



Introduction
Adolescence, the second decade of life, is the transition period from childhood towards adulthood and considered as a window of opportunity to build strong foundation for healthy and productive adulthood and consequently the health and wellbeing of the next generation(Reference Sawyer, Azzopardi and Wickremarathne1–Reference Azzopardi, Hearps and Francis3). In this era of fast demographic, epidemiological and nutritional transitions, adolescents are experiencing a complex burden of malnutrition worldwide(Reference Azzopardi, Hearps and Francis3,Reference Weiss and Ferrand4) . In Bangladesh and other developing countries, adolescents are suffering from a very high prevalence of undernutrition, micronutrient deficiencies, overweight or obesity(Reference Capacci, Mazzocchi and Shankar5–Reference Frenk and Gómez-Dantés8).
Poor diet, in terms of quantity and diversity, is one of the major causes of all forms of malnutrition at all stages of the life cycle. Evidence suggests that dietary diversity (DD), ‘an increase in the variety of foods across and within food groups over a reference period’(Reference Ruel9), reflects dietary quality in terms of nutrient adequacy of a diet at an individual level(Reference Ruel10–Reference Martin-Prevel, Arimond and Allemand15). Food-based dietary guidelines recommend the intake of more diversified foods to address malnutrition and prevent diet-related chronic diseases(16,Reference Nahar, Choudhury and Faruque17) .
Globally, adolescent diets are characterised by inadequately diversified food, less nutrient-dense food, more processed foods and beverages(Reference Patton, Sawyer and Santelli2,Reference Akseer, Al-Gashm and Mehta18,Reference Keats, Rappaport and Shah19) . In low- and middle-income countries (LMICs), inadequate DD is more prevalent across all age groups due to the ubiquity of a large proportion of starchy staple in the whole diets(Reference Arimond, Wiesmann and Becquey20–Reference Arimond and Ruel22) and similarly, in Bangladesh, the adolescent diets are poor in both diversity and micronutrient content(Reference Leroy, Ruel and Sununtnasuk23–26). Besides, systematic reviews show that in LMICs, a wide range of socio-economic determinants at the individual, parental, household, environmental and macro-system levels in different contexts influence the diversity and micronutrient contents of the diets among adolescents(Reference Keats, Rappaport and Shah19,Reference Madjdian, Azupogo and Osendarp27) .
To date, only a limited number of studies have been conducted considering DD as the main outcome and explored factors associated with it among adolescents in Bangladesh. Moreover, these studies were mostly focused on girls(26–Reference Akter, Mistry and Mukta28), school-based adolescents(Reference Ahmed, Zareen and Khan29) or pregnant adolescents(Reference Mridha, Matias and Arnold24,Reference Shamim, Mashreky and Ferdous25) . These studies had small sample sizes and only a few studies focused on the determinants of inadequate DD(Reference Mridha, Matias and Arnold24,Reference Shamim, Mashreky and Ferdous25,Reference Mridha, Hossain and Hassan30) . None of these studies included adolescent boys as the study population. Therefore, population-weighted, nationally representative data are scarce on the prevalence of inadequate DD and its determinants among adolescent girls and boys. Given this reality, we intended to explore the national prevalence of inadequate DD and factors associated with inadequate DD among adolescent girls and boys in Bangladesh.
Methods
Study design and settings
Since 1990, the government of Bangladesh has been implementing nutrition and food security surveillance among women and children. In the 2018–19 round of the surveillance, we included additional population groups, for example, adolescent boys and girls, adult males and elderly people. In this survey, we covered all types of geographical areas, that is, rural, non-slum urban and slums from all eight administrative divisions of the country. We enrolled participants from eighty-two clusters (fifty-seven rural, fifteen non-slum urbans and ten slums) to generate divisionally and nationally representative estimates of different indicators, including the DD of adolescent boys and girls. Adolescents were interviewed after obtaining appropriate informed written assent and consent from the guardians (for 10 to <18 years old adolescents) and informed written consent (for ≥18 years old adolescents).
Sampling technique
Different sampling designs were employed to select study sites from rural, non-slum urban and slum areas and to draw a representative sample of Bangladesh. A four-stage sampling procedure was employed to select clusters in rural areas. First, two districts were randomly selected from each of the eight divisions, and one sub-district was randomly selected from each of the selected districts. Then, two unions (the smallest administration unit) were randomly selected from each of the sub-district and were divided into segments with 250–400 households keeping the geographical demarcation of villages in the unions uninterrupted. Finally, two segments from each of the selected unions were randomly picked as the final data collection cluster (total 64).
In non-slum urban areas, sixteen wards (lowest administrative unit in the urban areas) from eight divisions were selected randomly. Then one mahalla/segment of 250–400 households was randomly picked from the list of mahalla/segments of each selected ward. Thus, a total of sixteen clusters (mahalla/segment) were selected from the urban areas, and data were collected from fifteen urban clusters. In slum settings, ‘Census of Slum Areas and Floating Population 2014’ were used to select the data collection clusters(31). A total of ten slum clusters, each with ≥300 households from eight divisions (two from Dhaka and two from Chattogram and one from each remaining six divisions), were randomly selected.
