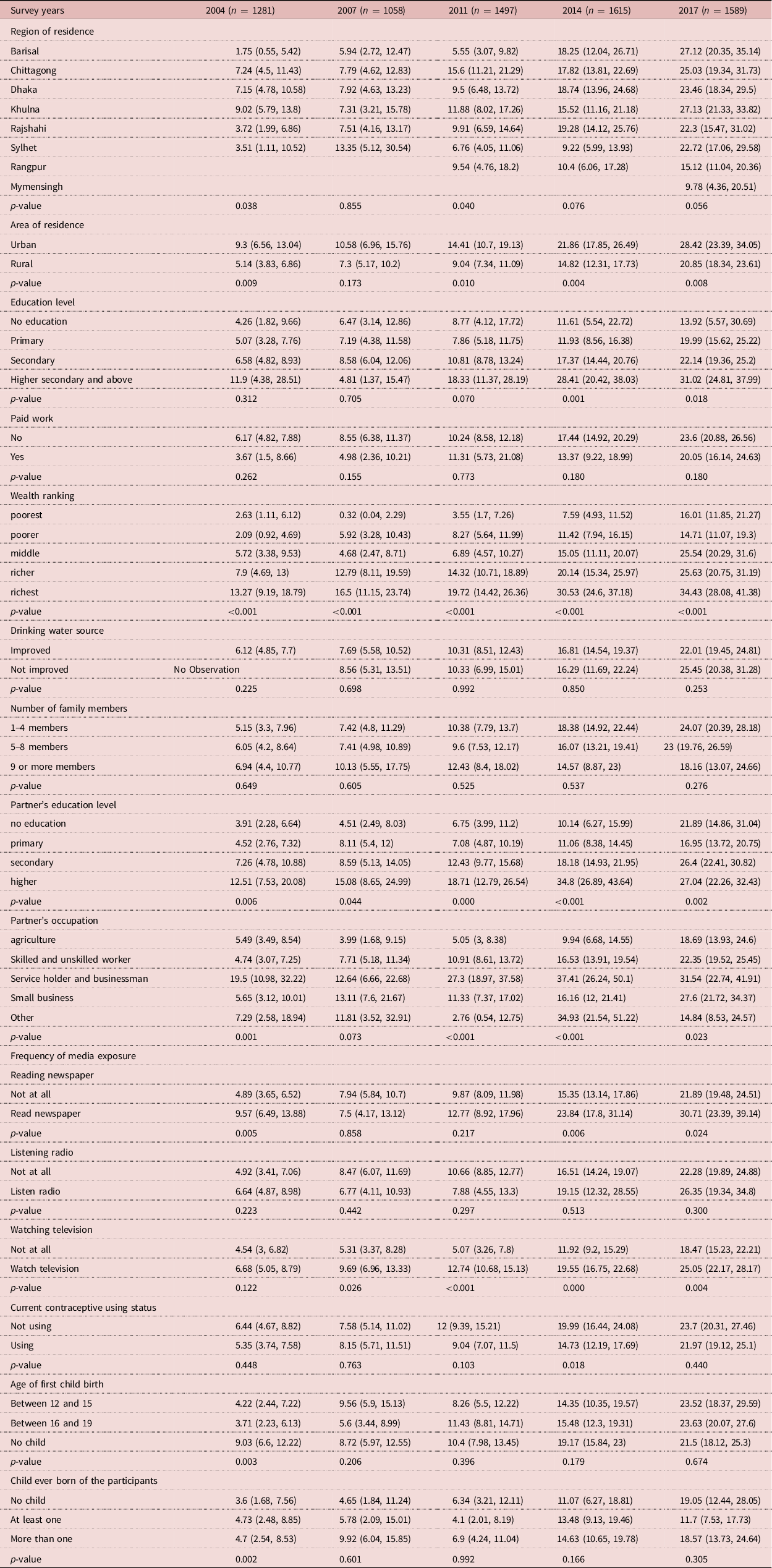
Figure 1 also shows that the prevalence of overweight/obesity among adolescent girls significantly increased from (5.9%, 95% CI: 4.67, 7.43) in 2004 to (22.71%, 95% CI: 20.39, 25.20) in 2017 (p < 0.01). The prevalence of overweight/obesity increased in all the divisions of the country over the past thirteen years (Table 3). In 2017, the prevalence of overweight was highest in Khulna division (27.13%, 95% CI: 21.33, 33.82) followed by Barisal (27.12%, 95% CI = 20.35, 35.14), and Chittagong (25.03%, 95% CI: 19.34, 31.73) divisions; and the differences were statistically significant for 2004, 2011. The prevalence of overweight/obesity in urban areas increased from (9.3%, 95% CI: 6.56, 13.04) in 2004 to (28.42%, 95% CI: 23.39, 34.05) in 2017. In the rural areas, the prevalence increased from (5.14, 95% CI: 3.83, 6.86) to (20.85%, 95% CI: 18.34, 23.61). Overall, the prevalence of having a BMI of more than 23 kg/m2 was higher in urban areas compared to rural areas at all the time points. However, the differences in 2004, 2011, 2014, and 2017 were statistically significant (p < 0.05). Ever-married adolescent girls who received higher education had significantly higher proportion of being overweight/obese in 2011 (18.33%, 95% CI: 11.37, 28.19, p = 0.070), 2014 (28.41%, 95% CI: 20.42, 38.03, p = 0.001) and in 2017 (31.02%, 95% CI = 24.81, 37.99, p = 0.018). Similar result was observed if their husband received higher education with significant differences in all the timepoints (p < 0.05). The proportion of overweight/obesity was significantly higher among adolescent girls coming from the richest wealth index in all the time points with statistically significant differences in 2004, 2007, 2011, 2014, and 2017 (p < 0.001). We also observed a higher prevalence of overweight/obesity among the adolescent girls who watch television compared to those who do not watch and the differences in 2011 (12.74 vs. 5.07, p < 0.001), 2014 (19.55 vs. 11.92, p < 0.001) and 2017 (25.05 vs 18.47, p = 0.004) were statistically significant. In 2014, the prevalence of overweight/obesity was lower in those using contraceptives (14.73 vs. 19.99, p = 0.018). Those who read newspaper regularly had significantly higher proportion of being overweight/obese in 2004 (9.57 vs. 4.80, p = 0.005), 2014 (23.84 vs. 15.35, p = 0.006), and 2017 (30.71 vs. 21.89, p = 0.024).
