

1 Introduction
The Domain-Specific Risk Taking scale (DOSPERT) (Blais & Weber, Reference Blais and Weber2006; Blais & Weber, Reference Blais and Weber2009; Weber, Blais, & Betz, Reference Weber, Blais and Betz2002) measures risk attitudes (willingness to engage), risk perceptions, and expected benefits for a set of activities organized into five domains: ethical, financial, health/safety, recreational, and social risk taking. Conceptually, DOSPERT assumes that risk perceptions and attitudes may differ among domains, and has often been used to examine whether willingness to engage in an activity is negatively associated with perceptions of the riskiness of the activities and positively associated with expected benefits (the so-called risk-return framework) (Sarin & Weber, Reference Sarin and Weber1993).
Studies that have compared conventional risk attitudes (willingness to engage in activities defined objectively as risky) with perceived risk attitudes (willingness to engage in activities that the respondent themselves perceives as risky) across domains suggest that people may be more consistent in their perceived risk attitudes than in their conventional risk attitudes (Weber et al., Reference Weber, Blais and Betz2002; Weber & Milliman, Reference Weber and Milliman1997).
A particular strength of DOSPERT is that it is available in several translations and risk attitudes and perceptions have been studied in participants in Quebec (Blais & Weber, Reference Blais and Weber2006), Germany (Johnson, Wilke, & Weber, Reference Johnson, Wilke and Weber2004), China (Cheung, Wu, & Tao, Reference Cheung, Wu and Tao2012; Hu & Xie, Reference Hu and Xie2012), and South Africa (Szrek, Chao, Ramlagan, & Peltzer, Reference Szrek, Chao, Ramlagan and Peltzer2012). Most of these studies have found within-nation domain-specificity in risk attitudes and perceptions (often with less interdomain variation in perceived-risk attitudes) and differences in levels of risk attitude and risk perception across nations or cultures (although not all made direct comparisons among cultures within the same study). A Japanese translation of DOSPERT was performed between 2006–2009 by Yusuke Takahashi at the University of Illinois (Takahashi, n.d.) but use of a portion of this translation only been reported in two Japanese publications (Hirahara & Yamagishi, Reference Hirahara and Yamagishi2009, 2011).
DOSPERT is also one of the few instruments Harrison et al. (Reference Harrison, Young, Butow, Salkeld and Solomon2005) recommends for assessing health-related or clinical risks. However, DOSPERT does not include a domain that focuses on health care activities; the health/safety scale is limited to preventive behaviors, and two Japanese studies suggest that health/safety risk perceptions are not related to perceptions of treatment risks by breast or blood cancer patients (Hirahara & Yamagishi, Reference Hirahara and Yamagishi2009, 2011). Butler et al. (Reference Butler, Rosman, Seleski, Garcia, Lee, Barnes and Schwartz2012) developed and provided initial psychometric evidence for an add-on medical risk domain consisting of six activities, modeled after the other DOSPERT domains. Adding the new domain’s items to the standard DOSPERT items produces a 36-item instrument that we refer to as DOSPERT+M. Rosman et al. (Reference Rosman, Garcia, Lee, Butler and Schwartz2013) administered DOSPERT+M to a nationally-representative U.S. sample and found that the medical risk domain appeared to measure a different construct than the health/safety domain. We sought to determine whether the same distinction would be observed in Japan, as a question of generalizability (rather than a cross-cultural comparison).
The goals of this study were to (1) translate the medical risk domain items to Japanese to create a Japanese DOSPERT+M, (2) administer the Japanese DOSPERT+M instrument to a representative sample of the Tokyo metro population, and (3) characterize risk attitudes, including medical risk attitudes, among the sample and examine the associations among domains. We take the DOSPERT+M instrument as pre-existing; our focus is application rather than item selection or the development of validity evidence per se. We specifically sought to examine whether the DOSPERT factor structure could be recovered in the data, whether perceived-risk attitudes were more stable across domains than willingness to take risks, and whether the DOSPERT health/safety scale was or was not associated with the DOSPERT medical scale.