Study participants and sample size
The sample size was calculated to obtain divisionally, nationally as well as slums representative prevalence estimates for the key variables of the study. For adolescents and other population groups, the prevalence (p) of key variables such as nutritional status and DD varied from 4 to 98 %. Considering the probability of Type I error, α = 0⋅05; allowable margin of error, d = 0⋅05 or p/2 when P ≤ 0⋅1; design effect, DEF = 1⋅61, sixty-two adolescent boys and sixty-two adolescent girls were needed from each cluster. Thus, the estimated sample size was 5580 for adolescent boys and 5580 for adolescent girls from 90 clusters. Due to an administrative embargo and financial constraints, data were finally collected from eighty-two clusters.
The data collection period of the study was from October 2018 to October 2019. In each cluster, all the households were listed to generate a sampling frame for each eligible participant from all six population groups (0–5 years old children, 10–19 years old adolescent girls, 10–19 years old adolescent boys, 20–59 years old women, 20–59 years old men and ≥60 years old persons). A total of 10 529 adolescent girls and 10 211 adolescent boys were listed from 25 371 households in 82 clusters and from them, 5084 boys (62 × 82) and 5084 girls (62 × 82) were randomly selected (62 girls and 62 boys from each cluster). If one household had more than one eligible participant from a population group, one of them was selected randomly. Five data collection teams, each comprising one supervisor and four to five data collectors, performed data collection and anthropometric measurements. As some of the randomly selected boys and girls were unavailable at home during the interview, and some refused the interviews, a total of 4907 adolescent boys and 4949 adolescent girls were enrolled in this survey. Among the adolescents, eighty-four girls were found pregnant during the data collection period. They were excluded from our analysis as pregnancy may influence food consumption. Therefore, the final number of adolescent girls was in 4865.
Data collection techniques
We collected data using a structured questionnaire by face-to-face interviews. Physical measurements, height in cm (using locally made stadiometer) and weight in kg (using TANITA, model UM-070 weighing scale) of the adolescents were measured. Three measurements for height and three measurements for weight were taken over light clothing after confirming the privacy and comfort of the participants. All anthropometric measurements were taken based on WHO guidelines, as specified in the FANTA anthropometry manual(Reference Cashin and Oot32). Data were collected electronically using a customised SurveyCTO on a tablet computer (Samsung Galaxy Tab A7) application and were uploaded to the system every day at the end of data collection.
Quality control
Data collectors received a 5-d training on interview tools and techniques, physical measurements, calibration and maintenance of data collection instruments, and went through a standardisation process. Data collection questionnaires were pre-tested and modified based on the pre-test findings. About 5 % of the interviewed households were randomly re-interviewed, and another 5 % of the randomly selected interviews were observed by the supervisors to ensure data quality. Besides, interim analyses were done to check the quality of the data and we found that collected data had internal consistency and were in alignment with similar studies from Bangladesh.
Outcome variable
Our outcome variable of interest was inadequate DD among adolescent boys and girls. DD is an indicator of dietary intake at the individual level, which describes how diversified food a person consumes(Reference Kennedy, Razes and Ballard13). Minimum dietary diversity for women (MDD-W) is a population-level, simple and dichotomous indicator to assess DD at national and subnational levels(Reference Martin-Prevel, Arimond and Allemand15,33,34) . The present study adopted the MDD-W questionnaire to collect dietary data using a list-based recall method on twenty-four food categories consumed in the last 24 h. These food categories were aggregated during analysis into the ten food groups ((1) grains, white roots and tubers and plantains; (2) pulses: beans, peas and lentils; (3) nuts and seeds; (4) dairy; (5) meat, poultry and fish; (6) eggs; (7) dark green leafy vegetables; (8) other vitamin A-rich fruits and vegetables; (9) other vegetables and (10) other fruits) following MDD-W guideline(33,34) . Regarding consumption of mixed dishes, we asked the respondents for all the ingredients included in that dish and record separately in the food list. We also considered the fact that whether the ingredient is usually consumed ‘large enough’ to be included as a separate food item or consumed usually very small amount to be classified as ‘Condiments and seasonings’ according to MDD-W guideline(33,34) . We used the same tool to collect dietary data and the same cut-off point for adolescent girls as well as for boys to define inadequate DD since there is no separate tool available to measure DD among the boys. A girl or boy was categorised as having inadequate DD when s/he consumed foods from four or less food groups from the ten food groups in the last 24 h.
Explanatory variables
We carried out a literature review to identify the variables that can be the possible determinants of DD(Reference Mridha, Matias and Arnold24,Reference Shamim, Mashreky and Ferdous25,Reference Mridha, Hossain and Hassan30,Reference Islam35) . From our dataset, we identified the following variables age, education, nutritional status, maternal and paternal education, the place of residence, religion, household size, household headship, household food security status and household wealth status (Table 1). In our study, we collected individual-level information from the adolescents, and household head was the respondent for parental-level and household-level information.
Table 1. Different categories/measurements of explanatory variables of the present study

We used the Household Food Insecurity Access Scale (HFIAS) questionnaire developed by the Food and Nutrition Technical Agency to collect data on behaviours and attitudes related to three domains of food insecurity (access) experiences including (1) anxiety and uncertainty about the household food supply; (2) insufficient food quality includes variety and preferences of the type of food and (3) insufficient food intake and its physical consequences to estimate the prevalence of food insecurity at the household level in Bangladesh(Reference Coates, Swindale and Bilinsky36). Based on this guideline, we asked nine occurrence questions to the respondents on perceptions of their households’ food vulnerability and on their behavioural responses to food insecurity with a recall period of 4 weeks (30 d) providing the options zero to three indicating frequency of the occurrence as never, rarely, sometimes and often, respectively. We used HFIA prevalence indicator to categorises households into four levels of household food insecurity (access): food secure, and mild, moderately and severely food insecure.