Table 3. Prevalence of Overweight/Obesity Among the Ever-Married Adolescent Girls in Survey Years From 2004 to 2014
Factors associated with underweight among ever-married adolescent girls in Bangladesh
Figure 2 shows the results of multinomial logistic regression analysis for factors associated with underweight among the ever-married adolescent girls in Bangladesh from 2004 to 2017. The adjusted model showed an inverse relationship between age and risk of being underweight among adolescent girls. The girls with a higher age were at low risk of developing underweight than their younger counterparts (OR = 0.94, 95% CI = 0.90, 0.99, p = 0.023). Urban residents were less likely to be underweight compared to rural population. This result was not statistically significant. The adolescent girls who received any form of education had a lower risk of being underweight than those who had no education with statistical significance for secondary (OR = 0.79, 95% CI = 0.64, 0.98, p = 0.032) and higher education (OR = 0.60, 95% CI = 0. 0.43, 0.83, p = 0.002). Adolescent girls from the poorer, middle, richer, and richest wealth index had significantly lower OR compared to girls from poorest families in the unadjusted model, but only the richest wealth index remained significant in adjusted model (OR = 0.78, 95% CI = 0.62, 0.98, p = 0.035). Adolescent girls with multi-parity, referring to more than one child, were more likely to be underweight (OR = 1.41, 95% CI = 1.15, 1.73 p = 0.001) than those with no child. Additionally, adolescent girls who gave birth to child between 16 and 19 years of age were more likely to be underweight (OR = 1.13, 95% CI = 0.97, 1.32, p = 0.064) compared to the girls who gave birth to child between 12 and 15 years old, although it was not statistically different.

