



Introduction
The concept of “care” has garnered significant interest in social science research and policy discussions over the past two decades. Traditionally associated with women’s roles as caregivers, the discourse surrounding care is primarily framed within gender studies and gender equality policymaking. Feminist economics has contributed to this discussion by highlighting the labor aspect of care, incorporating it into economic metrics and analyses, revealing its links to both market and non-market economic activities, and identifying pertinent economic policy frameworks (Folbre Reference Folbre1995; Razavi Reference Razavi2011; Elson Reference Elson2017).Footnote 1
As part of the feminist economics project of placing care in economic analyses, several applied country studies since the 2010s have focused on assessing the economic returns to investments in professional care services (Antonopoulos and Kim Reference Antonopoulos and Kim2008; Antonopoulos et al. Reference Antonopoulos, Kim, Masterson and Zacharias2010; İlkkaracan et al. Reference İlkkaracan, Kim and Kaya2015; Ilkkaracan and Kim Reference Ilkkaracan and Kim2019; Kim et al. Reference Kim, İlkkaracan and Kaya2019; de Henau and Himmelweit Reference De Henau and Himmelweit2021; Ilkkaracan et al. Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021; Onaran et al. Reference Onaran, Oyvat and Fotopoulou2022; Onaran and Oyvat Reference Onaran and Oyvat2023). While the primary focus of feminist literature on care services has been on its implications for gender equality, these studies go beyond the question of gender, to explore additional returns to care investments in terms of macroeconomic policy objectives. Investing in care services can significantly create jobs, reduce unemployment, boost labor force participation with a higher job multiplier than most other sectors,Footnote 2 and promote gender equality (Antonopoulos and Kim Reference Antonopoulos and Kim2008; İlkkaracan et al. Reference İlkkaracan, Kim and Kaya2015; de Henau et al. Reference De Henau, Himmelweit, Lapniewska and Perrons2016; Reference De Henau, Himmelweit and Perrons2017; International Labour Organization 2018; Ilkkaracan and Kim Reference Ilkkaracan and Kim2019; Kim et al. Reference Kim, İlkkaracan and Kaya2019; UN Women and International Labour Organization 2021). It also alleviates time- and income-poverty (Ilkkaracan et al. Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021), improves equality by socio-economic status (Antonopoulos and Kim Reference Antonopoulos and Kim2008; Antonopoulos et al. Reference Antonopoulos, Kim, Masterson and Zacharias2010; İlkkaracan et al. Reference İlkkaracan, Kim and Kaya2015), and boosts labor productivity and growth (Antonopoulos et al. Reference Antonopoulos, Kim, Masterson and Zacharias2010; Onaran and Oyvat Reference Onaran and Oyvat2023).
The research framework developed from these studies has been expanded upon by global policymaking institutions such as the International Labour Organization (ILO), International Trade Union Confederation, United Nations Development Program, and UN Women to inform policy design and advocacy efforts based on data analysis. The ILO and UN Women have collaborated on a policy simulation tool titled A Guide to Public Investments in the Care Economy: Policy Support Tool for Estimating Care Deficits, Investment Costs and Economic Returns (UN Women and International Labour Organization 2021) which builds on existing methodologies to achieve three key objectives: assessing unmet needs in various care subsectors; estimating necessary public spending to address these needs; and projecting the economic returns of investing in care services, particularly in terms of employment creation, earnings generation, and gender distribution (UN Women and International Labour Organization 2021). In the context of the pandemic, the discussion underscores the current care crisis as an opportunity for fostering inclusive growth. Investing in the care economy facilitates gender-equal recovery, bolsters societal resilience, creates jobs, and enhances labor force participation.
The tool lays out a methodology for assessing the coverage gaps, public expenditure needs, and economic returns in four sectors of care services: early childhood care and education (ECCE); primary and secondary education; healthcare; and long-term care (LTC) at the national level. While a substantial part of the gender literature on care services tends to focus on ECCE and LTC, based on prevailing shortages in these sectors and the strong substitution effect of women’s unpaid work, this focus has been criticized for its Global North bias (Esquivel Reference Esquivel2011; Ilkkaracan and Kim Reference Ilkkaracan and Kim2019). Esquivel (Reference Esquivel2021) points out that from a Global South perspective, shortages in access to care also entail inadequate provisioning of education and healthcare services, with similar, even if weaker, substitution effects. Moreover, ECCE, education, healthcare, LTC, and social services targeting different vulnerable groups constitute a continuum of services that cater to the care needs of a diverse range of care-dependent groups, e.g. children, adults, the elderly, and people with disabilities. Following this, recent studies have taken a diverse set of care sectors as a reference (International Labour Organization 2018; Ilkkaracan and Kim Reference Ilkkaracan and Kim2019).
This paper follows in the footsteps of these recent studies to undertake a comprehensive assessment of the need for investing in diverse care sectors, including ECCE, primary and secondary education, healthcare, and LTC services, in the case of Turkey and the potential therein for employment creation. We employ the analytical framework and methodology offered by UN Women and International Labour Organization (2021) and show how this global methodological tool can be revised and adapted to the national context. Three earlier studies conducted a similar analysis for Turkey focusing on investing in ECCE services and analyzing different types of economic returns. İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) benchmark ECCE services against Organisation for Economic Co-operation and Development (OECD) targets, assessing spending needs, job creation and its gender distribution, and earnings generation, contrasting the findings with construction spending outcomes. Kim et al. (Reference Kim, İlkkaracan and Kaya2019) use the findings of İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) to assess gender-related economic gaps. Lastly, Ilkkaracan et al. (Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021) investigate how ECCE investments affect gender-specific time- and income-poverty.
This paper builds upon the pre-existing work on Turkey and adapts the methodology outlined in UN Women and International Labour Organization (2021) to Turkish data to undertake a comprehensive assessment of care services coverage gaps, the required magnitude of public expenditures, and employment creation outcomes not only for the ECCE sector, but also primary, lower secondary, and higher secondary education, healthcare, and LTC services. Turkey presents an appropriate context for analyzing the impact of targeted government expenditures on care infrastructure. Job creation is a pressing macroeconomic challenge with an expanded unemployment rate exceeding 20 percent and a structurally low labor force participation rate (LFPR) of around 50 percent (Turkish Statistical Institute 2022). Turkey’s female LFPR at 35 percent (2023) lags significantly behind global and OECD averages (World Bank 2024). The scarcity of social care infrastructure, particularly childcare and LTC services, contributes to the low female LFPR (İlkkaracan Reference İlkkaracan2012; Kim et al. Reference Kim, İlkkaracan and Kaya2019; Ekiz Gökmen Reference Ekiz Gökmen2022; İzdeş Terkoğlu and Memiş Reference İzdeş Terkoğlu and Memiş2022). Comparative data show that higher care employment correlates with increased female employment rates (International Labour Organization 2018). In Turkey, however, care jobs represent only 13 percent of total employment and 25 percent of women’s employment (Bayar and İlkkaracan Reference Bayar, İlkkaracan, Ahi, Kerestecioğlu, Kolluoğlu and Tekin2022), contrasting with the norm of Europe and Central Asia, where Turkey is located (20 percent and 33 percent, respectively) (International Labour Organization 2018). Enhancing care services can thus facilitate gender-balanced employment growth, addressing Turkey’s unique challenges.
