


INTRODUCTION
The ability to act upon intentions is fundamental, and disruption of this ability by brain injury or disease can have important functional consequences. This finding is a common component of the Dysexecutive Syndrome (Baddeley & Wilson, 1988), a cluster of behavioral and cognitive changes that are relatively common consequences of brain injury. Executive processes have been particularly associated with functions of the prefrontal cortex (D'Esposito et al., 1995; Duncan & Owen, 2000; Milner, 1982; Shallice, 1982).
Many models of frontal and/or executive function could accommodate difficulties in acting on intentions (e.g., Dehaene et al., 1998; Duncan, 2006; Shallice & Burgess, 1996; Stuss, 2006). One conceptualization that applies particularly well to this deficit is that of goal neglect (Duncan et al., 1996), a phenomenon whereby a goal that has been understood and well-remembered is not acted upon as intended. Initially observed in patients with focal frontal damage (Duncan et al., 1996), and subsequently in people with head injuries (Duncan et al., 1997), it is thought at a neural level to be related to dysfunction of a frontoparietal network. Duncan (2006), drawing together work from primate neurophysiology, human functional magnetic resonance imaging (fMRI) and neuropsychology, proposed that a “multiple demand” network adjudicates between inputs competing for attention. In the intact system, this results in the strongest competitive weight being assigned to the most goal-relevant input. The damaged system is inefficient, so goal neglect errors result, in the context of more generalized disorganization of goal-directed behavior.
In understanding everyday problems of goal neglect, it can be helpful to examine the properties of the tasks at hand. Ellis (1988) distinguished types of delayed intentions, or Prospective Memory (PM) tasks, in terms of their specificity in time. She referred to intentions with a specific time for action (e.g., intending to watch a television program at 8 p.m.) as “pulse” intentions, and those that could be enacted over a broader time period (e.g., intending to phone the bank some time today), as “step” intentions. Ellis found differences in the memory aids spontaneously used by neurologically healthy participants to support these intentions, with diaries being frequently used for pulses, but rarely for steps. This difference was ascribed to the difficulty of assigning retrieval cues to step intentions. This classification has implications for the way we view intentions, and the way compensation for deficits in this area should be approached.
Turning to the rehabilitation of executive function more broadly, several group studies have shown that training in the use of step-by-step problem solving frameworks can be beneficial to people with executive dysfunction following brain injury (e.g., Levine et al., 2000; Rath et al., 2003; von Cramon et al., 1991). A limitation of these types of training, however, is the requirement for patients to abstract general principles from the specific training context and subsequently recognize the relevance of strategies for activities performed in different settings, as demands are placed upon the compromised resources. Lawson and Rice (1989) noted this difficulty in a single case study, finding that executive deficits limited generalization of memory strategy use. In this instance, combined executive and memory strategy training was effective.
Although these are promising findings, the initiation component of strategy use remains problematic. For this reason, it has been argued that portable cueing devices could be used to bring the trained techniques to mind during performance of everyday activities (Manly et al., 2002).
This principle has been illustrated in a series of experiments involving participants with acquired executive dysfunction. These have demonstrated that linking external cues with the process of monitoring current behavior in light of overall goals—cueing an “executive review”—facilitates executive performance. This effect has been demonstrated in laboratory tests of sustained attention and multitasking (Manly et al., 2002, 2004), as well as a naturalistic PM task (Fish et al., 2007).
Given the dramatic changes in the availability and cost of items that can be used for these purposes, there is a considerable body of research supporting the use of watch alarms, mobile phones, personal digital assistants, and so on as aids for memory and planning (see Kapur et al., 2004 for a review).
