


1. Introduction
A large body of epidemiological studies suggests that breastfeeding is associated with significant health benefits for children. These benefits are wide ranging, including lower incidence of obesity, asthma, allergy, and respiratory illnesses; fewer infections of the gastrointestinal tract, middle ear, and urinary tract; and consequently lower rates of hospitalizations [American Academy of Pediatrics (1997), Quigley et al. (Reference Quigley, Kelly and Sacker2007), Bernard (Reference Bernard2018)]. Breastfeeding mothers are also found to be less likely to develop breast or ovarian cancer and to exhibit a lower incidence of type II diabetes [Ip et al. (Reference Ip, Chung, Raman, Chew, Magula, DeVine, Trikalinos and Lau2007)]. More recent research has found positive effects of breastfeeding on children's psychosocial and cognitive development [Sacker et al. (Reference Sacker, Quigley and Kelly2006), Heikkila et al. (Reference Heikkila, Sacker, Kelly, Renfrew and Quigley2011), Borra et al. (Reference Borra, Iacovou and Sevilla-Sanz2012), Del Bono and Rabe (Reference Del Bono and Rabe2012), Rothstein (Reference Rothstein2013)]. Empirical evidence suggests that breastfeeding may have long-term benefits. Adults who were breastfed experienced lower mean blood pressure and total cholesterol, lower prevalence of overweight/obesity, and type-2 diabetes as well as higher score in intelligence tests [Horta et al. (Reference Horta, Bahl, Martines and Victora2007)].
On the basis of this evidence, numerous public health agencies promote initiatives to increase the incidence and the duration of breastfeeding. The American Academy of Pediatrics (2005) recommends exclusive breastfeeding for the first 6 months of a child's life and then continued breastfeeding through at least the first year. The World Health Organization goes even further, recommending breastfeeding alongside solid foods for up to 2 years [World Health Assembly (2001)]. However, despite these efforts, rates of breastfeeding in most developed countries remain largely below the proposed targets. For example, in 2015, about 83% of mothers in the United States initiated breastfeeding in hospital. However, less than 50% of infants were exclusively breastfed through 3 months and about 25% were exclusively breastfed through 6 months (CDC, 2018). In the UK, in 2010, about 81% of mothers breastfeed soon after birth, but only 17% exclusively through 3 months and 1% through 6 months. Higher initial rates show that most mothers want to breastfeed and start out doing so but difficulties may emerge along the way. Breastfeeding is also a highly emotive subject in the UK because many families have not breastfed, or have experienced the trauma of trying very hard to breastfeed and not succeeding.
Barriers at the workplace might exacerbate the problem, contributing to many women's decision to stop breastfeeding long before what is the minimum period recommended. According to data from the 2005 UK Infant Feeding Survey (IFS), among women who are at work by the time the child is 4 months old the incidence of breastfeeding is 25%, while the corresponding percentage for non-working mothers is 34%. Similarly, at 6 months after birth only 16% of working mothers are still breastfeeding, against 27% of non-working mothers.
Public health campaigns aimed at promoting breastfeeding for mothers returning to work advocate breastfeeding support at the workplace and point out important potential benefits to employers: breastfeeding mothers may have lower absenteeism rates because their babies suffer from fewer illnesses, breastfeeding mothers who have access to breastfeeding facilities at work may return to work earlier, and employers who support breastfeeding at work may be more successful in retaining their employees [Maternity Alliance (1997)].
On the basis of these arguments in the past few years more than 40 states in the US have enacted breastfeeding-related legislation, and about half of them require employers to provide breastfeeding support at work through time breaks and designated facilities. In 2010 these requirements became entrenched in federal law.Footnote 1 Similar laws have existed for a long time in Norway, Sweden, and Denmark, and in countries such as Italy breastfeeding mothers have the right to request shorter working days up to 1 year after the birth of the child. By contrast, in the UK, there is no legal obligation for employers to offer breastfeeding facilities at the workplace. The Health and Safety Work Regulations 1999 indicate that a breastfeeding mother should have access to a safe place where to breastfeed or express and store breast milk, but this is seen as an example of good practice rather than a requirement for the employer.Footnote 2
To date, there is very little empirical research which investigates the effect of breastfeeding facilities at the workplace on mother's breastfeeding rates, their labor supply, and their children's health. So, it is unclear whether the benefits emphasized in public health campaigns do in fact accrue to employers. The main exception is a study on maternal absenteeism conducted in the US [Cohen et al. (Reference Cohen, Mrtek and Mrtek1995)], which found that infants of breastfeeding mothers exhibit fewer severe illnesses and rates of maternal absence up to three times lower than those of mothers with formulafed babies. Very few other studies have been carried out since, and no evidence is available for the UK or for countries other than the US.
Our paper's main contribution is to offer evidence on the potential benefits of workplace breastfeeding facilities and on maternal breastfeeding. Using data from the 2005 UK IFS, we model the association between the availability of breastfeeding facilities at the workplace and the duration of breastfeeding and maternity leave. We utilize a sample of UK mothers who have initiated breastfeeding and who return to work by the time their child is 9 months old.
We find that breastfeeding facilities are significantly associated with longer breastfeeding durations for all working mothers and shorter maternity leave spells for higher educated mothers. Our data allow us to control for a comprehensive set of characteristics of the mother, the child, and the employer, which however does not completely mitigate concerns about causality. To give robustness to our results, we will also perform some falsification tests. The effects we uncover are non-negligible, as mothers with access to employer-provided breastfeeding facilities have a 16–20 percentage points higher probability of breastfeeding and a 5–8 percentage points higher probability of working (only for higher educated mothers) at 4 and 6 months, respectively. Health effects are equally relevant. We look at the effect of longer breastfeeding on children's health, using breastfeeding facilities as instrumental variables. Here we find improvements in the first half year of life, but not later. Children born to mothers who breastfeed longer (due to access to breastfeeding facilities) exhibit lower incidence of health problems, including gastrointestinal problems, ear infections, and skin conditions, in the first months of life. Given the selection of our sample, our results are generalizable to a population of women relatively attached to the labor market and with some intention of breastfeeding their baby.
2. Previous literature
From an economic perspective, the negative relationship between breastfeeding and maternal employment is the result of the fact that breastfeeding is an activity which is intensive in maternal time and therefore in direct competition with other uses of it, including market work. This implies that the opportunity cost of breastfeeding can be measured in terms of the costs of absence from work.
Previous studies provide evidence of a significant negative relationship between maternal employment and breastfeeding durations. Most of the earlier studies assume that employment decisions are exogenous to breastfeeding [Kurinij et al. (Reference Kurinij, Shiono, Ezrine and Rhoads1989), Gielen et al. (Reference Gielen, Faden, O'Campo, Brown and Paige1991), Visness and Kennedy (Reference Visness and Kennedy1997), Fein and Roe (Reference Fein and Roe1998)]. More recent papers model the duration of breastfeeding and the duration of maternity leave as jointly determined, trying to identify the direction of causality using different methods. For example, Roe et al. (Reference Roe, Whittington, Fein and Teisl1999) implement an instrumental variable strategy using maternal occupation and availability of maternal leave as direct determinants of maternal employment but not of breastfeeding. They find negative and significant effects of work leave and work intensity (hours) on breastfeeding duration and intensity (number of breast-feeds per day). Chatterji and Frick (Reference Chatterji and Frick2005) use a family fixed-effect estimator, using variation in the duration of leave and breastfeeding across siblings. They find significant negative effects of maternal employment on both breastfeeding initiation and durations. In the most convincing attempt to date to get to the causal effect of maternal employment on breastfeeding duration, Baker and Milligan (Reference Baker and Milligan2008) exploit an exogenous increase in maternity leave entitlement brought about by a change in the legislation in Canada. Their results show that the 6-month increase in entitlement increased maternal breastfeeding durations by approximately 3–3.5 months.
