


The social environment plays a crucial role in child development. Parents are the first key figures in children's lives. Later, parental influences remain substantial, but become intertwined with peer influences. Drawn from different theoretical frameworks (e.g. attachment theory, social dynamics and social network theory), these social relations are believed to shape children's emotional and behavioural development through mechanisms including social support, social influence, social engagement and attachment, and access to resources (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000; Smith and Christakis, Reference Smith and Christakis2008). For example, attachment theory postulates that having secure attachments provides a safe basis, a sense of security and self-esteem, which are regarded to be fundamental for healthy emotional development (Bowlby, Reference Bowlby1973). Indeed, adolescents attaining good quality relationships with parents and friends tend to be generally better adjusted than those with lower quality relations (e.g. Umberson et al., Reference Umberson, Crosnoe and Reczek2010). Early social contexts are also predictive of future adult adjustment. Longitudinal studies have shown that family experiences in adolescence predict multiple facets of functioning in adulthood, including physical and mental health, wellbeing and academic achievement (e.g. Korkeila et al., Reference Korkeila, Kivela, Suominen, Vahtera, Kivimaki, Sundell, Helenius and Koskenvuo2004; Paradis et al., Reference Paradis, Reinherz, Giaconia, Beardslee, Ward and Fitzmaurice2009; Huppert et al., Reference Huppert, Abbott, Ploubidis, Richards and Kuh2010; Harding et al., Reference Harding, Read, Molaodi, Cassidy, Maynard, Lenguerrand, Astell-Burt, Teyhan, Whitrow and Enayat2015). Similar findings have been reported for peer relations, which have been linked to mental health, overall disease risk, (un)employment and academic achievement in adulthood (e.g. Gest et al., Reference Gest, Sesma, Masten and Tellegen2006; Almquist and Brännström, Reference Almquist and Brännström2014; Sakyi et al., Reference Sakyi, Surkan, Fombonne, Chollet and Melchior2015).
Experiences from different social contexts do not act in isolation; ecological and social systems theories (Bronfenbrenner, Reference Bronfenbrenner1979; Hartup, Reference Hartup1989) posit that family and peer environments are interconnected systems, with influences of one system interacting with the other. For example, in line with the ‘dual-hit’ hypothesis, risk effects may be especially salient when negative experiences are present in both family and peer contexts, compared with problems in only one domain (Hazel et al., Reference Hazel, Oppenheimer, Technow, Young and Hankin2014). Alternatively, the stress-buffering model (Cohen and Wills, Reference Cohen and Wills1985; Rutter, Reference Rutter1985) suggests that supportive social environments can buffer stressful experiences or risk factors, such as problematic family or peer relations.
Prior research has shown that family and peer relations can both attenuate and exacerbate each other's effects (Gauze et al., Reference Gauze, Bukowski, Aquan-Assee and Sippola1996; Lansford et al., Reference Lansford, Criss, Pettit, Dodge and Bates2003; Gaertner et al., Reference Gaertner, Fite and Colder2010; Sentse et al., Reference Sentse, Lindenberg, Omvlee, Ormel and Veenstra2010; Véronneau and Dishion, Reference Véronneau and Dishion2010; Trudeau et al., Reference Trudeau, Mason, Randall, Spoth and Ralston2012). However, studies focusing on the effects of adolescent family and peer interplay into adulthood are scarce (see for exceptions Morojele and Brook, Reference Morojele and Brook2001; Pesola et al., Reference Pesola, Shelton, Heron, Munafò, Hickman and van den Bree2015), leaving it unclear whether and how such cross-context interactions may influence each other's effects in the long run. In addition, previous studies investigating cross-context interactions have often focused on certain aspects of social relations measured once or twice within a narrow developmental timeframe. Yet, the relative contribution of family and peer effects may change across adolescence, when the perception of parents as a primary source of support shifts to that of peers (Furman and Buhrmester, Reference Furman and Buhrmester1992). It is therefore highly relevant and informative to assess the effects of these experiences during multiple time points. Moreover, most research on social influences conducted so far has focused on either positive or negative functional outcomes, and often only on specific aspects thereof. This does not capture the complex and multidimensional nature of human functioning. In studies focusing on psychopathology, the absence of mental health problems is often considered as a positive outcome. However, health is more than the absence of disease or illness, rather it is ‘a state of complete physical, mental and social wellbeing’ (World Health Organization, 2006). Similarly, low positive functioning or wellbeing does not imply the presence of a mental disorder. Hence, assessing one aspect of functioning, such as mental health, does not necessarily give insight into functioning in other domains and, ideally, outcome measures should capture both positive and negative dimensions of several domains of functioning in order to gain insight into an individual's overall functional state (e.g. Westerhof and Keyes, Reference Westerhof and Keyes2010).