For other variables of data collection, standard questions used by MEASURE DHS (Monitoring and Evaluation to Assess and Use Results Demographic and Health Surveys) for Demographic Health Surveys were followed(37). For example, wealth index, a measure of relative wealth at the household level, was assessed through some specific assets, such as availability of amenities (electricity, solar electricity, radio, television, telephone, mobile, refrigerator, table/chair, watch/wall clock, almirah/wardrobe, electric fan, bicycle, motorcycle/motor scooter, car/truck, boat, water pump, etc.), household cooking fuel used (electricity, LPG, piped natural gas, kerosene, coal, wood, straw/grass/leaves, animal dung, bio-gas), main source of drinking water, type of toilet used, household materials of floor, walls and roof. All of these household characteristics and assets were analysed using principal component analysis. A composite wealth index was assessed using a DHS (Demographic and Health Survey) method consisting of area-specific indexes combined into a national model(37) The wealth index was divided into five quantiles. Categories for household size was done based on the national mean household size in Bangladesh, which is 4⋅5(37). That's why we kept it as ‘≤4 members’ and ‘≥5 members’. Regarding nutritional status, body mass index or BMI for age (BAZ) was calculated for adolescents using age- and gender-specific WHO growth charts in AnthroPlus software and adolescents were categorised as thin, normal weight and overweight and/or obese(Reference Blössner, Siyam and Borghi38).
Statistical analysis
Descriptive analyses (frequency distribution and percentage) were performed to report socio-economic and demographic information of the adolescent girls and boys. Pearson's χ 2 test was administered using weighted data to estimate and compare the distribution of inadequate DD between boys and girls within different categories of each explanatory variable. All tests were two-tailed and a P-value of <0⋅05 was considered as statistically significant.
Binary logistic regression was done to assess the relationship of inadequate DD with each of the explanatory variables separately. The explanatory variables with P-value ≤0⋅2 in the univariate model were included in the final multivariable logistic regression model(Reference Bursac, Gauss and Williams39,Reference Kibria40) . Multi-collinearity was checked using the ‘correlation matrix’ to identify the independent variables with higher correlation, and the variables with correlation coefficient ≥0⋅5 were excluded (age and paternal education: as these variables were highly correlated with educational attainment of adolescents and maternal education, respectively) before running the multivariable logistic regression. After considering P-value during univariate analyses and multi-collinearity, education, maternal education, place of residence, religion (only for boys), household headship, household food insecurity status and household wealth were included in the multivariable logistic regression model. The crude odds ratio (cOR), adjusted odds ratio (aOR) and 95 % CI of OR were estimated, and a P-value of <0⋅05 was considered as statistically significant. All statistical analyses were performed using the statistical software package Stata (version 13.0).
Research ethics
Ethical approval from the Institutional Review Board (IRB) of the BRAC James P Grant School of Public Health, BRAC University, Dhaka, Bangladesh, was sought (reference number 2018-020-IR) before conducting the study. Community sensitisation meetings with local leaders and the representatives from potential respondents were done to get the community consent before stating data collection in an area. Written informed consent (assent for 10–17 years old adolescents and informed consents from their guardians) were taken prior to the interview. Privacy, confidentiality and anonymity were fully maintained throughout the research process.
Results
Background characteristics of the respondents
Table 2 outlines the detailed socio-economic and demographic characteristics of adolescent boys and girls. A higher proportion of the adolescent boys (56⋅8 %) and girls (54⋅9 %) belonged to the early adolescent group (10–14 years). In our study, the girls were better educated than boys. Regarding thinness, the proportion among boys was higher compared to the proportion among girls (28⋅5 % v. 18⋅9 %). Approximately one in every ten adolescent boys and girls were overweight and/or obese (8⋅7 % v. 10⋅5 %). Moreover, 42⋅4 % of households experienced any food insecurity, with 12⋅2 % households reporting severe food insecurity.