One remaining drawback of these systems is that they still rely, to varying extents, upon clients themselves to program and maintain the system. This is one of the advantages of externally managed paging systems, such as NeuroPage (Hersh & Treadgold, 1994). This involves using radiopaging technology to send reminder messages to alphanumeric pagers according to a specified schedule. The pager is easy to use, and administrative staff are responsible for setting up and maintaining the system. Two research trials have demonstrated the efficacy of NeuroPage, showing on average, a 30% increase in attainment of individually specified goals (Wilson et al., 1997, 2001). In addition to group studies examining efficacy, individual case reports can provide practical information regarding how pagers might be used.
In this respect, Evans et al. (1998) published a case report on the use of two compensatory aids in the rehabilitation of R.P., who had a selective impairment in translating intention to action. The first aid was a pager (NeuroPage), used to remind R.P. of planned activities and appointments. In other words, the pager gave her explicit reminders to immediately undertake specific activities, prompting pulse intentions. The second aid, a checklist, was used to regulate perseverative behavior in R.P.'s morning routine (see case history, below). Some years following the Evans et al. (1998) report, R.P. replaced the pager with an electronic organizer, in an attempt to increase her independence. Initially this was reported to be successful, however, the effectiveness declined, possibly because of the burden on R.P. to set the reminders herself.
This study describes new work with R.P., more than 10 years on from the previous report. Specifically its aims are:
- To examine possible changes in R.P.'s cognitive function that might account for the decline in previously effective compensatory strategy use—or contraindicate the reintroduction of similar interventions.
- To report a controlled reintervention with R.P., which in contrast to the previous report, separately compares the effects of two strategies on a revised set of rehabilitation goals. Reports of “reinterventions” are rare and provide clinically valuable information. Additionally, the direct comparisons between the pager and checklist strategies allow inferences to be drawn regarding the mixed outcomes from R.P.'s prior use of compensatory strategies, with obvious implications for other people with similar problems. We hypothesized that the pager would be the superior intervention, as its ability to automatically interrupt current activity would increase R.P.'s propensity to review her aims and intentions.
- To examine whether strategy use is effective not only for pulse intentions (such as those common in previous NeuroPage studies), but also for step intentions. Here, the aim would be to interrupt R.P. and focus her attention on her more broadly specified goals, irrespective of whether immediate action was required (see goal setting, below).
CASE DESCRIPTION
R.P. is a 60-year-old woman who, aged 42, suffered a subarachnoid hemorrhage (SAH). Three-vessel angiography revealed three aneurysms: one situated at the anterior communicating artery (ACoA) complex, directed inferiorly (which was thought to have caused the SAH); one at the origin of the anterior choroidal artery (AChA); and a further on the right middle cerebral artery (MCA), distal to the lenticulostriate arteries. The ACoA and AChA aneurysms were clipped 5 days later, while the MCA aneurysm was untreated. Eighteen hours after surgery, cerebral vasospasm caused a severe ischemic neurological deficit. Computed tomography (CT) showed low attenuation areas in the right frontal lobe, in anterior and medial regions, extending superiorly to the parasagittal area. A smaller area of low attenuation was seen in the left inferior medial frontal lobe, thought to represent ischemia (confirmed by a further scan 4 years later). In the days after surgery, R.P.'s consciousness fluctuated, she was alert but essentially akinetic and mute for 3 weeks. She remained in a rehabilitation unit for 9 months.
R.P. has 11 years of education, and premorbidly had a variety of jobs. Most recently she was a school science technician. She lives with her husband, J.P., who is her full-time caregiver.
Previous Problems and Rehabilitation
Evans et al. (1998) used a paging system to remind R.P. of her regularly scheduled activities, which without assistance, she often failed to complete. The activities were taking medication, attending a voluntary placement, washing clothes, and watering plants. The second strategy, a checklist, addressed what was referred to as an obsessive–compulsive type problem. R.P. spent up to 90 min in the bath, engaged in a routine involving washing 33 body parts in sequence. She would lose track of her location in the sequence, and start again at the beginning. The checklist limited this sequence to eight body parts, and allowed R.P. to record the amount of time the routine took. This time was consistently reduced to 30 min. The authors noted that the obsessive–compulsive problem lacked the associated emotional component that would be expected with true Obsessive Compulsive Disorder. Such stereotyped or obsessional behavior is not unprecedented in disorders with medial frontal involvement (e.g., Berthier et al., 1996; Nyatsanza et al., 2003).