This study investigated which family and peer relations during early and middle adolescence (ages 11 and 16) predicted young adult functioning (age 22) in a prospective cohort study of Dutch adolescents. We expanded upon prior research by (a) not only considering long-term main effects, but also the interplay between family and peer environments, (b) including a comprehensive assessment of family and peer relations during two time points in adolescence, (c) adopting a multidimensional approach on functioning – encompassing subjective wellbeing, physical and mental health and socio-academic functioning – and (d) moving beyond a ‘not bad or just OK’ approach by including both positive and negative sides of health and functioning. To our knowledge, this is one of the first studies to focus on the long-term effects of cross-context interactions on multidimensional functioning in young adulthood.
Method
Participants and procedure
Participants were selected from the Dutch prospective cohort study TRAILS (TRacking Adolescents’ Individual Lives Survey), which involves bi- or triennial follow-up measurements. Detailed descriptions of TRAILS can be found in previous reports (Ormel et al., Reference Ormel, Oldehinkel, Sijtsema, van Oort, Raven, Veenstra, Vollebergh and Verhulst2012; Oldehinkel et al., Reference Oldehinkel, Rosmalen, Buitelaar, Hoek, Ormel, Raven, Reijneveld, Veenstra, Verhulst, Vollebergh and Hartman2015). Adolescents were recruited from five municipalities in the north of the Netherlands, including both urban and rural areas. Six assessment waves have been completed to date. The present study focused on the first (T1; 2001–2002), third (T3; 2005–2007) and fifth (T5; 2012–2013) wave. A total of 2230 adolescents enrolled at T1 (response rate 76%, mean age 11.1 years, 51% female). The response rates at T3 and T5 were, respectively, 81% (n = 1816, mean age 16.3, 52% female) and 80% (n = 1778, mean age 22.3, 53% female). The study was approved by the Dutch Central Committee on Research Involving Human Subjects (CCMO). Participants were treated in accordance with APA ethical standards and the Declaration of Helsinki, and all measurements were carried out with their adequate understanding and written consent.
Measures
Below, a brief description of the included measures is given, while more detailed information, including references for their validation, is provided in the online Supplementary material. An overview of the measures used in this study including information on informant, number of items and internal consistency, can be found in Table 1 (the scale scores represent the mean item score).
Table 1. Descriptive statistics of study variables
A, adolescent; P, parent.
a Strongly agree–strongly disagree.
b Never–(almost) always/very often.
c Reliability questionnaire about father/mother.
d Bad–good.
e Very unhappy–very happy.
f Very unsatisfied–very satisfied.
g Not true–very or often true.
h Primary–university.
i No occupation–full-time occupation.
j Reliability adolescent/parent report.
Family functioning and parenting (T1 and T3)
Family dysfunction was assessed at T1 and T3 using the general functioning scale of the McMaster Family Assessment Device (FAD; Epstein et al., Reference Epstein, Baldwin and Bishop1983). Parenting at T1 was measured using a short version of the Egna Minnen Beträffande Uppfostran (My Memories of Upbringing) for Children (EMBU-C) (Markus et al., Reference Markus, Lindhout, Boer, Hoogendijk and Arrindell2003). The participants reported on perceived warmth, overprotection and rejection. As answers for both parents were highly correlated (r = 0.67–0.81), these were combined to mean scores.
At T3, adolescents rated parental control (based on Stattin and Kerr, Reference Stattin and Kerr2000) and parental reactions to youth wrongdoing for both parents (based on Tilton-Weaver et al., Reference Tilton-Weaver, Kerr, Pakalniskeine, Tokic, Salihovic and Stattin2010; see online Supplementary Table S1, for included items). Parental reactions consisted of the subscales angry outbursts, guilt inducing and problem-solving reactions. Measures of both parents were highly correlated (r = 0.63–0.74) and therefore combined into one mean score.
Peer status, affection and relationship quality (T1 and T3)
Perceived peer status and affection at T1 were assessed using the Social Production Functions Questionnaire (SPF; Ormel et al., Reference Ormel, Lindenberg, Steverink and Vonkorff1997).
At T3, the relationship quality with peers was measured using a friendship-network interview conducted by trained researchers (based on Poulin and Pedersen, Reference Poulin and Pedersen2007). Adolescents could nominate up to seven friends, and reported on emotional support, practical help and fights for each friend (see online Supplementary Table S2).
Multidimensional functioning (T5)
Indicators for overall young adult functioning included measures assessing positive and negative functioning using existing questionnaires and questionnaires developed by TRAILS.
