


Introduction
Childhood maltreatment is a major ethical, public health, human rights, legal and social problem (Butchart et al. Reference Brown, Cohen, Johnson and Smailes2006). It is estimated that 1 in 5 women and 1 in 13 of men worldwide have been sexually abused during childhood, while 25% of all adults report being physically abused (WHO, Reference Toth, Manly and Cicchetti2014).
Childhood maltreatment is a leading contributor to the development of depression and anxiety disorders among children and adults. It contributes to the emergence of psychopathology (McCrory et al. Reference Maniglio2010) through many neurobiological mechanisms: (1) stress systems (Cicchetti & Toth, Reference Chen, Murad, Paras, Colbenson, Sattler, Goranson, Elamin, Seime, Shinozaki, Prokop and Zirakzadeh2005); (2) structural brain differences (Herringa et al. Reference Danese, Moffitt, Harrington, Milne, Polanczyk, Pariante, Poulton and Caspi2013), e.g. hippocampus, amygdala, corpus callosum and other white-matter tracts, and prefrontal cortex; (3) functional brain differences, e.g. hyperactivity of amygdala in response to negative facial affect; and (4) genetics and epigenetics of resilience and vulnerability. Maltreatment in childhood is also a threat to the optimal development of affective processing abilities, attachment relationships, self-system processes, peer relationships, and adaptation to school (Cicchetti & Toth, Reference Chen, Murad, Paras, Colbenson, Sattler, Goranson, Elamin, Seime, Shinozaki, Prokop and Zirakzadeh2005).
Depression and anxiety disorders are the major causes of psychiatric morbidity worldwide. According to the global burden of disease report 2010, depressive disorders contributed most to the burden of mental illness and substance use disorders (42.5%) followed by anxiety disorders (15.3%) (Whiteford et al. Reference Stoltenborgh, IJzendoorn, Euser and Bakermans-Kranenburg2013). Depressive disorders also accounted for 40.5% of disability-adjusted life years caused by mental illnesses and substance use disorders, with anxiety disorders accounting for another 14.6%.
Previous studies of childhood maltreatment have shown its significant impact on mental and physical health outcomes. Child abuse, including physical abuse, sexual abuse, and exposure to intimate partner violence, has been associated with psychiatric disorders, including depression, bipolar disorder, generalized anxiety disorder, alcohol and drug abuse, suicidal ideation and attempts, etc. (Afifi et al. Reference Afifi, MacMillan, Boyle, Tailliew, Cheung and Sareen2014). Children from abusive families are significantly more likely to report depressive symptoms than those from non-abusive homes (Toth et al. Reference Scott, McLaughlin, Smith and Ellis1992).
Reviews have also consistently shown the negative immediate and long-term psychological effects of the childhood maltreatment. Maniglio (Reference Hardt and Rutter2010, Reference Herringa, Birn, Ruttle, Burghy, Stodola, Davidson and Essex2012) in systematic reviews of reviews found that child sexual abuse was a significant risk factor for both depression and anxiety disorders. Adults who report being abused as children exhibited more post-traumatic stress symptoms, cognitive distortion, emotional distress (including depression and anxiety disorders), eating disorders, sleep disorders, substance abuse, and avoidance (Briere & Elliott, Reference Briere and Elliott1994; Chen et al. Reference Butchart, Harvey and Furniss2010; Nanni et al. Reference Meng and D'Arcy2012).
Although previous reviews have shown a significant direct relationship between childhood maltreatment and depression and anxiety, they either reviewed cross-sectional studies or studies that did not have an externally documented history of child abuse. Abuse exposure has generally been measured via recall methods which is prone to bias and false memory (Robins et al. Reference Neumann, Houskamp and Pollock1985; Taylor & Brown, Reference Sareen, Belik, Afifi, Asmundson, Cox and Stein1988; Coughlin, Reference Colman, Kingsbury, Garad, Zeng, Naicker, Patten, Jones, Wild and Thompson1990; Maughan et al. Reference Higgins, Thompson, Deeks and Altman1995; Neumann et al. Reference Meng and D'Arcy1996; Hardt & Rutter, Reference Cutuli, Ranby, Cicchetti, Englund and Egeland2004). A substantial proportion of individuals known to have suffered abuse/maltreatment do not report such abuse when interviewed in adult life (Hardt & Rutter, Reference Cutuli, Ranby, Cicchetti, Englund and Egeland2004). Taylor & Brown (Reference Sareen, Belik, Afifi, Asmundson, Cox and Stein1988) indicated that mental health is associated with a filtering out of negative memories and/or re-representing them in non-threatening terms. People with good functioning in adult life are apt to forget early parental negativity whereas there is a tendency for people with poor functioning to retrospectively exaggerate negativity that was not reported contemporaneously during childhood (Robins et al. Reference Neumann, Houskamp and Pollock1985; Maughan et al. Reference Higgins, Thompson, Deeks and Altman1995). Similarly, Colman et al. (Reference Cicchetti and Toth2015) found significant inconsistencies in the reporting of adverse childhood events between two time points 12 years apart. Concurrent mental health factors were found to influence the reporting of traumatic childhood experiences. The authors strongly suggest that studies estimating the association between adverse childhood events and mental health need to look at the consistency of the reporting such events. Further, cross-sectional studies cannot identify the temporal relationship between risk factors and outcomes. Additionally, questions have been raised concerning the use of rating scales as opposed to diagnostic instruments to measure mental illness outcomes.
Little can be found with respect to the potential impact of reducing childhood abuse in decreasing the incidence of psychiatric disorders in a population. Population attributable fractions (PAFs) are used to indicate the proportional reduction in a population of a disease (incidence or mortality) that would occur if exposure to a risk factor were reduced to an alternative ideal exposure level (Rockhill et al. Reference Norman, Byambaa, De, Butchart, Scott and Vos1998). PAFs have been commonly recognized as effective tools measuring the potential effects of risk factors on psychiatric disorders (Sareen et al. Reference Northridge2008; Bolton & Robinson, Reference Bolton and Robinson2010; Barnes & Yaffe, Reference Barnes and Yaffe2011; Meng & D'Arcy, Reference Maniglio2013, Reference Maniglio2014). Northridge (Reference Moher, Liberati, Tetzlaff and Altman1995) believed that PAFs could help policy-makers in judging priorities for public health action, intervention planning and decision-making.