The pager was used for approximately 5 years. When an opportunity arose to replace the pager with an electronic organizer, R.P. and J.P. chose to do so. They state that this change was because a self-programmed system offered a greater degree of flexibility than the pager, and consequently had potential to increase R.P.'s independence.
The Current Investigation
At the time of the current follow-up study, the electronic organizer was no longer in use. The couple stated that R.P. had been able to program the device and that it had been somewhat useful, but use of it waned and eventually ceased altogether. The reason behind this, according to J.P., was that the pager messages, unlike those from the organizer, were perceived by R.P. as coming from an external source. The implication seems to be that either R.P. exhibited greater compliance with cues perceived to be coming from a professional or clinical source, or that strategies were more effective when they took advantage, as the pager apparently did, of her urge to help others out. They reported that R.P. was again experiencing significant problems regarding disorganized behavior. R.P. was unreliable in her execution of important tasks such as taking her medication and more generally, chores around the house. She was aware that these tasks should be done, and actively wanted to do them, but was unable to get past the “knowing” and “wanting” to the “doing” stages of these intentions.
R.P. spent a long time getting ready each morning (5 hr), and again in the evening (90 min). Bathing was no longer a problem as her physical difficulties necessitated assistance from J.P., preventing R.P. from engaging in an overly perseverative routine. However, other parts of her routine now had compulsive or perseverative aspects. For example, R.P. would spend a long time cleaning her teeth, getting together various toiletries, applying moisturizers, and washing her glasses. J.P. referred to R.P.'s behavior as “compulsive.” He stated that if asked to stop, or focus on what she was doing, then she would do so, but that “as soon as my back's turned, she'll start again.” Again, there was no sense that R.P. experienced an emotional response if her routine was interrupted—just that she appeared unable to do this herself. Additionally, J.P. reported that R.P. was distractible, and frequently flitted between tasks without accomplishing anything. The evening routine was similar in nature.
This obviously restricted the couple's other activities, effectively preventing them from leaving the house before midday. Both R.P. and J.P. were motivated to attempt to improve their situation.
Ten-Year Follow-Up Assessment
A battery of standard tests, including those reported in Evans et al. (1998) was administered over five sessions. Overall, this testing revealed remarkably little change in performance over the 10 years between assessments (see Table 1).
R.P.'s neuropsychological test scores from previous and current assessments

R.P.'s performance on tests of general intellectual function (Wechsler, 1997), naming (Graded Naming Test, McKenna & Warrington, 1983) and memory (Doors and People, Baddeley et al., 1994; Rivermead Behavioural Memory Test, Wilson et al., 1985) were all in the average range (see Table 1 for details). Verbal fluency and Trail Making Test (Reitan, 1958) scores were impaired on prior testing, but upon second testing, letter fluency and trails A were within the normal range (Lezak, 1995). As part of a separate research project around 6 months later, letter fluency was administered a third time. On this occasion, R.P.'s performance was in the impaired range, which strongly suggests that the increase reflected normal variation. R.P.'s performance on subtests of the Test of Everyday Attention (TEA; Robertson et al., 1994), which assesses selective attention, sustained attention, and attentional switching, was inconsistent. On the Cambridge Prospective Memory Test (CAMPROMPT; Wilson et al., 2005), which includes six tasks to remember to perform over a 30-min period, R.P.'s performance was classified as poor, with failures relating to task initiation rather than retention of intention content.