Positive functioning. Physical health and general happiness were reported in questionnaires developed by TRAILS. Satisfaction was assessed with a question on general life satisfaction combined with questions regarding work (Copenhagen Psychosocial Questionnaire [COPSOQ]; Kristensen et al., Reference Kristensen, Hannerz, Høgh and Borg2005) and/or romantic relationship satisfaction (Investment Model Scale [IMS]; Rusbult et al., Reference Rusbult, John and Agnew1998) if applicable. Positive affect was measured using the Positive and Negative Affect Schedule (PANAS) (Watson et al., Reference Watson, Clark and Tellegen1988; MacKinnon et al., Reference MacKinnon, Jorm, Christensen, Korten and Jacomb1999). Items from the Adult Behaviour Checklist (ABCL; Achenbach and Rescorla, Reference Achenbach and Rescorla2003) personal strengths subscale were used for positive social functioning and personal achievement. Educational attainment was measured with two questions on the highest diploma obtained or on the current educational level if still at school (Veldman et al., Reference Veldman, Bültmann, Stewart, Ormel, Verhulst and Reijneveld2014). Finally, daily occupation assessed whether participants were currently working and/or studying full-time (3), part-time (2), or had no occupation (1).
Negative functioning. Negative affect was assessed with the PANAS (Watson et al., Reference Watson, Clark and Tellegen1988; MacKinnon et al., Reference MacKinnon, Jorm, Christensen, Korten and Jacomb1999). The Adult Self Report (ASR) and ABCL were used to assess mental health problems (Achenbach and Rescorla, Reference Achenbach and Rescorla2003). For affective problems, the mean scores of the depressive and anxiety problems of the Diagnostic and Statistical Manual 4th edition (DSM-IV) subscales (ASR and ABCL) were combined. Finally, the DSM-IV subscales attention (deficit hyperactivity) problems, antisocial personality problems and avoidant personality problems were included.
Covariates
Socio-economic status (SES) was determined by parental educational and occupational levels and family income at T1. Parental educational level was summarized in five categories. Occupational level was based on the International Standard Classification of Occupations (Ganzeboom and Treiman, Reference Ganzeboom and Treiman1996). Low family income was defined as a monthly net family income of less than €1135 per month, which approximately amounts to a welfare payment. Based on parental reports on their marital status, we included whether participants lived in a one-parent or two-parent household at T1. Finally, mental health at T1 was assessed using the mean total problems scores of the Child Behaviour Checklist (CBCL) and Youth Self Report (YSR) (Achenbach and Rescorla, Reference Achenbach and Rescorla2001).
Statistical analysis
First, confirmatory factor analysis was performed to assess the measurement model fit of young adult functioning. Two first-order latent variables were created for positive and negative functioning, which together formed the second-order variable of overall multidimensional functioning at T5. In order to accomplish model identification with two indicators of multidimensional functioning, the factor loadings for positive and negative functioning were constrained to be equal in strength, after reversing the scores for negative functioning, such that a higher score indicated less negative functioning. We allowed for correlated residuals between observed variables measured by the same instrument.
Next, structural equation models (SEM) were used to examine which social experiences during adolescence predicted later functioning. Measures of the social environment (i.e. general family functioning, perceived parenting, peer status and peer relationship quality) at ages 11 (T1) and 16 (T3) were included as potential predictors of functioning at age 22 (T5). In addition to main effects, the model included cross-sectional and longitudinal interactions between the family and peer environments to investigate potential exacerbating or attenuating effects on later functioning. Note that ideally the same measures of family and peer experiences should be included for comparing T1 and T3 effects. In our study, this was only possible for family functioning. Separate analyses were carried out for overall multidimensional functioning (model 1; Fig. 1a) and for positive and negative functioning (model 2; Fig. 1b) in order to compare whether effects found in overall functioning were also present for positive or negative functioning. More parsimonious models were derived with manual backward selection by excluding the least significant main or interaction effect considering all coefficients until reaching p < 0.05 for all included effects (with exception of non-significant main effects corresponding to significant interaction effects).
Fig. 1. Schematic overview of the structural equation models assessing effects of the social environment on the second-order latent variable multidimensional functioning (a) and the two first-order latent variables positive and negative functioning (b). For ease of interpretation, cross-sectional and longitudinal interaction effects between family and peer environments were omitted.
Model estimation was based on maximum likelihood estimation with robust standard errors (MLR) in Mplus version 7.31 (Muthén and Muthén, Reference Muthén and Muthén2015). MLR is capable of handling missing data as well as skewed distributions of outcome variables, issues both present in our data. MLR only excludes participants with missing data on all variables (n = 2), thus the sample size for the final models was n = 2228. Model fit was examined by the following criteria: the root mean square error of approximation (RMSEA), the comparative fit index (CFI) and the standardized root mean residual (SRMR). A fit is considered acceptable to good when the model achieves >0.90 on the CFI, <0.10 on RMSEA and <0.09 on SRMR (Hu and Bentler, Reference Hu and Bentler1999).