This study aims to: (1) systematically review the evidence for the association between childhood maltreatment and the later development of depression and anxiety using longitudinal cohort studies and studies with externally documented measures of childhood maltreatment and diagnostic measures of depression and/or anxiety; and (2) provide firm estimates of by how much the incidence of depression and anxiety in a population would be reduced if childhood maltreatment was reduced.
Method
This systematic review and meta-analysis was guided by the PRISMA guidelines, 2009 revision (Moher et al. Reference Maughan, Pickles, Quinton and McCord2009), and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) recommendations (Stroup et al. Reference Rockhill, Newman and Weinberg2000).
Inclusion and exclusion criteria
To be included in this review articles were evaluated for internal validity and the following inclusion and exclusion criteria: (1) be published in English within the last 25 years (1990–2014); (2) be a cohort study; (3) not using subject recall to assess childhood maltreatment; (4) give clear information on the assessment of adverse childhood experiences (e.g. types of abuse, years of age being abused, assessment and ascertainment tools, etc.); (5) use clear diagnosis criteria for depression or anxiety in adulthood, specifically DSM and its updates (APA, 2013), ICD-10 (WHO, Reference Stroup, Berlin, Morton, Ingram, Williamson, Rennie, Moher, Becker, Sipe and Thacker1992) or other generally accepted diagnostic criteria; (6) provide statistical indicators (e.g. relative risk) or original data to estimate the relationship between child abuse and depression/anxiety; (7) studies that measured childhood maltreatment via recall methods only or referrals without official documentary support (e.g. police records, records from social services, child protective services, and criminal court) were excluded.
Search strategy
We conducted computerized searches in the PubMed, PsycINFO, EMBASE, Medline, and Cochrane Library databases for the period from January 1990 to December 2014 for published articles. The search strategy is detailed in Supplementary Appendix 1. In addition, we manually searched other resources for other relevant studies. The reference lists of selected articles, review articles on relevant topics, and the grey literatures were also screened.
Data collection and quality assessment
The full-text article was retrieved for all studies that initially appeared to meet the inclusion criteria for further examination. Authors M.L. and X.M. independently assessed the articles for eligibility. Any disagreements among reviewers were resolved through discussion. Data on author, publication year, journal, sample size, methods, indicators, outcomes, comorbidities, adjustments, study design and results were extracted independently by the two authors. Newcastle–Ottawa Scale criteria were used to characterize study quality (Wells et al. Reference Stoltenborgh, Bakermans-Kranenburg, Alink and IJzendoorn2012). One author of a selected article was contacted for further information. One eligible study was excluded because of duplication.
Data synthesis
The reviewed articles were grouped for five analyses: (1) any maltreatment and depression; (2) any maltreatment and anxiety; (3) physical abuse and either depression or anxiety disorders; (4) sexual abuse and either depression or anxiety disorders; and (5) neglect and either depression or anxiety disorders. We report on each analysis separately. Studies were involved in multiple separate analyses as their available data permitted.
Statistical analyses
Meta-analysis
The analyses generated pooled estimates of the effects of childhood maltreatment in general and for specific types of abuse on depression and/or anxiety. We also evaluated heterogeneity with DerSimonian and Laird I 2 statistics for each category to determine the proportion of heterogeneity that is not due to chance (Higgins et al. Reference Egger, Davey, Schneider and Minder2003). Funnel plots and Egger's tests were used to inspect for publication bias (Egger et al. Reference Coughlin1997). Compared to funnel plot, Egger's test provides a more objective way to estimate the reliability of the results. If these tests show non-significant heterogeneity, we used fixed-effects model, whereas a more conservative random-effects model was used if we saw the possibility of heterogeneity. Sensitivity analysis assessed the influence of each individual study on overall estimates by recalculating odds ratios with each study being removed one at a time. The quality of each study was rated according to the Newcastle–Ottawa Scale, and meta-regression analyses were used to examine the impact of study quality on results. Stata v. 12, statistical software (StataCorp., USA) was used for the analyses.
Calculation of projected effects (PAFs)
PAF is the proportional reduction in average disease risk that would be achieved by elimination of an exposure of interest or its reduction to a specified level. It indicates that the proportion of people with a disease in a population that is potentially attributable to a given risk factor assuming that there is a causal relationship (Benichou, Reference Benichou2001). The PAF takes into account the strength of the association between the risk factor and the outcome as well as the prevalence of the risk factor. It was calculated by the following formula based on previous literature (Rockhill et al. Reference Norman, Byambaa, De, Butchart, Scott and Vos1998; Sareen et al. Reference Northridge2008; Barnes & Yaffe, Reference Barnes and Yaffe2011):
 $${\rm PAF} = \displaystyle{{\,p({\rm OR} - 1)} \over {\,p({\rm OR} - 1) + 1}},$$
$${\rm PAF} = \displaystyle{{\,p({\rm OR} - 1)} \over {\,p({\rm OR} - 1) + 1}},$$
where p is the population prevalence of the exposure, and OR is the pooled odds ratio of outcomes given different categories of childhood maltreatment. In the present study, worldwide PAFs were calculated for specific types of abuse. Present worldwide prevalence estimates were obtained from the most recent review of (Stoltenborgh et al. Reference Paolucci, Genuis and Violato2015). Both self-reported and informant prevalence estimates were used to generate self-reported and informant PAFs, respectively. Informant estimates are from studies collecting data from police records, social services, child protective services, child welfare workers, or teachers.