Although the evidence indicates that maternal employment and breastfeeding are negatively correlated on average, they are not incompatible, and many working mothers do feed their children breast milk [Ortiz et al. (Reference Ortiz, McGilligan and Kelly2004)]. In fact, there is a great variety of feeding practices among working women. One way of explaining this diversity of arrangements is to look at differences in workplace characteristics. Indeed, breastfeeding studies often mention aspects of the workplace as potentially important in maintaining breastfeeding rates among working mothers. Among the most cited workplace characteristics in this context are the availability of on-site nurseries, extended breaks, facilities to express and store milk, lactation rooms, and lactation consultants or programs [Johnston and Esposito (Reference Johnston and Esposito2007), Mills (Reference Mills2009)].
Above all, the most relevant policy in terms of breastfeeding and (eventual) return to work is that related to the duration of maternity leave. Longer periods of maternity leave are associated with longer breastfeeding durations [Baker and Milligan (Reference Baker and Milligan2008), Chuang et al. (Reference Chuang, Chang, Chen, Hsieh, Hurng, Lin and Chen2010)] and with a higher probability of returning to work [Pronzato (Reference Pronzato2009)]. We therefore expect that the availability of breastfeeding facilities may interact with maternity leave entitlement in important ways. For example, the presence of breastfeeding facilities should be more relevant in relation to breastfeeding initiation in countries such as the US where maternity leave is very short, while it should affect mainly breastfeeding duration in European countries where maternity leave durations are usually much longer.
There is however little evidence of the effectiveness of workplace policies on both breastfeeding rates and durations among working women [Hawkins et al. (Reference Hawkins, Griffiths, Dezateux and Catherine2007), Jacknowitz (Reference Jacknowitz2008)], and some indication that the effects might not be the same for all groups [Chun Chen et al. (Reference Chun Chen, Wu and Chie2006)]. Kozhimannil et al. (Reference Kozhimannil, Jou, Gjerdingen and McGovern2016), using data from Listening to Mothers III (an US national survey of women ages 18–45 who gave birth in 2011 and 2012), find that women with both break time and private space were twice as likely to breastfeed exclusively up to 6 months. More recent papers [Spitzmueller et al. (Reference Spitzmueller, Wang, Zhang, Thomas, Fisher, Matthews and Strathearn2016), Scott et al. (Reference Scott, Taylor, Basquin and Venkitsubramanian2019), Wallenborn et al. (Reference Wallenborn, Perera, Wheeler, Lu and Masho2019)] look instead at the effect of a more supportive working environment in terms of perception, and find that women who perceive a breastfeeding supportive workplace are more likely to initiate and continue breastfeeding.
Even less attention has been paid to these policies' effects on women's labor force participation, either in terms of turnover, absenteeism, or length of maternity leave. Most of those who advocate that creating a breastfeeding-friendly workplace has benefits for employers refer to a study conducted by Cohen et al. (Reference Cohen, Mrtek and Mrtek1995), who carried out a comparison of breastfeeding and non-breastfeeding mothers' rates of absenteeism in two corporations implementing a lactation program. The authors found fewer and less severe infant illnesses and lower rates of maternal absenteeism among the breastfeeding group, but the study was not experimental and based on a very small sample of observations (101 participants in total).
Yet, establishing whether breastfeeding-friendly working environments could benefit employers as well as employees is very important. A substantial literature in personnel economics looks at the effects of family-friendly working practices on various outcomes, including rates of absenteeism and retention [Lehrer et al. (Reference Lehrer, Santero and Mohan-Neill1991), Brown and Sessions (Reference Brown and Sessions1996), Hill et al. (Reference Hill, Hawkins, Ferris and Weitzman2001), Heywood and Jirjahn (Reference Heywood and Jirjahn2004), Eldridge and Pabilonia (Reference Eldridge and Pabilonia2007)]. Analyzing what effect breastfeeding-friendly practices might have not only on breastfeeding rates or durations but also on aspects of female labor force participation is important in order to gauge who is going to bear the costs of the implementation of these policies and how likely they are to be implemented in the absence of legislation.
3. Data
The IFS was carried out every 5 years, from 1975 to 2010. The main aim of the survey was to provide estimates on the incidence, prevalence, and duration of breastfeeding and other feeding practices adopted by mothers in the first 8–10 months after their baby was born. The survey was based on an initial representative sample of mothers who were selected from all births registered during August and September/October of the relevant year in all UK countries.Footnote 3 Three stages of data collection were conducted with each survey; the first stage took place when babies were 4–10 weeks old, the second one when they were four to 6 months old, the third one when they were eight to 10 months old. At all stages mothers were asked to return a postal questionnaire.Footnote 4
The IFS is the only UK survey which provides information on the availability of breastfeeding facilities (either to express or to actually breastfeed) at work, from 2005. Other surveys which collect information on breastfeeding from individual mothers, such as the Avon Longitudinal Study of Parents and Children (ALSPAC) and Understanding Society, do not ask any questions about facilities provided by the employer which could facilitate the reconciliation of motherhood and work. The Millennium Cohort Study collects information on the availability of family-friendly policies, such as part-time work, shift work, or the availability of a crèche, but nothing specifically related to breastfeeding facilities.
Apart from providing information on incidence, prevalence (exclusivity), and duration of breastfeeding at various points in time, the survey is rich in other information related to breastfeeding. For example, mothers are asked about their breastfeeding intentions during pregnancy, their breastfeeding problems, and the type of breastfeeding support they received before and after the birth of their child. The survey also contains information about other infant feeding practices, such as the timing of introduction of cow's milk or solid foods. There is a well-structured section on pregnancy habits, including mother's drinking and smoking habits, and in more recent years a small section on child health. General demographic characteristics of the individual, such as mother's age at birth, level of education, and family size, are collected in the first stage. Information on maternal employment, including some characteristics of the place of work, are also collected at stage two and three: the size of the firm (through categories, from small firms of 1–24 workers to large small with more than 500 workers) and the occupational code (clustered in six categories: manager and professional, associate professional, administrative and secretarial, skilled trades and personal services, sales and customer services, plant machine and elementary operators).
One problem, however, is that the IFS 2005 and 2010 ask questions about the availability of breastfeeding facilities only of working mothers at stage two and stage three. That is, we do not know anything about the characteristics of the workplace for mothers who are still on maternity leave by the time stage three is carried out.Footnote 5 Ideally, we would like to have information on breastfeeding facilities for all mothers who are working during their pregnancy. This would allow us to analyze whether these workplace characteristics influence women's propensity to return to work after the birth of their child as well as the duration of their maternity leave. Given the constraint imposed by the data, we can only analyze whether the availability of breastfeeding facilities at the workplace is associated with a shorter period of maternity leave, and we can do so only on the sample of mothers who are at work in stage three, i.e., when their child is aged 8–10 months. The effect we can identify is therefore at the “intensive” margin. Presumably, at least some of those mothers who did not return to work and were excluded from our sample would have represented the “extensive” margin.
