



Introduction
The current COVID-19 pandemic has generated a series of changes in the daily routines of people, including children and teenagers, in an unprecedented way(Reference Singh, Roy and Sinha1,Reference Nicola, Alsafi and Sohrabi2) . From this perspective, many factors influence negatively the physical and mental health of children and teenagers. They experience the stress inherent in the pandemic, such as the isolation itself, school closings, reduced social life and physical activities in parks, gyms or leisure areas, changes in routine, sleeping difficulties, exposure to disharmony at home, excessive use of screens and an unhealthy diet due to the excessive consumption of industrialised foods(Reference Eisenstein, Estefenon and Gama3–Reference Wang, Zhang and Zhao5). Nutritional risks in children must be evaluated because nutritional alterations (child malnutrition, overweight or obesity) are accentuated in the most vulnerable population sectors(Reference Eisenstein, Estefenon and Gama3–Reference Wang, Zhang and Zhao5). This is due to aspects such as a decrease in public support in these sectors (closures or restrictions of schools, nongovernmental organisations or restaurants that provide food) with consequent difficulties in healthy nutrition(Reference Araújo, Veloso and Souza4,Reference Wang, Zhang and Zhao5) . Therefore, it is important to evaluate and identify the factors related to the pandemic that negatively affect the growth and development of children and teenagers, so that prevention strategies can be developed(Reference Araújo, Veloso and Souza4,Reference Wang, Zhang and Zhao5) . These strategies should have an impact on the reduction of potential losses in individual and collective health, and the long-term deterioration of the cognition, physical and mental health, and work capacity of future adults(Reference Araújo, Veloso and Souza4,Reference Wang, Zhang and Zhao5) . The present study aims to evaluate the effects of confinement caused by the COVID-19 pandemic at the level of nutritional status, dietary and behavioural patterns of children and teenagers from elementary school in a small town of Colombia. The Mediterranean diet was taken as a nutritional reference. It is considered a model of a balanced and healthy diet due to its composition rich in vegetables, fruits, legumes, cereals and antioxidants(Reference Archero, Ricotti and Solito6,Reference Carvalho, Ronca and Michels7) that modulate pro-inflammatory cytokines such as interleukin (IL) 6, IL-1, IL-2 and Tumor Necrosis Factor (TNF) α7, and it has been associated with a lower frequency of preventable chronic diseases and some types of cancer(Reference Archero, Ricotti and Solito6–Reference Donini, Serra-Majem and Bulló14).
Materials and methods
An observational, analytical, prolective cross-sectional study was carried out with 266 children who attended one of the seven different elementary schools in the town called Santa Rosa del Sur, Colombia. A sample size of 290 was calculated using an assumed prevalence of childhood malnutrition and overweight/obesity of 0⋅31, with a 5 % margin of error at a 95 % confidence level (CI). Prior to the randomisation process, eight students were excluded due to eligibility criteria. The study response rate was 91⋅7 %. A stratified random sampling was performed, and the total number of students included from each institution was directly proportional to the total number of students of each of them. The eligibility criteria were to attend any of the basic primary grades in one of the seven educational institutions that are present there, not having a known disease, the absence of routine use of drugs to control underlying pathologies, and having a parent available to complete the proposed questionnaire. The data were collected after 4 months of mandatory confinement associated with the COVID-19 pandemic during the months of July and August 2020, in accordance with the Declaration of Helsinki and its subsequent modifications. The María Montessori school provided the ethical approval for this research work, informed assent and consent were obtained from the children and parents, respectively, for the taking of anthropometric measurements, completion of the questionnaire and anonymous registration of the data. Only the principal and the co-investigators who collected the data knew the identity of the children.
Anthropometric measurements and evaluation of fat mass
A team made up of six general practitioners and two undergraduate medical students filled out the questionnaires to learn about the socio-demographic, nutritional and lifestyle aspects of each child. A paediatric specialist collected the anthropometric variables such as weight, height and waist circumference (CC) using standardised methods. Weight (kg) and height (cm) measurements were taken with the child in light clothing, without shoes on and without accessories such as hair ornaments, braids or hats and socks. A portable scale (Health O Meter 844kl), a stadiometer (Seca 222 ®) and a flexible non-elastic measuring tape were used. Initially, two measurements were made: for the weight reading, the closest 0⋅1 kg was considered, and for the height, the closest 0⋅1 cm was taken into account. Also, the closest 0⋅1 cm for the WC was considered. WC was recorded after the children gently exhaled, and the measurement was made at the narrowest part between their lower rib and the iliac crest (natural waist). If there was a difference between the two corresponding anthropometric measurements, a third measurement would be taken and averaged.