Figure 2. Adjusted Odds Ratio (OR) for Factors Associated with Underweight and Overweight/Obesity Among Ever-Married Adolescent Girls in Bangladesh.
Factors associated with overweight/obesity among ever-married adolescent girls in Bangladesh
The multinomial logistic regression analysis (Fig. 2) showed that age was positively associated with having a higher BMI (OR = 1.22, 95% CI = 1.14, 1.32, p < 0.001). The urban adolescents were more likely to be overweight or obese than the rural girls (OR = 1.62, 95% CI = 1.36, 1.94, p < 0.001) in unadjusted model (Supporting Table 2) but became insignificant after adjusting the potential confounders. Adolescent girls from better economic status were more at risk of being overweight/obese than girls from poor economic status. Adjusted OR for being overweight/obese was significantly higher in girls from middle (OR = 1.65, 95% CI = 1.23, 2.22, p = 0.001), richer (OR = 2.1, 95% CI = 1.55, 2.85, p < 0.001), and richest (OR = 2.57 95% CI = 1.86, 3.55, p < 0.001) wealth quintiles. The girls who were married to an agricultural worker (OR = 0.60, 95% CI = 0.43, 0.84, p = 0.003), skilled or unskilled workers (OR = 0.58, 95% CI = 0.44, 0.77, p < 0.001), or to persons involved in small businesses (OR = 0.66, 95% CI = 0.49, 0.89, p = 0.007) had lower risk of having a high BMI. Girls who used contraceptive methods are less likely to be overweight/obese (OR = 0.8, 95% CI = 0.69, 0.94, p = 0.006) compared to the girls who didn’t use them. Those who gave birth to their first child between 16 and 19 years are less likely to be overweight/obese (OR = 0.77, 95% CI = 0.61, 0.97, p = 0.030) compared to their 12–15 counterpart. The risk of being overweight/obese was greater among the adolescent girls who had at least one child compared to those with no child, however, this association is not statistically significant.
Discussion
This study, involving data from past five demographic and health surveys over 13 years, found that the prevalence of undernutrition is declining, but the prevalence of being overweight/obese is increasing among the ever-married adolescent girls in Bangladesh. Although the proportion of being underweight is decreasing, almost one-fourth of the ever-married adolescent girls had a BMI less than 18.5 kg/m2 in 2017.
Our results indicate that both under- and over-nutrition are extant among the ever-married adolescent girls in Bangladesh. We observed that the prevalence of underweight among adolescent girls is decreasing, although the burden is still substantial. On the other hand, the prevalence of overweight/obesity is increasing significantly in the country. This finding is consistent with the studies conducted in neighbouring countries such as India, Pakistan, Nepal, and Myanmar (IIPS, Reference Iips2017; Macro, 2006). Studies showed that co-existence of both underweight and overweight/obesity – commonly referred to double burden of malnutrition (DBM) – is evident in low- and middle-income countries (LMICs), and Bangladesh is not an exception because of the nutritional transitions as well as changes in the food habits over the last couple of years (Das et al., Reference Das, Fahim, Islam, Biswas, Mahfuz and Ahmed2019; Kapoor and Anand, Reference Kapoor and Anand2002; Ramirez-Zea et al., Reference Ramirez-Zea, Kroker-Lobos, Close-Fernandez and Kanter2014; Sekiyama et al., Reference Sekiyama, Jiang, Gunawan, Dewanti, Honda, Shimizu-Furusawa, Abdoellah and Watanabe2015). It is evident that LMICs such as Vietnam, Indonesia, and Ghana are also experiencing nutritional transitions and suffering from the DBM (Doku and Neupane, Reference Doku and Neupane2015; Khan and Khoi, Reference Khan and Khoi2008; Winkvist et al., Reference Winkvist, Nurdiati, Stenlund and Hakimi2000). In India, the rate of overweight and obesity has increased from 2.4% to 4.2% within a time period of 10 years (2006–2016) among the