R.P.'s performance on tests of executive function was very mixed, which is understandable given the relative insensitivity of structured testing in detecting executive problems (Burgess et al., 2006). R.P. performed in the low average range overall on an ecologically valid test battery, the Behavioural Assessment of the Dysexecutive Syndrome (BADS; Wilson et al., 1996), and was well within the normal range on the modified Wisconsin Card Sorting Test (Nelson, 1976), but was markedly impaired on a BADS subtest, the modified Six Elements Test (see Shallice & Burgess, 1991; Wilson et al., 1996), and on the closely related Hotel Test (Manly et al., 2002).
The Hotel Test is functionally similar to the type of situations with which R.P. has daily difficulties, and this may account for its greater sensitivity compared to other executive measures. In this test, participants are presented with five simple tasks to attempt over a 15-min time period. Each task would take longer than 15 min to complete, so the challenge is to spend as much time as possible on each, whilst attempting all five—the optimal strategy being to change task every 3 minutes. Control subjects almost invariably attempt each task within the allotted time. R.P. was able to accurately report the aim of the test both pre- and posttesting, yet she attempted only two tasks, despite receiving a verbal prompt reminding her of the aim halfway through the task. A feature of her performance was that, during the relatively undemanding component tasks (e.g., sorting coins) she tended to try to initiate conversation with the assessor about unrelated matters. This appeared to prolong performance of whichever component task she was undertaking and increase her “neglect” of the main goal—despite, as discussed, this being well understood and retained (in purely mnemonic terms) across the duration of the task.
Summary of Assessment
The two assessments have shown that R.P. has well-preserved general intellectual and mnemonic functioning. It is noteworthy that R.P. showed clear impairments on tests that involve the coordination of multiple tasks (Six Elements and Hotel Tests).
The assessment results fit extremely well with J.P.'s reports of R.P.'s problems (i.e., acting “compulsively”), getting engrossed in activities unrelated to more pressing goals, and starting many tasks without completing any. We, therefore, concur with Evans et al. (1998), R.P. has impairment in translating intention to action, particularly when there is competition from multiple tasks, whereas her more basic cognitive functions are relatively well-preserved.
Rehabilitation
Establishing goals for intervention
Goal-setting took place in a session with R.P. and her husband who together decided that the goals were (1) To reduce the time R.P. spends getting ready in the morning from an estimated 5 to 3 hr (from waking to being ready to leave the house). (2) To reduce the time R.P. spends getting ready to go to bed from an estimated 90 to 30 min. (3) For R.P. to remember to take her medication three times per day (at 9 a.m., 6 p.m., and 9 p.m.), without J.P. prompting her.
Design
Our aim was to establish whether the reintroduction of the previously effective strategies would again be effective in reducing R.P.'s difficulties and to do so in a way that allowed us to separately examine the checklist and paging components. To this end, an alternating treatments design (Barlow & Hayes, 1979) was used to separately evaluate two strategies. After a baseline phase (A1–14 days), a checklist was introduced (B1–14 days), followed by a further baseline period (A2–14 days), an amended checklist (B2–14 days), further baseline (A3–4 days), the NeuroPage phase (C–17 days), baseline (A4–7 days), and combined pager and checklist (D–14 days) phases. These time intervals were designed to fit with R.P.'s schedule and to provide a strong basis for statistical inference regarding the efficacy of the interventions. The treatment order was dictated by the practicalities of conducting this type of research. We wanted to commence intervention as soon as possible, for R.P. and J.P.'s benefit. As the pager took some time to obtain, whereas use of the checklist could begin with relatively little preparation, introducing the checklist first offered the best solution. (It should be noted that this design may preferentially benefit treatments introduced later rather than earlier. Considering the results, however, this seems highly unlikely, both in terms of the magnitude of the effects and the immediate return to baseline-level performance upon removal of treatment seen in phase A4.)
Data recording
Over the length of the study, J.P. used a diary to record the time spent getting ready, in minutes, for both the morning and evening routines, and whether or not R.P. needed a prompt to remember to take her medication. Data collection complied with the regulations of our institution.
