



The home of former US President Jimmy Carter and his wife, Rosalynn, in Plains, Georgia, has transitioned from a hub of lively storytelling and travel souvenirs to a place of “quiet and calm,” according to their grandson, Josh Carter (Rosen and Alvord Reference Rosen and Alvord2023). The 39-year-old reflects on how the dynamic has shifted over time, especially after the recent health updates on his grandparents. In February 2023, the Carter Center announced that Jimmy Carter, now 98, had decided to cease medical intervention and enter hospice care to spend his final days at home with family. Three months later, it was revealed that Rosalynn Carter, 96, had been diagnosed with dementia. “Since Jimmy began hospice, there’s always somebody at the house,” says Josh. Despite their health challenges, Jimmy and Rosalynn remain aware and present. “He’s still fully Jimmy Carter. He’s just tired,” adds Josh, noting that his grandmother understands her condition and still recognizes family members. Hospice is a family experience requiring a tender, loving environment of support.
Watching his grandparents’ journey, especially Jimmy witnessing Rosalynn’s fading memory, has been a complex emotional experience for Josh. “Gotta be hard,” he says, “but on the other hand, they’ve experienced everything that you can together.” The family finds comfort in small but profound gestures of affection between the couple. “They are still holding hands … it’s just amazing,” Josh marvels. As they approach what Josh calls the “final chapter,” the family takes comfort in knowing that Jimmy and Rosalynn Carter “lived their lives to the fullest.” Though the impending losses won’t be any easier, this recognition offers solace. As the Carter family navigates this delicate period, they are enveloped in love and gratitude for the fulfilling lives that their patriarch and matriarch have given them. It’s a time for reflection, acceptance, and the quiet cherishing of the bonds that tie them together (Rosen and Alvord Reference Rosen and Alvord2023).
As this life-affirming story from People magazine describes, hospice is a service about life, family, and friends – loved ones surrounding. Beyond mere bodily care, a central guiding principle of hospice is that the patient and loved ones are the unit of care, reflecting the vitality of including family and other loved ones in the care at the end of life (Smith and Granbois Reference Smith and Granbois1982). In keeping with this principle, services for family members, while enrolled and post-death, are recognized as core components of high-quality hospice care (Ferrell et al. Reference Ferrell, Twaddle and Melnick2018). This holistic model of caring for grieving family members dates back to the historical roots of the hospice movement in the United Kingdom and was adopted by American hospices (Connor Reference Connor2008; Kissane et al. Reference Kissane, Lichtenthal and Zaider2007).
Yet, a plethora of evidence reveals that the hospice movement’s values and influence are being threatened by private equity and other profiteers (Aldridge et al. Reference Aldridge, Schlesinger and Barry2014; Brereton et al. Reference Brereton, Matlock and Fitzgerald2020; Davlyatov et al. Reference Davlyatov, He and Orewa2023; Hotchkiss Reference Hotchkiss2022; Price et al. Reference Price, Parast and Elliott2023, Reference Price, Tolpadi and Schlang2020). Long-time hospice expert, Teno (Reference Teno2023) captures the problem succinctly. With for-profit entities now comprising 73% of hospice programs, some prioritize profitability to a concerning degree. Weak or absence of regulations regarding visit frequency or professional staff qualifications allows for the potential reduction of visits and employment of less-qualified healthcare personnel, which, while increasing profit margins, can result in diminished emotional and bereavement support (Teno Reference Teno2023). Caregivers of hospice patients are considered enrollees by Medicare. In our caregiver studies, 5-star reviews (36%) had statistically significantly more declarations of family support and bereavement than concerns of nonsupport in 1-star reviews (25%) (Hotchkiss et al. Reference Hotchkiss, Ridderman and Hotchkiss2023c). Several studies chronicle large hospice profit-making negatively impacting US care quality (Aldridge et al. Reference Aldridge, Schlesinger and Barry2014; Brereton et al. Reference Brereton, Matlock and Fitzgerald2020; Davlyatov et al. Reference Davlyatov, He and Orewa2023; Hotchkiss Reference Hotchkiss2022; Price et al. Reference Price, Parast and Elliott2023, Reference Price, Tolpadi and Schlang2020). However, no study has reported on caregiver satisfaction on support received, expressed online by hospice.
With this shortfall in hospice quality colorfully described in a recent publication, Vivid Depictions of Big Hospice Quality (Hotchkiss Reference Hotchkiss2023), the purpose of this investigation was to evaluate the specific caregiver experience of emotional, spiritual, and bereavement support, appraise whether the care was respectful and compassionate to the care unit and assess the impact of profiteering on this type of support. As part of the Conditions of Participation, Centers for Medicare and Medicaid Services (CMS) defines this support as “emotional, psychosocial, and spiritual support and services provided before and after the patient’s death to assist with issues related to grief, loss, and adjustment” (Federal Register Reference Register2011). CMS specifically requires hospices to provide an initial and ongoing bereavement assessment of the needs of the patient’s family members. These assessments must be incorporated into the care plan, and psychosocial–spiritual care must be provided.
One study analyzed survey responses from 657,805 caregivers and their deceased loved ones involved with 3,160 hospice programs (Parast et al. Reference Parast, Elliott and Haas2021). Models were used to examine the link between the caregivers’ perception of emotional and spiritual support (“too little,” “right amount,” or “too much”) and their overall hospice ratings on a scale from 0 to 100. They also assessed how this relationship varied across racial, ethnic, and linguistic groups through interaction terms. Complaints of “too much” emotional support were rarer than those of “too little.” Across all groups, receiving “too little” support was strongly linked to lower hospice ratings than an appropriate support level.
RAND Corporation, who was contracted by CMS to design and manage the Hospice Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey, also has significant research demonstrating that on the topic of support in general in hospice (Parast et al. Reference Parast, Elliott and Haas2021). In a mixed-methods study with 623 survey responses and in-depth interviews with a subsample of 17 respondents, researchers asked caregivers: “During the last month of your family member’s life, did he or she receive too little, the right amount, or too much medical care?” Of the 623 survey respondents, 16.9% reported their loved one received “too little” care while only 1.4% reported “too much.” Likelihood of reporting too little medical care did not differ by age, gender, or being insured by Medicaid only. Respondents who reported “too little” compared with those that stated the “right amount” reported higher unmet needs for symptom palliation, physician communication concerns, with other important opportunities to improve the quality of care. Among the 17 in-depth interviews of those indicating “too little” care on the structured survey, the predominant concern (n = 10) was inadequate symptom management.