2 Translation
2.1 Initial Translation
Takahashi’s Japanese DOSPERT, including the 30 DOSPERT items (based on the Blais and Weber, Reference Blais and Weber2006 “revised” DOSPERT) and the 3 DOSPERT response tasks/scales was used as the basis for the Japanese DOSPERT+M. The DOSPERT+M uses 7 anchors in the expected benefits task, but the original DOSPERT uses only the two extremes and midpoint for anchors in this task (and thus only those three anchors appear in Takahashi’s translation). The 6 medical risk items and the 4 missing expected benefits anchors were translated to Japanese using the approach advocated by Weidmer et al. (Weidmer, Hurtado, Weech-Maldonado, Ngo-Metzger, & Bogen, Reference Weidmer, Hurtado, Weech-Maldonado, Ngo-Metzger and Bogen2006) for the translation of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) surveys administered by the U.S. Agency for Healthcare Research and Quality. Specifically, two independent forward translations were produced by co-authors who are native Japanese speakers (NH and HO). A third co-author (KY) served as the translation reviewer and compared the original English item with each of the two Japanese translations. The translation reviewer selected which translation was preferable or reconciled the two translations into a third translation. Finally, all three translators reviewed the final versions of items and anchors and approved their use. Table 1 presents the medical risk domain items in English and Japanese translation.
Table 1: DOSPERT+M medical risk items in English and Japanese

2.2 Application Issues
Following the DOSPERT+M translation, during survey preparation, Research and Development, the Japanese survey company managing the online panel indicated that six of the original DOSPERT items were not useable in Japan according to the Japanese Marketing Research Association code because survey researchers are not permitted to ask about participation in illegal activities. These items, and their domains, are listed in Table 2.
Table 2: DOSPERT activities illegal in Japan (Research and Development, personal communication, 2012)

For the ethics and health/safety items, we presented reversed items (e.g. “Not taking questionable deductions on your tax return”) to respondents but omitted them from the data analysis as they clearly were not going to measure the same construct. Instead, we constructed abbreviated subscales for these domains without the illegal activity items. Gambling privately is illegal in Japan, but regulated gambling is allowed. Accordingly, for the financial items, we replaced these items with acceptable forms of gambling: “Betting a day’s income at a Pachinko game” (一日分の収入を、パチンコに費やす) and “Spending a day’s income for gambling such as a horse race, bicycle race, or boat race” (一日分の収入を、競馬、競輪、競艇といった賭け事に使う).
The two earlier Japanese studies employed only the health/safety items of the original Japanese DOSPERT translation (Hirahara & Yamagishi, Reference Hirahara and Yamagishi2009, 2011) and only the risk perception task. These studies were conducted as part of interviews with patient support groups and not as large-scale survey research, did not ask about willingness to engage in activities, and were not examined in the context of the Japanese Marketing Research Association code. We thus faced this problem for the first time.
3 Study Methods
3.1 Instrument
The 36 DOSPERT+M items, each describing a risky activity, can be presented in any of the three standard DOSPERT tasks (risk-taking, risk perception, or expected benefit). In the risk-taking task, participants indicate their likelihood of participating in the activity on a 1–7 scale from extremely unlikely to extremely likely. In the risk perception task, participants indicate how risky they believe the activity is on a 1–7 scale from not at all risky to extremely risky. In the expected benefit task, participants indicate the benefits they believe they would receive from each activity on a 1–7 scale from no benefits at all to great benefits. To reduce respondent fatigue, each participant was block-randomized to receive two of the three tasks presented in either order (30 participants in each of the 6 task-pair/ordering combinations).
3.2 Participants
DOSPERT+M was administered online by Research and Development, a Japanese survey research company. The sample was probability-weighted to be representative of the greater Tokyo metropolitan area and stratified by gender. Each participant was also asked a series of demographic questions related to age, gender, location (Tokyo, Saitama, Chiba, or Kanagawa), marital status, household income, whether participant had children, and occupation. On Japan’s prefecture list by population rank, these places are 1st, 2nd, 5th, and 6th, respectively, and the stratified sample from these areas is reasonably representative of Japan’s manufacturing and service industry region (Japan Ministry of Land, Infrastructure, Transport and Tourism, 2011). Data collection took place between August 23, 2012 and August 29, 2012.