Strategies
The checklist
In the goal-setting session, R.P. and J.P. listed the stages that made up R.P.'s morning and evening routines. These stages formed the three sections of the checklist, one for the morning routine, one for the evening routine, and one for medication. Each stage was simply named (e.g., “put on make-up”), rather than described in any detail, as R.P. knew what she was supposed to be doing in each section. Each stage also had a box to tick as it was completed. There was additional space for R.P. to record the total time she had taken, as Evans et al. (1998) found that this was a crucial factor in their intervention.
One new item was added to the checklist in the second phase (B2). This was to have the radio rather than the television on during breakfast. As R.P. found the latter rather absorbing, it was more likely to distract her from other aspects of her routine.
The paging strategy
Fourteen messages were automatically sent daily by the NeuroPage system to an alphanumeric pager worn by R.P. (see Table 2). The message schedule was created by R.P. and J.P. in a meeting before the commencement of the NeuroPage phase (C).
Structure of R.P.'s message schedule
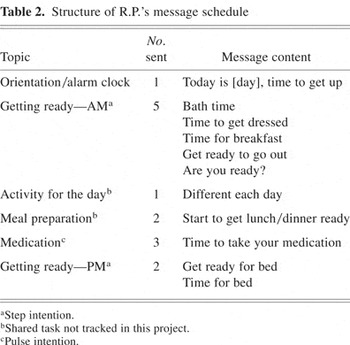
Goals 1 and 2: Getting ready. Seven messages referred to a series of stages necessary for R.P. to achieve the generally specified goal of getting ready more quickly (the step intention). Five messages were sent in the morning and two in the evening. The aim was not so much to prompt immediate action, as to heighten awareness of the overall intention and thereby influence subsequent actions. For example, one of the morning messages said “bath time.” R.P. had several related activities that were prompted by receipt of this message. The pager message did not explicitly state each of these substeps, but rather prompted the initiation of a series of tasks to reach the overall goal.
Goal 3: Taking medication. Three messages gave specific instructions regarding tasks to be immediately acted upon—for the goal of achieving independence in taking medication (a pulse intention). The remaining four messages referred either to tasks jointly completed by R.P. and J.P. or ones that required no overt action (see Table 2).
RESULTS
Visual analysis of the time-series data (Figure 1) suggests a positive effect of the pager in comparison with baseline and checklist phases, for all three measures. The impact of the checklist is less clear, but there is a possible effect upon the evening routine and medication measures. There is also a suggestion that time engaged in the evening routine declined steadily over time. For these reasons, statistical analyses were required. Additionally, several authors have advocated the implementation of both visual and statistical analyses in single-case designs (Brossart et al., 2006; Morley & Adams, 1991).

Graphical representation of the three behavioral measures over each phase of the study. A phases represent baseline, B1 and B2 are checklist phases, C is the NeuroPage without checklist phase, and D is the NeuroPage plus checklist phase. Dotted lines represent R.P.'s target level.
The data showed evidence of serial dependency, with autocorrelations around .3 for all measures. This is common with time-series data, and means that data points close in time are correlated to a greater extent than those further apart (Hersen & Barlow, 1976). This finding makes standard t and F tests inappropriate, as they assume independence of data points. We, therefore, used ARIMA (autoregressive integrated moving average), an interrupted time series model (Hartmann et al., 1980), with a first-order autoregressive model, which makes an allowance for serial dependency (Box & Jenkins, 1970; Robertson et al., 1995). Due to the large number of comparisons resulting from this analysis, we used Bonferroni-corrected p values, taking into account the degree of correlation (r = .55) between measures. This strategy resulted in an adjusted 5% value of .015, and 1% value of .003.