Considering the large number of tests performed, we applied a correction for multiple testing based on the effective number of independent tests (M eff) (Li and Ji, Reference Li and Ji2005). The M eff was calculated separately for the number of outcome and predictor variables present in the full models using the eigenvalues of the corresponding correlation matrices (see online Supplementary Tables S3 and S4 for more information). This resulted in a total number of 75 tests (1.47 × 51 = 74.97) and a corresponding p value threshold of 0.05/75 = 0.00066. To avoid being overly conservative, we discuss both robustly (i.e. those effects surviving multiple testing correction: p < 0.00066) and nominally (p < 0.05) significant results. The latter should be interpreted with particular caution as replication is necessary. Significant interaction effects were probed using the Johnson–Neyman procedure (Johnson and Fay, Reference Johnson and Fay1950). This procedure allows us to model interactions between two continuous variables using regions of significance, thereby showing at which levels of a variable the effect of the other variable is significant.
Sensitivity analyses
Differences in sex, SES and family structure have been associated with both social environments and functioning (e.g. Rose and Rudolph, Reference Rose and Rudolph2006; Bramlett and Blumberg, Reference Bramlett and Blumberg2007; Almquist et al., Reference Almquist, Modin and Östberg2010), and may therefore act as potential confounders. In addition, the association between social factors and functioning can be bidirectional, that is, early mental health problems may give rise to problems with family and peers as well (Meeus, Reference Meeus2016). Therefore, following our main analyses, we tested whether robustly and nominally significant effects remained present while controlling for sex, SES, number of parents and mental health at age 11, and tested for potential sex moderation effects.
Results
Bivariate correlations and a graphical overview of the final SEM models including factor scores for multidimensional and positive or negative functioning are presented in the online Supplementary material (Table S5 and Figs S1 and S2). The confirmatory factor analysis of functioning measures showed that the measurement model provided a good fit to the data (χ2 401.91; RMSEA 0.07; CFI 0.94; SRMR 0.06). All factor loadings were significant (p < 0.001) and ranged between 0.19 and 0.76 for positive functioning and 0.53 and 0.90 for negative functioning. Factor loadings for multidimensional functioning were estimated as 0.91 for both positive and negative functioning.
Multidimensional functioning
Table 2 shows the standardized regression coefficients of the final SEM models. Together, adolescent family and peer experiences explained 12–15% of the variance in functioning at age 22. Multidimensional functioning was robustly predicted by T1 parental overprotection and T3 parental anger. Nominally significant associations were found with T1 family dysfunction, T1 parental warmth and T3 parental guilt inducing. Two interaction effects were found in which peer effects depended on family experiences. First, the effect of T3 peer fighting depended on T3 parental control; only when parental control was low did peer fighting significantly predict worse functioning (z-score <−0.06). This negative effect became stronger as parental control decreased (see Fig. 2a). Second, the positive effect of T1 peer status depended on T3 family dysfunction, and was only significant when family dysfunction was low (Fig. 2b). Here, peer status was a stronger predictor for later functioning when family dysfunction decreased. Note that these interactions were nominally significant; none survived correction for multiple testing.

Fig. 2. Johnson–Neyman plots showing (a) the conditional effect of T3 peer fighting for T3 parental control and (b) of T1 peer status for T3 family dysfunction on young adult multidimensional functioning. The non-shaded area indicates regions-of-significance.
Table 2. Results of structural equation models predicting young adult functioning
Structural equation models are based on maximum likelihood with robust standard error estimation (MLR), sample size n = 2228. For ease of interpretation, scores for negative functioning were reversed back such that a higher score indicates more negative functioning. Significant effects surviving the correction for multiple testing (p < 0.00066) are shown in bold.
Positive and negative functioning
Family and peer effects on positive and negative functioning showed both general and specific effects. The effect of T3 parental guilt inducing was found on both positive and negative functioning. The direct effects of T1 parental warmth, T1 parental overprotection and T3 family dysfunction appeared to be specific for positive functioning, whereas the effects of T1 family dysfunction and T3 parental anger were found for negative functioning only. In addition, positive functioning was nominally significantly predicted by parental problem solving, which did not have an effect on either multidimensional or negative functioning.