On the other hand, the negative impact of “too much” support on hospice ratings was much less pronounced, especially among caregivers of white and black decedents. Interestingly, “too much” support resulted in more favorable ratings among caregivers of Hispanic decedents. The findings indicate that having “too much” support is a far less significant factor in poor hospice ratings than not having enough. This suggests that in hospice evaluations, “too much” support should not be rated the same as “too little” support. Therefore, hospices should prioritize ensuring adequate emotional and spiritual support for caregivers, erroring on the side of providing too much support.
While it is noble to allow caregivers to define what is supportive, this narrow way of appraising a vital aspect of hospice care has created ceiling effects – skewing scores so high that their ability to distinguish performance is lost. Poor-performing hospices still have high scores for Emotional, and spiritual support and Treating patient with respect – the bar is set too low in the item design of the CAHPS survey. We found that spiritual, emotional support and treating patient with respect were the highest CAHPS scores in all sourced CAHPS studies in an extensive literature search (Davlyatov et al. Reference Davlyatov, He and Orewa2023; Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b; Parast et al. Reference Parast, Haas and Tolpadi2018b; Price et al. Reference Price, Parast and Elliott2023, Reference Price, Stucky and Parast2018, Reference Price, Tolpadi and Schlang2020; Quigley et al. Reference Quigley, Parast and Haas2020). Among the 50 hospices in our studies, 46 of 50 (92%) had these 2 scores much higher than the other 6.
As further evidence, 10 bottom-dwelling hospices with the lowest overall quality, CAHPS scores for the other 6 measures had distinguishing capability (77, 79, 71, 77, 73, 70; Mean = 74) (Hotchkiss Reference Hotchkiss2023). While CAHPS scores for the above 2 “easy-street” CAHPS survey measures were respectively (88 and 89). The 2 sources of national norms, 1 posted on Hospice Care by CMS (Hotchkiss Reference Hotchkiss2022) and the second Davlyatov’s (Reference Davlyatov, He and Orewa2023) large national study of 1,956 hospices have scores reported as follows, respectively Emotional, spiritual support (90.00, 90.06) and Treating patient with respect (90.00, 90.08). This means that performance in these arenas needs to be better adequately distinguished in the test design of the CAHPS. As a testament to the value of “support” by caregivers, emotional–spiritual support specifically, very few white and black decedents describe the support as “too much.” Hispanic decedent valued this as well, since “too much” support was associated with better CAHPS scores. In sum, this is death, dying, grief, and loss, caregivers said it is near impossible to provide “too much” support.
The CMS, anticipating that caregivers would need post-death support, have stipulated that bereavement care must be provided for up to 13 months after a patient’s passing in the Conditions of Participation (Register Reference Register2008). Hospice providers, from time of admission, must also conduct initial bereavement and ongoing risk assessments before patients’ end of life to identify any social, spiritual, or cultural factors that may affect the grieving process. This assessment also helps providers determine the best combination of services and support to offer families before and after patients’ passing.
Evidence indicates that supportive services for grieving families can improve their post-loss adjustment (Allumbaugh and Hoyt Reference Allumbaugh and Hoyt1999; Forte et al. Reference Forte, Hill and Pazder2004; Schut and Stroebe Reference Schut and Stroebe2005), particularly if provided soon after a loss and to those at risk for prolonged or complicated grief (Jordan and Neimeyer Reference Jordan and Neimeyer2003; Schut and Stroebe Reference Schut and Stroebe2005; Zhang et al. Reference Zhang, El-Jawahri and Prigerson2006). Although Medicare-certified hospice programs are required to support bereaved family members, services are not separately billable, and the specific services offered are left to the discretion of the hospice. As Medicare reimbursement is not tied to the level or quality of services provided to family members, limited financial incentives exist to deliver more than a minimal level of care. A study by Carlson et al. (Reference Carlson, Morrison and Holford2007) examined caregiver support services provided by hospices and found that only 59% of hospices offered some level of emotional support. The limited financial incentives to provide quality bereavement services have led to neglect of grieving caregivers and family members.
This trend conflicts with the fundamental philosophy of hospice care, which emphasizes providing quality, personalized, and compassionate end-of-life care. While the emergence of profit-driven entities in hospice care has shifted the focus toward numbers and admissions, it’s crucial to acknowledge the presence of numerous committed hospice providers, both nonprofit and for-profit, who prioritize exceptional patient care. Further research and policy development are essential to ensure the Medicare Hospice Benefit maintains its original aim of delivering high-quality end-of-life care for all qualified patients.
With less than one-third of hospices having CAHPS scores reported on Hospice Compare (Rahman et al. Reference Rahman, Cardenas and Singleton2021; Rahman and Enguidanos Reference Rahman and Enguidanos2020), there exists an untapped, rich resource of hospice quality data in open-ended online reviews providing assessment of hospice consumer experience data, where it is missing or not meeting the criteria for number of reviews per hospice (>30 reviews). CMS requires a minimum of 30 decedent caregiver reviews to post CAHPS scores on Hospice Compare (CMS 2021). In sum, because hospices are required to pay for their own third-party CAHPS assessment, survey responses must meet a minimum threshold (n > 30), and due to low (29%) mean response rate (CAHPS 2021), over two-thirds of hospices programs have no CAHPS scores posted on Hospice Compare. The above limits of CAHPS increases the value of online reviews, especially since this enrollee feedback is monetarily free and always available.