3.3 Data Analysis
We examined the relationship among risk-taking, risk perception, and expected benefits in each domain by computing correlations among domain subscale scores in each task. Because participants were randomized to complete two of three tasks, each intra-domain (inter-task) correlation is based on a different group of participants.
Following Weber et al. (Reference Weber, Blais and Betz2002), we computed conventional risk attitudes for each domain on the 120 subjects who completed the risk-taking task based on whether the domain scale score was less than 1 SD below the mean (risk averse), from 1 SD below to 1 SD above the mean (risk neutral) or more than 1 SD above the mean (risk seeking). These attitudes are “conventional” in that they assume that every DOSPERT item is a risky activity and base risk attitude on stated willingness to participate in the activity. We compute perceived risk attitudes by considering willingness to engage in activities that respondents themselves perceive to be risky. Because of our design, we were not able to compute perceived risk attitudes controlling for expected benefit by regressing risk taking on both risk perception and expected benefit as in Weber et al. Reference Weber, Blais and Betz2002), so we computed perceived risk attitudes for each domain on the 60 subjects who completed both risk-taking and risk perception tasks based on whether the coefficient for the risk perception scale score was significantly positive (risk-seeking), significantly negative (risk averse), or nonsignificant (risk neutral) when risk taking was regressed on risk perception (only) in each domain.
We conducted confirmatory factor analyses for each task excluding the medical domain items to determine whether we could recover the 6-factor solution found in Weber et al. (Reference Weber, Blais and Betz2002), in which each domain except the financial is a factor constituted of that domain’s items, and the financial domain items are split between two factors, one composed of the three gambling items, and the other composed of the three investment items. We then conducted a similar analysis including the medical domain items and hypothesizing a 7th factor composed of those items. We considered the fit acceptable if RMSEA was less than 0.06. If the fit was not acceptable, we investigated the factor structure through exploratory factor analyses with and without medical items, extracting six factors by maximum likelihood methods and using an oblimin rotation, and examined the factor pattern matrix and inter- factor correlations. (Fabrigar, Wegener, MacCallum, & Strahan, Reference Fabrigar, Wegener, MacCallum and Strahan1999). Our planned sample size of 120 per task was deemed to be sufficient for factor analysis based on the rule of thumb of 3–5 participants per item.
We also conducted multiple linear regressions to determine whether variance in domain task scores (risk-taking, risk perception, and expected benefits) was associated with demographic factors. Age, gender, cohabitation (married/living with partner or not), and occupational status (employed full or part time outside the home vs. not) were included as predictors.
Analyses were conducted using R 3.0 and the packages reshape, GPArotation, psych, nFactors, Hmisc, gmodels, sem, and semPlot (Bernaards & I.Jennrich, Reference Bernaards and Jennrich2005; Epskemp, Reference Epskamp2013; Fox, Nie, & Byrnes, Reference Fox, Nie and Byrnes2013; Harrell, Reference Harrell2013; R Core Team, 2013; Raiche, Reference Raiche2010; Revelle, Reference Revelle2013; Warnes, Reference Warnes2013; Wickham & Hadley, 2007).
4 Results
4.1 Participants
Table 3 presents the demographic characteristics of the 180 study participants.
Table 3: Demographic characteristics.

4.2 Relationships among Tasks
Within the medical subscale, risk-taking scores were not significantly correlated with risk perception scores (r=.08) in the subsample that completed those two tasks. Risk taking was significantly positively correlated with benefit perception scores (r=.42, p=.0008) in the subsample that completed those two tasks. Benefit and risk perception scores were negatively correlated (r=−.44, p=.0005) in the subsample that completed those two tasks, a pattern labeled the “halo effect” by other researchers (Finucan, Alhakami, Slovic, & Johnson, Reference Finucane, Alhakami, Slovic and Johnson2000). A similar pattern of associations was found for the social subscale; for recreation, financial, abbreviated ethical, and abbreviated health/safety subscales, risk-taking and risk perception were also significantly negatively correlated (r=−.38, r=−.38, r=−.32 and r=−.46, respectively).