Finally, we estimated the total number of depression and/or anxiety cases attributable to different categories of childhood maltreatment by multiplying PAF estimates and the present number of cases worldwide. We also calculated the number of cases that could potentially have been prevented if the prevalence of exposure to childhood maltreatment were 10% or 25% lower than present levels. We also calculated confidence ranges for PAF estimates, number of attributable cases, and number of cases potentially prevented by using the 95% confidence intervals (CIs) from the pooled OR estimates.
Results
Meta-analysis
Selection of articles
Fig. 1 shows the process of study selection. The initial search produced 5340 titles, from which 392 abstracts were reviewed, subsequently 199 articles were retrieved for full evaluation. Eight articles met our inclusion and exclusion criteria (see Supplementary Appendix 2).
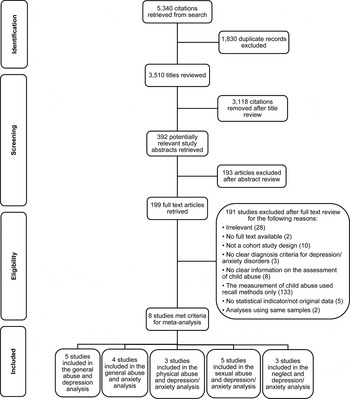
Fig. 1. PRISMA flow diagram – childhood maltreatment and later depression and/or anxiety.
Table 1 presents the detailed data on characteristics of the reviewed articles. The articles were assessed for quality using the Newcastle–Ottawa Quality Assessment Criteria as well as for the external ascertainment of childhood maltreatment exposure. All the included studies rated highly in terms of quality (see Supplementary Appendix 3). This quality is evident in the fact that none of the study characteristics examined had any impact on observed odds ratios in any of the analyses reported. Nor was there any publication bias observed.
Table 1. Summary of the studies’ attributes

VIFM, Victorian Institute of Forensic Medicine; CYF, Child, Youth and Family Agency; NYSCR, New York State Central Registry for Child Abuse and neglect; PTSD, Post-traumatic stress disorder; SCID, Structured Clinical Interview for DSM disorders; DSM, Diagnostic and Statistical Manual of Mental Disorders; WHO-ICD, WHO International Diagnostic Interview; DIS, National Institute of Mental Health Diagnostic Interview Schedule; CIDI, WHO Composite International Diagnostic Interview; DISC, National Institute of Mental Health Diagnostic Interview Schedule for Children.
Relationship between any maltreatment and depression
Five articles (Brown et al. Reference Vos, Flaxman, Naghavi, Lozano, Michaud, Ezzati, Shibuya, Salomon, Abdalla, Aboyans, Abraham, Ackerman, Aggarwal, Ahn, Ali, Alvarado, Anderson, Anderson, Andrews, Atkinson, Baddour, Bahalim, Barker-Collo, Barrero, Bartels, Basáñez, Baxter, Bell, Benjamin, Bennett, Bernabé, Bhalla, Bhandari, Bikbov, Bin Abdulhak, Birbeck, Black, Blencowe, Blore, Blyth, Bolliger, Bonaventure, Boufous, Bourne, Boussinesq, Braithwaite, Brayne, Bridgett, Brooker, Brooks, Brugha, Bryan-Hancock, Bucello, Buchbinder, Buckle, Budke, Burch, Burney, Burstein, Calabria, Campbell, Canter, Carabin, Carapetis, Carmona, Cella, Charlson, Chen, Cheng, Chou, Chugh, Coffeng, Colan, Colquhoun, Colson, Condon, Connor, Cooper, Corriere, Cortinovis, de Vaccaro, Couser, Cowie, Criqui, Cross, Dabhadkar, Dahiya, Dahodwala, Damsere-Derry, Danaei, Davis, De Leo, Degenhardt, Dellavalle, Delossantos, Denenberg, Derrett, Des Jarlais, Dharmaratne, Dherani, Diaz-Torne, Dolk, Dorsey, Driscoll, Duber, Ebel, Edmond, Elbaz, Ali, Erskine, Erwin, Espindola, Ewoigbokhan, Farzadfar, Feigin, Felson, Ferrari, Ferri, Fèvre, Finucane, Flaxman, Flood, Foreman, Forouzanfar, Fowkes, Franklin, Fransen, Freeman, Gabbe, Gabriel, Gakidou, Ganatra, Garcia, Gaspari, Gillum, Gmel, Gosselin, Grainger, Groeger, Guillemin, Gunnell, Gupta, Haagsma, Hagan, Halasa, Hall, Haring, Haro, Harrison, Havmoeller, Hay, Higashi, Hill, Hoen, Hoffman, Hotez, Hoy, Huang, Ibeanusi, Jacobsen, James, Jarvis, Jasrasaria, Jayaraman, Johns, Jonas, Karthikeyan, Kassebaum, Kawakami, Keren, Khoo, King, Knowlton, Kobusingye, Koranteng, Krishnamurthi, Lalloo, Laslett, Lathlean, Leasher, Lee, Leigh, Lim, Limb, Lin, Lipnick, Lipshultz, Liu, Loane, Ohno, Lyons, Ma, Mabweijano, MacIntyre, Malekzadeh, Mallinger, Manivannan, Marcenes, March, Margolis, Marks, Marks, Matsumori, Matzopoulos, Mayosi, McAnulty, McDermott, McGill, McGrath, Medina-Mora, Meltzer, Mensah, Merriman, Meyer, Miglioli, Miller, Miller, Mitchell, Mocumbi, Moffitt, Mokdad, Monasta, Montico, Moradi-Lakeh, Moran, Morawska, Mori, Murdoch, Mwaniki, Naidoo, Nair, Naldi, Narayan, Nelson, Nelson, Nevitt, Newton, Nolte, Norman, Norman, O'Donnell, O'Hanlon, Olives, Omer, Ortblad, Osborne, Ozgediz, Page, Pahari, Pandian, Rivero, Patten, Pearce, Padilla, Perez-Ruiz, Perico, Pesudovs, Phillips, Phillips, Pierce, Pion, Polanczyk, Polinder, Pope, Popova, Porrini, Pourmalek, Prince, Pullan, Ramaiah, Ranganathan, Razavi, Regan, Rehm, Rein, Remuzzi, Richardson, Rivara, Roberts, Robinson, De