Since the quality of hospice care in the United States has become a topic of concern over the last 2 decades (Carlson et al. Reference Carlson, Gallo and Bradley2004; Perry and Stone Reference Perry and Stone2011; Wang et al. Reference Wang, Beltran and Gammonley2021), we developed a method and model of hospice quality assessment from caregiver reviews using Watson’s carative model (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a). Hospice caregivers made caring staff the highest indicator of hospice quality in their reviews. CMS’ Medicare-sponsored hospice benefit views the “unit of care” as the patient, their family, or other loved ones (Barry et al. Reference Barry, Carlson and Thompson2012; CMS 2021).
Examining caregivers’ expressions from a grounded theory perspective digs deeply into their values, and supports, the processes and outcomes of standardized assessments like CAHPS. This research focuses on elucidating caregivers’ sentiments concerning emotional, spiritual, and bereavement support, drawn from open-ended reviews. While CAHPS scores have been employed in previous studies, this research makes a distinct contribution by delving into the caregiver experience of support as conveyed in online feedback within the hospice context, employing sentiment analysis with natural language processing.
Our central research question in this study was: how do enrollees feel about Big Hospice in America? That big-picture question was operationalized by the following detailed research questions from which associated hypotheses were formed. (1) How did caregivers feel about emotional, spiritual, and bereavement support in nonprofits vs. for-profits? (2) How did perceived compassion and respect vary by profit status? (3) How does the caregiver experience, captured by the closed-ended CAHPS survey, differ from the story told by online reviews of the same hospices? Thus, this study aimed to evaluate the hospice caregiver experience of emotional, spiritual, and bereavement support, appraise whether the care was respectful and compassionate to the care unit, and assess the impact of profiteering on the resulting emotional and spiritual support.
Methods
Adopting a retrospective user experience approach, this research builds upon 4 preceding studies, briefly summarized here due to their methods, results, and selected variables being leveraged in the current study. The initial study, employing a quantitative design, revealed that Glassdoor scores and profit status predicted Hospice CAHPS scores among the 50 largest US hospices (Hotchkiss Reference Hotchkiss2022). The second study employed qualitative thematic analysis, identifying 20 themes from 3389 Google and Yelp reviews organized into 5 primary categories. We formulated a method and model to qualitatively code hospice caregiver review themes, compare themes between star ratings, and utilize Watson’s carative model as an interpretative framework for comprehending the needs of decedent caregivers (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a). In a third study, we applied the model to a stratified sample of reviews to assess the overall quality of hospice in the United States (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b).
To summarize our prior findings, in Table 1, we integrated the prescribed topics in the CAHPS assessed by close-ended questions and contextual topics offered up in open-ended caregiver reviews. Having established a method for comparing review themes, we concentrate our reporting on addressing current research questions about quality differences between nonprofit and for-profit hospices on the topic of support. Then, most recently, our study focused on CAHPS and overall sentiment by profit status (Hotchkiss et al. Reference Hotchkiss, Ridderman and Hotchkiss2023c). Readers may consult this prior study for details on the development of review themes and our Hospice Quality Model (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a) and its application to overall US quality (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b). Table 1 depicts our Hospice Care Quality Model broken out into main topics and subtopics, summarizes the findings from these prior studies. This study extends these findings and applies the developed methods to explore specifically how caregivers feel about emotional, spiritual, and bereavement support among for-profit and nonprofit hospices.
Table 1. Hospice Quality Model by main topics and subtopics in online caregiver reviews with relationships to CAHPS and Watson’s carative factors
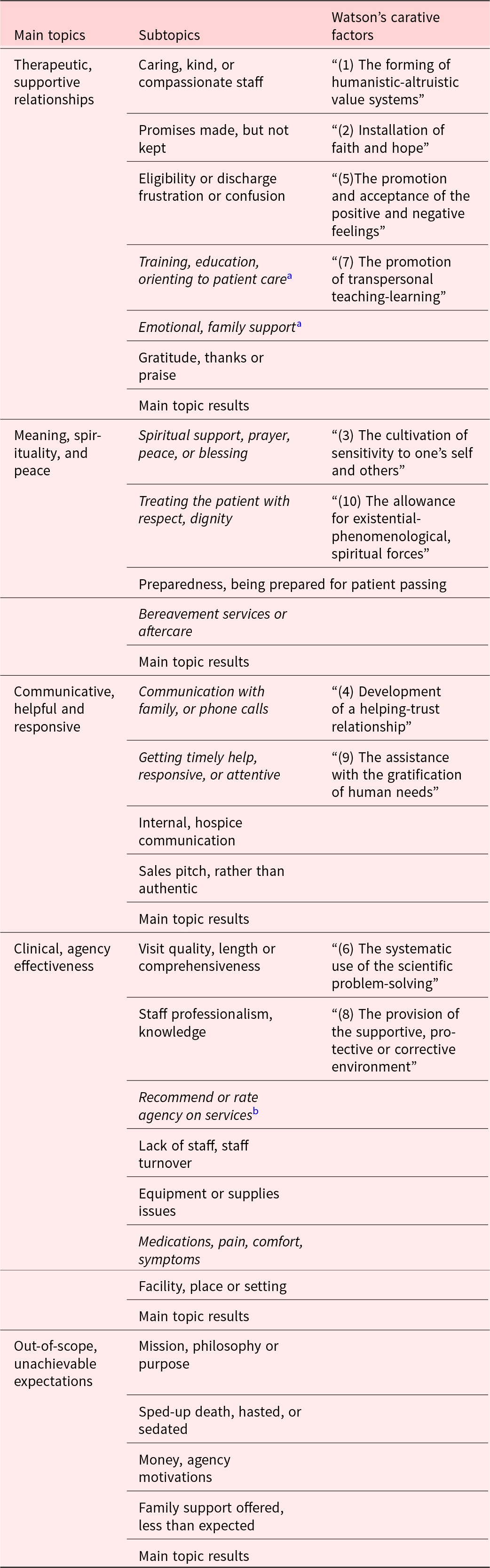
Note: Adapted from Hotchkiss (Reference Hotchkiss, Ridderman and Buftin2023a) – Hospice Quality Model.