BMI, BMI Z-score and waist-to-height ratio (WtHR) were calculated as previously reported. Children were classified as thin or at risk of thinness, normal weight, overweight and obesity according to the age- and sex-specific International Obesity Task Force (IOTF)(Reference Cole, Bellizzi and Flegal15).
Questionnaires
The instruments used included a socio-demographic characterisation questionnaire, the KIDMED(Reference Serra-Majem and Ribas16) and two questions related to changes in behaviour during confinement. The first information collection format (ICF) included variables such as sex, age of the child, age and profession/occupation of the parents, composition of the household and nutritional status of relatives within the household. The questionnaire also inquired about the characteristics and behaviours of the child related to sleep pattern, the practice of physical activity and the hours dedicated to leisure (television, telephone and computer measured in minutes per day). Additionally, an open self-assessment question was asked to estimate the parents’ perception of their child's real weight: ‘In your opinion, is your son/daughter in: underweight, normal weight, overweight or obesity?’
KIDMED(Reference Serra-Majem and Ribas16) is a validated scale, made up of sixteen questions, which aims to analyse the consumption and the frequency of daily intake of various foods. This instrument was originally developed to assess the level of adherence to MD in Spanish children and young people from 2 to 24 years of age. The sum of their values varies between 0 and 12 points, and it allows classifying adherence to MD as follows: high (≥8 points), moderate (4–7 points) and low adherence (≤3 points). The version used in the present study was adapted from the version by Serra-Majem et al. (Reference Serra-Majem and Ribas16).
Statistic analysis
In the univariate statistical analysis, the qualitative variables with absolute frequencies and percentage, and the quantitative variables with mean and standard deviation were described. The nutritional status was established in four categories according to the Z-score of the BMI. To complement, the perception of weight by the parents was described, and a variable was formed with the level of agreement between the real weight and the weight estimated by the parents, and it was established whether the nutritional status of their children is overestimated or underestimated (Table 3).
Differences were established between all variables, including nutritional status with high adherence to the MD considering the dichotomous variable, collapsing low and moderate with high adherence according to sex using Pearson's Chi-square test (χ 2) or Fischer's exact test or student's t. 95 % confidence intervals were calculated. To explain the high adherence to the MD, we included sex, categorised age (<9 years: ≥9 years), high abnormal weight (thin and normal weight: overweight and obesity), having received breastfeeding for 12 months (<12 months: ≥12 months), categorised mother and father education, father and brother overweight and lifestyle variables using logistic regression. Differences were established considering as significant a value of P < 0⋅05. The processing and analysis of the information was carried out in the statistical program Stata 14.
Results
Table 1 shows the socioeconomic, anthropometric, nutritional and lifestyle characteristics of the children grouped according to sex. In total, 266 elementary school children between 5⋅1 and 14⋅8 years old were evaluated, including 142 (53⋅4 %) women and 124 (46⋅6 %) men. The mean age of the participants was 8⋅5 ± 2⋅04 years. In relation to nutritional status, a total of 164 (61⋅7 %) students were classified as having adequate nutritional status (eutrophic), while 102 were considered to have altered nutritional status, including 27 (10⋅1 %) in thinness or risk of thinness, 39 (14⋅7 %) with overweight and 36 (13⋅5 %) with obesity. The 50th percentile of BMI of the participants was 56⋅8 ± 31⋅3. Thinness or risk of thinness was more prevalent in children (n 17/27, 62⋅9 %; P = 0⋅1746). Women were twice as overweight (26/39,⋅66⋅7 %) compared to men (13/39,⋅33⋅3 %; P = 0⋅0439). Likewise, obesity was slightly more frequent in men (n 19/36, 52⋅7 %; P = 0⋅7193).