For our analysis, we will use the survey carried out in 2005, since we can observe a larger number of women returning to work by the 8–10th month of life of the child (around 50% of the sample). The change in the length of maternity leave from 6 to 12 months affects the probability of mothers being back to work in the 2010 survey, that would leave us only with less than 30% of the sample. Not only that, for women in 2005 the availability of breastfeeding facilities may be more crucial.
We now go through the selection of the sample employed for the analyses. Table 1 provides information on the sample selection process we follow in order to achieve our final sample of mothers. The initial sample interviewed at stage one consists of 12,290 women. From this we select only singleton births and drop a small number of observations with missing values on variables which are particularly important for our analysis, such as the age of the mother and her level of education. We are left with a sample of 11,728 mothers, 10,876 of whom have held a job in the past (88.5% of the original sample).Footnote 6
Table 1. Information about the sample and selection process
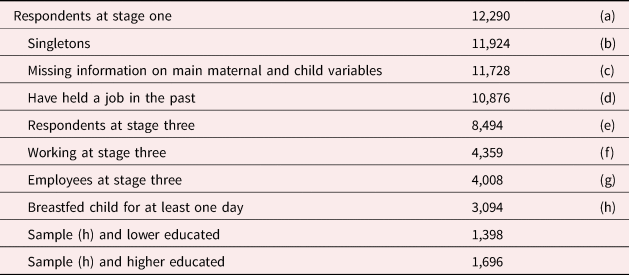
Note: Data from the 2005 UK Infant Feeding Survey. Description of sample size and selection process. Unweighted number of observations shown.
The subsequent selection is due to the fact that we need to restrict our analysis to women who reply to the stage three questionnaire. This implies a further drop in the number of observations, which is now down to 8,494 (69.0% of the original sample). Selecting only women working at stage three, and for whom we have information about employer-provided facilities reduces the sample to 4,359 observations, 4,008 of which are employees (32.6% of the original sample).
Finally, as we want to look at the association between workplace breastfeeding facilities and breastfeeding as well as the duration of maternity leave, we restrict our attention to mothers who have ever breastfed. This final selection takes the number of mothers in our data to 3,094 (25.2% of the original sample).
Table 2 describes the main variables of interest and provides further evidence that selection issues are not a cause concern. In particular, we compare sample (d) to sample (e) in order to consider the effect of attrition, since our analysis is restricted to women who respond to the third questionnaire. As we can see, at least in terms of breastfeeding initiation, mothers who respond to the third survey are very similar to all mothers interviewed in the initial sample. In terms of their characteristics, mothers in sample (e) are slightly older, more educated, and more likely to be married, but their mean number of children is very similar to that of the whole sample of mothers and so are the characteristics of their children. Restricting to women employees at stage three brings us to sample (g). Again, the characteristics of this sample are not very different from that of the general sample of women respondent at stage three [sample (e)]. The only important differences are in terms of breastfeeding and working behavior. As these women exhibit a stronger attachment to the labor market, they are not surprisingly also found to be less likely to breastfeed and more likely to work at 4 and 6 months than the general sample of women who respond to the stage three questionnaire.Footnote 7
Table 2. Descriptive statistics and analysis of selection process
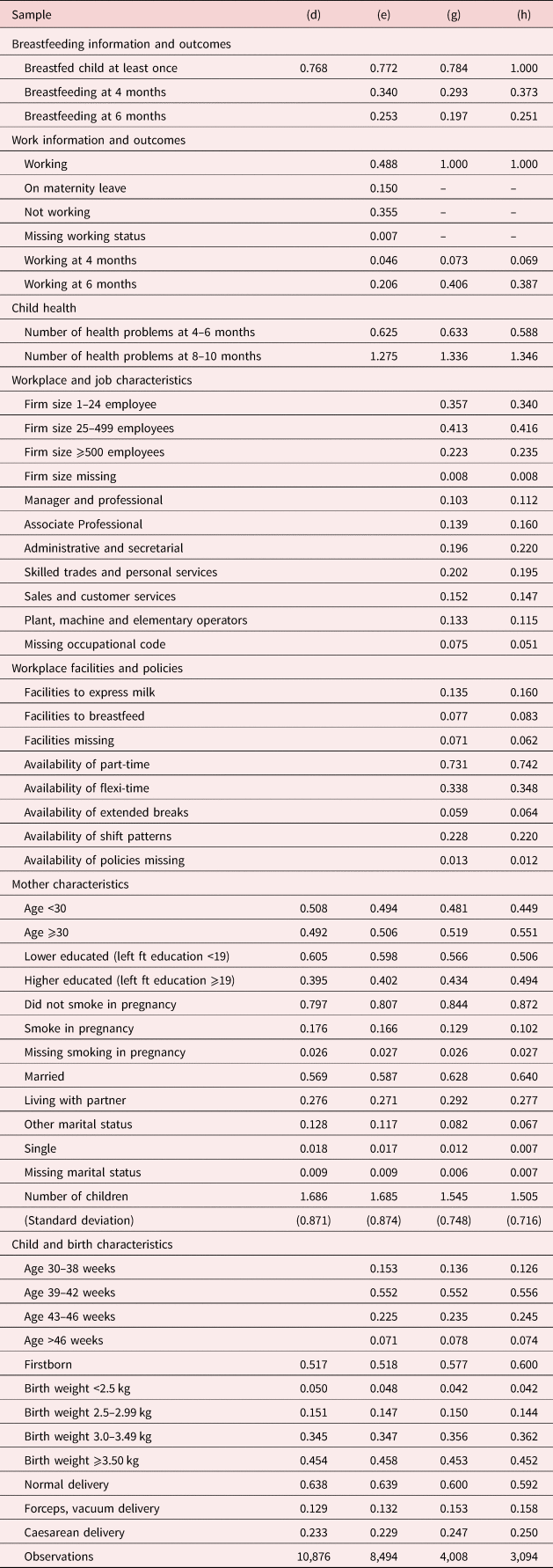
Note: Data from the 2005 UK Infant Feeding Survey. Distribution of different samples according to characteristics of the mothers, the children, and the jobs. As most of the variables are binary indicators or categorical variables, only the weighted frequencies are reported. Where the variable is continuous (number of children), we report the weighted mean and the standard deviation. Weights are survey weights which take into account differences in the probability of selection for mothers in different countries, for mothers without partners, and for differential non-response at each stage of the survey.
We finally compare sample (g) to sample (h), as we include in our analysis only women who have at least tried to breastfeed once. Here we see that the incidence of breastfeeding at 4 and 6 months increases, the probability of having returned to work by 4 and 6 months slightly decreases, while the probability of experiencing any health problem remains almost unchanged, with only a slight decrease at 4 months.Footnote 8 However, the general characteristics of the mothers and the children remain very similar. For these two samples it is also interesting to compare the characteristics of the job and the availability of facilities and policies which might facilitate combining work and breastfeeding. If we were to observe statistically significant differences in the distribution of the sample according to these variables we might suspect that mothers with a propensity to breastfeed select themselves into jobs or firms with different facilities/policies. As we can see, although there are small differences, these are not statistically significant. In general, therefore, the selection process does not represent a cause of concern.