CAHPS-related are presented in italics, there are 8 measures: 6 specific and 2 global.
a Six specific CAHPS measures – “Emotional, spiritual support”, “Communication with family”, “Timely Help”, “Help with pain and symptoms,” “Training family to care for patient,” and “Treating patient with respect”.
b Two Global CAHPS measures – “Willingness to recommend” and “Rate the hospice”.
Measures
With the model of hospice quality, developed in prior research (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a) and tested and validated among the 50 largest hospices (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b), we drew upon the developed model with its main and subtopics, 8 of which correspond to the 8 CAHPS measures. Main topics and selected subtopics were explored in more depth to fit this study’s aims. CAHPS Composite was a latent variable, and the 8 measures were its observed variables. In this study, Caregiver Sentiment on a given topic operationally defined how a caregiver felt about a given hospice on a particular topic. CAHPS Composite and Caregiver Sentiment are latent, composite measures with 8 and 25 variables, respectively.
The quantitative data used were CAHPS scores and hospice characteristics of the 50 largest US hospices. Sentiment analysis of full-text, open-ended caregiver reviews was how the qualitative hospice user experience was captured. This is how we assess how caregiver felt about their hospice experience. User experience expressed in reviews was quantified into measures compared to each hospice’s CAHPS data and hospice characteristics. We now define these study variables below.
CAHPS variables
The CAHPS Hospice Survey instrument comprises 47 items and calculates 6 topical and 2 global hospice quality measures. For a given hospice, CAHPS scores were calculated based on all available data since the commencement of the CAHPS process in 2015 until 2023. These measures range from 0 to 100, where a higher number indicates higher caregiver satisfaction (CMS 2023). Current CAHPS data were obtained from Hospice Compare which reports the 8 cumulative CAHPS scores for a given hospice (CMS 2023). Due to the focus here on the human aspects of hospice care, we only selected 3 CAHPS measures described below.
CAHPS Composite
CAHPS Composite (0–1) is the mean of all CAHPS scores and can be conceptually interpreted as a grade out of 100. All CAHPS scores are reported from 0 to 1 (CMS 2023).
CAHPS “Emotional, spiritual support”
Three items are used to appraise emotional, spiritual, and post-death bereavement support. (1) How much support for your religious and spiritual beliefs did you get from the hospice team? (2) While your family member was in hospice care, how much emotional support did you get from the hospice team? and (3) In the weeks after your family member died, how much emotional support did you get from the hospice team? Each question has only 3 options, “Too little, Right amount, Too much” (CMS 2023).
CAHPS “Treating patient with respect”
One item is leveraged to assess respect and dignity. 1. While your family member was in hospice care, how often did the hospice team treat your family member with dignity and respect? The response options were “Never, Sometimes, Usually, Always.”
Other hospice variables
Two hospice characteristic variables were also gathered: profit status and market share. Profit status was set at 0 = nonprofits and 1 = for-profits. Market share was operationally defined by the 2020 Lexis–Nexis list of 50 of the 100 largest US hospices by market share (Shabbir Reference Shabbir2021).
Sentiment analysis
Caregiver Sentiment
The caregiver experience of hospice was captured and reported with ± in front of 2 decimal places (+.54). Caregiver Sentiment was operationally defined as the mean of all 25 topic sentiments of caregivers weighted by Prevalence. Sentiment scores ranged from –1 to +1. Scores closer to +1 express positivity, and closer to –1 express negativity. A sentiment score greater than +.40 is defined as an excellent experience (indicated by blue), between +.25 and +.40 is considered a good experience (green), 0 to +.25 is defined as neutral (yellow), between 0 and –.25 is regarded as a dissatisfying experience (orange), and finally, lower than –.25 is operationalized as frustrated-to-angry (red).
Topical sentiments
The main topics and subtopics are also presented in Table 1. CAHPS-related topics are in italics. To keep reporting concise, operational definitions are available for reference on each topic in the Hospice Quality Model, presented in the first table in both studies (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a, Reference Hotchkiss, Ridderman and Buftin2023b). We developed the model of hospice quality in the first study (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a) and then leveraged the topical model for hospice quality assessment in a second study (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b).
Emotional Intensity
Emotional Intensity, which gauges the degree of emotional expression in a review, takes into account review length and is defined as the mean of all caregiver topic magnitudes, adjusted by Prevalence, with scores spanning from 0 to infinity. Scores nearer to 0 signify minimal emotion, whereas higher values indicate more Emotional Intensity and lengthier reviews. Raw scores were employed to differentiate overall emotional expressions by hospice and topic.
Procedure
Using the list of 50 largest hospices already established (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a), we conducted a qualitative analysis of these hospices’ reviews obtained from Google and Yelp. We leveraged an application called ExportComments.com to download all reviews from a given program star ratings on either rating platform. Using the developed Python code for sentiment analysis, we outputted results from main and subtopics by hospice. Since, we already developed a method for comparing review themes between star ratings and reported on the results in a prior study, we focus our findings on the difference by profit status. To normalized topical sentiment scores (–1 to +1) to compare with CAHPS scores (0–1), we used the following standard formula: normalized topical sentiment = (topical sentiment +1)/2. This method could be used to normalize any sentiment scores for major, subtopics or the overall Caregiver Sentiment.
Analysis
This study utilized a mixed-methods approach to explore the relationship between variables, seeking to grasp caregivers’ views on Big Hospice in America through narrative data processed using natural language programming and analyzed following sentiment analysis best practices. Utilizing our preestablished method and model for quality assessment from open-ended caregiver reviews, we conducted sentiment analysis on each sample using our Python code, calculating sentiment, emotional Intensity scores, and prevalence for each of the 25 topics across all hospices. Due to the substantial quantity of variables (94 total), our analysis is divided into 2 reports, with the first already exploring the relationship between overall sentiment, employee satisfaction, and CAHPS scores (Hotchkiss et al. Reference Hotchkiss, Ridderman and Hotchkiss2023c). The latent measures of CAHPS Composite and Caregiver Sentiment were established as highly associated global measures converging on caregiver-rated quality from 2 disparate sources (Hotchkiss et al. Reference Hotchkiss, Ridderman and Hotchkiss2023c).