Table 1. Demographic and anthropometric characteristics, nutritional status and lifestyles according to sex
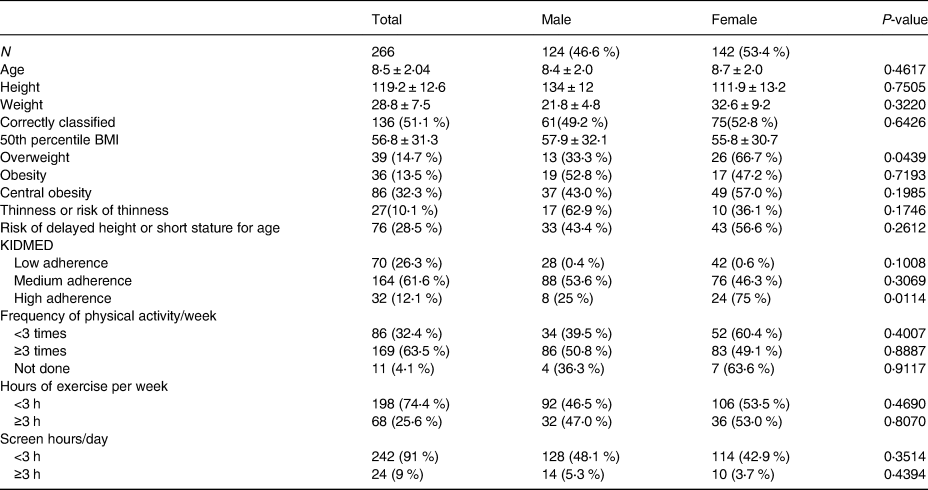
Abdominal obesity (waist/height index ≥ 0⋅5) was found in 32⋅3 %, 95 % CI (0⋅27, 0⋅38) of the participants, and it was more prevalent in women (49/86, 57 %) compared to men (37/86, 43⋅0 %; P = 0⋅417), also corresponding to 14 (87⋅5 %) in overweight condition and 11/25 (44 %) in obesity condition.
The analysis of nutritional habits showed that only 12⋅1 %, 95 % CI (0⋅09, 0⋅16) of the participants had high adherence to the MD, 61⋅6 and 26⋅3 % of them had moderate and low adherence, respectively.
During the confinement period, it was found that 65⋅8 % of the participants reported changes in behaviour, predominantly irritability and hyperactivity (40 % v. 27⋅4 %, respectively). There were no statistically significant differences in behaviour according to the sex of the participants (P = 0⋅2360).
Table 2 shows the responses obtained in the KIDMED questionnaire according to gender and the total sample. We found very similar responses according to the gender of the participants. Among the positive results, we highlight the habit of having breakfast every day as well as the consumption of legumes more than once a week, and consumption of pasta or rice almost daily (5 d or more a week). In turn, we highlight a low number of responses in the items that inquire about the consumption of nuts at least two or three times a week and the use of olive oil. The responses to each item were analysed by gender to verify associations between these variables. No statistically significant differences were found between the variables of the KIDMED questionnaire and gender.
Table 2. Responses obtained in the questionnaire of adherence to the Mediterranean diet according to gender

KIDMED, Mediterranean Diet Quality Index in Children and Adolescents.
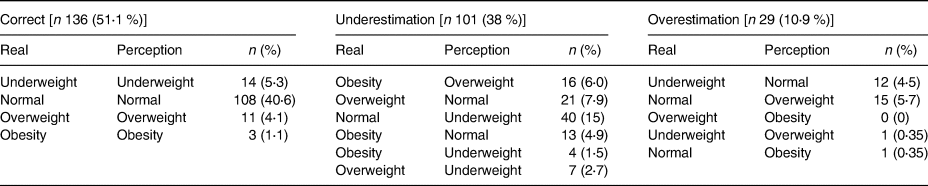
Table 3 shows the perception of parents about the weight of their children and its corresponding interpretation according to the real weight. In 51⋅1 % of the participants, there was an adequate correlation between the perception of weight of the parents and the actual weight of the child, an underestimation of the child's weight was observed in 38 % (n 101) and an overestimation in 10⋅9 % (n 29) of the participants.