We perform our analysis on the whole sample of individuals thus selected, and on the subsamples of mothers with lower and higher levels of education separately. This is because there are likely to be important differences in breastfeeding and working behavior for these two groups of women which is important to take into account. In particular, it is well-known that breastfeeding rates are higher for more educated women and that this group also tends to breastfeed for longer periods of time. At the same time, more educated mothers generally exhibit a stronger attachment to the labor force. So, we might expect that the availability of breastfeeding facilities is more important for this group.
Table 3 explores differences in characteristics and behavior of higher and lower educated mothers in some detail. First, we look at labor market status at stage three to analyze whether we observe statistically significant differences in the probability of going back to work by the time the child is aged 8–10 months between these groups. Indeed, panel A shows that 53% of highly educated mothers are working at stage three, against 45.9% in the lower education group. This difference is explained by the fact that lower educated mothers are 1.5 times more likely to be inactive than higher educated mothers while higher educated mothers enjoy longer periods of maternity leave. As we can see from the χ 2 statistics, these differences in labor market status at stage three are statistically significant at the 1% level.
Table 3. Differences between mothers according to education
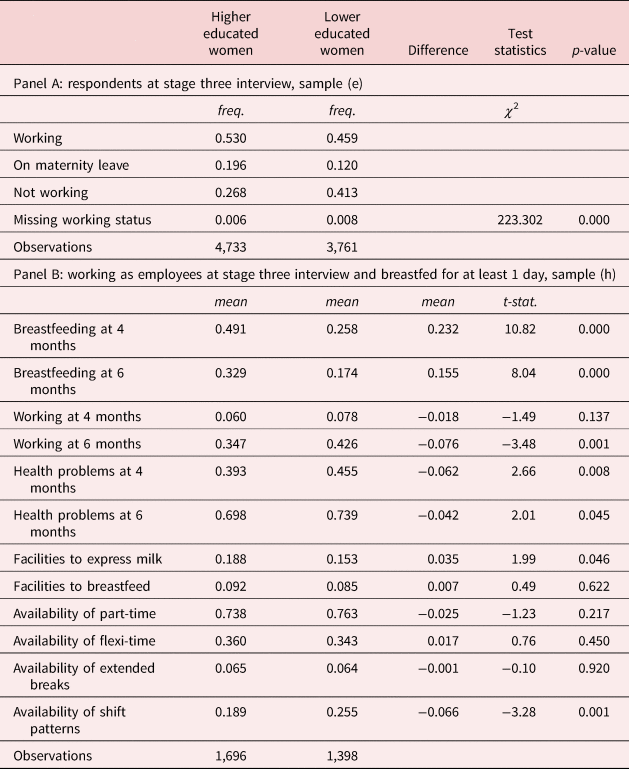
Note: Data from the 2005 UK Infant Feeding Survey. Differences in the distribution of outcome variables and variables capturing the availability of facilities and family-friendly policies according to mothers' education. Panel A shows difference in mothers' labor market status at stage three and reports a χ 2 test with 3 degrees of freedom. Panel B reports means and differences in duration of breastfeeding and maternity leave by level of education for the sample of mothers who work as employees at stage three and have breastfed for at least one day. A t-test of the difference in means is provided with associated level of significance. When looking at facilities and family-friendly policies we restrict the sample to non-missing observations on these variables. Data are weighted using survey weights (see notes to Table 2).
Panel B of Table 3 considers differences by level of education in the outcome variables (breastfeeding behavior, working status, and child's health at 4 and 6 months) and in the availability of facilities and family-friendly policies among mothers who are observed working in stage three and have at least some experience of breastfeeding [sample (h)]. The most significant differences between these two groups are found in respect of breastfeeding behavior. As we can see, more highly educated mothers are 23.2 percentage points more likely to breastfeed at 4 months and 15.5 percentage points more likely to breastfeed at 6 months. There are also some smaller but significant differences concerning child's health: the probabilities of experiencing any health problem are lower for children of higher educated mothers (6.2 percentage points less likely at 4 months and 4.2 percentage points less likely at 6 months). Finally, there are significant differences in relation to the duration of maternity leave, but only when the child is 6 months old: conditioning on working at stage three, less educated mothers are 7.6 percentage points more likely to be at work. Differences in working status at 4 months are not significant.
Next, we look at the availability of breastfeeding facilities. This is because higher educated mothers might be in better jobs or firms, and therefore enjoy better access to employer-provided facilities. As we can see, while the difference in the probability of having access to facilities to express milk is statistically significant, the magnitude is quite small, with higher educated mothers being only 3.5 percentage points more likely than lower educated mothers to have access to these facilities. Notice also that there is almost no difference in access to facilities to breastfeed. In terms of other family-friendly policies, we see almost no differences in these groups. The main exception is related to the availability of shift patterns, which is more common for lower educated mothers.
Taken together, the evidence presented in Table 3 shows that the main difference between lower and higher educated mothers is in their observed breastfeeding duration and observed length of maternity leave. More educated mothers are much more likely to breastfeed for longer periods of time than less educated mothers, and enjoy longer maternity leave spells. We therefore expect that the availability of breastfeeding facilities might help mainly this group of women to reconcile breastfeeding with work.
4. Empirical strategy
Previous literature has focused on the effect of family-friendly workplace characteristics on the probability of breastfeeding [Chun Chen et al. (Reference Chun Chen, Wu and Chie2006), Hawkins et al. (Reference Hawkins, Griffiths, Dezateux and Catherine2007), Jacknowitz (Reference Jacknowitz2008)]. In this work, we want to consider the problem from an additional angle, taking an employer's perspective. In order for employers to offer breastfeeding facilities or family-friendly policy schemes to their employees (at no additional cost to them) there has to be a return in terms of (i) lower turnover or (ii) increased labor force participation either in terms of shorter maternity leave or lower absenteeism.
As explained in the previous section, our data do not contain data on turnover or absenteeism. Using the IFS data, however, we can analyze whether the presence of breastfeeding facilities and the availability of family-friendly workplace policies, such as the presence of part-time or flexitime arrangements, has an impact on the working status of the mother, and in particular on the length of her maternity leave.
We start from a model in which the decision to go back to work and the decision to breastfeed are simultaneously determined. That is, we have a system of equations specified as follows:


where W i* and B i* are two unobserved random variables capturing the propensity to work and breastfeed after the birth of the child, X i is a vector of mother and child-specific variables, WC i is a vector of workplace characteristics and β 1, β 2, γ 1, and γ 2 are vectors of unknown parameters and δ 1 and δ 2 are scalars of unknown parameters. It is further assumed that { 1i, 2i} are i.i.d. bivariate normal variables. As mentioned, we identify the effects at the intensive margin, for a sample of women who have started breastfeeding and who return to work when the baby is 8–10 months old.
Contrary to what is commonly assumed, no exclusion restrictions are needed to identify the model [Heckman (Reference Heckman1978), Wilde (Reference Wilde2000)]. However, it is good practice to identify the effect of the endogenous regressors using at least one exclusion restriction. So, we would need to find a variable which affects the decision to breastfeed directly but has no impact on the decision to work if not through breastfeeding. Similarly, we would need to find another variable which affects the mother's labor force status but does not exert a direct effect on breastfeeding. In the absence of plausible identifying restrictions, the only model we can estimate is a reduced-form model:


where the parameters are a combination of the structural parameters of interest. In particular, the main vector of parameters we are interested in, γ̃1, will capture the direct effect of breastfeeding facilities on W i*, γ 1, as well as the indirect effects of these facilities on W i* which operate through breastfeeding, δ 1γ 2. Similarly, the vector of parameters γ̃2 will be a combination of the direct effect of the policies on breastfeeding, as well as its indirect effect through labor market participation.