Table 2. Distribution of adolescent boys and girls by socio-demographic characteristic
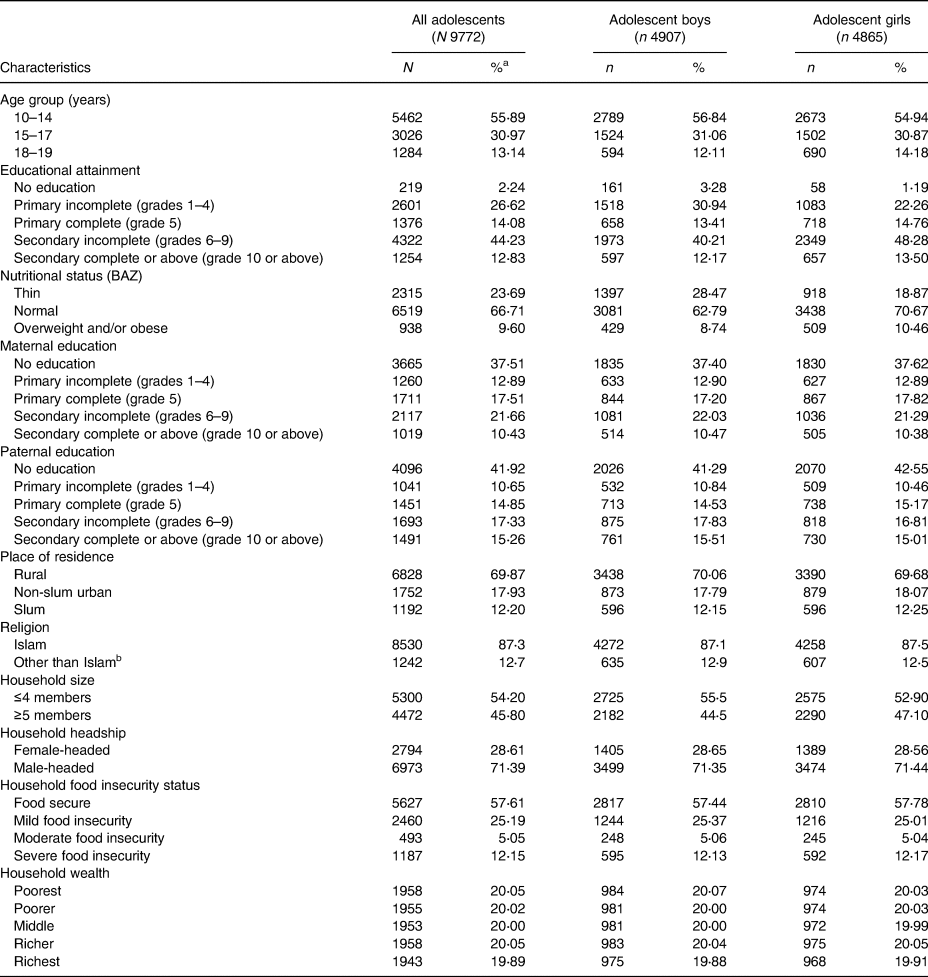
a Column percentages.
b Buddhism, Christianity and Hinduism.
Socio-demographic distribution of inadequate DD among adolescents
The weighted prevalence of inadequate DD among adolescent boys and girls across the background characteristics is summarised in Table 3. The study revealed that, nationally, the prevalence of inadequate DD significantly (P = 0⋅001) varied by sex, and the prevalence was higher among girls (55⋅4 %) than boys (50⋅6 %). Although when adolescents were categorised in three age groups, the inadequate DD prevalence was significantly higher only among girls of 15–17 years age group compared to the boys of the same age (girls 58⋅5 % v. boys 47⋅5 %, P = 0⋅002). The DD score for boys was higher than girls (4⋅49 ± 1⋅65 v. 4⋅39 ± 1⋅61) and the overall score was 4⋅44 ± 1⋅63. A higher prevalence of inadequate DD was found among adolescents who had no education (68⋅6 %), were thin (54⋅7 %), lived in a slum (64⋅5 %), lived in a household with >4 members (54⋅7 %), and belonged to a female-headed household (58⋅0 %) compared to their respective counterparts. These findings were applicable for boys and girls separately, though the prevalence differed between girls and boys within the same variable categories in most cases. Regarding parental education, a lower prevalence of inadequate was observed among adolescents with highly educated mothers and fathers. Compared to adolescents from food-secured households, the prevalence of inadequate DD was observed higher among adolescents from households with any (mild to severe) food insecurity.
Table 3. Distribution of inadequate DD among adolescent boys and adolescent girls by socio-economic characteristics
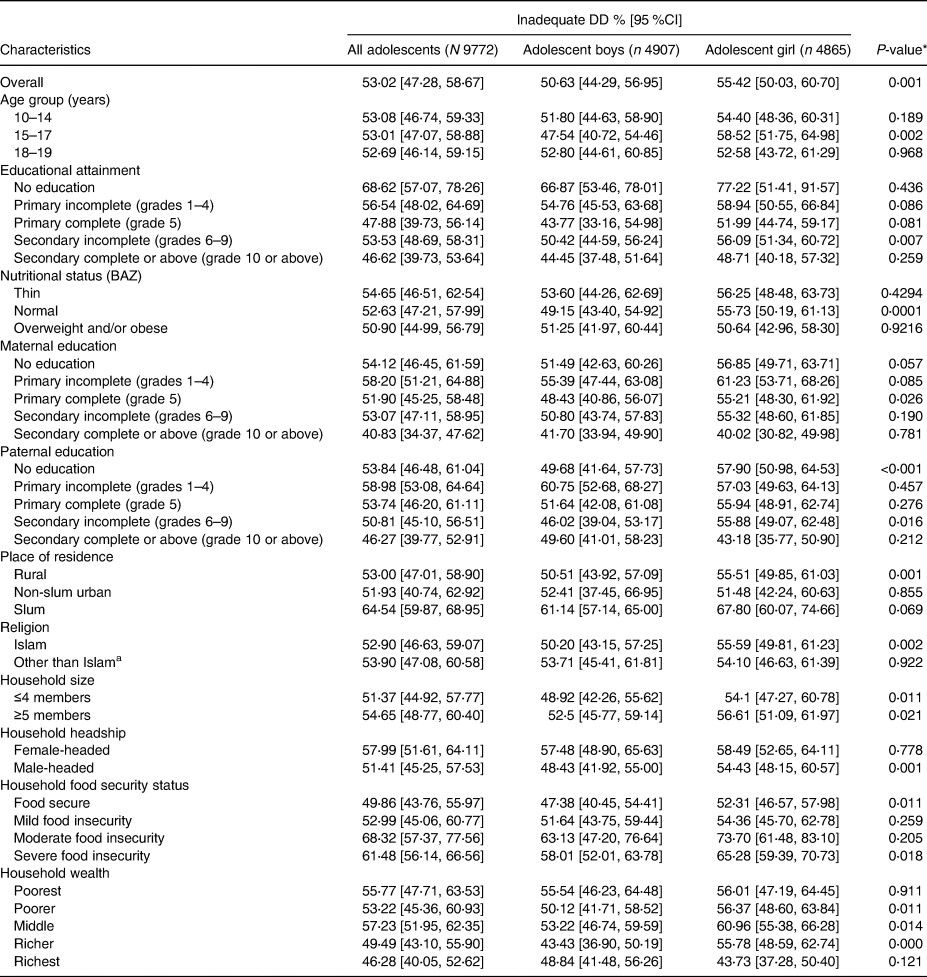
* P-value is between boys and girls of same variable categories.