As shown in Tables 3 and 4, there was no difference in the length of time taken in the morning routine when using the checklists in comparison with baseline (ABAB comparison, with A and B phases collapsed). There was, however, a significant reduction (12.58 min) in the duration of the evening routine [t(52) = 2.767; p = .008]. There was also a significant improvement in medication adherence, with R.P. achieving on average one more unprompted dose of medication with the help of the checklist [t(52) = 2.788; p = .007]. The two types of checklist differed only in their effect on evening routine, but this effect was significant only at the 5% threshold [t(25) = 2.744; p = .011]. As is obvious from the visual representation of the data, the checklists were not nearly so effective as the pager, which, compared with baseline (all A phases collapsed vs. C) resulted in:
(1) a 60.8-min reduction for the morning routine [t(74) = 11.762; p = 10−8],
(2) a 37.47-min reduction for the evening routine [t(73) = 10.747; p = 10−8], and
(3) perfect performance (1.03 independent dose increase) in taking medication (t(74) = 9.331; p = 10−8]
Descriptive statistics of the three target behaviors over each phase of the study

Autoregression analysis comparing the effects of the strategies against baseline and directly comparing the different types of strategy
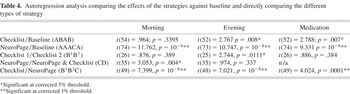
Performance during the NeuroPage-only phase was significantly better than the checklist-only phases for all measures, with a reduction of 58.5 min in the morning routine [t(49) = 7.399; p = 10−7], 29.9 min in the evening routine [t(48) = 7.021; p = 10−7], and a .54 increase in medication doses achieved without verbal prompting [t(49) = 4.024; p = .0001].
There was a significant difference in time taken to complete the morning routine between the NeuroPage and NeuroPage plus checklist phases (C vs. D), showing a 17.9-min reduction in favor of the latter [t(35) = 3.053; p = .004], although this was not seen in the evening and medication measures.
Aside from the statistical significance, it is clear that R.P. consistently reached her goals on all three measures with the paging intervention. She occasionally achieved this in the baseline and checklist phases, but not consistently. From the perspective of patients and their caregivers, the reliability of an effect may be as, or more important than its absolute magnitude.
Six-Month Follow-Up
R.P. continues to use the pager, without the checklist. Both she and J.P. report that they are happy with this, and that it is working well. R.P. appears to very much enjoy using the pager. The message schedule remains the same, with one addition. Given the success of the generally specified goal messages (related to R.P.'s routines), an even more general message (“stop and think about what you're doing”) is now sent at 11 a.m. and 2.30 p.m. 3 days per week. This is to encourage R.P. to focus on her goals, whatever they happen to be. Although the effect of this particular message has not been formally evaluated, after using it for a period of 6 months, the couple says that they find it useful.
Reflecting upon the changes they have experienced while using the pager again, J.P. reports that they have more free time. As a result of this, their potential for social participation has increased—they can accept appointments and social engagements that take place in the morning, even on the spur of the moment. Before re-initiating the paging system, this would have been almost impossible. In J.P.'s opinion, the pager works better for R.P. than other strategies because the messages have an external origin. He sees this as beneficial both because R.P. is not required to program the device herself, and also because it adds to the sense of the pager being a “friendly helper.”
DISCUSSION
This case study investigated compensatory strategy use in R.P., a patient with specific executive deficits secondary to bilateral frontal lobe damage. Before the current investigation, R.P. had used two strategies in conjunction, a pager and a checklist. After several years R.P. began to use a self-programmed device, which was only effective in the short-term. At 10-year follow-up, it became clear that R.P.'s everyday difficulties had returned. Repeat neuropsychological assessment showed no discernible change in R.P.'s test scores, suggesting that the decline in strategy use did not stem from increased cognitive impairment. An alternating treatments design was used to differentiate between the two strategies that were previously used in combination. Although the checklist resulted in a statistically significant improvement on two of the three goals, the pager was associated with greater and more consistent functional gains.
The behavioral manifestations of R.P.'s deficits seems to fit well with dysfunction of the “multiple demand” network—R.P. is unable to appropriately direct her behavior to achieve the most important goal. This is most noticeable in the face of multiple competing demands. She engages in task-irrelevant behavior, fails to monitor her behavior, seems to forget what she is doing, and flits from task to task. Her lesion is certainly compatible with disruption to this system.