adolescent girls (15–19 years), whereas the rate of undernutrition has declined from 46.8% to 41.9% in the same population during the same duration (IIPS, Reference Iips2017). The rate of overnutrition has been increased from 6.7% to 24.7%, and the prevalence of underweight decreased from 20.3% to 18.6% among the adolescent girls in Pakistan during 2013–2018 (Macro, 2006). The prevalence of overweight/obesity was 4.5% among the adolescent girls of Myanmar in 2016 (ICF, 2017). In Nepal, the proportion of being overweight/obesity among the same age population has increased from 2.1 to 3.3 during 2006–2016, and the prevalence of underweight in the same group has reduced from 30.3% to 25.8% from 2011 to 2018 (Macro, 2006). Perhaps, rapid urbanisation, economic development, consumption of less plant-based diets, more refined and energy-dense foods, and decreased physical activity are the factors responsible for the increasing trend of overnutrition and reduction of undernutrition among the adolescent girls in the South Asian countries including Bangladesh (Das et al., Reference Das, Fahim, Islam, Biswas, Mahfuz and Ahmed2019; El Kishawi et al., Reference El Kishawi, Soo, Abed and Muda2016).
In this study, we observed that education, wealth index, and parity were the factors found to be associated with being underweight. Additionally, adolescent girls from younger age group were more likely to be underweight. Previous study conducted in Bangladesh reported that poor dietary intake and discriminatory food allocation for females at household levels were responsible for higher prevalence of undernutrition among women (Kamal and Islam, Reference Kamal and Islam2010). It can be assumed that discriminatory behaviour towards the adolescent girls as well as less support from their family members to avail health care services are attributable to greater prevalence of underweight among ever-married adolescent girls in Bangladesh (Ahmed et al., Reference Ahmed, Adams, Chowdhury and Bhuiya2000; Kamal and Islam, Reference Kamal and Islam2010; Nguyen et al., Reference Nguyen, Sanghvi, Kim, Tran, Afsana, Mahmud, Aktar and Menon2017). Moreover, adolescent girls with lower academic qualifications and poorer economic conditions are more likely to have inadequate knowledge about healthy dietary practise and proper nutrition (Ahmed et al., Reference Ahmed, Adams, Chowdhury and Bhuiya2000; Kamal and Islam, Reference Kamal and Islam2010; Nguyen et al., Reference Nguyen, Sanghvi, Kim, Tran, Afsana, Mahmud, Aktar and Menon2017). This can be an explanation for higher nutritional ailment among the adolescents with less education and from poorest wealth index (Tareke and Abate, Reference Tareke and Abate2020). Studies conducted in Bangladesh and India identified that women of younger age, living in rural and urban slum areas, having a lower level of education and lower wealth index were more likely to suffer from different types of nutritional deficiencies (Goli et al., Reference Goli, Rammohan and Singh2015; Islam et al., Reference Islam, Islam, Bharati, Aik and Hossain2016; Subramanian and Smith, Reference Subramanian and Smith2006). Our study results are also analogous to those findings. Previous studies among young Bangladeshi women indicate that age at first marriage, age at first birth, and total number of children were important factors associated with nutritional status (Islam et al., Reference Islam, Islam, Bharati, Aik and Hossain2016; Khan and Kraemer, Reference Khan and Kraemer2009). Studies also indicate that economic status and education level are correlated with early childbirth and more number of childbirth (Islam et al., Reference Islam, Islam, Bharati, Aik and Hossain2016). Consistent with those reports, our study results also demonstrated that adolescent girls with low education, poorer economic condition, and multi-parity are more likely to be underweight.