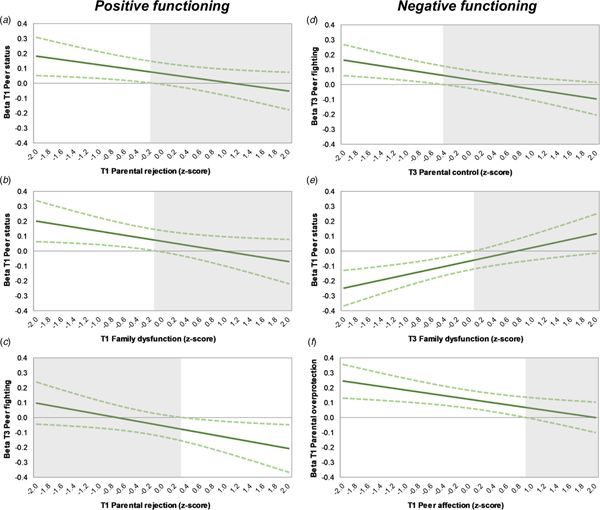
Associations were also found with T1 family dysfunction for positive functioning, and T1 overprotection and T3 family dysfunction for negative functioning, however these interacted with peer experiences. For negative functioning, two interactions similar to those found for multidimensional function were present (Figs 3d and 3e). In addition, negative functioning was predicted by an interaction effect between T1 peer affection and T1 parental overprotection; the negative effect of parental overprotection attenuated as peer affection increased and was no longer significant at high levels of peer affection (Fig. 3f). For positive functioning, three interactions were significant. Peer status predicted functioning only when T1 parental rejection or T1 family dysfunction was low (Figs 3a and 3b); and T3 peer fighting predicted poor functioning only when parental rejection was high (Fig. 3c). Here too interactions were found to be nominally significant at the most.
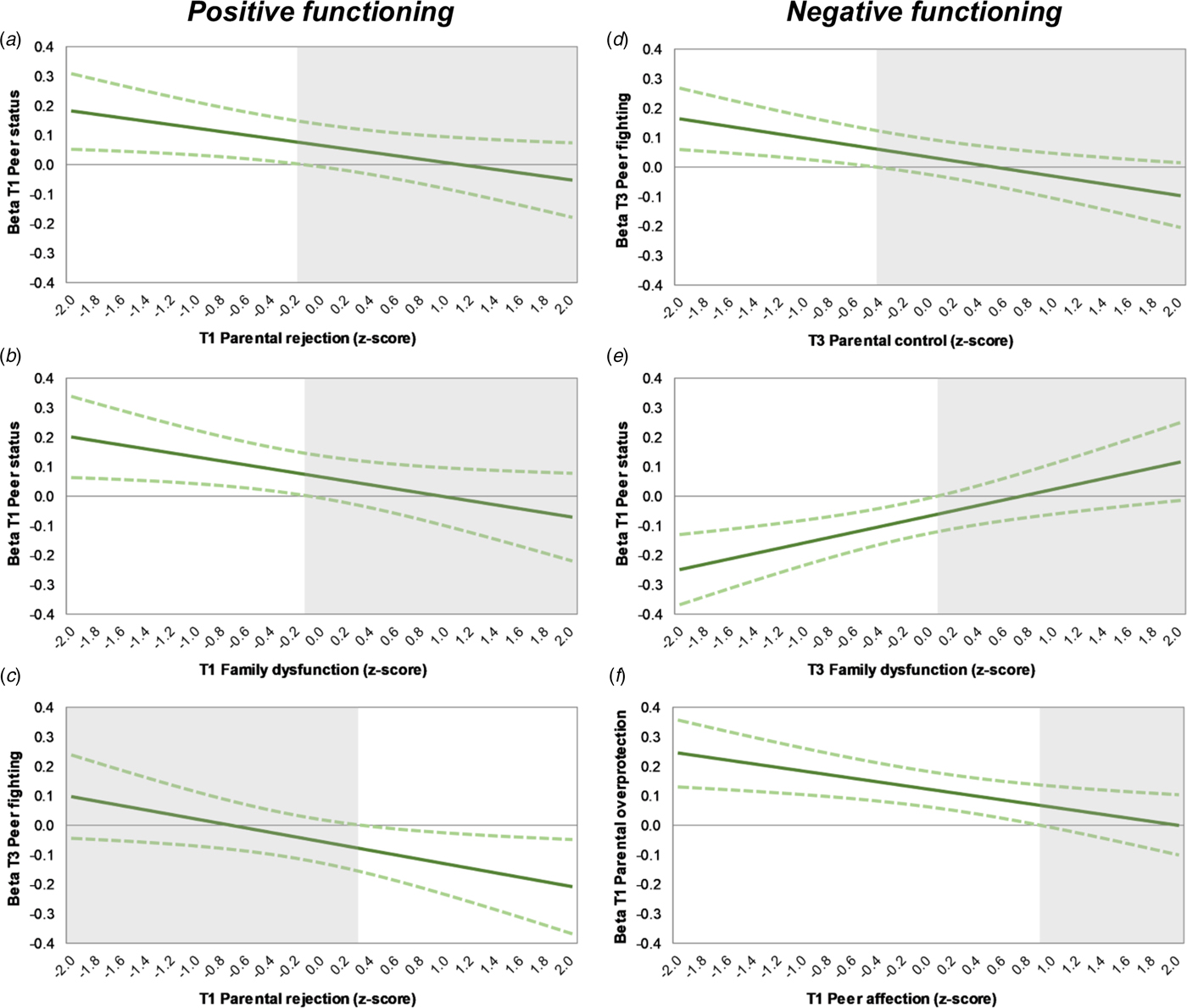
Fig. 3. Johnson–Neyman plots showing (a) the conditional effect of T1 peer status for T1 parental rejection, (b) of T1 peer status for T1 family dysfunction, and (c) of T3 peer fighting for T1 parental rejection on young adult positive functioning, and (d) the conditional effect of T3 peer fighting for T3 parental control, (e) of T1 peer status for T3 family dysfunction, and (f) of T1 parental overprotection for T1 peer affection on young adult negative functioning (c). The non-shaded areas indicate regions-of-significance. For ease of interpretation, scores for negative functioning were reversed back such that a higher score indicates more negative functioning.
Sensitivity analyses
Most effects remained equal in strength, as well as statistically significant when controlling for sex, SES or number of parents in the final models, although a few dropped to non-significance (see Supplementary Tables S6–S8). In contrast, controlling for T1 mental health problems generally reduced the number of significant effects. Nearly all T1 effects became non-significant, with the exception of parental warmth for positive functioning. Additionally, for T3, the effects of family dysfunction on positive functioning and the interaction family dysfunction × T1 peer status on multidimensional functioning became non-significant (p > 0.07). Similar results were found when simultaneously controlling for all potential confounders. Finally, no sex moderation effects survived the correction for multiple testing.
Discussion
This study examined to which extent family and peer experiences during adolescence jointly predict wellbeing and functioning in young adulthood. The results showed that 12–15% of the variance in functioning at age 22 was explained by adolescent family and peer experiences, of which family relations during early and mid-adolescence (ages 11 and 16) were most predictive. Young adolescents reporting less negative family experiences overall demonstrated better adjustment in young adulthood. Peer experiences did not independently predict functioning. Furthermore, certain family and peer experiences appeared interdependent in their prediction of later functioning.