This study, part 2, will look more deeply at the sentiment analysis on the human services topics of caring, respect, emotional, spiritual, and post-death bereavement support. We seek to understand the relationship of common topics in reviews to the close-ended assessment of CAHPS. Thus, the following hypotheses and testing methods guided the study.
Hypothesis 1a: Therapeutic, supportive relationships; Emotional, spiritual, and bereavement support will be positively associated with close-ended CAHPS Composite.
Hypothesis 1b: Therapeutic, supportive relationships; Emotional, spiritual, and bereavement support will be positively associated with open-ended Caregiver Sentiment. Pearson’s correlation will be used to evaluate Hypotheses 1a and b.
Hypothesis 2a: Therapeutic, supportive relationships, as expressed in Caregiver Sentiment, will be higher for nonprofits than for-profits.
Hypothesis 2b: Emotional, spiritual support will be higher for nonprofits than for-profits.
Hypothesis 2c: Caring, compassionate staff, as expressed in Caregiver Sentiment, will be higher for nonprofits than for-profits.
Hypothesis 2d: Treating patient with respect will be higher for nonprofits than for-profits.
Independent sample t-tests will be used to test Hypotheses 2a–d.
Hypothesis 3a: CAHPS measurement of Emotional, spiritual support have limited variance and thus less discriminating values than the same evaluation gleaned from caregiver reviews.
Hypothesis 3b: CAHPS measurement of Treating patient with respect have limited variance and thus less discriminating values than the same evaluation gleaned from caregiver reviews.
Distribution and variance results will be used to test Hypotheses 3.
Results
Table 2 reports all study variables for the 50 largest US hospices, ordered by overall quality Emotional, spiritual support. Among 4279 reviews, hospices received an average of 86 each, ranging from 32 to 341. On time context, the range of the review year was from 2013 to 2023. The median was 2019 and the mode was 2021 with skew in the direction of more recent reviews. The median year of these submissions was 2019, and the most frequently occurring year was 2021, indicating a skew toward more recent reviews. To provide a basis for comparison, the CAHPS scores used in this study were collected from 2015 through the end of 2023. Notably, a substantial 96% of the 4,297 reviews were submitted during the years 2015–2023. Therefore, both the CAHPS surveys and online reviews were gathered over a nearly 10-year timeframe, with a specific focus on the period from 2015 to 2023. Consequently, it can be observed that the data collection periods for CAHPS and online reviews largely overlap.
Table 2. Study variables for the 50 largest US hospices, ordered by emotional, spiritual, and bereavement support

Note: 1. Caregiver Sentiment is the mean of all topical sentiments of caregivers weighted by prevalence. Scores range from −1 to +1. Scores closer to +1 express positivity, closer to −1 express negativity.
2. Emotional Intensity is the mean of topic magnitudes of caregivers by prevalence. Scores range from 0 to infinity. Scores closer to 0 express little emotion, the higher score means more intensity.
3. CAHPS Composite is the mean of all CAHPS measures.
4. Reviews per hospice. For small market share <.3%, we obtained 30 reviews; for medium size (.3–.5%) = 50 reviews; larger (.5−1.0%) = 100 reviews, and the largest (>1.0%) = 200−250 reviews.
6. Market share is Lexis–Nexis reported percentage US Hospice Market Share; ranged between .22% (Transistions) to 4.42% (VITAS)
7. CAHPS “Emotional, spiritual support” is composed of 3 items, 1 for each of these: emotional, spiritual, and bereavement support.
8. CAHPS “Treating patient with respect” is composed of 1 item.
9. Lack of staffing (%) is the prevalence of reviews where caregivers report staffing, either in quality or quantity, as the cause of their service problems.
10. Out-of-scope, unachievable expectations that reveal aspects of end-of-life care that are outside the scope of the Medicare Hospice Benefit, Conditions of Participation describe what is in-scope.
11−18. Topical sentiments, both main and subtopics, see Table 1 for Hospice Model topic details.
19. Emotional, spiritual support (normalized, 0−1) = (Emotional, spiritual support +1)/2.
20. Respect, honor, and dignity (normalized, 0−1) = (Respect, honor, and dignity + 1)/2.
While nonprofits (n = 27) exceeded for-profits (n = 23) in number, most notably, large for-profit conglomerates own several nonprofits. Nonetheless, for-profits held almost double the market share (20.80%) compared to nonprofits (11.34%). The market remains fragmented, with the 50 largest hospices comprising only 32.32% of the hospice industry’s market share, valued at $34.5B in 2022 (NHPCO 2022).
Among the top 25 in quality, as measured by Emotional, spiritual support, 21 were nonprofits. Contrarily, the bottom 25 in quality comprised 17 for-profits, and only 8 were nonprofits. Table 3 reports bivariate correlations between study variables, and the strong relationships are noteworthy. Three main topic sentiments – Therapeutic, supportive relationships; Communicative, helpful, and responsive; and Clinical, agency effectiveness – were co-occurring in reviews to such a high degree (.73 < r < .78, p < .001) that in the minds of reviewers, seems impossible to mention any of these main topics without touching on a highly related one.
Table 3. Bivariate correlations of CAHPS and Caregiver Sentiment variables

Bivariate correlations are limited to CAHPS and Caregiver Sentiment variables necessary to answer the study research questions.
* p < .05, **p < .01, ***p < .001.
Therapeutic, supportive relationships (r = .64, p < .001); Emotional, spiritual, and bereavement support (r = .59, p < .001) both had strong associations with closed-ended CAHPS Composite. Likewise, Therapeutic, supportive relationships (r = .69, p < .001); Emotional, spiritual, and bereavement support (r = .68, p < .001) had even stronger relationships to open-ended Caregiver Sentiment. The null hypothesis for Hypotheses 1a and b were rejected.