Table 3. Parental perception of children's weight status
In relation to the factors associated with having high adherence to the MD, the bivariate analysis found significant differences in sex OR 0⋅34 (0⋅15, 0⋅78; P = 0⋅012) and categorised age: OR 0⋅35 (0⋅15, 0⋅81; P = 0⋅015). Finally, in the multivariate model constructed with having been breastfed for >12 months, having a high abnormal weight, categorised age and sex, it was found that being less than 9 years old is associated with high adherence to the MD (OR 0⋅32; 0⋅14, 0⋅75; P = 0⋅009), and being a man increases 3⋅2 times more the chance of having low or moderate adherence to the MD compared to women (OR 0⋅31; 0⋅14, 0⋅75).
Discussion
The present study aimed to evaluate the effects of confinement caused by the COVID-19 pandemic at the level of nutritional status, dietary and behavioural patterns of children and teenagers from elementary school in a small town of Colombia. In this sense, the prevalence rates of the double burden of disease (malnutrition, overweight/obesity) found in the present study generate great concern regarding the health of children and teenagers in Santa Rosa del Sur, Colombia during the current COVID-19 pandemic. The present study estimates a prevalence of underweight, overweight and obesity among school children and teenagers of 10⋅1, 14⋅7 and 13⋅5 %, respectively, and these numbers that turn out to be higher compared to those reported in the last national health survey in Colombian children (Ensin2015)(17) with prevalences of underweight and overweight of 7 and 24⋅4 %, respectively. Compared with other studies, prevalence rates were similar to those previously reported in children and teenagers in Europe(Reference Smetanina, Albaviciute and Babinska18–Reference Valdes Pizarro and Royo-Bordonada21), Africa(Reference Gyamfi, Obirikorang and Acheampong22), Asia(Reference Ivanovitch, Keolangsy and Homkham23,Reference Esmaili, Bahreynian and Qorbani24) and South America(Reference Silva, Feilbelmann and Silva25,Reference Dumith and Farias Júnior26) . However, we estimate higher proportions of both, obesity measured by BMI and central obesity, than those reported in other studies(Reference Archero, Ricotti and Solito6,Reference Ivanovitch, Keolangsy and Homkham23,Reference Esmaili, Bahreynian and Qorbani24,Reference Dumith and Farias Júnior26–Reference Adebimpe33) . The prevalence of high abnormal weight was 28⋅2 % similar to that reported by Garrido et al. where it is described that 32⋅1 % of young people aged 7–13 years were overweight and obese(Reference Garrido-Miguel, Cavero-Redondo and Álvarez-Bueno34).
The overweight ratio was two women for every man and obesity was slightly more frequent in men (19/36, 52⋅7 %). These findings contrast with those previously described in Asian(Reference Karki, Shrestha and Subedi31,Reference Hoang, Orellana and Le35) and European(Reference Archero, Ricotti and Solito6,Reference Smetanina, Albaviciute and Babinska18–Reference Valdes Pizarro and Royo-Bordonada21) children, but they are similar to those reported in 2018 by Silva et al. in the state of Minas Gerais, Brazil(Reference Silva, Feilbelmann and Silva25).
With regard to sedentary and nutritional habits and despite the fact that 74⋅4 % of the participants in our studies performed <3 h of physical activity per week, no statistically significant differences were found in the nutritional status of the patients. This is a finding that is consistent with the one reported by Smetanina et al. in Lithuania(Reference Smetanina, Albaviciute and Babinska18), but it is different from what was reported in Brazil(Reference Silva, Feilbelmann and Silva25,Reference Camelo Ldo, Rodrigues and Giatti36,Reference De Souza Dantas, Dos Santos and Lopes37) , Mexico(Reference Lopez-Gonzalez, Partida-Gaytán and Wells38), Australia(Reference Mihrshahi, Drayton and Bauman39), Egypt(Reference El-Gilany and El-Masry40), Nigeria(Reference Adebimpe33), Nepal(Reference Karki, Shrestha and Subedi31), Iran(Reference Ghobadi, Totosy de Zepetnek and Hemmatdar41) and among others(Reference Ivanovitch, Keolangsy and Homkham23,Reference El-Kassas and Ziade42) . The relationship between the educational level of the parents and the nutritional status of the children continues to be contradictory, because some studies have reported higher frequencies of overweight or obesity in children whose parents have a higher educational level(Reference Silva, Feilbelmann and Silva25,Reference Karki, Shrestha and Subedi31,Reference Hoang, Orellana and Le35,Reference Leal, Lira and Oliveira43) , yet, other studies associate less education with higher rates of overweight/obesity(Reference Smetanina, Albaviciute and Babinska18). In our particular case, we did not find significant differences in such variables.