Assuming that facilities to encourage breastfeeding at work have a positive direct impact on breastfeeding (γ 2 > 0), and that breastfeeding and employment status are negatively correlated (δ 1 < 0), the estimated reduced-form parameters capturing the association between facilities and working will be a lower bound of the true effects of interest.
Both * and W i* are latent variables for which only the dichotomous variables W i and B i can be observed:

Using this information, and further assuming that the error terms υ 1i and υ 2i follow a bivariate standard normal distribution:

leads us to estimate the model in (3)–(4) via a bivariate probit [Greene (Reference Greene1993)].
In order to estimate the effect of breastfeeding duration on child's health, we use the following equation:

where Si is the sum of childhood diseases experienced by the child. B represents the endogenous choice of breastfeeding, which is instrumented by the availability of breastfeeding facilities at the place of work. As the dependent variable is the number of childhood diseases, coefficients will be estimated via a Poisson model.
5. Results
5.1 Work and breastfeeding durations
The first results are presented in Tables 4 and 5. Here we show estimates of bivariate probit models where the dependent variables are the probability of breastfeeding and being at work at 4 and 6 months, respectively.Footnote 9 Given that the presence of breastfeeding facilities might be correlated with the availability of other workplace policies aimed at reconciling work and motherhood, we first estimate models in which only one type of facility or policy is included (panel A), and then a model in which we consider the availability of any breastfeeding facilities (either to express or breastfeed) and the availability of other workplace practices at the same time (panel B).
Table 4. Effects of facilities to breastfeed and family-friendly policies on the probability to breastfeed and the probability to be at work at 4 months
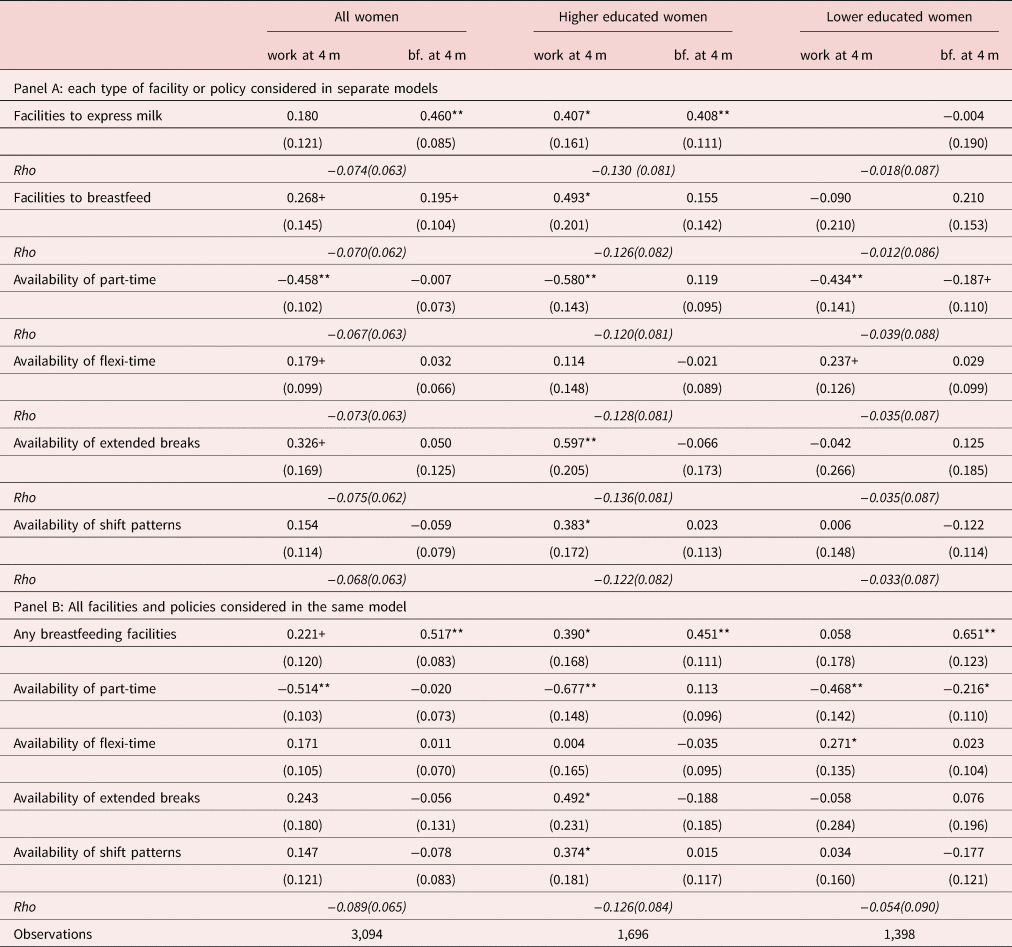
Note: Data from the 2005 UK Infant Feeding Survey. Bivariate probit model estimated through maximum likelihood. Dependent variables are: probability to be at work and probability to be breastfeeding at 4 months. Panel A reports results from separate models in which only one type of facility or policy is included. Panel B reports results from a single model in which the availability of any breastfeeding facilities and of all the family-friendly policies are included at the same time. All models control for the set of maternal, child and work characteristics reported in Table 2, as well as a complete set of regional dummies and dummies derived from an index of local area deprivation (Acorn). Coefficients and heteroscedasticity-robust standard errors (in parentheses) shown. Estimation takes into account survey weights (see notes to Table 2). Symbols: +significant at 10% level, *significant at 5% level, **significant at 1% level.