Leòn, Ronfani, Room, Rosenfeld, Rushton, Sacco, Saha, Sampson, Sanchez-Riera, Sanman, Schwebel, Scott, Segui-Gomez, Shahraz, Shepard, Shin, Shivakoti, Singh, Singh, Singh, Singleton, Sleet, Sliwa, Smith, Smith, Stapelberg, Steer, Steiner, Stolk, Stovner, Sudfeld, Syed, Tamburlini, Tavakkoli, Taylor, Taylor, Taylor, Thomas, Thomson, Thurston, Tleyjeh, Tonelli, Towbin, Truelsen, Tsilimbaris, Ubeda, Undurraga, van der Werf, van Os, Vavilala, Venketasubramanian, Wang, Wang, Watt, Weatherall, Weinstock, Weintraub, Weisskopf, Weissman, White, Whiteford, Wiersma, Wilkinson, Williams, Williams, Witt, Wolfe, Woolf, Wulf, Yeh, Zaidi, Zheng, Zonies, Lopez, Murray, AlMazroa and Memish1999; Widom et al. 2007; Danese et al. Reference Widom2009; Scott et al. Reference Widom, DuMont and Czaja2012; Cutuli et al. Reference Whiteford, Degenhardt, Rehm, Baxter, Ferrari, Erskine, Charlson, Norman, Flaxman, Johns, Burstein, Murray and Vos2013) were included in the analysis to examine the relationship between any childhood maltreatment and depression. Fig. 2a presents the individual study, pooled estimates, and funnel plots that were used to visually assess the presence of publication bias. A random-effects model was used.

Fig. 2. Odds ratios (OR) between childhood maltreatment and depression and/or anxiety and funnel plots. In the funnel plots, the x-axis shows the logarithmic scale of OR estimate for each study and y-axis is standard error of the logarithmic function of the OR. The dashed line represents the 95% confidence interval CI) and the point estimate of logarithmic transition of OR illustrates as the solid line. (a) Relationship between any maltreatment and depression, (b) relationship between any maltreatment and anxiety, (c) relationship between physical abuse and depression and/or anxiety, (d) relationship between sexual abuse and depression and/or anxiety, (e) relationship between neglect and depression and/or anxiety.
The pooled OR for depression for individuals with any type of childhood maltreatment compared to those without maltreatment history was 2.03 (95% CI 1.37–3.01, χ 2 = 10.94, I 2 = 63.4%, p = 0.027), indicating those with a child abuse history were 2.03 times more likely to have depression than those without such history.
As shown in the funnel plot in Fig. 2a , all the studies were within the domain, which represents 95% CI limits. No asymmetry was shown in the funnel plot. There was no evidence of publication bias (Egger's test, p = 0.46).
Sensitivity analysis was used to assess the influence of each study on overall estimates by omitting one study at a time. The analysis yielded with/without childhood maltreatment ORs ranging from 1.69 (95% CI 1.09–2.64) to 2.24 (95% CI 1.33–3.79). The combined OR was 1.91 (95% CI 1.27–2.85), which clearly indicates the experience of childhood maltreatment was a risk factor for depression.
Relationship between any maltreatment and anxiety
Four articles (Widom, 1999; Spataro et al. 2004; Cutajar et al. Reference Wells, Shea, O'Connell, Petersen, Welch, Losos and Tugwell2010; Scott et al. Reference Widom, DuMont and Czaja2012) were used to examine the relationship between any type of childhood maltreatment and anxiety disorders. Fig. 2b shows the individual study and pooled estimates, and funnel plots. A random-effects model was used.
The pooled OR for anxiety for individuals who experienced any type of childhood maltreatment compared to those who did not was 2.70 (95% CI 2.10–3.47, χ 2 = 6.65, I 2 = 54.9%, p = 0.084), indicating that those who experienced child abuse were 2.70 times more likely to have anxiety disorders in adulthood than those who did not experience maltreatment.
The funnel plot in Fig. 2b showed that all the studies were within the 95% CI domain. No asymmetry was found in the funnel plot. No evidence of publication bias was found (Egger's test, p = 0.26).
Sensitivity analyses found that with/without childhood maltreatment ORs ranging from 2.65 (95% CI 1.91–3.68) to 3.11 (95% CI 2.34–4.13). The combined OR was 2.84 (95% CI 2.19–3.68), clearly indicating that childhood maltreatment experience was a risk factor for anxiety disorders.