Investment in the care economy holds significant importance, particularly in the context of displacement. Turkey currently hosts the largest refugee population globally (3.4 million, of which 3.1 million are Syrians) (United Nations Refugee Agency 2024). Over the past two decades, there has been a notable rise in forced migration to Turkey, primarily involving refugees fleeing war and persecution in the Middle East, Asia, and Africa. Enhancing the availability and quality of care services is crucial for sustaining education and healthcare systems, which are vital for addressing the needs of socio-economically disadvantaged groups, including refugees. Furthermore, the COVID-19 pandemic has highlighted the existing vulnerabilities within the care sectors, underscoring the urgent need for resilient infrastructure and investments in quality services.
Against this background, this paper contributes to the literature as follows: firstly, we go beyond the focus on ECCE services of previous applied work on Turkey, to assess care services coverage gaps, the required magnitude of public expenditures, employment creation outcomes, and gender distribution of new jobs separately for the following care subsectors: ECCE; primary, lower secondary, and higher secondary education; healthcare; and LTC services. Secondly, in undertaking the assessments for the ECCE sector: (i) we use updated data (2018–2019 data) in this study versus 2013–2014 data in İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) and Kim et al. (Reference Kim, İlkkaracan and Kaya2019); (ii) also following UN Women and International Labour Organization (2021), we set higher ECCE policy targets than the ones used in the earlier three studies, concerning enrolment rates, decent employment conditions of ECCE workers, and service quality indicators such as child-to-teacher ratios. Thirdly, we undertake the assessments for the subsectors of care services by also including the Syrian refugee population.
The subsequent section offers a literature review on investing in care services and positions our study within the existing research landscape. Following that is an examination of the current state of care service provision in Turkey. Next is an outline of the data and methodology employed. Then we present our findings concerning coverage gaps, costs, and the direct and indirect employment impacts of investing in care services. It also includes estimations incorporating the Syrian refugee population. The penultimate section discusses the investment costs and overall job creation potential. Finally, the last section concludes by discussing policy implications and study limitations.
Economic assessments of investing in care services
Care work has been a long-standing focus in research and policy debates on gender equality. The focus has been on the identification of gender gaps in unpaid care work as a primary source of inequalities in time use, with spillover effects on gender gaps in employment, wages, and job stratification. The feminist literature has evolved and shifted its focus from “unpaid care work” as a constraint on women’s time and labor supply, as a source of gender economic gaps, to entail new conceptual thinking around “care work,” “caring labor,” “care services,” and “the care economy” as a significant area of economic production and consumption, indispensable for social welfare (Folbre Reference Folbre2006; Razavi Reference Razavi2011; Elson Reference Elson2017).
Recent research attempts to quantify caregiving activities to demonstrate their size and economic value (Atasü-Topcuoğlu Reference Atasü-Topcuoğlu2021), emphasizing the positive outcomes of high-quality care services both for caregivers and recipients (International Labour Organization 2018). This literature has spearheaded the emergence of operational concepts such as care infrastructure, economic returns on care investments, as well as visions of a new economic and social order called the “purple economy” (Ilkkaracan Reference Ilkkaracan, Bargawi, Cozzi and Himmelweit2016; Reference Ilkkaracan, Leite and Morales2023), “caring economy” (Elson Reference Elson2017), and “care society” (United Nations Economic Commission for Latin America and the Caribbean 2022).
The pandemic led to a worldwide public health, economic, and care crisis, further unveiling the importance of a comprehensive care services infrastructure. Many countries had a large coverage gap in the care sector before the pandemic (International Labour Organization 2018). The outbreak has increased unpaid care burdens, especially for families with dependants, due to limited professional care and reduced family support, deepening pre-existing inequalities by gender, household income, labor market status, etc. International development agencies urge governments to create robust care infrastructures through proactive policies, reducing inequalities, and increasing crisis resilience (United Nations Secretary-General 2021).
Studies applying care economy concepts find investing in services like ECCE and HIV patient care (Antonopoulos and Kim Reference Antonopoulos and Kim2008) in South Africa and ECCE and LTC in the United States (US) (Antonopoulos et al. Reference Antonopoulos, Kim, Masterson and Zacharias2010) yields higher economic returns than other sectors such as construction and green energy. Care service investments create more jobs, distribute earnings more equitably by gender and status, and better reduce poverty and inequality. Investing $50 billion in US care facilities could create 1.2 million jobs, 90 percent for women, with half aiding the bottom 40 percent in income (Antonopoulos et al. Reference Antonopoulos, Kim, Masterson and Zacharias2010; Antonopoulos and Kim Reference Antonopoulos and Kim2011). In South Africa, dedicating 2 percent of gross domestic product (GDP) to public spending could add 772,000 jobs, 60 percent for women, and cut poverty by 1.8 percentage points (Antonopoulos and Kim Reference Antonopoulos and Kim2008).
İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015), based on Antonopoulos and Kim (Reference Antonopoulos and Kim2011), analyze the ECCE sector’s expansion in Turkey, contrasting it with infrastructure and construction similar to the South African study. It undertakes a survey of daycare centers and preschools for a detailed and data-based estimation of the costs of such an expansion.Footnote 3 The analysis details Turkey’s ECCE coverage gap versus OECD goals and the costs of enrolling 3.3 million additional children, equating to 1.2 percent of GDP. This spending could create 720,000 jobs in ECCE and backward-linked sectors, 73 percent for women, and reduce poverty by 1.4 percentage points, outperforming similar investments in construction.
Following these studies, multi-country applied studies showed that care investment drives job creation. De Henau et al. (Reference De Henau, Himmelweit, Lapniewska and Perrons2016) report that a 2 percent GDP investment in ECCE across seven OECD countries could increase employment by 2.4 to 6.1 percent, with women’s employment rising by 3.3 percent to 8.2 percent. Similarly, a study in six emerging economies suggests a 2 percent GDP investment in ECCE could grow employment directly and indirectly by 1.2 percent to 2.4 percent (de Henau et al. Reference De Henau, Himmelweit and Perrons2017).
The most comprehensive study by Ilkkaracan and Kim (Reference Ilkkaracan and Kim2019) covers forty-five countries, about 85 percent of the world’s population, and a broad range of care sectors in line with the definition adopted by the International Labour Organization (2018) which are ECCE, primary, secondary, and tertiary education, healthcare, and LTC. The study projects care needs and job creation to 2030 under two scenarios: current spending (“status quo”); and increased spending aligned with Sustainable Development Goals (SDGs) (“high-road”). The latter requires boosting public care spending by 3.4 percent of GDP, potentially creating 120 million jobs in the care and other related sectors, 55 percent of which could be for women.
Care investment studies highlight the ECCE sector’s role in job creation, with extensions to HIV care in South Africa and LTC in the US. Ilkkaracan and Kim (Reference Ilkkaracan and Kim2019) further include education and healthcare beyond ECCE and LTC. Esquivel (Reference Esquivel2011; Reference Esquivel2021) critiques the narrow focus on ECCE and LTC as a developed economy bias, advocating for a Global South view that incorporates education and healthcare shortages and quality. Esquivel (Reference Esquivel2011) sees “care work” as nurturing service work, addressing unpaid caregivers’ burdens, and aiding recipients’ capability development. Ilkkaracan and Kim (Reference Ilkkaracan and Kim2019) recognize social services and workers as care providers for vulnerable groups like refugees, women victims of violence, and youth with addictions. Following such a comprehensive definition of care services, Mendez Santolaria and Rodriguez Enriquez (Reference Mendez Santolaria and Rodriguez Enriquez2023a,b) conducted studies on the expansion of educational and social services in Argentina by also including children who need special education and gender violence victims who require mental health and support.