The proportion of adolescent girls with a BMI of more than 25 kg/m2 was higher among those who were from richest wealth quintiles, dwellers of urban areas, received higher education, used contraceptives, read newspapers, and watched television regularly. We also observed that age of the respondents, place of residence, wealth index, partner’s occupation, contraceptive use, age of first child birth, and number of ever born child were the factors demonstrating significant relationship with overweight/obesity among the adolescent girls included in this analysis. A study conducted among Bangladeshi ever-married women showed that women from an older age group were more likely to be overweight (Biswas et al., Reference Biswas, Uddin, Al Mamun, Pervin and Garnett2017). We found that girls who were living in the urban areas and hailing from richer and richest wealth quintiles were more likely to be overweight/obese. Evidence shows that adolescent girls from the comparatively better economic conditions were more likely to be overweight and obese than the women who are from poorer economic status (Ly et al., Reference Ly, Ton, Ngo, Vo and Fitzpatrick2013; Ramesh and Jareena, Reference Ramesh and Jareena2009; Subramanian et al., Reference Subramanian, Kawachi and Smith2007, Reference Subramanian, Perkins and Khan2009). It is evident that better economic status is associated with an increased intake of energy and fat, and consumption of animal and processed foods, all of which were found to be associated with overweight and obesity (Du et al., Reference Du, Mroz, Zhai and Popkin2004). Studies confirmed that the prevalence of overweight/obesity among women is higher in the developing countries due to rapid urbanisation (Mendez et al., Reference Mendez, Monteiro and Popkin2005). Another study conducted in Bangladesh showed that the prevalence of overweight/obesity is higher among the urban residents (Tanwi et al., Reference Tanwi, Chakrabarty and Hasanuzzaman2019). Report shows that residents from the urban areas have access to advanced technology, which help them to perform daily activities without losing substantial amount of energy (Monteiro et al., Reference Monteiro, Moura, Conde and Popkin2004). A study documents that shift in dietary habits towards western foods containing high protein and energy may also contribute to the increase in BMI (Pingali, Reference Pingali2007). Urban people are more likely to consume readily available processed foods and avail better transportation system resulting in less physical activities, which ultimately contribute to increase in the prevalence of overweight obesity among them (Monteiro et al., Reference Monteiro, Moura, Conde and Popkin2004). Adolescent girls from comparatively richest economic conditions were more likely to be overweight/obese in our study. Previous studies conducted in Bangladesh also found the similar result (Tanwi et al., Reference Tanwi, Chakrabarty and Hasanuzzaman2019). Perhaps, adolescent girls from richer families have access to western diet with high ingredients of energy and proteins and that is responsible for an increasing trend of being overweight/obese among the ever-married adolescent girls from better economic conditions (Tareke and Abate, Reference Tareke and Abate2020). Our results highlight that adolescent girls married to workers and small business owners were less likely to be overnourished. This finding can also be linked with wealth index as workers or small entrepreneurs are expected to be from lower economic conditions. The findings on relationship between parity and overweight/obesity are also supported by previous reports (Heliövaara and Aromaa, Reference Heliövaara and Aromaa1981; Huayanay-Espinoza et al., Reference Huayanay-Espinoza, Quispe, Poterico, Carrillo-Larco, Bazo-Alvarez and Miranda2017). It is evident that weight gain during pregnancy enhances the risk of postpartum weight retention (Butte et al., Reference Butte, Ellis, Wong, Hopkinson and Smith2003; Linne et al., Reference Linne, Dye, Barkeling and Rössner2003). Perhaps, gestational weight gain and certain puerperal conditions could play a potential role in the pathogenesis of parity-related overnutrition. The finding on negative relationship between older age (16–19 years) at first childbirth and overweight/obesity is analogous to previous reports, although the underlying mechanism is not yet clear (We et al., Reference We, Han, Kwon and Kil2016). However, studies revealed that younger age at first childbirth is associated with multi-parity and restriction of physical activity (Gunderson et al., Reference Gunderson, Murtaugh, Lewis, Quesenberry, West and Sidney2004; Lao et al., Reference Lao, Thomas, Jiang, Zhang, Yin, Schooling, Heys, Leung, Adab and Cheng2006). Apart from behavioural and genetic factors, these could be the probable causes for developing overweight/obesity among the girls with early childbearing age. Our result also indicates that adolescent girls who used contraceptives had lower risk of being overweight/obese. Although it has been assumed that contraceptive use may have role in a high BMI, a study reported to have no association between use of contraceptives and BMI in women (Schraudenbach and McFall, Reference Schraudenbach and Mcfall2009). However, the negative relationship between contraceptive and overweight/obesity observed in this analysis can be a spurious finding and needs to be elucidated further. We have documented that adolescent girls who could avail entertainment facilities including newspapers and television had higher prevalence of being overweight/obese. This finding is consistent with previous studies done in South Asian countries including Nepal and India (Das Gupta et al., Reference Das Gupta, Haider, Hashan, Hasan, Sutradhar, Sajal, Joshi, Haider and Sarker2020; Das Gupta et al., Reference Das Gupta, Haider, Hashan, Hasan, Sutradhar, Sajal, Joshi, Haider and Sarker2019).