Relationship between physical abuse and depression or anxiety
Three articles (Brown et al. Reference Vos, Flaxman, Naghavi, Lozano, Michaud, Ezzati, Shibuya, Salomon, Abdalla, Aboyans, Abraham, Ackerman, Aggarwal, Ahn, Ali, Alvarado, Anderson, Anderson, Andrews, Atkinson, Baddour, Bahalim, Barker-Collo, Barrero, Bartels, Basáñez, Baxter, Bell, Benjamin, Bennett, Bernabé, Bhalla, Bhandari, Bikbov, Bin Abdulhak, Birbeck, Black, Blencowe, Blore, Blyth, Bolliger, Bonaventure, Boufous, Bourne, Boussinesq, Braithwaite, Brayne, Bridgett, Brooker, Brooks, Brugha, Bryan-Hancock, Bucello, Buchbinder, Buckle, Budke, Burch, Burney, Burstein, Calabria, Campbell, Canter, Carabin, Carapetis, Carmona, Cella, Charlson, Chen, Cheng, Chou, Chugh, Coffeng, Colan, Colquhoun, Colson, Condon, Connor, Cooper, Corriere, Cortinovis, de Vaccaro, Couser, Cowie, Criqui, Cross, Dabhadkar, Dahiya, Dahodwala, Damsere-Derry, Danaei, Davis, De Leo, Degenhardt, Dellavalle, Delossantos, Denenberg, Derrett, Des Jarlais, Dharmaratne, Dherani, Diaz-Torne, Dolk, Dorsey, Driscoll, Duber, Ebel, Edmond, Elbaz, Ali, Erskine, Erwin, Espindola, Ewoigbokhan, Farzadfar, Feigin, Felson, Ferrari, Ferri, Fèvre, Finucane, Flaxman, Flood, Foreman, Forouzanfar, Fowkes, Franklin, Fransen, Freeman, Gabbe, Gabriel, Gakidou, Ganatra, Garcia, Gaspari, Gillum, Gmel, Gosselin, Grainger, Groeger, Guillemin, Gunnell, Gupta, Haagsma, Hagan, Halasa, Hall, Haring, Haro, Harrison, Havmoeller, Hay, Higashi, Hill, Hoen, Hoffman, Hotez, Hoy, Huang, Ibeanusi, Jacobsen, James, Jarvis, Jasrasaria, Jayaraman, Johns, Jonas, Karthikeyan, Kassebaum, Kawakami, Keren, Khoo, King, Knowlton, Kobusingye, Koranteng, Krishnamurthi, Lalloo, Laslett, Lathlean, Leasher, Lee, Leigh, Lim, Limb, Lin, Lipnick, Lipshultz, Liu, Loane, Ohno, Lyons, Ma, Mabweijano, MacIntyre, Malekzadeh, Mallinger, Manivannan, Marcenes, March, Margolis, Marks, Marks, Matsumori, Matzopoulos, Mayosi, McAnulty, McDermott, McGill, McGrath, Medina-Mora, Meltzer, Mensah, Merriman, Meyer, Miglioli, Miller, Miller, Mitchell, Mocumbi, Moffitt, Mokdad, Monasta, Montico, Moradi-Lakeh, Moran, Morawska, Mori, Murdoch, Mwaniki, Naidoo, Nair, Naldi, Narayan, Nelson, Nelson, Nevitt, Newton, Nolte, Norman, Norman, O'Donnell, O'Hanlon, Olives, Omer, Ortblad, Osborne, Ozgediz, Page, Pahari, Pandian, Rivero, Patten, Pearce, Padilla, Perez-Ruiz, Perico, Pesudovs, Phillips, Phillips, Pierce, Pion, Polanczyk, Polinder, Pope, Popova, Porrini, Pourmalek, Prince, Pullan, Ramaiah, Ranganathan, Razavi, Regan, Rehm, Rein, Remuzzi, Richardson, Rivara, Roberts, Robinson, De Leòn, Ronfani, Room, Rosenfeld, Rushton, Sacco, Saha, Sampson, Sanchez-Riera, Sanman, Schwebel, Scott, Segui-Gomez, Shahraz, Shepard, Shin, Shivakoti, Singh, Singh, Singh, Singleton, Sleet, Sliwa, Smith, Smith, Stapelberg, Steer, Steiner, Stolk, Stovner, Sudfeld, Syed, Tamburlini, Tavakkoli, Taylor, Taylor, Taylor, Thomas, Thomson, Thurston, Tleyjeh, Tonelli, Towbin, Truelsen, Tsilimbaris, Ubeda, Undurraga, van der Werf, van Os, Vavilala, Venketasubramanian, Wang, Wang, Watt, Weatherall, Weinstock, Weintraub, Weisskopf, Weissman, White, Whiteford, Wiersma, Wilkinson, Williams, Williams, Witt, Wolfe, Woolf, Wulf, Yeh, Zaidi, Zheng, Zonies, Lopez, Murray, AlMazroa and Memish1999; Widom, 1999; Widom et al. 2007) were used to examine the relationship between physical abuse and either depression or anxiety disorders. Fig. 2c presents the individual study, pooled estimates, and funnel plots. A random-effects model was used. Analysis using a fixed-effects model did not affect the results.
The pooled OR for depression and/or anxiety for individuals who were physically abused in childhood compared to those who were not was 2.00 (95% CI 1.25–3.19, χ 2 = 2.98, I 2 = 32.9%, p = 0.225), indicating that children who were physically abused were two times more likely to develop depression or anxiety in adulthood than those who were not.
The funnel plot in Fig. 2c indicated that all the studies were within the 95% CI domain. No asymmetry was found in the funnel plot. No evidence of publication bias was found (Egger's test, p = 0.449).
Sensitivity analysis produced with/without physical abuse ORs ranging from 1.71 (95% CI 0.83–3.53) to 2.41 (95% CI 1.05–5.54). The combined OR was 1.96 (95% CI 1.02–3.78), indicating that childhood experience of physical abuse was an important risk factor for depression and anxiety disorders.