The focus on care studies reviewed so far typically employs a macro–micro modeling approach. The studies focus on particular sectors of care services, undertaking country-specific assessments of sectoral gaps and costs, estimating employment creation using input–output (IO) analysis, and, in some cases, using microsimulation to assess distributional outcomes, as in the three seminal studies discussed above. A different methodological approach is the use of macromodelling, as in Onaran et al. (Reference Onaran, Oyvat and Fotopoulou2022) for the United Kingdom, Oyvat and Onaran (Reference Oyvat and Onaran2022) for South Korea, and Onaran and Oyvat (Reference Onaran and Oyvat2023) for seven developing economies, including Turkey. These studies base their simulations on an assumed change in public spending (a cursory increase of typically 1 percent of GDP) on overall care services to evaluate the impact on employment, GDP, and productivity growth using what they call a post-Keynesian feminist macromodelling framework. Onaran and Oyvat (Reference Onaran and Oyvat2023) find that a five-year public spending increase on care services boosts GDP by 11.1 percent and employment by 6.3 percent, with a stronger impact on women’s employment in the emerging economies of Colombia, Indonesia, South Korea, South Africa, Turkey, the Philippines, and India. For Turkey, GDP is estimated to increase by 4.9 percent and employment by 3.1 percent. A one-time care economy spending boost has a 1.6 percent GDP multiplier, with women’s employment up by 1.2 percent and men’s by 0.8 percent.
As mentioned, there are two other studies on Turkey, focusing on ECCE and building upon the work of İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015): Kim et al. (Reference Kim, İlkkaracan and Kaya2019) and Ilkkaracan et al. (Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021). Using the average cost per child derived from their field survey of early childhood education centers, İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) estimate that enrolling an additional 3.27 million children to reach the OECD average ECCE enrollment rates would require 1.2 percent more of GDP. Later, Kim et al. (Reference Kim, İlkkaracan and Kaya2019) suggest that to ensure decent employment in the ECCE sector, spending should rise to 1.8 percent of GDP. They also find that higher ECCE spending could decrease the gender employment gap by 1.9 percentage points and the earnings gap by 2.5 percentage points, whereas spending on construction would trigger a further increase (by 0.8 percentage points) in the former and would only have a modest reduction (0.7 percentage points) in the latter. Moreover, ECCE spending would increase gender job segregation, but less than spending on construction, as ECCE employment consists predominantly of women and vice versa for the construction sector.
Finally, Ilkkaracan et al. (Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021) investigate the impact of ECCE investments on gender-specific time- and income-poverty. Analyzing Turkish time-use data matched with living-conditions surveys from 2015, the study goes beyond direct job creation to include induced employment from increased household spending. It suggests that over 1.043 million new jobs could be generated, with over half in the ECCE sector. While these jobs could alleviate income-poverty, they also present a significant time-poverty risk for women with young children due to increased employment. However, access to childcare services could reduce women’s unpaid care work time by over one-third, significantly mitigating time-poverty rates for newly employed mothers and reducing their combined time- and income-poverty rate by 67 percent. Thus, ECCE investments not only stimulate job creation and reduce income-poverty but also alleviate time-poverty for working mothers, fostering sustainable labor force participation.
This paper extends earlier work, to assess the case for investing in care services not only for the ECCE sector, but also for its other subsectors for which data are available, namely primary, lower secondary, and upper secondary education, healthcare and LTC for the elderly population. We adapt the methodology proposed in UN Women and International Labour Organization (2021) to the case of Turkey to estimate the gaps, costs, and employment creation potential of public spending on the care services sector, disaggregated by four subsectors. In the case of estimations for the ECCE sector, we update the data to 2018–2019 and set higher policy targets at 50 percent for ages 0–2 years and universal coverage for ages 3–5 years. Our estimations are grounded by also including a separate estimation of care service needs considering the Syrian refugee population, which has created a demand shock through a substantial migration inflow in the 2010s.
Current status of care services in Turkey
Early childhood care and preschool education
Contributing to the significant supply gap in care services, ECCE is an underdeveloped sector in Turkey. For 2019, the ECCE enrollment rate in the 0–3 years age group was 0.2 percent, and in the 3–5 years age group was 42 percent (Ministry of National Education 2019a) compared to the OECD averages of 28 and 88 percent, respectively (Organisation for Economic Co-operation and Development 2020a). The enrollment rate in the 5-year-old group, even at the highest level, was only 71 percent, which was below the national target of 100 percent for 2023 (Republic of Turkey Presidency of Strategy and Budget 2019).
The low coverage rate in preschool education is because ECCE services are mostly available to 5-year-olds, especially for those provided by the public, and the law does not mandate public service provision for children under 3 years old (World Bank 2015). Participation in preschool education increases as the child gets older: the enrollment rates for ages 3, 4, and 5 years were 10.7 percent, 39.5 percent, and 69 percent, respectively. Public nursery facilities are very limited, and private kindergartens are not accessible to every family under market conditions. The mother provides daycare for small children at a rate of 88.4 percent, and the grandmother at a rate of 6.3 percent. The care provided by kindergartens and nurseries is only 2.7 percent (Ministry of Family, Labor and Social Services 2019).
Primary, lower secondary, and upper secondary education
Turkey extended compulsory education from 8 to 12 years in 2012 to align with OECD and European Union (EU) standards. Enrollment rates were 94 percent in primary school (grades 1–4) and 96 percent in lower secondary school (grades 5–8) in 2019. However, enrollment rates remained lower in upper secondary (high school) education (85 percent). Turkey lags behind the OECD in terms of average years of education and enrollment rates. The average education period for 90 percent of Turkey’s population was 10 years in 2018, compared to 14 years in the OECD and EU. Regarding total expenditures for primary, lower secondary, and upper secondary education, Turkey’s ratio to GDP was 3.3 percent in 2017, slightly below the OECD average of 3.5 percent.
Healthcare services
Despite advancements in healthcare services capacity, mortality rates, and healthcare expenditures, Turkey still falls behind OECD countries. Even with the increase in healthcare professionals and institutions, Turkey ranks lowest among OECD nations for physicians, nurses, and midwives per 100,000 people (Ministry of Health 2019a) and also remains in the lower range for bed capacity (Organisation for Economic Co-operation and Development 2020b). Additionally, Turkey’s GDP share of health expenditures is much lower than the OECD average, resulting in significantly lower per capita health expenditures (Organisation for Economic Co-operation and Development 2020b).
The COVID-19 pandemic exposed a shortage of care services, particularly in healthcare. With Turkey’s aging population, the demand for healthcare services is also expected to increase.
Long-term care services
LTC encompasses a range of services provided to the elderly and people with chronic disabilities and illnesses. The population aged 65+ years increased from 9 percent in 2019 to 10.2 percent in 2023, classifying Turkey as a “very elderly population country.” While most of elderly care is provided by family members (96 percent in 2016), the availability of such care within households has been declining (Ministry of Family and Social Services 2020). Financial support and cash aid to the elderly, introduced in 2015, have helped sustain caregiving by family members. However, these responsibilities often lead women to withdraw from work and social activities. Despite high demand, the availability of nursing homes remains limited, and Turkey lags behind OECD30 in terms of LTC bed capacities (Organisation for Economic Co-operation and Development 2020b).