Therapeutic, supportive relationships among nonprofits was rated as excellent (M = .42, SD = .16) and significantly higher than for-profits (M = .32, SD = .19), t(48) = 2.13, p < .05 with moderate effect, Cohen’s d = .60. Emotional, spiritual, and bereavement support sentiment was in the excellent range (M = .47, SD = .14) for among nonprofits, and yet fell to dissatisfying with for-profits (M = –.15). Encouragingly, caring, kind, and compassionate professionals were lauded with deeply grateful sentiments in nonprofits (M = .57, SD = .15) and for-profits (M = .46, SD = .21). Even though a statistical difference was detected t(48) = 2.08, p < .05 with moderate effect (d = .59), both were rated in the excellent range for caring staff (>+.40). Thus, the null hypothesis for Hypotheses 2a–c were all rejected. Relatedly, nonprofits (+.36) had significantly higher sentiment on the main topic, Clinical, agency effectiveness, than for-profit hospices (+.21), t(48) = 3.12, p < .001 with a powerful effect, Cohen’s d = .89. Nonprofits score nearly 1 SD above their for-profit counterparts in overall care quality – Clinical, agency effectiveness, whereas for-profits scored in the neutral range.
As displayed in Table 4, it is noteworthy that all independent sample t-tests for main topics revealed that nonprofits received more favorable Caregiver Sentiments than for-profits. The effect size ranged from moderate to large. Only Respect, honor, and dignity was not significantly higher among nonprofits. A respectful experience (16.04%) was much less commonly expressed than a compassionate one (38.32%). Out-of-scope expectations (–.28) in for-profits were associated with more frustration than among nonprofits (–.11), likely due to the selling and promises made before admission.
Table 4. Descriptive results for topical sentiments, emotional intensity, prevalence, and t-tests by profit status

M = mean, SD = standard deviation.
While all 25 subtopics were used to reports on the main topics, we restricted our report of subtopics to relevant aims.
a Cohen’s d can range above 1. For example. Cohen’s d of 1.0 indicates difference of 1 SD.
b Emotional, spiritual support included family, bereavement support, and aftercare.
c Emotional intensity = Magnitude of feeling expression and review length. Only measures intensity.
d There were no significant statistical differences in Emotional Intensity of any topics by profit status; thus, t-tests are not displayed.
e Prevalence was a more valuable and practical measure of caregiver values than Emotional Intensity, at the topical level.
f To focus on research questions, subtopics Spiritual support was combined with Emotional support to align with the CAHPS-equivalent.
* p < .05, **p < .01, ***p < .001
CAHPS Treating patients with respect and Emotional, spiritual support and appears to be suffering from ceiling effects since these scores are high even when other CAHPS measures are deficient. The bottom 10 in CAHPS quality are an excellent example of this. The variance was minimal in this study of Big Hospices and is congruent with other studies.
For-profits had significantly higher overall Emotional Intensity than nonprofit hospices, again with a strong effect. However, Emotional Intensity by topic (displayed at the bottom of Table 4) did not vary significantly by profit status. On the whole, the main topics and subtopics in this study were discussed with the same degree of intensity regardless of profit status.
The third most common subtopic in reviews was emotional, spiritual, and bereavement support. We noticed a pattern of caregivers mentioning supportive experiences beyond the direct medical care of their loved one in over one-third of reviews (36.13%). The difference in overall Caregiver Sentiment between nonprofits and for-profits was even more manifest than the individual topical sentiments. Nonprofits (.41) had significantly higher overall Caregiver Sentiment than for-profit hospices (.15), t(48) = 4.106, p < .01 with strong effect, d = 1.17. Nonprofits scored more than 1 SD higher than their for-profit counterparts. Nonprofit hospices had significantly higher Caregiver Sentiment and CAHPS-related sentiments than for-profit hospices. To test how well our sample stratified by hospice size simulated the current daily census of hospice enrollees in the United States, we ran a regression to determine whether the sample could predict market share from sample size by hospice. The association was robust (r = –.92, p < .01).
Illustrated summary of findings
In summary, Figures 1 and 2 illustrate critical insights on how caregivers felt about Big Hospice by topic and profit status. We used a color legend to represent how caregivers felt about their experience; color definitions are described in the methods above. Because Emotional Intensity did not vary significantly by topic in this study, we report the Prevalence of main and subtopics as a way of advocating for what was most frequently expressed by caregivers. Emotional Intensity did vary widely by hospice, and was negatively correlated to Caregiver Sentiment. In short, enrollees were angry that they weren’t better supported by for-profits.

Figure 1. Non-Profit Caregiver Experience Expressed in Topical Caregiver Sentiments.

Figure 2. For-Profit Caregiver Experience Expressed in Topical Caregiver Sentiments.
Figure 1 illustrates the Nonprofit Caregiver Experience, and Figure 2 depicts the For-profit Caregiver Experience. Sentiment and Prevalence (±, %) are the 2 parameters reported in parenthesis. Nonprofits had 4 CAHPS-related sentiments rated as excellent by caregivers compared to none among for-profits. Hallmarks of the nonprofit “quality” experience were the following excellent topics as rated by caregivers: Getting timely help (+.43, 30%); Caring and compassionate staff (+.57, 38%); Spiritual, emotional support (+.47, 36%); and Gratitude, thanks, and praise (+.82, 32%). This led to caregivers rating the overall experience as good-to-excellent as captured in Clinical and agency effectiveness (+.36, 64%) and Willingness to recommend, Rate the hospice (+.38, 34%). Dissatisfying critiques of Lack of staffing (–.18, 6%) occurred at a low rate and were less impactful than in the for-profit experience.
For-profits had 2 CAHPS-related sentiments rated as frustrating-to-angry and 1 rated as dissatisfying. Trademarks of the for-profit “quantity” experience was an admission-first focus leading to frustrating laments of Lack of staffing (–.40, 15%), which cascaded into angry protests of Expected more family support (–.28, 36%); dissatisfying palliative care, Help with pain and symptoms (–.05, 13%). Fortunately, there were some commendations, Caring and compassionate staff (+.46, 45%), and occasional Gratitude, thanks, and praise (+.73, 19%). However, the overall experience was neutral as captured in Clinical and agency effectiveness (+.21, 55%); and Willingness to recommend, Rate the hospice (+.22, 35%). Gratitude was more commonly expressed toward nonprofits (32%) than for-profits (19%).