Parental overprotection and negative parental reactions robustly predicted future functioning, which is in line with previous research (e.g. Huppert et al., Reference Huppert, Abbott, Ploubidis, Richards and Kuh2010; Tilton-Weaver et al., Reference Tilton-Weaver, Kerr, Pakalniskeine, Tokic, Salihovic and Stattin2010; Baker and Hoerger, Reference Baker and Hoerger2012). Parental overprotection is thought to limit a child's opportunity to independently explore the world and to develop healthy self-regulating and coping strategies (Thomasgard and Metz, Reference Thomasgard and Metz1993). Similarly, negative parental reactions to misbehaviour, such as anger, are thought to increase feelings of being restricted and decrease feelings of connectedness (Tilton-Weaver et al., Reference Tilton-Weaver, Kerr, Pakalniskeine, Tokic, Salihovic and Stattin2010). Our findings are in agreement with the McMaster model of family functioning, which considers affective responsiveness and involvement as core functions of families; with inappropriate responses and involvement viewed as detrimental for a child's development (Epstein et al., Reference Epstein, Bishop and Levin1978).
In line with ecological and social systems theories, we found that the effects of peer contexts can depend on the family context and vice versa (Bronfenbrenner, Reference Bronfenbrenner1979; Hartup, Reference Hartup1989). For example, the negative effect of peer fighting was absent in case of high parental control or low parental rejection. In addition, the negative effect of parental overprotection was no longer significant at high levels of peer affection. This suggests both family and peer contexts may function as ‘buffers’, in line with previous studies on adolescent functioning (Gauze et al., Reference Gauze, Bukowski, Aquan-Assee and Sippola1996; Lansford et al., Reference Lansford, Criss, Pettit, Dodge and Bates2003; Gaertner et al., Reference Gaertner, Fite and Colder2010; Sentse et al., Reference Sentse, Lindenberg, Omvlee, Ormel and Veenstra2010; Véronneau and Dishion, Reference Véronneau and Dishion2010; Trudeau et al., Reference Trudeau, Mason, Randall, Spoth and Ralston2012). According to the stress-buffering model, supportive social contexts – such as positive parenting characterized by low levels of rejection – can protect against the adverse effects of stressful events by attenuating the appraisal of stress. That is, the observation that others are willing to invest in a person may help to decrease the experience of stress (Cohen and Wills, Reference Cohen and Wills1985). Note that these effects can also be interpreted as reflecting a dual-hit pattern, in which negative family or peer effects are particularly relevant when experiences in the other context are negative as well. This is line with the idea that the same variable can act both as buffer and risk factor, depending on what ‘side of the coin’ is focused on (Lösel and Farrington, Reference Lösel and Farrington2012).