Methodology and data
This paper applied the policy simulation tool developed by UN Women and International Labour Organization (2021) to calculate coverage gaps, costs of required investments, and job creation in Turkey’s education and health sectors using data from the Ministries of National Education and Health (2018–2019), TurkStat's Household Labor Force Survey (2012; 2019), and TurkStat's IO data (2012). The first country application of the UN Women and International Labour Organization (2021) policy tool is carried out for Turkey in this paper.Footnote 4 Investments in care services can play a crucial role in driving socio-economic development and supporting disadvantaged segments of the population. Therefore, this paper’s application of the simulation tool in the case of Turkey mainly aims to exemplify the substantial job creation potential of care services in a rapidly developing country context by also measuring the care gaps and required costs of investments.
The methodology comprises four steps applied to each of the four care services sectors, namely ECCE, primary and secondary education, healthcare, and LTC:
-
i. Estimate the care coverage gaps in the sector (in terms of the additional population to be covered by services and/or the additional number of care workers in line with the policy targets in our simulation scenario);
-
ii. Estimate the costs of eliminating the care coverage gaps (based on the per care receiver and/or per caregiver annual cost);
-
iii. Estimate the magnitude of direct employment creation in the care services sectors disaggregated by direct care workers and support workers (administrative and other service personnel);
-
iv. Estimate the magnitude of indirect employment creation through IO analysis.
To estimate the care coverage gaps in the education sector (ECCE, primary, lower secondary, and upper secondary levels), we used the targets that the International Labour Organization (2018) set and adjusted as needed based on national legislation.
Calculations for healthcare included LTC for the elderly and short-term care (STC) for the sick and elderly. LTC can be offered in a variety of organizational settings, including institutional care (residential care facilities or daycare centers), home care (formal professional services delivered in a home setting), informal paid care (services delivered by home workers), and free care (services delivered by family and friends) (Ilkkaracan and Kim Reference Ilkkaracan and Kim2019). The paper mainly focuses on institutional care in LTC services. We could include elderly care but not disability care services in our LTC calculations, as the manual by UN Women and International Labour Organization (2021) does not suggest any methodology for disability care services. This might be related to the fact that disability care services are offered in a broad variety of organizational structures, which makes it difficult to cover the various forms of employment of disability care workers.Footnote 5 Based on 2019 statistics, estimates for STC and LTC services have been made.
We also estimate the direct and indirect job creation disaggregated by gender resulting from investments in the care sectors. To estimate direct employment creation within the care services sectors, we apply the methodology in UN Women and International Labour Organization (2021) based on data for population size disaggregated by care receiver category (small children, students, ill, elderly), target coverage rates, and care receiver-to-care worker ratios, as well as care worker-to-support worker ratios (i.e. administrative and support workers employed in care services).
Indirect employment, i.e. employment to be created through backward linkages of care services sectors, is estimated by utilizing the 2012 IO table for Turkey.Footnote 6 IO tables are matrices that illustrate the flow of goods and services between different sectors of an economy. They show how the changes in the output of one industry impact the output in other sectors that feed inputs into the target industry (called backward linkages), capturing the cross-sector interdependencies within an economy. These tables are used to understand the structure of an economy and assess the overall impact of economic policies or shocks. In other words, IO models are simple mathematical models that allow multi-sectoral analysis by showing the mutual relationship between production and the final and intermediate consumption units that make up the economic structure of a macroeconomy.
The use of IO analysis can be justified for several reasons. One of the main objectives is to estimate the employment creation impact of increased public spending on care services. As the discussion of findings in the Empirical results section shows, a significant share of new employment comprises direct jobs in the care sector (estimated through a different method as explained above). Indirect employment estimates aim to make the point that employment creation via increased spending on care is not restricted to direct employment only, but also indirect employment in other sectors from which care services purchase inputs via backward linkages. The care services sectors are labor intensive but show relatively low input usage from other sectors. Consequently, our analysis estimates that only 8.7 percent of total employment creation consists of indirect employment (see Table 1). To keep the indirect employment estimates to a minimum, we refrain from reporting on induced employment (jobs created in other sectors via increased household spending by job recipient households).
Table 1. New employment created by investments in care services
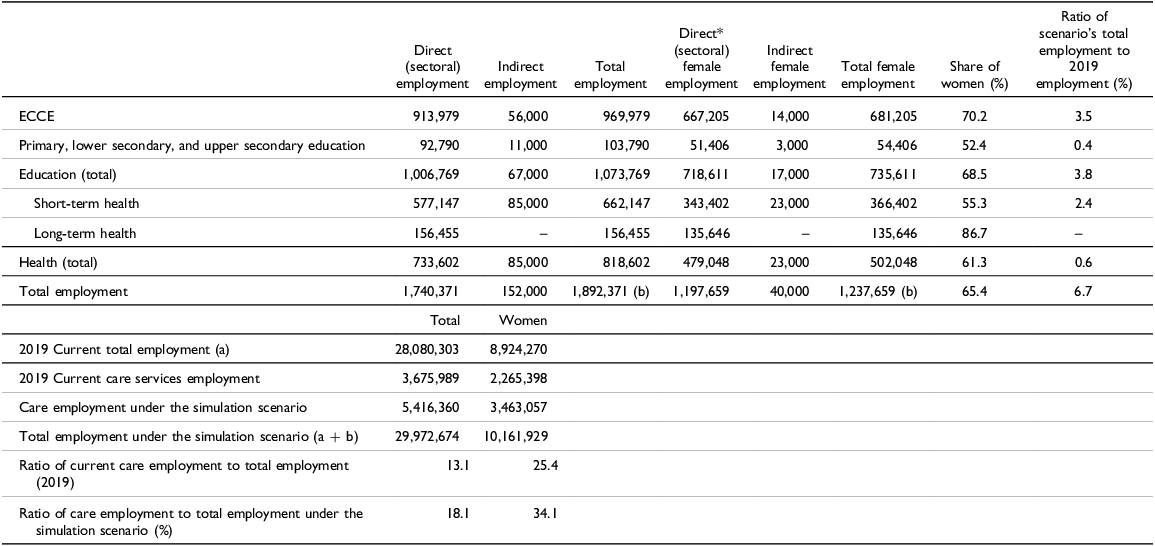
ECCE, early childhood care and education.
* ECCE data are sourced from İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015), indicating that 73 percent of ECCE employment was held by women in 2015. For sectors beyond ECCE, we report the following female shares of employment in care services sectors: 55.4 percent in education, 59.5 percent in short-term healthcare, and 86.7 percent in long-term care, drawing from the Household Labor Force Survey (2019).
Source: Authors’ own calculations based on Ministry of National Education (2019a), Ministry of Health (2019a), Turkish Statistical Institute (2019a), and Organisation for Economic Co-operation and Development (2023) data.
Given the production structure of care services (labor intensive but weak use of other inputs), the assumption of no capacity constraints also seems justified. Given the high unemployment and low LFPR, the workforce is far from being constrained. Instead, there is an oversupply in the job market and unused potential, especially among women, that could be harnessed. Furthermore, the weak use of other inputs also means that supply from other sectors to the care sector is unlikely to encounter capacity constraints.