This is the first study to describe the trends and risk factors of overweight/obesity and undernutrition among the ever-married adolescent girls in Bangladesh using national data. The use of data from well-designed nationally representative surveys is the major strength of our analysis. Moreover, we can assure that the respondents included in this analysis are nationally representative because of the sampling strategy used in the BDHS. Therefore, we believe that the findings from this study would help the policymakers to yield proper initiative and take appropriate measures to fight against both under- and over-nutrition among the most vulnerable age group of the population. However, there are several limitations. We could only include the ever-married adolescent girls aged between 15 and 19 years in this analysis. The unmarried adolescent girls and those with an age between 10 and 14 years were not included owing to unavailability of data. Since the surveys were cross-sectional, the relationship between the exposures and outcome variables does not infer causality. Further studies are required to elucidate the causality of the risk factors identified in this study. Additionally, the BDHS data do not include information on nutrient intake as well as dietary diversity and physical activities of the adolescent girls, although these variables are considered to be important determinants of nutritional insufficiencies and malnutrition. Moreover, BMI – the indicator that we have used to determine nutritional status of the girls – cannot differentiate between fat and fat-free mass. However, BMI is a widely recognised indicator to assess nutritional status in adolescents and adults (Fahim et al., Reference Fahim, Das, Gazi, Alam, Mahfuz and Ahmed2020).
Conclusion
In conclusion, the results showed that the prevalence of overweight/obesity is increasing among the ever-married adolescent girls aged between 15 and 19 years in Bangladesh, while the prevalence of underweight is decreasing among the same population. Nevertheless, the burden of being underweight is still high among the rural residents, those who received no education and came from poorest wealth quintiles. The likelihood of overweight/obesity is higher among the urban dwellers as well as educated and richer population in Bangladesh. The existence of both of the spectrum of malnutrition may lead to adverse clinical consequences in later stage of life of the adolescent mothers as well as to an unfavourable growth of the future generation. Our results emphasise the necessity of effective public health approaches to address the issue of malnutrition among the ever-married adolescent girls in Bangladesh.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S0021932023000160.
Data availability statement
The dataset of BDHS 2004 to 2017 is available on the website of Demographic and Health Surveys Program. This is an open-source dataset, which is available on request at http://dhsprogram.com/what-we-do/survey/survey-display-349.cfm.
Acknowledgements
The authors used data from the open-access dataset of the Demographic and Health Survey (DHS) Program funded by the US Agency for International Development (USAID). icddr,b acknowledges with gratitude the commitment of USAID to its research efforts. icddr,b is also grateful to the Governments of Bangladesh, Canada, Sweden, and the UK for providing core/unrestricted support.
Funding statement
This research received no specific grant from any funding agencies.
Competing interests
The authors declare no competing interests.