Evaluating Hypothesis 3, the distribution of CAHPS Treating patient with respect (M = 89.62, SD = 2.63) and CAHPS Emotional, spiritual support (M = 89.80. SD = 2.04) were very limited among the 50 largest. The corresponding topic sentiments from online reviews, reported in Table 4, had more variance, and thus increased discriminating value, as noted in Figures 3 and 4. Therefore, the null hypothesis of Hypotheses 3a and b was also rejected. CAHPS measurement of Emotional, spiritual support and Treating patient with respect have limited variance and thus less discriminating values than the same evaluation gleaned from caregiver reviews, where the variance was able to capture the difference between profit status that were more in keeping with the other CAHPS scores: Communication with family, Timely help, Help for pain and symptoms, Rating the hospice, and Willingness to recommend.

Figure 3. Histogram of CAHPS and Review Emotional, Spiritual Support.

Figure 4. Histogram of CAHPS and Review Respect, Dignity.
Discussion
Among the 50 largest hospices, this investigation aimed to evaluate the hospice caregiver experience of emotional, spiritual, and bereavement support, appraise whether the care was respectful and compassionate to the care unit, and assess the impact of profiteering on this type of support. The discussion here is focused on Caregiver Sentiment and satisfaction by size and profit status rather than individual hospice results. Readers are encouraged to source Vivid Depictions of Big Hospice Quality for detailed by hospice appraisals (Hotchkiss Reference Hotchkiss2023).
Three main insights on the caregiver experience will be discussed here: (1) Caring professionals deliver care whose quality is stunningly impacted by profit status; (2) Caregivers felt nonprofits provided much more effective spiritual and emotional support than for-profits; (3) CAHPS survey results appear to paint a much rosier picture of hospice support than online reviews, respecting patients is a low bar and should be raised to providing compassionate care to all enrollees, including patients. CAHPS items for Emotional, spiritual support need a re-designed scale with 4 options to raise the bar for emotional and spiritual support.
Compassionate professionals were thanked and praised regardless of profit status
The good news is that caregivers notice caring and compassionate professionals among both nonprofit and for-profit hospices. However, three red flags emerged from this study of caregiver reviews. The hot buttons of concern from caregivers were the following: lack of staffing; emotional, spiritual, and bereavement support for families; and help for pain and symptoms. Nonprofits had four CAHPS-equivalent sentiments rated as excellent by caregivers compared to none among for-profits. Hallmarks of the nonprofit “quality” experience were getting timely help from good responses to phone calls. The staff who arrived were caring and compassionate, providing practical spiritual and emotional support, which led to frequent praise. Lack of staffing was occasionally reported in one in 14 reviews. This level of staffing concern is likely due to market conditions. Whereas the for-profit experience reveals a quantity hospice focus, leading to more frequent complaints of lack of staffing.
For-profits had two CAHPS-related sentiments rated as frustrating-to-angry and 1 rated as dissatisfying. Trademarks of the for-profit “quantity” experience were an admission-first focus leading to off-hours, frustrating laments of lack of staffing, which cascaded into angry protests of expecting more family support and help with pain and symptoms. The overall experience was neutral, as captured in clinical and agency effectiveness and willingness to recommend the hospice. Gratitude was expressed toward nonprofits at one in three compared to for-profits, where the rate dropped below one in five. The longest and most emotionally intense reviews were from caregivers who could not reach anyone; when they finally got returned calls, visits were delayed, or no staff was available. On arrival, the family support was weak; thus, they were understandably frustrated and angry.
Caregivers felt nonprofits provided much more effective spiritual and emotional support
Caregivers felt nonprofits provided much more effective support. This finding agrees with wider research on profiteering. The transition toward prioritizing quantity over quality has altered the hospice care landscape. Evidence indicates that for-profit hospices tend to have lower patient-to-staff ratios, allocate fewer resources to direct patient care, weaker bereavement care, and exhibit a higher percentage of patients discharged before death than nonprofits (Appelbaum et al. Reference Appelbaum, Batt and Curchin2023). It shouldn’t be a surprise that quality degrades when more attention is given to obtain reimbursement than supply quality care to enrollees.
One implication of these findings for providers is that emotional and bereavement support should be offered from the first day of hospice admission since anticipatory grief is already experienced by the patient and loved ones as hospice admission is deliberated. In addition, we noticed that the word support appeared often related to this topic. Family members seemed to expect firm support from the hospice. Spiritual, emotional care and treating patient with respect were the highest CAHPS scores in all sourced CAHPS studies in an extensive literature search (Davlyatov et al. Reference Davlyatov, He and Orewa2023; Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b, Reference Hotchkiss, Ridderman and Hotchkiss2023c; Parast et al. Reference Parast, Haas and Tolpadi2018b; Price et al. Reference Price, Parast and Elliott2023, Reference Price, Stucky and Parast2018, Reference Price, Tolpadi and Schlang2020; Quigley et al. Reference Quigley, Parast and Haas2020).
For the former, the reason for this is that the bar of supportive psychosocial–spiritual care is set low for each of the three questions on emotional, spiritual, and post-death bereavement support, with only three options: “too little, right amount, too much.” Mental health leaders have long been calling for and pleading to establish parity for mental healthcare – that mental healthcare receives the same resources as physical healthcare. We are making the same appeal in the realm of end-of-life care. A caregiver beside herself with grief in the middle of the night is a severity 1 crisis as much as shortness of breath is an emergency. Why does the physical body garner many resources, yet mental health so little? These kind of assessments can indirectly minimize the role of social workers, counseling, and spiritual care (Cabin Reference Cabin2023), which should be lifted up as high values given the emotional and spiritually taxing nature of death and dying. According to caregiver values, we need the same questions and scales as the bodily measures of care.
Seen from a more pragmatic, business-minded perspective, the CAHPS survey is going to caregivers. Providing good overall support, especially emotional and spiritual support for caregivers, is a good business decision. How much support for your religious and spiritual beliefs did you get from the hospice team? Should be changed to: How often did you receive support for your religious and spiritual beliefs? (Never, Sometimes, Usually, Always). We make the same recommendations for the single items for both emotional and bereavement support in the CAHPS. This sets the bar for psychosocial–spiritual care at the same level as the other items in the CAHPS assessment and also acknowledges the high value (third most prevalent topic) caregivers place on spiritual, emotional, and bereavement care.