Using the 2012 IO tables and the sectoral employment data from the Household Labor Force Survey (2012), we estimate the number of jobs expected to be created in other related sectors (such as manufacturing or transport) from which the care services sectors (education and health) purchase inputs. The number of necessary expenditures for education (including ECCE) and health (including LTC) identified under steps i and ii above are injected into these care services sectors to estimate the change in output and hence the change in employment triggered in the other sectors. Pulling together the estimate of direct employment creation under step iii (care services jobs) and indirect employment estimated under step iv via IO analysis (jobs in other sectors), we are able to report the total number of jobs to be created resulting from increased expenditures for expansion of care services.
Initially, we conducted coverage gap, cost, and direct employment calculations excluding the Syrian refugee population and then repeated them including this group for all subsectors of care services. The only exception is that due to data constraints, in ECCE services, we could only calculate for Syrian children aged 5 years. The results for the coverage gap, cost in care sectors, and the direct employment impact of care service investments, both with and without the Syrian population, are presented in separate tables.
Empirical results: coverage gap, required expenditures and employment creation impact of investments in care services in TurkeyFootnote 7
Education services
To begin with, to meet ILO standards, approximately 4.3 million more enrollments are needed in Turkey’s preschool system out of the 7.8 million children in the relevant age group (Equation 1) (International Labour Organization 2018). This comprises 1.9 million children under the age of 3 years and 2.4 million children aged 3–5 years. Meeting the legally mandated minimum ratios would necessitate 349,591 teachers and 349,591 aides (totaling 699,182 instructors). The overall expenditures, including salary and non-salary expenses, reach 82.8 billion TL, equivalent to 1.92 percent of GDP (Equations 2, 3, and 4).Footnote 8
As a comparison, İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) and Kim et al. (Reference Kim, İlkkaracan and Kaya2019) estimated the number of additional children at 3.2 million and the required number of teachers and aides at 243,845 each (totaling 487,690 instructors). The difference has to do primarily with higher enrolment targets in our calculations than the target enrolment rates employed in İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015). Following the policy targets proposed in UN Women and International Labour Organization (2021), we set the desired enrolment at 50 percent for the age group 0–2 years and 100 percent for the age group 3–5 years (see Appendix 2). The ECCE policy scenario in İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) used OECD average enrolment rates by age group, ranging from 33 percent for the age group 0–2 years, 70 percent for age 3 years, 84 percent for age 4 years, and 94 percent for age 5 years. Moreover, the child population figures in our analysis from 2019 are higher than the figures in İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015). İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) assess ECCE costing at 1.2 percent of GDP, setting similar targets as in our analysis for child-to-service provider ratios but without revising the costing for decent work criteria. Kim et al. (Reference Kim, İlkkaracan and Kaya2019) estimate the cost at 1.78 percent of GDP based on similar child and caregiver numbers but improving wage and salary costs for decent work conditions. We use similar decent work conditions as in Kim et al. (Reference Kim, İlkkaracan and Kaya2019), but given the higher number of children, we estimate ECCE coverage costs at 1.92 percent (Table 2).Footnote 9
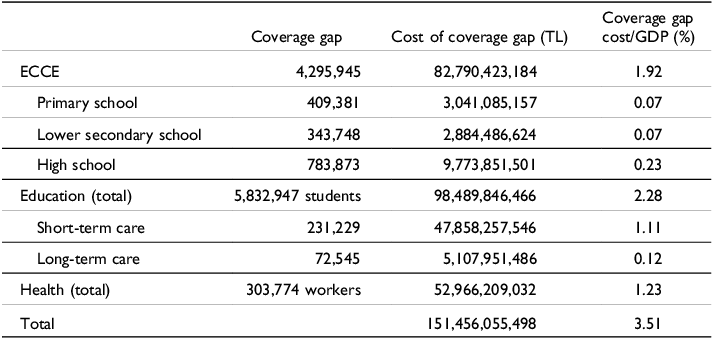
Table 2. Coverage gap and cost in care sectors
Secondly, the preschool calculations were repeated for primary, lower secondary, and high school education to achieve the ILO’s 2018 goal of 100 percent coverage. In the primary education system, the entire population of children aged 6 to 9 years (5,066,591) should be included. There is a need for 409,381 additional enrolments to cover the gap (Equation 1). Therefore, an investment of 3 billion TL (including salary and non-salary spending) is necessary to enroll 409,381 pupils in primary school, equivalent to 0.07 percent of GDP (Equations 2, 3, and 4). In lower secondary school education, the entire population of children aged 10 to 13 years (5,115,296 students) should be included (Equation 1). This indicates a coverage gap of 343,748 students. Enrolling these additional students would necessitate a total investment of 2.9 billion TL, equivalent to 0.07 percent of GDP (Equations 2, 3, and 4). In high school education, 4,961,220 students need to be enrolled within the age range of 14 to 17 years, implying a coverage gap of 783,873 students (Equation 1). Consequently, a total investment of 9.8 billion TL (for salary and non-salary expenditures) is necessary to meet the ILO target for high school education (twenty-eight students per teacher), representing 0.23 percent of GDP (Equations 2, 3, and 4) (Table 2).
Thirdly, we calculated the total direct employment effect. In ECCE, preschools need to hire a total of 913,979 employees, including 214,797 non-teaching personnel (Table 3). The primary, lower secondary, and high school education services will generate 92,790 additional direct jobs. Overall, investment in education services for a total of 5,832,947 children will generate 752,660 teaching positions and 254,109 non-teaching jobs, resulting in a total of 1,006,769 new jobs.
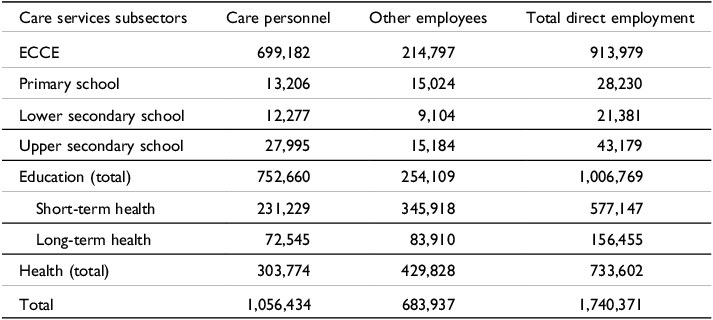
Table 3. Direct employment impact of social care investments (number of new jobs)
We have repeated the estimations by also including the Syrian children. In 2019, Syrian refugees comprised 3.5 percent of all students (2.0 percent of preschoolers, 6.9 percent of elementary school students, 3.1 percent of secondary school students, and 1.3 percent of high school students) (Ministry of National Education and UNICEF 2019). Due to the absence of disaggregated population data for Syrians under the age of 5 years, calculations for ECCE services were conducted solely for Syrian children aged 5 years. It revealed that including 95,094 Syrian 5-year-olds in 2019 (Ministry of National Education 2019b) increased the total number of children needing coverage by 2 percent to 4,391,039. This adjustment raised the cost from 83 billion TL (1.92 percent of GDP) to 84 billion TL (1.95 percent of GDP).
Considering the Syrian population of primary school age, the number of students to be covered is 792,000, and the cost of the coverage gap reaches 5.9 billion TL (from 0.07 percent to 0.14 percent of GDP). For lower secondary schools, the coverage gap is 644,000 students, and the cost of the gap reaches 4.5 billion TL (0.07 percent to 0.10 percent of GDP). In upper secondary education, the coverage gap increases to 1 million students, and the cost increases to 13 billion TL (from 0.23 to 0.30 percent of GDP).