Regarding the second objective, adherence to the MD was low in 26⋅3 %, moderate in 61⋅6 % and high in 12⋅1 % of the participants, in discrepancy with what was reported by Santos Marques et al. in two villages in Portugal (Porto and Maia), in whose study describes a high adherence to MD in 77⋅6 % of the participants(Reference Marques, Pinto and Reis44). These differences may be due to the urban environment of these cities and their concern for the promotion of healthy lifestyles, which is different from the rural environment and the lack of clear and well-defined public policies in our case. Furthermore, our results also disagree with different studies in the European population with low adherence between 16⋅7 and 18⋅5 %, and high between 19⋅6 and 29⋅3 % of the participants(Reference Archero, Ricotti and Solito6,Reference Sirico, Fernando and Bianco45,Reference Tapia Serrano, Vaquero-Solís and López-Gajardo46) . No significant differences were found between adherence to the MD and the BMI of the participants, so it should be noted that such an adherence does not guarantee adequate nutritional status by itself, since we would be leaving aside the synergistic role that healthy habits can exert, such as physical activity and sedentary time(Reference Tapia Serrano, Vaquero-Solís and López-Gajardo46). We found that age under 9 years and female sex had a statistically significant association with high adherence to the MD, although our results are in contrast to those described by Novak et al. (Reference Novak, Štefan and Prosoli47) in European teenagers, this could be due to the fact that both school children and teenagers were included in the study, and their hypothesis was valid that during adolescence, women were more sedentary because of their school obligations accompanied by stress and irregular eating. This would suggest that the protective factor found in the present study dissipates in as much as there are more academic and/or work responsibilities acquired by women, which would explain the higher prevalence of overweight/obesity in females, mainly after the age of 15(Reference Conde, Mazzeti and Silva48).
Finally, we found another important concern in the present study, and it is a wrong perception of parents about the weight of their children in 48⋅9 % of the cases (underestimation: 38 %, overestimation: 10⋅9 %). This is a higher percentage compared to what was reported by Sirico et al. in Italian parents(Reference Sirico, Fernando and Bianco45), which suggests a poor awareness in general regarding childhood overweight/obesity, and medium and long-term complications in parents both in the study by Sirico et al. and in the present study. This can be linked to various sociocultural factors, as well as to their educational level, and the psychology and economy of the parents(Reference Sirico, Fernando and Bianco45,Reference Bahreynian, Qorbani and Khaniabadi49) .
All things considered, however, reveal that the present study has some limitations. First, physical activity and screen times were not measured objectively, but through a questionnaire given to parents. Secondly, the data correspond to school children and teenagers in a town in Colombia, so the results cannot be extrapolated to the general Colombian population. Finally, since it is a descriptive and cross-sectional study, cause and effect relationships cannot be established between the study variables. Despite the limitations, the work has great strength, since it provides updated and representative information that represents a starting point from the nutritional approach of the paediatric patient during the current COVID-19 pandemic.
In conclusion, we observed a worrying nutritional, dietary and behavioural situation in the children and teenagers studied during the confinement associated with the COVID-19 pandemic. This unveils the need to establish strategies and/or public policies in our town that help to promote an adequate biopsychosocial development of the paediatric patient and their family group, having as fundamental pillars a healthy diet and adequate physical activity.
Acknowledgements
The authors thank Dra. Jessica Estefania Plata Ortiz for the academic assistance provided during the execution of this research work.
This research was not funded by any government agency or state programme.
W. J. M. C., S. E. O. Z. and J. M. M. D. designed the study, collected and analysed the data and wrote the preliminary manuscript. M. A. M. C., A. C. H. C., A. R. A., E. J. D. V., A. C. C., L. X. N. A., L. C. A. M. and A. M. N. S. contributed to the development of the study protocol, supervised the study, actively contributed to the interpretation of the results and critically reviewed the paper.
We declare the complete compliance by each author, in the design and development of the study, the analysis of the results, the writing of the manuscript, the approval of the final version and the responsibility in all aspects of the manuscript of the current research work.
All authors have participated in the drafting of the manuscript and have read and approved its final version.
The authors declare no conflicts of interest.




 Open access
Open access