Table 5. Effects of facilities to breastfeed and family-friendly policies on the probability to breastfeed and the probability to be at work at 6 months
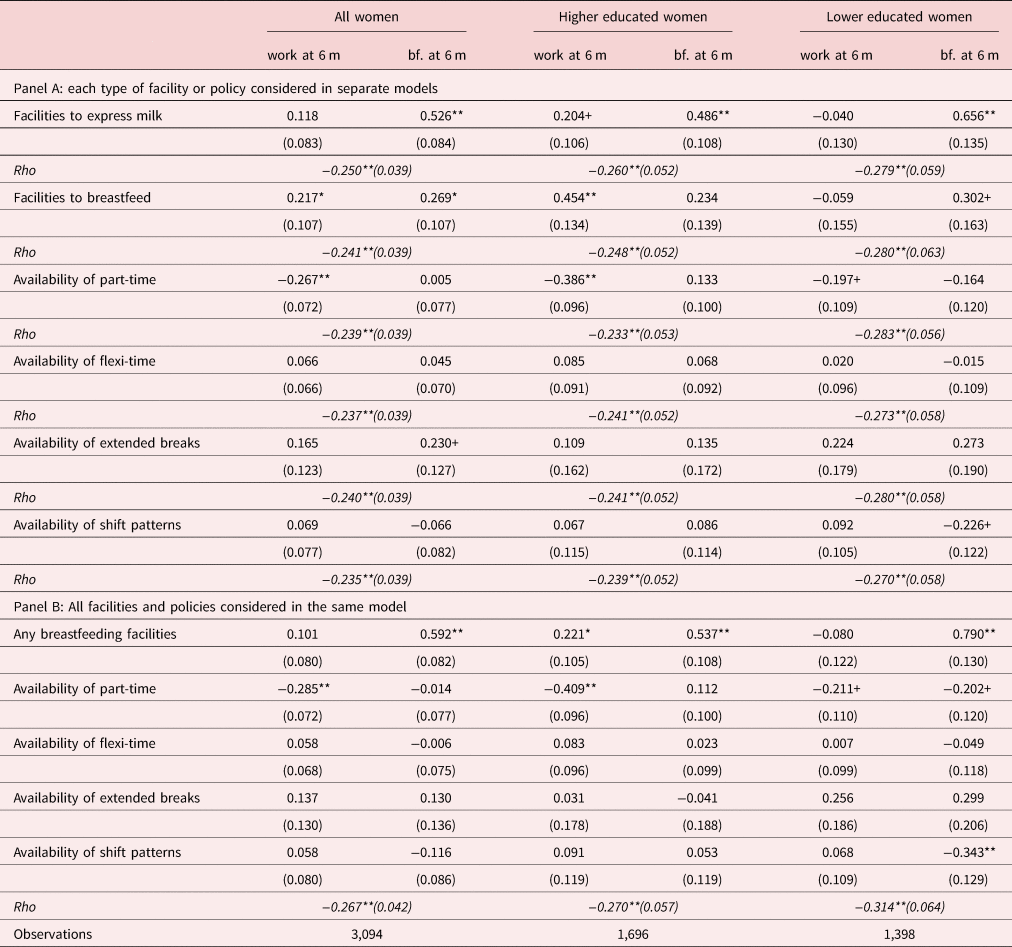
Note: Data from the 2005 UK Infant Feeding Survey. Bivariate probit model estimated through maximum likelihood. Dependent variables are: probability to be at work and probability to be breastfeeding at 6 months. Panel A reports results from separate models in which only one type of facility or policy is included. Panel B reports results from a single model in which the availability of any breastfeeding facilities and all the family-friendly policies are included at the same time. All models control for the set of maternal, child, and work characteristics reported in Table 2, as well as a complete set of regional dummies and dummies derived from an index of local area deprivation (Acorn). Coefficients and heteroscedasticity-robust standard errors (in parentheses) shown. Estimation takes into account survey weights (see notes to Table 2). Symbols: +significant at 10% level, *significant at 5% level, **significant at 1% level.
All models are first estimated on the entire sample of women, and then separately for higher and lower educated women. All the specifications control for characteristics of the mother and child, as well all the aspects of the job and firm we observe in our data (see Table 2). The latter variables are particularly important in this context. Variables which control for job characteristics (such as the occupational code) and firm characteristics (such as the firm size) help us to account for other aspects of the job and the employer which might be associated with the presence or availability of breastfeeding facilities and family-friendly policies and therefore help identifying the effects of interest. In addition, we also control for regional dummies and a full set of dummies measuring the level of deprivation of the area (17 Acorn groups).Footnote 10
We start by looking at Table 4, which presents the results for the dependent variables measured at 4 months. Looking at the effect of “facilities to express milk” (observed for 16% of the sample) on the probability of working, we see that there are no significant associations here, except in the sample of higher educated mothers where the coefficient is positive and statistically different from zero. By contrast, there is always a positive and very strong correlation between facilities to express milk and the probability of breastfeeding at 4 months. The second row of results considers “facilities to breastfeed”, which are observed for 8.3% of mothers. Again, we find a positive and statistically significant association with mothers' labor market participation for higher educated women, but a weaker relationship with breastfeeding durations. These weaker results might be due to the fact that these types of facilities are relatively uncommon and require bringing the child to work which is probably not a feasible strategy for many women.
In the subsequent rows of panel A, we consider the effect of different types of family-friendly policies, including the availability of part-time, flexi-time, extended breaks, and shift patterns.Footnote 11 Here we find a strong and negative association between the availability of part-time and the probability of going back to work, which might reflect undesirable characteristics of the jobs (low level of control, e.g.) which we are unable to capture in our vector of controls or could be a consequence of the fact that women with lower attachment to the labor force choose jobs with easy access to part-time. We also find a positive correlation between the availability of extended breaks and the probability of working at 4 months for higher educated women. The effects of this type of workplace policy on the probability of breastfeeding are however statistically insignificant.
In panel B of Table 4 we include in our specification the availability of any breastfeeding facilities (either to express milk or breastfeed) as well as the availability of other workplace policies.Footnote 12 What we intend to do here is to use the availability of other family-friendly policies at the workplace as implicit indicators of the characteristics of the job, rather than variables of interest per se. The idea is that if breastfeeding facilities are correlated with positive aspects of the job or the employer, controlling for other types of family-friendly policies should take this into account. As we can see, the positive association between breastfeeding facilities and mother's labor force participation is still statistically significant after the introduction of these other controls. As in the previous panel, this is so only for more educated mothers. Similarly, we find again a positive association between breastfeeding facilities and breastfeeding durations is relevant for all women, irrespective of their level of education.
The table reports also the estimate of the rho, the correlation between the residuals. This is always negative, higher in magnitude among the more educated group, but always statistically insignificant. The latter result is due to the fact that there is a very small percentage of women who go back to work at 4 months (about 7%, as shown in Table 2), so that most women are both not working and not breastfeeding (about 57% of the sample), while very few are at work and not breastfeeding (about 4.5%) at this point in time.
A much larger proportion of women—about 41%—is at work by the time the child is 6 months. Moreover, the minimum recommended duration of exclusive breastfeeding according to the World Health Organization is 6 months [World Health Assembly (2001)]. Therefore 6 months is an important point in time to consider. The results are presented in Table 5, and show that the main findings are exactly the same as discussed for the 4 months threshold. The main exception here is that the association between the availability of “facilities to express milk” and mothers' working status is slightly less significant than at 4 months, although as we can see in panel B access to any breastfeeding facilities is still associated with mothers' return to work at the conventional level of significance. Also, we generally find no significant association between the availability of other family-friendly practices and either maternal labor supply or breastfeeding, with the exception of part-time work. Finally, the residual correlation between the probability to breastfeed and the probability to work, captured by the estimated rho, is now statistically significant and indicates clearly that the two processes are not independent of one another.
The coefficients in a limited dependent variable model are useful only insofar as they give an idea of the sign and the level of statistical significance of the effect of interest. In order to consider the magnitude, it is necessary to take into account the distribution of the dependent variable. As we have two dependent variables in this case, several effects of interest could be considered, according to whether we want look at the joint, marginal, or conditional probabilities.
Table 6 presents some of these calculations. In particular, we consider the effect of having access (vs. not having access) to any breastfeeding facilities on: (i) the marginal probability of working, (ii) the marginal probability of breastfeeding, (iii) the joint probability of working and breastfeeding, and (iv) the conditional probability of working given that breastfeeding takes place. We calculate these effects using the specification in panel B of Tables 4 and 5, and setting the availability of all the other family-friendly working practices to zero.