a Buddhism, Christianity and Hinduism.
Determinants of inadequate DD among adolescents
The determinants of inadequate DD among adolescents and the strength of the association as revealed by crude and adjusted odds ratios are presented in Table 4 (for boys) and Table 5 (for girls). In the unadjusted analyses, education, maternal education, paternal education, place of residence, household headship, household food insecurity status, and household wealth were identified as significantly associated with inadequate DD among both boys and girls. Among these factors, education, maternal education, household headship, household food insecurity status, and household wealth were remained as significant predictors for inadequate DD after adjusting all the potential covariates in the final model for both boys and girls.
Table 4. Multivariable logistic regression analysis on the socio-economic factors influencing inadequate DD among adolescent boys
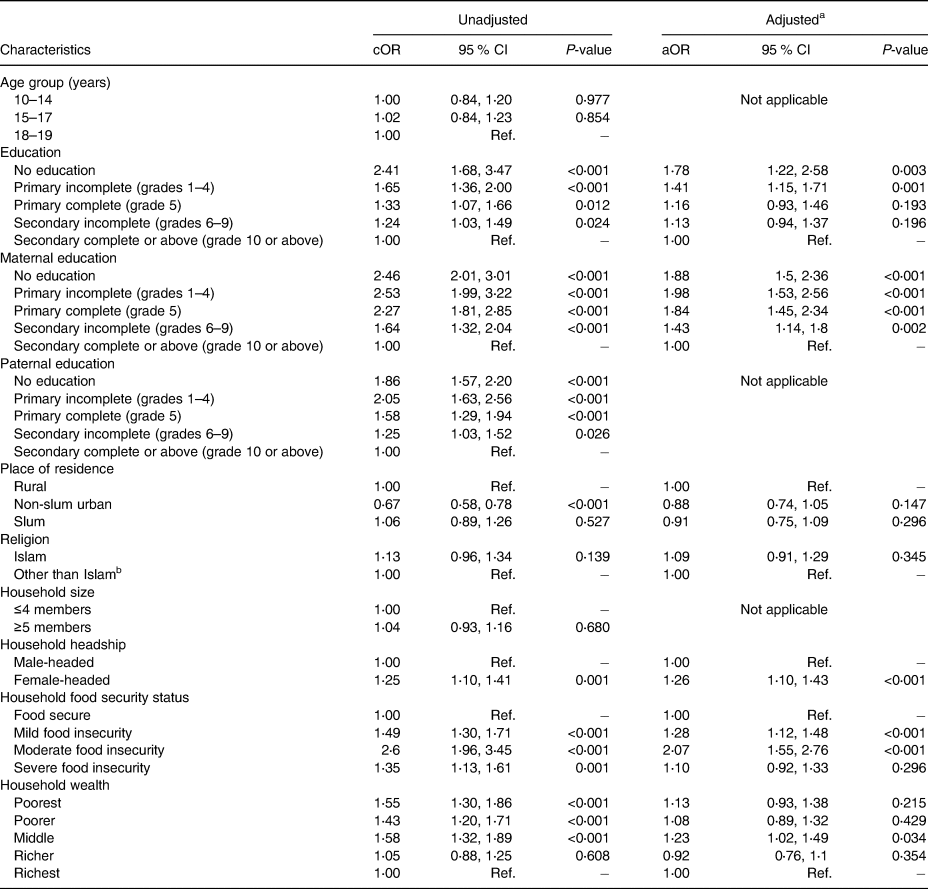
aOR, adjusted odds ratio; cOR, crude odds ratio; Ref., reference category.
a Adjusted for education, maternal education, place of residence, religion, household headship, household food security status and household wealth.
b Buddhism, Christianity and Hinduism.
Table 5. Multivariable logistic regression analysis on the socio-economic factors influencing inadequate DD among adolescent girls

aOR, adjusted odds ratio; cOR, crude odds ratio; Ref., reference category.
a Adjusted for education, maternal education, place of residence, household headship, household food security status and household wealth.
b Buddhism, Christianity and Hinduism.