Relationship between sexual abuse and depression or anxiety
Five articles (Brown et al. Reference Vos, Flaxman, Naghavi, Lozano, Michaud, Ezzati, Shibuya, Salomon, Abdalla, Aboyans, Abraham, Ackerman, Aggarwal, Ahn, Ali, Alvarado, Anderson, Anderson, Andrews, Atkinson, Baddour, Bahalim, Barker-Collo, Barrero, Bartels, Basáñez, Baxter, Bell, Benjamin, Bennett, Bernabé, Bhalla, Bhandari, Bikbov, Bin Abdulhak, Birbeck, Black, Blencowe, Blore, Blyth, Bolliger, Bonaventure, Boufous, Bourne, Boussinesq, Braithwaite, Brayne, Bridgett, Brooker, Brooks, Brugha, Bryan-Hancock, Bucello, Buchbinder, Buckle, Budke, Burch, Burney, Burstein, Calabria, Campbell, Canter, Carabin, Carapetis, Carmona, Cella, Charlson, Chen, Cheng, Chou, Chugh, Coffeng, Colan, Colquhoun, Colson, Condon, Connor, Cooper, Corriere, Cortinovis, de Vaccaro, Couser, Cowie, Criqui, Cross, Dabhadkar, Dahiya, Dahodwala, Damsere-Derry, Danaei, Davis, De Leo, Degenhardt, Dellavalle, Delossantos, Denenberg, Derrett, Des Jarlais, Dharmaratne, Dherani, Diaz-Torne, Dolk, Dorsey, Driscoll, Duber, Ebel, Edmond, Elbaz, Ali, Erskine, Erwin, Espindola, Ewoigbokhan, Farzadfar, Feigin, Felson, Ferrari, Ferri, Fèvre, Finucane, Flaxman, Flood, Foreman, Forouzanfar, Fowkes, Franklin, Fransen, Freeman, Gabbe, Gabriel, Gakidou, Ganatra, Garcia, Gaspari, Gillum, Gmel, Gosselin, Grainger, Groeger, Guillemin, Gunnell, Gupta, Haagsma, Hagan, Halasa, Hall, Haring, Haro, Harrison, Havmoeller, Hay, Higashi, Hill, Hoen, Hoffman, Hotez, Hoy, Huang, Ibeanusi, Jacobsen, James, Jarvis, Jasrasaria, Jayaraman, Johns, Jonas, Karthikeyan, Kassebaum, Kawakami, Keren, Khoo, King, Knowlton, Kobusingye, Koranteng, Krishnamurthi, Lalloo, Laslett, Lathlean, Leasher, Lee, Leigh, Lim, Limb, Lin, Lipnick, Lipshultz, Liu, Loane, Ohno, Lyons, Ma, Mabweijano, MacIntyre, Malekzadeh, Mallinger, Manivannan, Marcenes, March, Margolis, Marks, Marks, Matsumori, Matzopoulos, Mayosi, McAnulty, McDermott, McGill, McGrath, Medina-Mora, Meltzer, Mensah, Merriman, Meyer, Miglioli, Miller, Miller, Mitchell, Mocumbi, Moffitt, Mokdad, Monasta, Montico, Moradi-Lakeh, Moran, Morawska, Mori, Murdoch, Mwaniki, Naidoo, Nair, Naldi, Narayan, Nelson, Nelson, Nevitt, Newton, Nolte, Norman, Norman, O'Donnell, O'Hanlon, Olives, Omer, Ortblad, Osborne, Ozgediz, Page, Pahari, Pandian, Rivero, Patten, Pearce, Padilla, Perez-Ruiz, Perico, Pesudovs, Phillips, Phillips, Pierce, Pion, Polanczyk, Polinder, Pope, Popova, Porrini, Pourmalek, Prince, Pullan, Ramaiah, Ranganathan, Razavi, Regan, Rehm, Rein, Remuzzi, Richardson, Rivara, Roberts, Robinson, De Leòn, Ronfani, Room, Rosenfeld, Rushton, Sacco, Saha, Sampson, Sanchez-Riera, Sanman, Schwebel, Scott, Segui-Gomez, Shahraz, Shepard, Shin, Shivakoti, Singh, Singh, Singh, Singleton, Sleet, Sliwa, Smith, Smith, Stapelberg, Steer, Steiner, Stolk, Stovner, Sudfeld, Syed, Tamburlini, Tavakkoli, Taylor, Taylor, Taylor, Thomas, Thomson, Thurston, Tleyjeh, Tonelli, Towbin, Truelsen, Tsilimbaris, Ubeda, Undurraga, van der Werf, van Os, Vavilala, Venketasubramanian, Wang, Wang, Watt, Weatherall, Weinstock, Weintraub, Weisskopf, Weissman, White, Whiteford, Wiersma, Wilkinson, Williams, Williams, Witt, Wolfe, Woolf, Wulf, Yeh, Zaidi, Zheng, Zonies, Lopez, Murray, AlMazroa and Memish1999; Widom, 1999; Spataro et al. 2004; Widom et al. 2007; Cutajar et al. Reference Wells, Shea, O'Connell, Petersen, Welch, Losos and Tugwell2010) were included in the analysis of the relationship between sexual abuse and depression and anxiety disorders. Fig. 2d presents the individual study and pooled estimates, and funnel plots. A random-effects model was used.
The pooled OR for depression and anxiety for individuals sexually abused in childhood compared to those who were not was 2.66 (95% CI 1.88–3.75, χ 2 = 9.06, I 2 = 55.9%, p = 0.06), indicating that children who experienced sexual abuse were 2.66 times more likely to develop depression or anxiety in adulthood than those without such experience.
As shown in Fig. 2d , the funnel plot indicated that all the studies were within the 95% CI domain. No asymmetry was found in the funnel plot. No evidence of publication bias was found (Egger's test, p = 0.417).
Sensitivity analysis yielded with/without sexual abuse ORs ranging from 2.75 (95% CI 1.81–4.16) to 3.16 (95% CI 2.35–4.27). The combined OR was 2.96 (95% CI 2.22–3.95), showing that childhood experience of sexual abuse was a strong risk factor for depression and anxiety disorders.