Hospices do well to remember to care for the whole family unit, especially since the primary caregiver will speak for the patient and all loved ones in their review of hospice in the CAHPS survey process. The two most notable responses to excellent care, including emotional and spiritual support, were gratitude and recommending hospices.
CAHPS survey results paint a rosier picture of support in hospice than online reviews
CAHPS survey results paint a much rosier picture of support in hospice than online reviews. Emotional–spiritual support and respect for patients is a low bar that should be raised to provide compassionate care to all enrollees, including patients. We found that spiritual, emotional care and treating patient with respect were the highest CAHPS scores in all sourced CAHPS studies in an extensive literature search (Davlyatov et al. Reference Davlyatov, He and Orewa2023; Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023b, Reference Hotchkiss, Ridderman and Hotchkiss2023c; Parast et al. Reference Parast, Haas and Tolpadi2018b; Price et al. Reference Price, Parast and Elliott2023, Reference Price, Stucky and Parast2018, Reference Price, Tolpadi and Schlang2020; Quigley et al. Reference Quigley, Parast and Haas2020). CAHPS Treating patient with respect and Emotional, spiritual support appears to suffer from ceiling effects since these scores are high even when other CAHPS measures are very low. The bottom 10 in CAHPS quality are an excellent example of this. The variance was minimal in this study of Big Hospices and is congruent with other findings (Davlyatov et al. Reference Davlyatov, He and Orewa2023; Parast et al. Reference Parast, Haas and Tolpadi2018b; Price et al. Reference Price, Parast and Elliott2023, Reference Price, Stucky and Parast2018, Reference Price, Tolpadi and Schlang2020; Quigley et al. Reference Quigley, Parast and Haas2020). Caregivers need more choices than the “right amount,” since the topic of support, in general, was very common among reviewers (>40%) (Hotchkiss et al. Reference Hotchkiss, Ridderman and Buftin2023a).
Two CAHPS measures have a low bar and cannot effectively differentiate between low and high performers. We also suspected that the narrow range of CAHPS Emotional, spiritual support and Treating patient with respect might reflect the aging survey methods – phone and mail. For-profits had significantly higher overall Emotional Intensity than nonprofit hospices, again with strong effect; caregivers were angry at for-profits. Online reviews, which permit more open-ended feedback, foster a more genuine, nuanced, and substantive sharing of concerning hospice experiences. Online reviews tend to attract caregivers with high praise or some degree of critique, and the open-ended review format allows them to elucidate why. Conversely, the CAHPS survey attracts caregivers with more positive hospice reviews, and the absence of an opportunity to express their thoughts in a narrative form motivates some caregivers with negative experiences to post online.
Limitations and future research
A significant strength of this study is the comprehensive analysis of 4,279 caregiver reviews, providing a deep insight into hospice care sentiments. The time context of the CAHPS scores and online reviews were in agreement, as evidenced by 96% of online reviews falling between 2015 and 2023 – the time context of the CAHPS data gathering. We meticulously categorized hospices by topical Caregiver Sentiments, profit status, and CAHPS performance to discern the implications of profiteering in end-of-life care. Yet, with an average of 87 reviews per hospice and a focus on only 50 hospices (representing 32% of the total market share), the findings might only partially represent the broader hospice industry.
It’s important to note that reviewers on platforms like Google and Yelp voluntarily post their experiences, which could introduce a selection bias. The frequent acquisitions and subsequent name changes in the hospice sector posed a challenge. To enhance accuracy, we matched each review’s physical hospice address with the CMS-provided CAHPS dataset from 2019 to 2020. Still, unaccounted variables need to be accounted for, such as older reviews corresponding to hospices that have since changed ownership and potentially differing scores.
While CMS regards the Hospice CAHPS survey results as definitive quality indicators, potentially influencing reimbursement rates, the CAHPS survey has shortcomings. Notably, its reliance on mail and phone survey techniques may not resonate with younger caregivers’ preferred communication methods, leading to potential oversights of this demographic not being captured in the CAHPS process (Parast et al. Reference Parast, Elliott and Hambarsoomian2018a; Parast et al. Reference Parast, Haas and Tolpadi2018b). “Caregivers who were the decedent’s parent or spouse or partner were more likely to respond to the survey than caregivers who were the decedent’s child” (Parast et al. Reference Parast, Haas and Tolpadi2018b). With the current move afoot to value mental healthcare equally to physical healthcare, parity for mental health, emotional, spiritual, and bereavement, at end of life is a vital research topic. Future research could also investigate the caregiver experience regarding promises and marketing before admission.
In sum, caregivers lauded caring and compassionate professionals regardless of profit status. Yet, sadly, anger was expressed toward large, for-profits more fixated on numbers than emotional, spiritual, and bereavement support. Caregivers felt nonprofits provided much better emotional, spiritual, and bereavement support than for-profits. CAHPS items for Treating patient with respect and Emotional, spiritual support offer limited discriminating value since otherwise low CAHPS performers still have high scores on these measures but deficient scores on the other CAHPS scores. Online reviews on the same topic provide a more substantive and realistic appraisal. For example, not sending staff when requested was associated with the most mentions of disrespect. A higher bar than mere respect is needed to assess human caring. Compassion would be a highly relevant addition to CAHPS, since caring and compassionate staff was the second most prevalent review topic. Decedent caregivers made caring staff, emotional, and spiritual support chief indicators of hospice quality in their reviews. This fits with the Medicare-sponsored hospice benefit, which views the “unit of care” as the patient, their family, or other loved ones (Barry et al. Reference Barry, Carlson and Thompson2012; CMS 2021).
Data availability statement
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We wish to acknowledge RAND researchers, overseeing the CAHPS process, who seek healthcare equity in their assessment of hospice quality.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests
The author declares no competing interest.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Cornerstone University on August 20, 2022.