The chances of having inadequate DD had an inverse association with educational attainment among both boys and girls; however, the association was statistically significant only for those who had incomplete primary education (boys: aOR 1⋅41; 95 % CI 1⋅15, 1⋅71; P = 0⋅001 and girls: aOR 1⋅41; 95 % CI 1⋅15, 1⋅73; P = 0⋅001) and those who received no education (boys: aOR 1⋅78; 95 % CI 1⋅22, 2⋅58; P = 0⋅003 and girls: aOR 3⋅28; 95 % CI 1⋅65, 6⋅49; P = 0⋅001) compared to those who completed at least secondary level education. Moreover, we found that maternal education has a highly significant inverse relationship with inadequate DD among both boys and girls. Meanwhile, boys belong to female-headed households had 26 % higher odds ratio (aOR 1⋅26; 95 % CI 1⋅10, 1⋅43; P < 0⋅001), and adolescent girl belonged to female-headed households had 21 % higher odds ratio (aOR 1⋅21; 95 % CI 1⋅06, 1⋅38; P = 0⋅004) to have inadequate DD in relation to adolescents from male-headed households. The chances of having inadequate DD among adolescents are relatively higher for the food-insecure households compared to the food-secure household. Similarly, the girls of relatively poorer households had higher chances of having inadequate DD compared to the girls from the richest households. However, there was no such pattern among boys. No association was found either between the place of residence and inadequate DD or between religion and inadequate DD.
Discussion
Using nationally representative data from rural, non-slum urban and slum areas, this is the first study in Bangladesh to explore the prevalence of inadequate DD and its determinants among adolescent boys and girls. The findings of the study revealed that half of the adolescents in Bangladesh consumed less diversified diets, and girls were more likely to have inadequate DD than boys in all socio-economic categories. Poor educational attainment, poor maternal education, female household headship, household food insecurity and poor household wealth were identified as factors significantly associated with inadequate DD in both sexes.
Prevalence of inadequate DD
Our study revealed that in Bangladesh, more than half of the adolescent girls (55⋅5 %) consumed inadequately diversified diets, which is consistent with other studies in Bangladesh. One study conducted during 2017–18 in rural settings found that 53⋅0 % of adolescent girls had inadequate DD(Reference Islam35), which is close to our findings. However, this estimation is lower than the prevalence of inadequate DD among adolescent girls reported from an analysis using national-level databases of Bangladesh reported by Mridha et al. (60⋅4–65⋅3 % in 2014)(Reference Mridha, Hossain and Hassan30) and another recent national-level survey among women aged 10–49 years(26). Besides, results from several small-scale studies in Bangladesh also provided similar estimates though those studies were carried out among adolescent population groups in specific settings, for example, urban slum, schools among pregnant adolescent girls(Reference Shamim, Mashreky and Ferdous25,Reference Nguyen, Huybregts and Sanghvi41,Reference Alam, Rahman and Mia42) . This variation in inadequate DD prevalence within Bangladesh could be due to different methodological aspects such as food grouping, the number of food groups considered, various recall periods, types of the questionnaire (open recall or list-based method) used for data collection, etc., or contextual aspects like seasonality, geographical settings, etc., or might be due to different categories of study participants for different studies(33,Reference Islam35,Reference Birru, Tariku and Belew43–Reference Aurino, Fernandes and Penny45) .
In our study, the prevalence of inadequate DD among adolescent boys (50⋅6 %) was lower than the adolescent girls. As per our knowledge, there is only one study(Reference Islam35) that reported the prevalence of inadequate DD among the adolescent boys. Similar to our findings, the present study identified the lower prevalence of inadequate DD among boys than girls(Reference Islam35). However, several studies in Bangladesh(Reference Leroy, Ruel and Sununtnasuk23,Reference Thorne-Lyman, Shaikh and Mehra46) and other countries reported dietary diversity score (DDS)(Reference Aurino, Fernandes and Penny45,Reference Aurino47,Reference Nithya and Bhavani48) , consumption of foods from individual food groups or inadequate intake at the nutrient level(Reference Leroy, Ruel and Sununtnasuk23,Reference Thorne-Lyman, Shaikh and Mehra46,Reference Venkaiah, Damayanti and Nayak49) among adolescent boys, which are not exactly comparable with our study results. A study in India(Reference Aurino47) reported that among adolescents, DDS among boys was significantly higher (DDS = 4⋅5) compared to girls (DDS = 4⋅1), which in other way indicates higher inadequate DD among girls compared to boys and is similar to our findings. Less favourable dietary practices among adolescent girls compared to boys was also observed in Pakistan(50,Reference Adeel, Awan and Anjum51) . However, a longitudinal multi-country study reported that DDS among boys was slightly lower than adolescent girls in India, but this disparity was not statistically significant(Reference Aurino, Fernandes and Penny45). This higher prevalence of inadequate DD among girls compared to adolescent boys could be due to unequal allocation of food at the household level that advantaged the boys in the consumption of nutrient-rich foods along with other factors such as socio-cultural norms and malpractices as well as different dietary behaviours among girls than boys(Reference Aurino, Fernandes and Penny45,Reference Harris-Fry, Shrestha and Costello52–Reference Herrador, Perez-Formigo and Sordo56) .