Finally, we found that the positive effect of peer status was only present in the absence of negative family experiences, including low parental rejection and family dysfunction. As such the positive effect of peer status does not appear to be able to compete with negative family experiences. Together these findings suggest that family and peer experiences can interact in different ways. Risk factors in one context can be exacerbated by negative experiences or buffered by positive experiences in the other context, and protective factors in one context can be overshadowed by negative experiences in the other context. Furthermore, interactions between parent and peer contexts appear to be circumscribed, that is, holding for some aspects of family and peer experiences, but not for others. As none of the interaction effects survived the correction for multiple testing, future studies are necessary to investigate the robustness of these findings.
When comparing the relative contribution of family and peers on future functioning, we primarily found family effects. That is, when taking both contexts into account, the type of peer relations we measured at ages 11 and 16 did not seem incremental to the predictive ability of family experiences for young adult functioning. As such, our findings suggest that adolescent family experiences may be more important for future functioning than adolescent peer relations. So far, little research has considered adolescent family and peer relations in one model when predicting (young) adult adjustment. Moreover, studies that have done so often included other aspects of social relations than studied here, such as deviant peer behaviours or romantic relations, or focused specifically on substance abuse as outcome, making it difficult to compare results. For example, in line with our findings, two studies reported stronger family than peer effects for positive social relations and autonomy support (der Giessen et al., Reference Der Giessen, Branje and Meeus2014; Jones et al., Reference Jones, Hill, Epstein, Lee, Hawkins and Catalano2016). Seemingly inconsistent with our study is that Jones et al. (Reference Jones, Hill, Epstein, Lee, Hawkins and Catalano2016) reported particularly strong effects of peer drug abuse on future functioning. This suggests that the relative contributions of family and peer relations on future adjustment are likely to depend on the type of peer factors (e.g. peer relationship quality v. deviant peer behaviours).
In addition to the kind of peer factors involved, the relative importance of family and peer relations may also depend on developmental timing. Whereas some have argued that adolescence marks a shift from parents to peers as the primary source of support (Furman and Buhrmester, Reference Furman and Buhrmester1992), others have emphasized the continued importance of the family environment (Raja et al., Reference Raja, McGee and Stanton1992). In agreement with the latter, our findings stress the role of family experiences at both ages 11 and 16. Although the use of different measures over time prevents us from drawing firm conclusions. Possibly, the importance of peer relationship quality for adult functioning has shifted from adolescence towards young adulthood. In recent decades, the period of adolescence has lengthened, with a protracted transition into adulthood in terms of leaving the parental home and becoming financially independent (Steinberg, Reference Steinberg2014). It is plausible that peers matter most in this transition to independence and beyond. Indeed, studies have shown that the effects of adolescent peer relations are mediated by current (romantic) peer relations in young adulthood (Englund et al., Reference Englund, Kuo, Puig and Collins2011; Jones et al., Reference Jones, Hill, Epstein, Lee, Hawkins and Catalano2016). Overall, considering the scarcity of studies comparing the synergy of long-term family and peer effects, further research, also beyond the traditional end of adolescence, is warranted.
We looked whether the effects found for overall multidimensional functioning were also present for positive or negative functioning. Most effects appeared similar for both sides of functioning. However, effects of parental warmth and parental problem solving – the only two positively framed family experiences – seemed to be specific for positive functioning, while parental anger specifically predicted negative functioning. This might suggest that positive social experiences may be especially relevant for predicting young adult positive adjustment, while negative experiences are more relevant for negative functioning. Such a pattern of specificity is not unlikely considering that positively framed experiences and behaviours usually tend to be skewed to (i.e. contain more variance in) the positive side of the distribution, and negatively framed variables to the negative side. That said, positive functioning was also predicted by negative social experiences, thus negative experiences and behaviours do not merely predict negative outcomes. In all, our findings are in line with the idea that mental health problems and wellbeing can have both overlapping and distinctive correlates (e.g. Kinderman et al., Reference Kinderman, Tai, Pontin, Schwannauer, Jarman and Lisboa2015; Patalay and Fitzsimons, Reference Patalay and Fitzsimons2016), and suggests that targeting predictors of one domain shall not necessarily benefit the other.