4.3 Relationships among Domains
Table 4 presents the correlations among domain subscale scores in each task, which exhibit a positive manifold. Medical domain scores were least strongly correlated with the financial domain scores, but were correlated with health/safety domain scores.
Table 4: Correlations among domains and Cronbach’s α for each domain.

* p < .05
** p < .01
Note: Cronbach’s α on main diagonals, correlations on off-diagonals.
4.4 Risk attitudes
Table 5 presents conventional and perceived risk attitudes by domain. For perceived risk attitudes, missing subjects are those where regression failed due to lack of variance in predictor and outcome variable. Similar to the findings of Weber et al. (Reference Weber, Blais and Betz2002), conventional risk attitudes across participants reflected primarily risk neutrality in all domains (although with a dearth of risk averse individuals in the financial and recreational domain). Perceived-risk attitudes were largely neutral or perceived-risk averse.
Table 5: Conventional and perceived risk attitudes by domain.
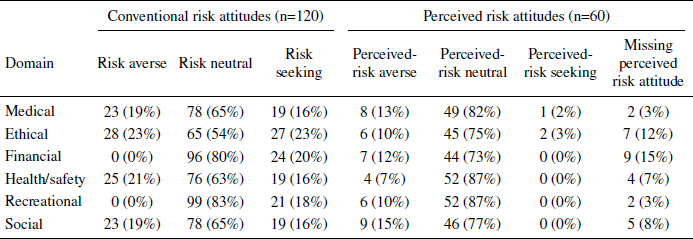
Among the 52 individuals for whom both conventional and perceived risk attitudes could be obtained for every domain, 23 (44%) had the same perceived risk attitude (perceived risk neutrality) in all domains; only 7 (14%) had the same conventional risk attitude (risk neutrality) in all domains (McNemar test chi-squared(1 df) = 10.2, p=0.001).
4.5 Confirmatory Factor Analysis
Confirmatory factor analyses of the risk-taking and expected benefits tasks with (7 factor) and without (6 factor) the medical domain items provided acceptable fit (RMSEA = .055 for risk-taking, RMSEA = .035 for expected benefits). In each case path coefficients between items and the expected factors were significantly positive, except that the path coefficients for items R2 (“Going down a ski run that is beyond your ability”) and H2 (“Engaging in unprotected sex”) were not significant in the expected benefits model.
In the risk perception task, the confirmatory analysis did not fit as well (RMSEA = .072 for 6 factors without medical items, RMSEA = .074 for 7 factors with medical items), although all of the path coefficients were significant and positive except for item M2 (“Giving blood”). Accordingly, we proceeded to examine responses in this task with exploratory factor analysis.
4.6 Exploratory Factor Analysis
Table 7 presents the pattern matrix from exploratory factor analysis of the responses in the risk perception task including the medical domain items with loadings with absolute value smaller than 0.3 suppressed. Parallel analysis suggested a 5-factor solution was most appropriate for the data, but the fit was more interpretable with a 6-factor solution, which we report here.
The social items, financial (gambling) items, and financial (investment) items loaded onto separate factors. However, the (abbreviated) ethics subscale shared common variance with the health/safety scale in this task that was unexpected (this was also observed in exploratory analyses omitting the medical items). Several recreational domain items loaded together with the medical domain items. Item M6 (general anesthesia) did not load strongly on any factor.
Table 6: Exploratory factor analysis of responses to the DOSPERT+M risk perception task (6-factor solution).