Determinants of inadequate DD
Education (adolescent and their parents)
Our findings indicated that poor educational attainment of adolescents was a consistent and strong determinant of inadequate DD among adolescent boys and girls. The risk of having inadequate DD was significantly higher among adolescent boys and girls with no education or among those who did not complete primary education compared to those who had at least secondary level education. In most of the previous studies about the dietary intake of adolescents, the educational accomplishment of them was not examined as a predictor of their DD. However, a few studies in Bangladesh among pregnant adolescent girls(Reference Mridha, Matias and Arnold24,Reference Shamim, Mashreky and Ferdous25) and women of reproductive ages(Reference Harris-Fry, Azad and Kuddus57) also found a positive association between education and DD. On the other hand, we did not find any research that analyzed the determinants of inadequate DD among adolescent boys. It is evident that a low level of food and nutrition literacy is associated with low DD among school-going children(Reference Doustmohammadian, Omidvar and Keshavarz-Mohammadi58) but an understanding of how educational attainment affect diet quality require further exploration.
Since parents, particularly mothers, are the major decision-maker of adolescents’ food intake, parental education, particularly maternal education is considered worthy of examining as an explanatory variable for adolescents’ dietary intake(Reference Akter, Mistry and Mukta28–Reference Mridha, Hossain and Hassan30,Reference Islam35,Reference Aurino47) . Among boys and girls, our data suggested that lower maternal education, which in fact represents both maternal and paternal education (paternal education was highly associated with maternal education), was a significant predictor of inadequate DD. The existing literature indicates that for adolescents’ (irrespective of sex) diet quality, maternal education level is a stronger predictor than the paternal education(Reference Ahmed, Zareen and Khan29,Reference Aurino47,Reference Rashid, Smith and Rahman59) . In urban Bangladesh, one study among school girls reported that poor maternal education was associated with girls’ intake of protein, fat and riboflavin(Reference Ahmed, Zareen and Khan29). Other studies among adolescent girls in Bangladesh and neighbouring countries frequently reported that low maternal education was associated with poor and less diversified diets and lower consumption of nutrient-rich foods(Reference Mridha, Matias and Arnold24,Reference Shamim, Mashreky and Ferdous25,Reference Mridha, Hossain and Hassan30,Reference Adeel, Awan and Anjum51) . Educated parents are more likely to have better nutritional knowledge and awareness and be economically better-off, which might be reflected in their children's diet quality and hence still demand further study.
Household headship
In our analyses, living in a female-headed household emerged as a significant factor that limits the diversity of diet among both boys and girls. In line with our findings, several studies reported that being part of female-headed households is associated with a poor diet in terms of quality and diversity at the individual and household levels(Reference Rashid, Smith and Rahman59,Reference Workicho, Belachew and Feyissa60) . On the contrary, there are studies from South Africa, Tanzania, Dominican Republic that reported female-headed households had a lower risk of inadequate DD at the household level compared to male-headed counterparts(Reference Taruvinga, Muchenje and Mushunje61–Reference Rogers63), which could be due to women’ more involvement in food preparation, decision-making power on the household budget for high-quality diet, etc.(Reference Workicho, Belachew and Feyissa60,Reference Rogers63) .
Findings from our study support the conventional idea that female-headed households are more vulnerable to poor-quality diets at the individual level and also at the household level. Being a household head, a woman is responsible for earning income in the unfavourable labour market, maintaining the whole household, including childcare. As a result, they face a high dependency ratio, which makes the household and the individuals vulnerable to poor diet quality(Reference Harris-Fry, Azad and Kuddus57,Reference Fuwa64,Reference Mallick and Rafi65) . Besides the work burden, female-headed households face unique constraints concerning diet quality through low education, food insecurity and poverty(Reference Buvinić and Gupta66). Though we did not report the education of household heads, our study suggested that inadequate DD was also associated with different levels of food insecurity and low household wealth (see later).
Household food security status
We observed that compared to adolescents from food-secure households, adolescents from mild and moderate food-insecure households had a significantly higher risk of having inadequate DD. Our result supports previous studies conducted among adolescents girls(Reference Mridha, Hossain and Hassan30,Reference Islam35) and among women of reproductive age in Bangladesh(Reference Na, Mehra and Christian67). Moreover, a study found that food insecurity status is linked with lower consumption of animal source foods, vitamin C-rich fruits and vegetables among pregnant adolescent girls(Reference Mridha, Matias and Arnold24). It is already established that household DD reflects household food security, and a considerable association was found between individual level DD and household food security(Reference Ruel10,Reference Kennedy, Razes and Ballard13,Reference Thorne-Lyman, Valpiani and Sun68,Reference Hoddinott and Yohannes69) . Besides, evidence suggests that the three pillars of food security, that is, availability, accessibility and utilisation(Reference Taruvinga, Muchenje and Mushunje61,Reference Steyn, Nel and Nantel70,Reference Hillbruner and Egan71) are associated with DD.