Strengths and limitations
This study should be viewed in light of certain strengths and limitations. Strong points include the longitudinal prospective study design and multidimensional approach encompassing positive and negative functioning. Moreover, we extended previous literature by accounting for both family and peer factors, which were measured at two developmentally relevant time points in adolescence. Some limitations should be noted as well. First, although we included multiple informants when possible, most data were based on self-reported questionnaires. Observational measures of social experiences and adult functioning would have been a valuable addition. Nevertheless, it can be argued that the way a person perceives social relations is likely to be more important for one's development compared with actual, but unperceived social experiences (e.g. Laceulle et al., Reference Laceulle, Jeronimus, Aken and Ormel2015). Second, except for family dysfunction, different measures of the social environment were used in TRAILS at each time point. Consequently, we were unable to investigate whether specific aspects of social experiences, such as parental overprotection or peer popularity, have the same influence in early and mid-adolescence. Third, several factors may mediate the associations found between adolescent social experiences and later functioning which have not been investigated in the current study. Future research is needed to investigate such mediating factors in more detail.
Another issue that should be pointed out is that while our longitudinal design allows for temporal ordering, we cannot infer causality from the reported findings. It is certainly plausible that the adolescent social experiences studied here are a direct cause of later maladjustment; however, they can also be markers of true underlying causal factors of later functioning, such as genetic predisposition or prior maladjustment. To account for potential reverse causality, we performed sensitivity analyses with baseline mental health problems included in the model. Although correcting for functioning before age 11 would have been preferable, such measures were not available within our sample. The results showed that most effects during mid-adolescence were not the result of initial levels of functioning. However, most social experiences in early adolescence and the interplay between parental control and peer fighting no longer predicted future functioning. As such, here we cannot rule out the possibility that mental health at age 11 may have caused problems in adolescent family and peer relations. The sensitivity analyses further showed that overall differences in sex, SES or number of parents do not explain the found effects either. Further longitudinal research including multiple assessments of functioning over time is necessary to elucidate the potential mechanisms that play a role in the link between early social experiences and later functioning.
To conclude, the results indicate that both family and peer relations during adolescence can be predictive for young adult functioning, but that especially adolescent family experiences, such as parental overprotection and family dysfunction, are associated with young adult functioning. The findings further suggest that certain family and peer experiences are interdependent in their prediction of later functioning, which highlights the importance of considering the relative effects of one context in relation to the other. Nevertheless, despite a comprehensive assessment, adolescent family and peer experiences played a modest role in predicting young adult functioning. Thus, having negative family or peer experiences during adolescence does not necessarily mean one will function worse in young adulthood. At least, for adolescents growing up in fairly normal circumstances such as the participants included in this study from the TRAILS population cohort. That is, more extreme social experiences, especially at the adverse end, may have a greater predictive value for later functioning than the effects found here suggest. Future studies are necessary to further investigate whether the relative contribution and interdependence of families and peers holds true for other social experiences as well.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291718001976.
Acknowledgements
The authors are grateful to everyone who participated in the TRAILS study or worked on the project to make this study possible.
Financial support
This research is part of the TRacking Adolescents’ Individual Lives Survey (TRAILS). Participating centres of TRAILS include the University Medical Center and University of Groningen, the University of Utrecht, the Radboud Medical Center Nijmegen and the Parnassia Bavo group, all in the Netherlands. TRAILS has been financially supported by various grants from the Netherlands Organization for Scientific Research NWO (Medical Research Council program grant GB-MW 940-38-011; ZonMW Brainpower grant 100-001-004; ZonMw Risk Behavior and Dependence grant 60-60600-97-118; ZonMw Culture and Health grant 261-98-710; Social Sciences Council medium-sized investment grants GB-MaGW 480-01-006 and GB-MaGW 480-07-001; Social Sciences Council project grants GB-MaGW 452-04-314 and GB-MaGW 452-06-004; NWO large-sized investment grant 175.010.2003.005; NWO Longitudinal Survey and Panel Funding 481-08-013 and 481-11-001), the Dutch Ministry of Justice (WODC), the European Science Foundation (EuroSTRESS project FP-006), Biobanking and Biomolecular Resources Research Infrastructure BBMRI-NL (CP 32) and the participating universities.
Conflict of interest
Dr Verhulst is a contributing author of the Achenbach System of Empirically Based Assessment, from which he receives remuneration. All other authors report no financial interests or potential conflicts of interest.







 Open access
Open access