Short-term healthcare services
Although Turkey met the ILO’s minimum threshold of 4.45 doctors, midwives, and nurses (DMN) per 1,000 people in 2019 (International Labour Organization 2018; Ilkkaracan Reference Ilkkaracan2020), the COVID-19 pandemic significantly increased the demand for healthcare services. Therefore, the coverage gap in STC was determined by using the OECD averages.
Health workers were divided into two groups (International Labour Organization 2018; UN Women and International Labour Organization 2021): DMN; and health workers in the other cadres (HWOC). There was a total of 1,033,767 health professionals (including 160,810 doctors, 198,103 nurses, and 249,222 HWOC), serving a population of 83,154,997 in 2019 (Ministry of Health 2019a; Turkish Statistical Institute 2019b).
A total of 148,395 nurses and midwives and 82,834 doctors are needed to meet the threshold values set by the Organisation for Economic Co-operation and Development (2020b) and the Ministry of Health’s 2019–2023 Strategic Plan (Equation 5) (Ministry of Health 2019b). These result in a total deficit of 231,229 in the DMN category. To close the HWOC gap, an additional 138,737 workers are required (Equations 6 and 7). The overall staff deficit in STC, including DMN and HWOC, amounts to 369,966 (Equation 8). Additionally, there is a projected shortage of 207,181 administrative and support staff (AS) (Equations 9 and 10). To address the coverage gap of 231,229 healthcare professionals, the total expenditure required, including salaries and non-salary expenses, is 47.9 billion TL, equivalent to 1.11 percent of GDP (Equations 11, 12, and 13).
Considering the limited data availability, the direct employment impact in the STC sector was primarily analyzed for health professionals. This assessment indicates that STC is expected to generate a total of 577,147 new jobs.
In STC services calculations, when we incorporated 3,576,370 Syrian refugees as beneficiaries, the coverage gap in STC services amounts to 259,018 employees, with a corresponding cost of 54 billion TL (increasing from 1.11 percent to 1.24 percent of GDP).
Long-term healthcare services
The coverage gap in LTC services is calculated only for the elderly, excluding disabled care, due to data constraints. Therefore, the LTC coverage gap and cost calculations represent a minimum estimate.
The coverage gap for LTC services can be determined using either the number of LTC employees or the number of individuals aged 65+ years receiving services (UN Women and International Labour Organization 2021). We chose to consider international targets for both factors to determine the service gap. This approach is preferred because relying solely on the number of employees does not provide a definitive ratio for the 65+ years age group that is targeted for LTC services. With this method, both the expected elderly population benefiting from LTC services and the direct employment impact of the required investments are determined.
In 2019, Turkey had a population of 7,550,727 individuals aged 65+ years. According to ILO’s target rate (12.4 percent for the population aged 65+ years) (International Labour Organization 2018), there is a coverage gap of 909,004 individuals in terms of service recipients (Equation 14).
We calculated the coverage gap also in terms of the LTC worker number. As the threshold, we chose the legal requirement in Turkey for nursing homes (8.67 nurses and caregivers per 100 elderly residents), which aligns with the global standard. This is also higher than the International Labour Organization (2018) target of 4.2 employees. Considering that 8,631 formal LTC workers were employed, to achieve the universal coverage rate of 12.4 percent (i.e. for 936,290 elderly to be covered in total, including the available 27,286 nursing home residents), an additional 72,545 full-time LTC personnel are needed (Equation 15). The employment of the additional full-time LTC employees would require a total compensation of 5.1 billion TL, representing 0.12 percent of GDP (Equation 16).
Turkey had an average nursing home capacity of sixty-five, accommodating 27,286 elderly individuals across 420 public and private facilities as of 2019. To achieve the 12.4 percent universal coverage rate, a projected total of 13,985 nursing homes is anticipated for 909,004 elderly individuals. However, this study proposes a future approach that does not solely rely on residential (nursing home) services, aligning with the International Labour Organization (2018). Given the scarcity of residential services, it is crucial to expand the range of available options for care and increase the number of services offered to individuals aged 65+ years to close the coverage gap. Considering that the new LTC services will predominantly involve daycare and home professional services, the number of AS has been halved. Accordingly, the spending on LTC services will result in 156,455 new direct jobs in the LTC industry (72,545 nurses and caregivers and 83,910 other AS).
Lastly, upon incorporating 65,346 Syrians over the age of 65 years into LTC service calculations, the coverage gap expanded to 73,000, with the cost rising to 5.2 billion TL. The ratio of the coverage gap to GDP remained unchanged.
Discussion: cost of investments in care services and job creation potential
There is a growing demand for paid care work because of shifts in family structures, unfavorable care dependency ratios, evolving care needs, and the rising participation of women in the workforce in specific countries (International Labour Organization 2018). Turkey must proactively promote the availability of paid care jobs, given its ageing population, the disproportionate unpaid domestic care burden on women, and the challenges posed by the refugee influx. Otherwise, she will face a deepening care crisis and gender inequalities. Moreover, the growth in paid care jobs should be synchronized with labor market policies that advocate for formal employment, job security, and equitable wages. This is crucial due to the dual nature of the labor market, which imposes greater precariousness on specific segments of the workforce, including informal and immigrant workers. The International Labour Organization (2018, 14–15) warns that the rise in female employment in certain countries has not been matched by an overall improvement in job quality, as “it is often characterized by low pay, temporary contracts, poor working conditions, and low-status jobs.” Turkey also needs to develop the care services sector, as its infrastructure has been under additional pressure since the last decade due to refugee flux.
Table 2 presents the coverage gaps in the education and health sectors and the cost of those gaps. The education services have a deficit of 5,832,946 students, with ECCE accounting for 84 percent of this gap. The cost of closing the education coverage gap amounts to 98.5 billion TL (2.28 percent of GDP). There is a shortage of 303,774 personnel in the health sector, and addressing this gap would require an investment of 53 billion TL (1.23 percent of GDP). STC bears responsibility for 90 percent of the healthcare coverage gap. The total investment required to meet the ILO’s 2018 goals for healthcare and education is 151 billion TL (3.51 percent of GDP).
Table 3 presents the direct employment effects of investments in care services. Combining the number of teachers, assistant teachers, and non-educational personnel (349,591 + 349,591 + 214,797), the number of new direct jobs in ECCE amounts to 913,979. Additionally, it is projected that there will be 92,802 new positions in primary, lower secondary, and high school education, comprising 53,478 teachers and 39,312 non-educational staff. Consequently, a total of 1,006,769 new jobs will be created in the education sector (Table 3).
The direct employment impact of the STC services was assessed, resulting in a projected addition of 577,147 new jobs. This includes 231,229 physicians, midwives, and nurses, 138,737 other healthcare professionals, and 207,181 AS. Additionally, the LTC sector is expected to create 156,455 new jobs, with 72,545 nurses and elderly caregivers and 83,910 other LTC employees. Overall, health services will employ 733,602 individuals. Consequently, a total of 1,740,371 additional jobs will be generated directly in the care sector (Table 3).
Using IO analysis, this study examines indirect job creation in industries related to care services. In the IO table, the education sector includes ECCE, elementary, and secondary education, while health services are part of the health sector. LTC services are categorized under the other services sector. This study predicts that LTC services will be primarily professional services offered at home, and the cost structure will primarily consist of care workers’ wages, as discussed in the cost estimate for the LTC gap. Estimates of indirect employment were not undertaken for LTC since a sector dominated by home services has limited interaction with other sectors. This aligns with the approach of the International Labour Organization (2018) to LTC services.