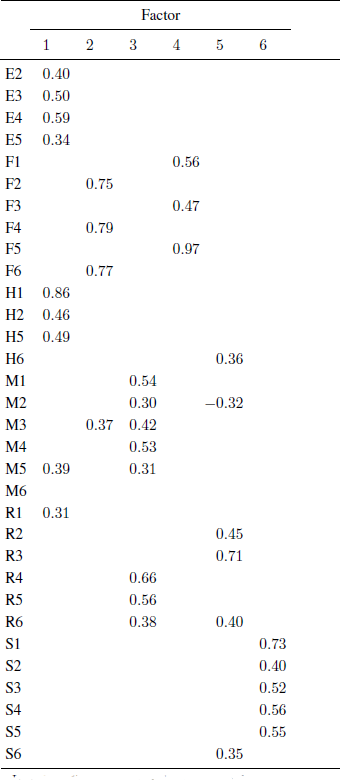
Note: Loadings with absolute value ≥0.3 shown.
4.7 Demographic Predictors of Medical Domain Scores
The regression model for medical risk-taking scores did not account for significant variance in the scores (F(4,115)=1.22, p=0.31). For risk perception of medical activities, the model reached significance (F(4,115)=3.34, p=0.01) and two predictors were associated with risk perceptions. Married respondents had lower scores for risk perception (B=−0.34, SE=.15, p=.022) and older respondents had higher scores (B=0.014 per year of age, SE=0.005, p=.005). For expected benefit of medical activities, the regression model reached significance (F(4,115)=3.7, p=0.007). The only significant demographic predictor was age: older respondents had lower scores for expected benefit (B=-0.028 per year of age, SE=0.008, p=.0004).
5 Discussion
5.1 Summary of results
In this study, we report the first attempted application of DOSPERT (and DOSPERT+M) in Japan. In the process, we experienced practical difficulty due to regulations related to acceptable survey practices. Using our modified instrument and a Tokyo metropolitan area-representative panel sample, the DOSPERT+M items generally did not cluster cleanly into the expected domains, although items within the same domain usually were intercorrelated. Participants demonstrated domain-specific conventional risk attitudes, although nearly half of those assessed were perceived risk neutral in all domains. In part, this is likely a consequence of the restricted numbers of items in each domain; researchers interested in this particular question may be better served by using the original (8 items per domain) DOSPERT of Weber et al. (Reference Weber, Blais and Betz2002) rather than the revised (6 items per domain) DOSPERT of Blais and Weber (Reference Blais and Weber2006).
Unlike our recently reported findings in the U.S. population, DOSPERT+M medical domain scores were associated with (abbreviated) health/safety domain scores, although they were often more strongly associated with scores in other domains, such as recreational activities. DOSPERT+M risk-taking scores were not associated with demographic factors; DOSPERT+M risk perception scores were lower for married respondents and increased with age. Expected benefit scores decreased with age.
5.2 Limitations
A major limitation of the study is the finding that several of the original DOSPERT scales cannot be used as written in large-sample survey research in Japan. Accordingly, conclusions drawn about the ethics and health/safety domains are based on abbreviated subscales and should be considered tentative; conclusions drawn about the financial domain, where two items required modification to make them suitable, also require caution. We obtained the responses of breast and blood cancer patients to the risk perception task using the 8-item health/safety scale administered by Hirahara and Yamagishi (Reference Hirahara and Yamagishi2009, 2011) and found that in each of those studies, the full 8-item scale was highly correlated with the abbreviated scale (r=0.94 and r=0.93, respectively); however, it should be noted that the patient sample is highly unrepresentative and this was reflected in lower perceptions of the riskiness of these everyday items than in our population sample.
We did not measure actual decision behavior, and do not know whether medical domain subscale scores might be associated with actual medical decisions. This is an area for future investigation.
Out of concern for survey fatigue, we present only two of the three DOSPERT tasks to each participant. Although this is an improvement on past studies using DOSPERT that have simply omitted the expected benefits scale, it remains a limitation on our ability to conduct within-subject comparisons of responses to each task, and to measure the risk return attitude in the manner of Weber et al. (Reference Weber, Blais and Betz2002).
5.3 Implications
Although there is good evidence for domain-specificity of risk perceptions and risk attitudes overall, patterns of responses to particular DOSPERT (and DOSPERT+M) items do not universally reproduce the expected domains, and the relationships among domains may differ for different populations. These valuable instruments for studying risk require pilot-testing when introduced to new populations and new languages.









 Open access
Open access