Household wealth status
Our data suggested that adolescent girls and boys from poor households were more likely to have inadequate DD compared to the girls from the wealthiest households. Similar findings have been observed in many other studies in Bangladesh. Different studies reported that poor asset quintile(Reference Mridha, Hossain and Hassan30), low socio-economic status(Reference Mridha, Matias and Arnold24,Reference Ahmed, Zareen and Khan29,Reference Islam35) , low household expenditure(Reference Leroy, Ruel and Sununtnasuk23), low income(Reference Shamim, Mashreky and Ferdous25,Reference Rashid, Smith and Rahman59) , low wealth score(Reference Harris-Fry, Azad and Kuddus57) increased the risk of having inadequate DD among adolescents and women compared to their counterparts. A close look at the ten food groups of DD score, where fruits and vegetables were included in four groups, and animal source foods covered another three groups, could be helpful to explain this association. The consumption of fruits and vegetables along with animal source foods increases with income in Bangladesh like many other developing countries(Reference Arimond and Ruel22,Reference Mridha, Matias and Arnold24,Reference Singh, Acharya and Gautam72) ; hence poor households cannot afford the animal source foods in the first place. Besides, poor household members prioritise fulfilling the basic energy requirement from staples foods to get rid of hunger within their budget allocation for foods(Reference Ruel9). Moreover, the lack of knowledge about the health benefits of vegetables and fruits and the personal preference of adolescents from poor households limits the consumption too(Reference Ruel9,Reference Singh, Acharya and Gautam72) . Thus, lower economic conditions act as a risk factor for inadequately diversified diets among adolescents.
Strengths and limitations
The present study has several strengths over other studies of this kind. Firstly, the present study used the latest national-level survey dataset, covering rural, non-slum urban and slum areas and collected at the community level. Thus, the results of the present study could be generalised to the entire adolescent population. Secondly, for the first time in Bangladesh, adolescent boys were included for a comprehensive assessment of their dietary practices, which is a timely response to the urgency of gender-segregated data on the diets of adolescents. Lastly, previous studies on DD mostly used DDS as a measure of diversified diets, but there were no clear cut-off points to define as ‘adequate’ of ‘inadequate’ DD, which was crucial for advocacy and to take public health actions(Reference Harris-Fry, Azad and Kuddus57); our study will serve this purpose perfectly. Based on the findings of the present study, national policies and programmes could be designed to address inadequate DD among adolescent boys and girls who need it most, considering the identified determinants and their socio-economic stratification.
However, our study has some limitations too. ‘We had to drop several rural clusters due to some administrative and financial hurdles which might have affected the representativeness of the study’. As the data source of the present study is a cross-sectional survey, it must be acknowledged that associations were estimation and causality cannot be determined from these findings. Besides, there are many other sets of explanatory variables omitted from the model that may have predictive power on inadequate DD among adolescents such as behavioural, cultural and environmental, here we just considered the socio-economic factors. More research must be done to understand better how these factors employ their impact on diet among adolescents, particularly since the variance in the outcome variable was largely unexplained. Besides, all dietary data were self-reported, and it is evident that dietary recall in adolescents affected by lack of motivation and willingness, and thus, assessment of dietary intake of adolescents can be subject to underreporting and misreporting(Reference Ochola and Masibo44,Reference Masibo73,Reference Livingstone and Robson74) . It may have exaggerated responses non-randomly across the study participants. Moreover, we used a list-based recall method for dietary data collection in the last 24 h only, which tends to provoke biased towards socially desirable responses, such as untrue positive responses for high-status foods (e.g. meat) compared to the open recall method. Besides, a single 24 h recall has its own limitation regarding inability to capture day-to day variation.
Conclusion
We found that more than half of the adolescent boys and girls consume inadequately diverse diets in Bangladesh, and the prevalence of inadequate DD was higher among girls than boys. Our study also identified that a number of socio-economic risk factors such as lower educational level of adolescents and their parents, living in female-headed, food insecure and poor households were associated with inadequate DD among adolescent boys and girls in Bangladesh. These findings have manifold operational and policy implications for improving adolescents’ DD in resource-poor countries like Bangladesh. Gender disparity and socio-economic inequity of adolescents’ DD emerged from the present study should be addressed through policy interventions. At the household level, broader poverty alleviation initiative, particularly for female-headed households, is necessary to address inadequate DD among adolescents through improving households’ economic and food security status, which will, in turn, enable households’ accessibility to nutrient-rich diversified foods. Hence, investing in adolescents would be the best utilisation of resources not only for the betterment of adolescents themselves but for the future generations.
Acknowledgements
We acknowledge all the study participants, research assistants, field supervisors, community leaders, the local administrators, all the supporting staff of the BRAC James P Grant School of Public Health and Institute of Public Health and Nutrition, and members of the Technical Advisory Committee for their support during this work. We also acknowledge the National Institute for Health Research (NIHR), UK, and the Wellcome Trust, UK, for supporting some of the co-authors with salaries and administrative help while writing the manuscript.
The study was funded by the National Nutrition Services (NNS), Institute of Public Health Nutrition, Ministry of Health and Family Welfare, Government of Bangladesh (Memo: 45.165.032.01.00.003.2016-325; Date: 10-12-2017). Besides, salaries and administrative support for some of the authors came from the National Institute for Health Research (NIHR) (16/136/68), using UK aid from the UK Government to support global health research and by Wellcome Trust (212945/Z/18/Z). The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care.
F. A. conceptualised and drafted the initial manuscript. M. M. H. conducted the data analysis. A. A. S., M. S. A. K., M. H., A. A. M. H., M. He., N. J. U., M. A. U., S. K. S., S. M. M. R., D. K. M. and M. M. I. B. were involved in the conceptualisation and design of the study as well as reviewed and approved the final version of the manuscript. M. K. M. led the design and implementation of the whole research project, approved the data analysis plan, critically reviewed the manuscript and approved the final manuscript. All authors read and approved the final version of the manuscript.
The authors declare that they have no conflict of interest.






 Open access
Open access