Table 1 illustrates the direct and indirect job creation potential in subsectors of the care economy. ECCE demonstrates the highest capacity with 970,000 new jobs, comprising 914,000 direct and 56,000 indirect jobs. STC follows with 662,000 new jobs, including 577,000 direct and 85,000 indirect jobs. Primary, lower secondary, and high school education contributes 104,000 new jobs, consisting of 93,000 direct and 11,000 indirect jobs. LTC generates 156,000 direct jobs.
The expected gender distribution of the new jobs can be estimated based on the current observed gender balance by sector and assuming that the gender composition of sectoral employment remains constant. Accordingly, 70.2 percent of the new jobs created through increased expenditures on ECCE services are expected to employ women (corresponding to 681,000 women employees) versus 52.4 percent of the jobs created through increased expenditures on education for eliminating the coverage gaps in primary and secondary schooling (54,000 women employees). LTC services exhibit the highest female share at 86.7 percent, i.e. 136,000 jobs created for women. Healthcare services (short term) are relatively more gender-balanced but still favor women’s employment, with a 55.3 percent female share in new job creation (366,000 jobs for women). Total employment creation for women stands at 1.2 million jobs, or 65.4 percent of the total.
These findings indicate that investments in the care sector carry the potential for substantial employment creation as also argued by de Henau (Reference De Henau, Himmelweit, Lapniewska and Perrons2016; Reference De Henau, Himmelweit and Perrons2017). Additional care services expenditures can significantly boost employment, with a total of 1.89 million new jobs across all sectors. This represents a 6.7 percent increase from the 2019 employment level of 28.1 million. Of these new jobs, 1.74 million are direct positions in the care sector, while 152,000 (8 percent) are indirect jobs in other industries through backward linkages in the care services sectors.Footnote 10 Considering the current gender distribution, women are expected to occupy nearly two-thirds (65.4 percent) of the newly created positions, leading to a 14 percent improvement in female employment. This finding aligns with the literature that stresses that investments in care services will predominantly employ women (Antonopoulos et al. Reference Antonopoulos, Kim, Masterson and Zacharias2010; Antonopoulos and Kim Reference Antonopoulos and Kim2011; İlkkaracan et al. Reference İlkkaracan, Kim and Kaya2015; Ilkkaracan and Kim Reference Ilkkaracan and Kim2019). Hence, care service expansion is shown to contribute to women’s inclusion not only by relieving constraints on their time, helping to improve their labor supply, but also on the demand side by creating ample demand for women workers. Furthermore, expanding care employment will support human capital development through children’s education (International Labour Organization 2018) and increase life quality and well-being for recipients and providers, especially unpaid careers.
This paper builds upon earlier studies (İlkkaracan et al. Reference İlkkaracan, Kim and Kaya2015; Kim et al. Reference Kim, İlkkaracan and Kaya2019; Ilkkaracan et al. Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021) and expands the analysis to include primary, lower secondary, and higher secondary education, healthcare, and LTC services for a comprehensive assessment with updated data and higher coverage targets. Onaran and Oyvat (Reference Onaran and Oyvat2023) estimated at a macro level the GDP- and employment-multiplying effects of public spending in the care economy for eight emerging economies, including Turkey based on time-series data and without any differentiation by subsector of care services. Our study contributes to the literature by providing sector-specific estimation of the gaps and highlighting both direct and indirect gender-disaggregated employment effects of investments separately in each subsector by applying the policy simulation tool developed by UN Women and International Labour Organization (2021). The unequal domestic care burden adversely affects female labor force participation in both developed and developing countries; however, it poses a more significant obstacle in the latter, where the patriarchal mindset is dominant and child and elderly care services are inadequate (Ekiz Gökmen Reference Ekiz Gökmen2022). Therefore, this paper’s focus on a developing country case, Turkey, is particularly deserving.
Bayar and İlkkaracan (Reference Bayar, İlkkaracan, Ahi, Kerestecioğlu, Kolluoğlu and Tekin2022) using the Turkish Statistical Institute Household Labor Force Survey microdata for 2019 estimate care employment to stand at 3.7 million workers, corresponding to 13.1 percent of total employment. Of this, 2.3 million are women workers, corresponding to 25.4 percent of total female employment. The bottom half of Table 1 assesses our simulation scenario against this background. We find that under an expansion of care services in Turkey in line with the SDG targets, total care services employment will rise to 18.1 percent of total employment, increasing total care sector employment to 5.4 million workers (i.e. when 1.7 million additional care jobs are added to the existing 3.7 million care sector employees). The number of women employed in the care sector will increase from 2.3 million (25.4 percent of total female employment) to 3.5 million (34.1 percent of total female employment). As such, Turkey will move from being an outlier in Central Asia and Europe in care employment to average rates. Care services sector employment comprises 19.5 percent of total employment in the region and 33.1 percent of women’s employment (International Labour Organization 2018).
As highlighted by the International Labour Organization (2018), collaboration between care policies, along with macroeconomic, social protection, labor, and migration policies, fosters an environment conducive to quality care work. Increased public investment in care services necessitates a higher share of government spending. However, this investment can address both the care and economic crises by bolstering employment, effective demand, and income generation, thereby boosting tax revenue for financing government budgets. Governmental authorities must ensure fair wages and favorable working conditions for new care jobs, including job and social security benefits. In Turkey, approximately 520,000 beneficiaries of cash-for-care schemes provide around-the-clock home care. Additionally, care services are frequently offered by unregistered workers, who are often underpaid. Therefore, Atasü-Topcuoğlu (Reference Atasü-Topcuoğlu2021) critiques the current system as a distorted commodification of care. Transitioning to a system employing qualified care workers for home-based services would promote decent employment and quality care provision, necessitating government regulation shifts away from cash-for-care towards an institutionalized professional care services system.
The inclusion of the Syrian refugee population into calculations gives insight into the strain on the care services infrastructure in Turkey due to the refugee influx. As of 2019, Turkey’s registered Syrian population totaled 3,576,370 individuals, with 54 percent men and 46 percent women (Refugees Association 2019). Syrians under temporary protection have the right to benefit from free education, healthcare, and LTC services in public institutions (Ombudsman Institution 2018).
We have estimated the coverage gap and costs of required investments in the education services sector for Syrian children except those under 5 years. When the Syrian school-age population is considered in education services, the coverage gap rose by around 1 million students, corresponding to an increase in the ratio of the cost of the coverage gap to GDP from 2.28 percent to 2.50 percent. In the health sector, with the inclusion of Syrians as beneficiaries, the coverage gap increased from 303,774 to 332,266 workers, bringing about a rise in the cost of the coverage gap from 1.23 percent to 1.24 percent of GDP. Overall, the initial investment cost for care services was 151.5 billion TL, or 3.51 percent of GDP. After including the Syrian population, it rose to 161.6 billion TL, or 3.74 percent of GDP (Table 4).