Table 6. Marginal effects of having access to any breastfeeding facilities
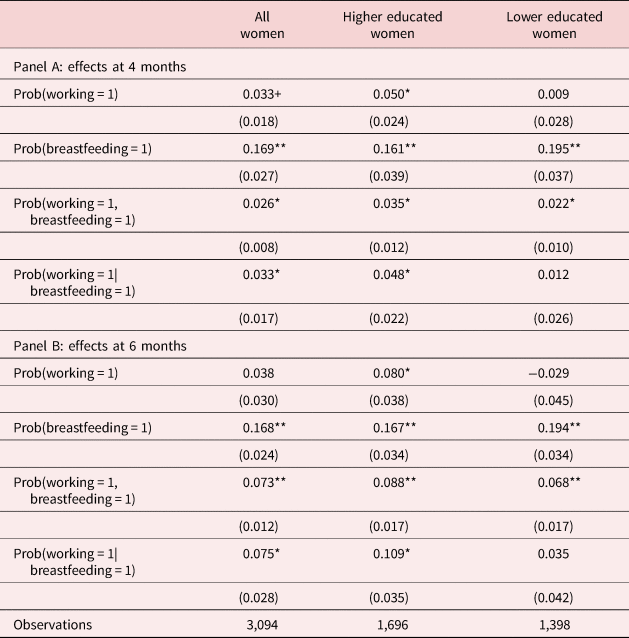
Note: Data from the 2005 UK Infant Feeding Survey. Marginal effect of the availability of any breastfeeding facilities on the marginal, joint, and conditional probabilities of working and breastfeeding. All other family-friendly policies are set to be zero for these calculations. The effects are estimated using the models presented in panel B of Tables 4 and 5. Estimation takes into account survey weights (see notes to Table 2). Symbols: +significant at 10% level, *significant at 5% level, **significant at 1% level.
The first two rows of each panel reflect closely the results shown in the previous tables, in that the availability of breastfeeding facilities is found to affect the probability of working only among more educated women. The effect is of a 5 percentage increase in the probability of working at 4 months and an 8 percentage increase in the probability of working at 6 months. By contrast, the effect of breastfeeding facilities on the probability to breastfeed is significant for all groups of women, and much larger in magnitude, about 16–19.5 percentage points. Here there is relatively little difference in the magnitude of the effect at 4 or 6 months, but some indication that the effect is larger for lower educated mothers. The third row reports the effects on the joint probability of breastfeeding and working, and is therefore a combination of the above effects.
One of the aims of this paper is to consider whether the availability of facilities to breastfeed could be of benefit to employers in terms of, for example, an increase in labor force participation of mothers through shorter maternity leave spells. In statistical terms this means that we might want to look at how the conditional probability of working, given breastfeeding, is affected by the availability of breastfeeding facilities. This could be interpreted as the effect of breastfeeding facilities on the probability of working for those mothers who have a strong propensity to breastfeed. Table 6 therefore shows the effects of the availability of any breastfeeding facilities on this conditional probability at 4 and 6 months. We see that if a breastfeeding woman were offered facilities to breastfeed, the probability that she would be working at 4 months after birth would increase by 3.3 percentage points overall. For higher educated women this effect is about 4.8 percentage points, while there is no effect on lower educated women. At 6 months, making breastfeeding facilities available to all breastfeeding mothers is associated with an increase of 7.5 percentage points in their employment rate at 6 months, which is largely driven by an increase in the employment rate of higher educated mothers of almost 11 percentage points.
5.2 Child health
In Table 7, we report results concerning the effect of breastfeeding duration on child's health. Our indicator of child health is the sum of childhood diseases experienced up to the time of the interview: for the second interview (first column), it expresses the number of diseases experienced by the child in her/his first 4–6 months of life; for the third interview (second column), the number of diseases experienced in her/his first 8–10 months of life. We select the health conditions most frequently thought to be affected by breastfeeding [American Academy of Pediatrics (1997), Quigley et al. (Reference Quigley, Kelly and Sacker2007)]: experience of (i) diarrhea, (ii) constipation, (iii) ear infection, (iv) eczema, (v) rash, (vi) congestion, and (vii) thrush. As shown in Table 2, the number (and the variety) of childhood diseases increases in the second half of the first year of life, going from an average of 0.59 to 1.35.
Table 7. Effects of breastfeeding on child health
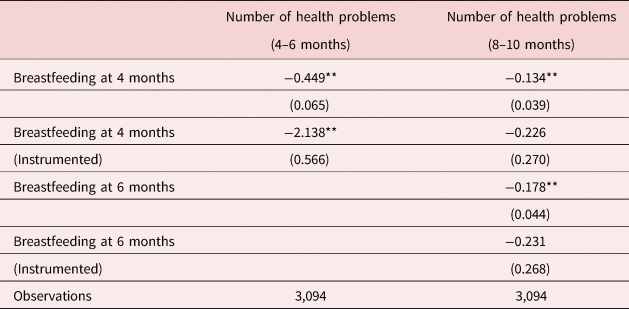
Note: Data from the 2005 UK Infant Feeding Survey. The model is estimated via a Poisson model. Dependent variables are the sum of childhood diseases experienced by the child: (i) diarrhea, (ii) constipation, (iii) ear infection or (iv) eczema, (v) rash, (vi) congestion, (vii) thrush. All models include dummies for the presence of other family-friendly policies and additionally control for the set of maternal, child, and work characteristics reported in Table 2, as well as a complete set of regional dummies and dummies derived from an index of local area deprivation (Acorn). Estimation takes into account survey weights (see notes to Table 2). Symbols: +significant at 10% level, *significant at 5% level, **significant at 1% level.
As breastfeeding indicators, we utilize our main variables of interest: breastfeeding at 4 and 6 months. We solve the problem of the endogeneity of the choice of breastfeeding by using breastfeeding facilities in the place of work as an instrumental variable.
Table 7 reports the estimated coefficients of breastfeeding at 4 months when the child is 4/6 and 8/10 months old, and of breastfeeding at 6 months when the child is 8/10 months old. We generally find negative correlations: breastfed children experience fewer diseases. However, in terms of strength and causality, only breastfeeding at 4 months seems to matter for health in the first 4/6 months of life. The number of childhood diseases decrease, on average, from 0.69 to 0.44 (corresponding parameter: −0.449**). The estimated effect, as indicated by the IV model, is even larger, though less precisely estimated.Footnote 13
6. Endogeneity of workplace characteristics
One important issue we still need to address is the potential endogeneity of workplace characteristics, in particular of breastfeeding facilities. Women who have a high propensity to breastfeed might choose jobs with facilities that make it easier to continue breastfeeding while working at the same time. If this were the case, then our estimates of the impact of breastfeeding facilities on both breastfeeding and return to work would be biased upwards. More generally, if women with different propensities to breastfeed choose their jobs or employers on the basis of the workplace policies they offer, then the coefficients on the availability of these workplace policies (as well as all the other coefficients) in the model will be inconsistently estimated.
The IFS collects information about women's breastfeeding intention during pregnancy. The survey also asks whether the mother herself was breastfed as a child, and whether she is aware of the benefits of breastfeeding. All these variables are collected at stage 1, i.e., 4–6 weeks after birth, so well before we measure women's labor force working status or breastfeeding.Footnote 14 We consider these variables as proxies of a woman's propensity to breastfeed and examine their correlation with the availability of breastfeeding facilities or family-friendly policies at the workplace. If women with a higher propensity to breastfeed select jobs with different facilities and/or policies, then we would have some indication that we are facing a problem of endogeneity.
In Table 8 we estimate probit models for the probability that a specific type of facility or policy is available as a function of the usual set of mother, child, and area characteristics as well as a variable capturing the propensity to breastfeed. As for our main analysis, we present results for all women and for higher educated and lower educated women separately. As we can see by looking at the first two columns, there is no indication that women who intended to breastfeed, who were breastfed as a child, or who were aware of the benefits of breastfeeding are more likely to be in firms where breastfeeding facilities are available. The only exception is in panel C, where we see that lower educated mothers who were breastfed as a child have a higher probability of being in firms with “facilities to express milk”.