Relationship between neglect and depression or anxiety
Three articles (Brown et al. Reference Vos, Flaxman, Naghavi, Lozano, Michaud, Ezzati, Shibuya, Salomon, Abdalla, Aboyans, Abraham, Ackerman, Aggarwal, Ahn, Ali, Alvarado, Anderson, Anderson, Andrews, Atkinson, Baddour, Bahalim, Barker-Collo, Barrero, Bartels, Basáñez, Baxter, Bell, Benjamin, Bennett, Bernabé, Bhalla, Bhandari, Bikbov, Bin Abdulhak, Birbeck, Black, Blencowe, Blore, Blyth, Bolliger, Bonaventure, Boufous, Bourne, Boussinesq, Braithwaite, Brayne, Bridgett, Brooker, Brooks, Brugha, Bryan-Hancock, Bucello, Buchbinder, Buckle, Budke, Burch, Burney, Burstein, Calabria, Campbell, Canter, Carabin, Carapetis, Carmona, Cella, Charlson, Chen, Cheng, Chou, Chugh, Coffeng, Colan, Colquhoun, Colson, Condon, Connor, Cooper, Corriere, Cortinovis, de Vaccaro, Couser, Cowie, Criqui, Cross, Dabhadkar, Dahiya, Dahodwala, Damsere-Derry, Danaei, Davis, De Leo, Degenhardt, Dellavalle, Delossantos, Denenberg, Derrett, Des Jarlais, Dharmaratne, Dherani, Diaz-Torne, Dolk, Dorsey, Driscoll, Duber, Ebel, Edmond, Elbaz, Ali, Erskine, Erwin, Espindola, Ewoigbokhan, Farzadfar, Feigin, Felson, Ferrari, Ferri, Fèvre, Finucane, Flaxman, Flood, Foreman, Forouzanfar, Fowkes, Franklin, Fransen, Freeman, Gabbe, Gabriel, Gakidou, Ganatra, Garcia, Gaspari, Gillum, Gmel, Gosselin, Grainger, Groeger, Guillemin, Gunnell, Gupta, Haagsma, Hagan, Halasa, Hall, Haring, Haro, Harrison, Havmoeller, Hay, Higashi, Hill, Hoen, Hoffman, Hotez, Hoy, Huang, Ibeanusi, Jacobsen, James, Jarvis, Jasrasaria, Jayaraman, Johns, Jonas, Karthikeyan, Kassebaum, Kawakami, Keren, Khoo, King, Knowlton, Kobusingye, Koranteng, Krishnamurthi, Lalloo, Laslett, Lathlean, Leasher, Lee, Leigh, Lim, Limb, Lin, Lipnick, Lipshultz, Liu, Loane, Ohno, Lyons, Ma, Mabweijano, MacIntyre, Malekzadeh, Mallinger, Manivannan, Marcenes, March, Margolis, Marks, Marks, Matsumori, Matzopoulos, Mayosi, McAnulty, McDermott, McGill, McGrath, Medina-Mora, Meltzer, Mensah, Merriman, Meyer, Miglioli, Miller, Miller, Mitchell, Mocumbi, Moffitt, Mokdad, Monasta, Montico, Moradi-Lakeh, Moran, Morawska, Mori, Murdoch, Mwaniki, Naidoo, Nair, Naldi, Narayan, Nelson, Nelson, Nevitt, Newton, Nolte, Norman, Norman, O'Donnell, O'Hanlon, Olives, Omer, Ortblad, Osborne, Ozgediz, Page, Pahari, Pandian, Rivero, Patten, Pearce, Padilla, Perez-Ruiz, Perico, Pesudovs, Phillips, Phillips, Pierce, Pion, Polanczyk, Polinder, Pope, Popova, Porrini, Pourmalek, Prince, Pullan, Ramaiah, Ranganathan, Razavi, Regan, Rehm, Rein, Remuzzi, Richardson, Rivara, Roberts, Robinson, De Leòn, Ronfani, Room, Rosenfeld, Rushton, Sacco, Saha, Sampson, Sanchez-Riera, Sanman, Schwebel, Scott, Segui-Gomez, Shahraz, Shepard, Shin, Shivakoti, Singh, Singh, Singh, Singleton, Sleet, Sliwa, Smith, Smith, Stapelberg, Steer, Steiner, Stolk, Stovner, Sudfeld, Syed, Tamburlini, Tavakkoli, Taylor, Taylor, Taylor, Thomas, Thomson, Thurston, Tleyjeh, Tonelli, Towbin, Truelsen, Tsilimbaris, Ubeda, Undurraga, van der Werf, van Os, Vavilala, Venketasubramanian, Wang, Wang, Watt, Weatherall, Weinstock, Weintraub, Weisskopf, Weissman, White, Whiteford, Wiersma, Wilkinson, Williams, Williams, Witt, Wolfe, Woolf, Wulf, Yeh, Zaidi, Zheng, Zonies, Lopez, Murray, AlMazroa and Memish1999; Widom, 1999; Widom et al. 2007) contributed to the analysis of the relationship between neglect and depression and anxiety disorders. Fig. 2e presents the individual study and pooled estimates, and funnel plots. A fixed-effects model was used.
The pooled OR overall for depression and anxiety for individuals experienced neglect compared to those did not experience neglect was 1.75 (95% CI 1.37–2.24, χ 2 = 1.08, I 2 = 0.0%, p = 0.58), indicating that children who experienced neglect were 1.75 times more likely to develop depression or anxiety in adulthood than those who were not neglected.
As shown in Fig. 2e , the funnel plot indicated that all the studies were within the 95% CI domain. No asymmetry was found in the funnel plot. There was no evidence of publication bias (Egger's test, p = 0.284).
Sensitivity analysis for with/without neglect ORs ranged from 1.70 (95% CI 1.07–2.70) to 1.91 (95% CI 1.04–3.51). The combined OR was 1.76 (95% CI 1.13–2.75), pointing to childhood experience of neglect as a significant risk factor for depression and anxiety disorders.
Projected effects (PAFs)
Self-reported prevalence of childhood maltreatment and PAFs
In 2014, the worldwide self-reported prevalence of physical abuse was 22.6% (Stoltenborgh et al. Reference Paolucci, Genuis and Violato2015). Worldwide depression and anxiety disorders are estimated to affect 350 million (WHO, Reference Taylor and Brown2012) and 273 million adults (Vos et al. Reference Spataro, Mullen, Burgess, Wells and Moss2012), respectively. The PAF estimate used here for the effect of physical abuse on the incidence of depression and anxiety disorders was 18.4%, which indicates that nearly 115 million of depression and anxiety cases are potentially attributable to childhood physical abuse (Table 2). If the global prevalence of physical abuse was reduced by 10%, we estimated that there would be 9.5 million fewer depression and anxiety cases worldwide, whereas a 25% reduction could reduce prevalence by 24.6 million cases (Fig. 3). It should be noted that the numbers of cases attributable to any specific type of abuse and any specific mental disorder maybe an overestimate due to the existence of co-morbidity among mental disorders and the potential for an individual to suffer multiple types of abuse.