Table 4. Coverage gap and cost in care sectors (Syrians included)
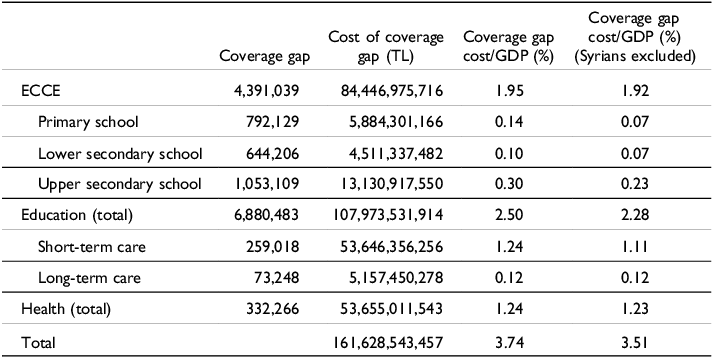
GDP, gross domestic product; ECCE, early childhood care and education.
Source: Authors’ own calculations based on Ministry of National Education (2019a), Ministry of Health (2019a), Turkish Statistical Institute (2019a), Organisation for Economic Co-operation and Development (2023), and Refugees Association (2019) data.
Including the Syrian population, education sector job creation will total 1,084,000, and health sector job creation will reach 794,000, culminating in 1,878,000 new direct jobs (Table 5). This represents an 8 percent increase compared to the scenario excluding Syrians.
Table 5. Direct employment impact of care services investments (number of new jobs) (Syrians included)
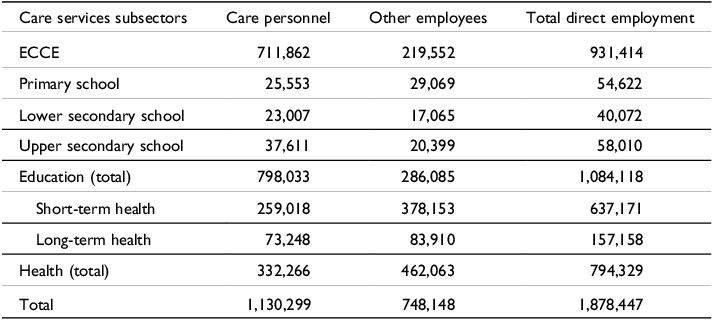
The expansion of the analysis to include the Syrian refugee population offers valuable insights for policy design on care service expansion in a time of significant refugee arrivals. Turkey, as a developing nation, shoulders a substantial responsibility in accommodating a large refugee population, which faces considerable hurdles in labor market integration and social integration. Despite high primary school enrollment rates among Syrian students, there is a significant drop in continuing education compared to Turkish students (Kırdar et al. Reference Kırdar, Koç and Dayıoğlu2023). The strain on the health system from the growing Syrian refugee population is evident, impacting both physical and human resources (Aygün et al. Reference Aygün, Kirdar and Tuncay2020). Additionally, older refugees face more significant challenges in resettlement and living conditions than other refugee groups (Yaylagül and Aslan Reference Yaylagül and Aslan2020). The presence of refugees intersects with strains in the economic and care systems, necessitating focused attention to bolster care infrastructure and address the multifaceted challenges.
Conclusion
Our analysis of care investments in Turkey has shown that care coverage gaps are substantial, particularly in ECCE and LTC, but also non-negligible in education and healthcare. The cost of eliminating the gaps is also substantial, amounting to as much as 3.52 percent of GDP. In the face of demographic trends such as an increasing and aging population or external shocks such as global pandemics or refugee and migrant arrivals, the gaps and costs are bound to increase. Hence, an investment plan to be rolled out over time must be implemented without delay.
On the positive side, our findings show that investing in a comprehensive care services infrastructure also comes with multiple social and economic payoffs. Prioritizing investments in care services will play a critical role in designing macroeconomic policies towards the full employment goal, given the sector’s high employment multipliers. Our analysis showed that expanding care services towards comprehensive coverage can create as many as 1.9 million new jobs, both directly and indirectly. If so, the share of care services employment in total employment in Turkey is estimated to increase from its current low level of 13 percent to 18.1 percent, bringing it closer to the regional average for Central Asia and Europe (19.5 percent) (International Labour Organization 2018). The strong job (and earnings) generation outcome of care investments implies also their potential for self-financing through increased tax revenues, which has been shown in previous applied work (İlkkaracan et al. Reference İlkkaracan, Kim and Kaya2015; Kim et al. Reference Kim, İlkkaracan and Kaya2019; Onaran and Oyvat Reference Onaran and Oyvat2023).
Prioritization of investments in public spending decisions will also serve to build resilience against external shocks such as the COVID-19 pandemic and ensure economic and social sustainability in the face of economic crises. The epidemic once again reminded us of the importance of the social state in terms of managing crises and eliminating social inequalities through an institutionalization and policy design that prioritizes social benefit and care for the people and the planet instead of market-centered solutions (İlkkaracan and Memiş Reference İlkkaracan and Memiş2021).
Universal access to quality care services improves the quality of life and decreases the vulnerability of care-dependent groups such as small children, youth, the elderly, and the ill. It also serves as an essential strategy for promoting gender equality. Access to quality care services alleviates time constraints on women’s labor supply by shifting an important share of care work from unpaid domestic work to paid public work. Expansion of care services employment also promotes women’s integration into the labor market on the demand side, as job creation through care spending is not only substantial but also favors demand for female labor. The findings of this paper show that 65.4 percent of new jobs created through increased care spending (more than 1.2 million new jobs) are likely to employ women, improving women’s labor force participation and narrowing the gender gaps in the labor market.
Prioritizing investments in a comprehensive care services infrastructure in public budgetary decisions is of particular importance in a country such as Turkey, where economic growth has weak job creation performance, a high rate of joblessness poses a structural challenge, gender gaps in the labor market persist over time, and a large refugee population exerts further demands on the existing care services system.
We should conclude by noting some of the limitations of the analysis and identifying the need for further research. First, the IO analysis of indirect employment estimation suffers from its static nature and restricting assumptions. Most importantly, we used IO tables from 2012 as the most recent table compiled by the Turkish Statistical Institute. However, by incorporating 2019 data from the care services sector into the 2012 IO tables, our computations for indirect employment were based on the assumption that the input coefficients of care services sectors remained constant over time. The synthetic sector approach used by İlkkaracan et al. (Reference İlkkaracan, Kim and Kaya2015) and Ilkkaracan et al. (Reference Ilkkaracan, Kim, Masterson, Memiş and Zacharias2021) can serve to alleviate some of these concerns. This methodology, however, can be costly to the extent that it requires conducting field surveys with care providers to collect data on their cost structure and determine their relationship with other sectors.
Secondly, the study’s coverage of care services subsectors does not present a complete picture. Primarily, LTC calculations were confined to the elderly but did not include care and support services for the disabled. This was in part due to the exclusion of this category in the policy tool by UN Women and International Labour Organization (2021) and in part due to data limitations. Further research would benefit from the development of global methodological tools such as UN Women and International Labour Organization (2021) to cover care services for people with disabilities. Moreover, examples of niche studies such as Mendez Santolaria and Rodriguez Enriquez (Reference Mendez Santolaria and Rodriguez Enriquez2023a, b) show that social services for particular vulnerable groups (such as children with special needs and gender violence victims) are also worth assessing depending on the national or local context.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/npt.2024.32
Acknowledgments
This paper is based on a research study funded by the Turkish Scientific and Technical Research Agency (TÜBİTAK) (grant no. 120K602) entitled “The COVID-19 Pandemic and Care Crisis from a Gender Perspective: Employment Impact of Public Investments in Care Services.”
Competing interests
None.








 Open access
Open access