Table 8. Endogeneity of breastfeeding facilities and family-friendly policies
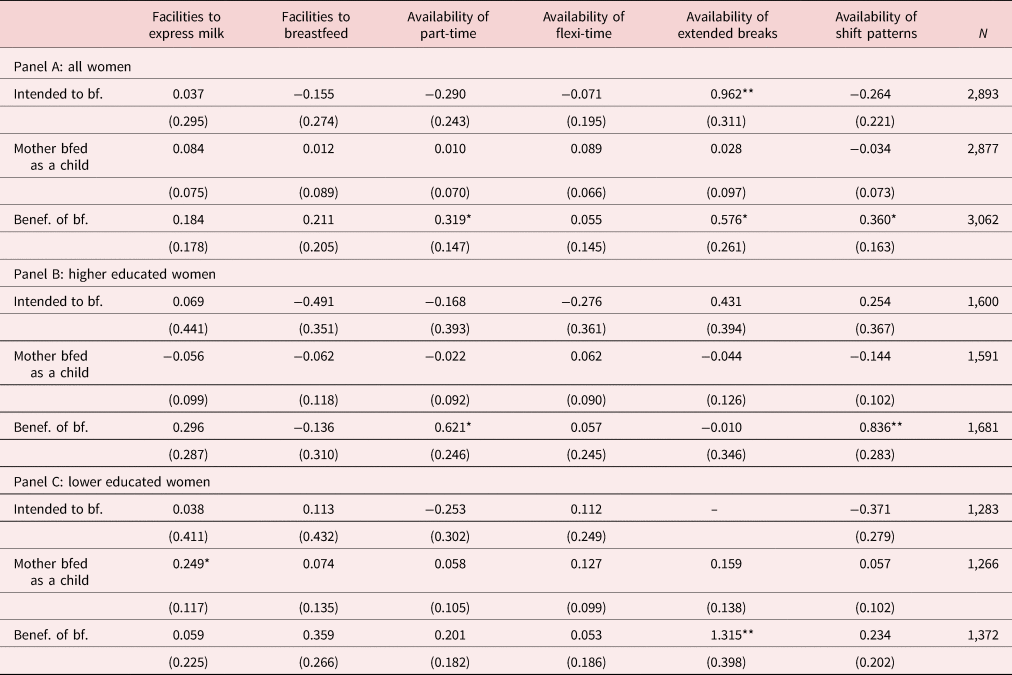
Note: Data from the 2005 UK Infant Feeding Survey. Probit model estimated through maximum likelihood. Dependent variables are: probability to have access to facilities to express milk, probability to have access to facilities to breastfeed, probability to have access to part-time, flexi-time, extended breaks, and shift work. Main independent variable of interest: whether the mother had intended to breastfeed the child, whether she was breastfed as a child, whether she was aware of the benefits of breastfeeding (all measured at stage one). Each coefficient represents the result of a separate regression. Panel A refers to all women, while panels B and C refer to higher educated and lower educated women, respectively. All models control for the set of maternal, child, and work characteristics reported in Table 2, as well as a complete set of regional dummies and dummies derived from an index of local area deprivation (Acorn). Coefficients and heteroscedasticity-robust standard errors (in parentheses) shown. Estimation takes into account survey weights (see notes to Table 2). Symbols: +significant at 10% level, *significant at 5% level, **significant at 1% level.
The other columns present results for the other types of family-friendly policies we consider. Here we find some evidence that women who are aware of the benefits of breastfeeding are more likely to be found in firms who offer part-time, extended breaks and shift patterns. Among lower educated mothers, all women who intended to breastfeed are found to be in a firm which offers “extended breaks”, so that the relevant coefficient is not identifiable in this case.Footnote 15
Overall these results suggest that the availability of breastfeeding facilities is not likely to be endogenous in our model, while the presence of other family-friendly working practices might be. In particular, we are mainly concerned about the positive association between a woman's awareness of the benefits of breastfeeding and the presence of part-time opportunities, especially among higher educated mothers. This might explain why, for example, we find that the availability of part-time work reduces the probability that a mother is working at 4 and 6 months. As we have seen by comparing the results in panels A and B of Tables 4 and 5, however, including all other workplace practices in the model does not affect our estimates of the impact of breastfeeding facilities.
7. Conclusions
The main objective of this paper is to explore whether employers who facilitate breastfeeding at work through the provision of breastfeeding facilities derive a benefit in terms of increased female participation. Although these benefits are often thought to accrue to employers, and form part of the argument put forward by those who advocate workplace policies in support of breastfeeding, there is very little empirical evidence in support of these claims.
Using data from the 2005 UK IFS on a sample of women who return to work before their child is 1 year old, we find that the availability of breastfeeding facilities is associated with higher breastfeeding rates at 4 and 6 months after the birth of the child. By contrast, we do not find any significant positive association between breastfeeding and the availability of other family-friendly policies—such as part-time, flexi-time, extended breaks, and shift patterns, which are meant to capture characteristics of the job or the employer which may affect women's breastfeeding rates and maternity leave spells.
Our main finding is that the availability of breastfeeding facilities is positively associated to the probability of working at 4 and 6 months after the birth of the child, resulting in a shorter duration of maternity leave. This is so only for highly educated women, while we do not find any significant association for the lower educated group of mothers.
A second objective of our analysis is to assess whether by increasing breastfeeding durations the availability of breastfeeding facilities can impact child health, thus providing more (indirect) evidence about the benefits of breastfeeding. We find that there is indeed a positive association between child health and the availability of breastfeeding facilities, but this is so only for health conditions measured when the child is 4–6 months old. We interpret this finding as evidence that breastfeeding has significant effects on the health of the child (as measured in our data) in the first few months of life, but that these effects do not extend to the long term.
As this is essentially an observational study, we need to be cautious about the interpretation of the effects we find in causal terms. Self-selection of women with unobserved characteristics which are associated with speedier return to work, higher rates of breastfeeding, and healthier children into jobs or employers which offer access to breastfeeding facilities is a serious concern. However, we control for a large set of mother, child, and employer characteristics, including firm size and availability of other family-friendly policies. We also find no indication that the availability of breastfeeding facilities is different according to a woman's breastfeeding intentions, own mother breastfeeding practices, and knowledge about the benefits of breastfeeding. A second proviso is that in our data information on the availability of breastfeeding facilities and other family-friendly policies is only collected of women who return to work. Therefore, our evidence should be seen to be relevant for women with a relatively strong attachment to the labor force.
Despite these limitations, our results suggest that providing access to breastfeeding facilities would benefit employers, mothers, and children at the same time. The evidence in this study therefore supports the introduction of legislation requiring employers to provide breastfeeding support measures for women at the workplace.
Acknowledgements
We would like to thank participants at the ISER seminar (University of Essex), at DondenaCHILD-Bank of Italy Workshop, and at conferences of the Population Association of America, European Society of Population Economics, European Association of Labour Economists, Alpine Population for their comments on an earlier version of this work; we are grateful to Paola Battaglia, Maria Iacovou, Chiara Monfardini, Steve Pudney, Birgitta Rabe, Lucia Schiavon, Almudena Sevilla-Sanz, and Saskia Walcott for their suggestions. This work was funded by the ESRC under grant RES-062-23-1693. All mistakes are the authors' only responsibility. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.