An interesting aspect of the current study is the differential effectiveness of the pager and checklist strategies. This does not seem to stem from R.P. simply neglecting to use the checklist, as her compliance with both strategies was excellent and she diligently completed the checklists throughout. Therefore, in both the checklist and pager strategies, R.P. was receiving reminders about what she should be doing and yet these were much more effective coming from the pager. While speculative without further data to constrain the issue, it is relatively easy to imagine the type of factors that might be at work. First, as suggested by Evans et al. (1998), the pager makes a loud bleep, drawing attention in a way that a checklist cannot. Second, while R.P. presumably consulted the checklist during pauses in activity or between activities, the pager can interrupt ongoing and potentially suboptimal behaviors. Finally, although delivered automatically, information relayed by the pager may be experienced as if coming from another person, which may facilitate a form of social compliance in a way not achievable by the paper checklist. As suggested by J.P., a similar factor may have accounted for the decline in use of the self-programmed organizer.
One might wonder why the checklist, which was very effective in limiting R.P.'s bathing routine in Evans et al. (1998), did not have a beneficial effect upon her current morning routine. This disparity may be attributable to differences in the goals themselves, the components of the bathing routine being more amenable to constraint than those of the morning routine targeted here.
An important issue addressed in this case is the support of general goals (or “step” intentions: for example, following a routine but without a specific initiation time) in addition to specific ones (“pulse” intentions: e.g., taking medication at a given time). In Evans et al. (1998), specific messages were designed to cue immediate specific action. However, by the time of the current study, R.P. had few such “pulse” activities and most of her goals now lacked a specific window of time in which they had to be met. This necessitated a different approach to message schedule construction. While the logic and mechanisms of a specific cue leading to immediate action are relatively straightforward, as Ellis (1988) stated, it is inherently difficult to create strategies to aid performance of step intentions. The beneficial effects of pager messages upon R.P.'s step intentions are reminiscent of those observed in recent studies that have linked the provision of a general external cue (“think about what you should be doing”) with the process of reviewing intentions (Fish et al., 2007; Manly et al., 2002, 2004). As noted, these studies suggest that provision of such cues can be sufficient to help people with executive dysfunction actively review current and future goals, with positive consequences for behavior. Like those participants, R.P. knows the content of her goals, such as when she should take her medication. She also, according to her report, wants to act upon them. Despite this, she finds it incredibly difficult to fulfill them without the pager. Although R.P.'s messages were not quite as general as “think about what you are doing” (e.g., referring to the “night-time routine”), they nevertheless may have served a similar purpose, drawing attention to thinking about these more general goals.
The current results suggest that use of compensatory strategies for executive dysfunction can hold significant benefits for day-to-day function, even when the difficulties may not initially seem amenable to this type of approach; previous attempts have been met with limited success; or use of previously successful strategies has ceased. It also illustrates the benefits of using automated reminding systems, which can extend much further than merely reminding people to do things. For caregivers, having to continually remind someone can be extremely draining. For the patient, such reminders may be perceived as nagging. This is likely to increase stress on both sides and may also be detrimental to the very goal of prompting action. In contrast, a pager is clearly benign, and crucially, is under the control of the patient. It may be the subsequent effects upon mood, relationships, and social participation that are equally important and justifiable uses of such systems.
ACKNOWLEDGMENTS
We thank R.P. and J.P. for the dedication and enthusiasm they showed throughout the course of this work. Thanks also to Jon Evans and Hazel Emslie for useful discussions during the early stages of this project; to Andrew Bateman and Janet Beveridge at the Oliver Zangwill Centre for their help with setting up the pager; and to the anonymous reviewers for their insightful comments. The authors have no financial interests in the NeuroPage service. This work was supported by the UK Medical Research Council.