Fig. 3. Potential depression and anxiety cases that could be prevented through child maltreatment reduction worldwide.
Table 2. Depression and anxiety disorder cases attributable to specific types of childhood maltreatment worldwide
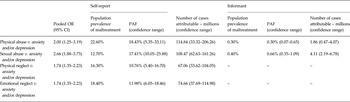
OR, Odds ratio; CI, confidence interval; PAF, population attributable fraction.
The self-reported prevalence of sexual abuse is 12.7% based on the Stoltenberg et al. (Reference Robins, Schoenberg, Holmes, Ratcliff, Benham and Works2011, Reference Paolucci, Genuis and Violato2015) meta-analyses. Approximately 17.4% (over 108 million) of depression and anxiety cases in the world are potentially attributable to childhood sexual abuse. If the prevalence of sexual abuse was reduced by 10%, about 9.1 million cases could potentially be prevented; a 25% reduction in sexual abuse prevalence could potentially prevent about 23.4 million cases worldwide.
It was estimated that 16.3% and 18.4% of worldwide population respectively have been exposed to physical and emotional neglect (Stoltenborgh et al. Reference Paolucci, Genuis and Violato2015). Our meta-analysis suggests about 10.8% (67 million) and 12.0% (75 million) of depression and anxiety cases respectively are potentially attributable to physical and emotional neglect. A 10% of reduction in the prevalence of physical neglect could potentially lower the number of cases of depression and anxiety by 6.1 million globally; this number would increase to 15.4 million if the prevalence physical neglect were reduced by 25%. Similarly, around 6.7 and 16.9 million of cases of depression and anxiety, respectively could be prevented by a 10% and a 25% reduction in the prevalence of emotional neglect.
Adding up specific types of maltreatment, over half (58.59%) of depression and anxiety cases worldwide are potentially attributable to childhood maltreatment. A 10% reduction in child maltreatment could potentially prevent 31.36 million depression and anxiety cases, and a 25% reduction could potentially prevent 80.28 million cases.
Informant prevalence of childhood maltreatment and PAFs
The informant prevalence of physical abuse was 0.3% (Stoltenborgh et al. Reference Paolucci, Genuis and Violato2015). It is estimated that 0.3% (nearly 1.9 million) of depression or anxiety cases are potentially attributable to childhood physical abuse. A 10–25% reduction of the prevalence could potentially prevent 190 000 to 460 000 of depression and anxiety cases.
It reported that 0.4% of the worldwide population have been exposed to sexual abuse based on informant studies (Stoltenborgh et al. Reference Paolucci, Genuis and Violato2015). The PAF estimate is 0.66%, which indicates that 4.1 million of depression and anxiety cases are potentially attributable to the exposure of sexual abuse in childhood. If the prevalence of sexual abuse was reduced by 10%, about 410 000 cases could potentially be prevented; a 25% reduction could potentially prevent about 1 020 000 cases.
Discussion
This meta-analyses consistently showed significant relationships between various types of maltreatment and depression and/or anxiety outcomes. The pooled OR between any type of maltreatment and depression was 2.03 (95% CI 1.37–3.01) and 2.70 (95% CI 2.10–3.47) for anxiety. For specific types of maltreatment and depression or anxiety disorders, the ORs were: physical abuse (OR 2.00, 95% CI 1.25–3.19); sexual abuse (OR 2.66, 95% CI 1.88–3.75); and neglect (OR 1.75, 95% CI 1.37–2.24).
Consistent with previous reviews, our results show childhood maltreatment is a risk factor for depression and anxiety disorders. Several meta-analyses, using less rigorous criteria for the measurement of maltreatment exposure, evaluating the short- and long-term effects of various types of childhood maltreatment on mental health support our finding that all types of child maltreatment are associated with an elevated risk of developing psychological disorders, including depression and anxiety disorders (Maniglio, Reference Fergusson, Horwood and Woodward2009; Paolucci et al. Reference Nanni, Uher and Danese2010; Nanni et al. Reference Meng and D'Arcy2012; Norman et al. Reference McCrory, De Brito and Viding2012).
This paper provides the first quantitative estimates on the projected reduction of mental disorders cases that could result from a reduction in child maltreatment. The PAFs estimate that over half of depression and anxiety cases worldwide are potentially attributable to childhood self-reported maltreatment. A 10–25% reduction in childhood maltreatment could potentially prevent 31.36–80.28 million depression and anxiety cases worldwide. When using informant based reports approximately 9 million cases are attributable to childhood physical or sexual abuse. A 10–25% of reduction in the prevalence of such child abuse could potentially prevent 0.4–1 million cases.
Both self-reported and informant measures of maltreatment have strengths and limitations. An obvious drawback of self-reported is the reliance on retrospective memory, which is often seen as unreliable and could be biased; whereas informant reports are often reflecting the most severe cases of maltreatment. Informant measures may better assess the continuity and circumstances of maltreatment experiences, such as neglect or emotional abuse; while self-reported measures may work better for some types of maltreatment, such as sexual abuse, which may be more invisible to informants. Additionally, informant studies may substantially underestimate abuse since they are based on reports by professionals to child protective services and cover shorter periods of childhood (usually a 1-year period), compared to self-report studies. However, a conclusion as to whether self-report prevalence rates are over- or underestimates is less clear cut. Childhood maltreatment may be overestimated when chronicity is not taken into account; it could also be underestimate when abuse is measured at a single time point (Fergusson et al. Reference Cutajar, Mullen, Ogloff and Thomas2000; Colman et al. Reference Cicchetti and Toth2015; Stoltenborgh et al. Reference Paolucci, Genuis and Violato2015).
PAF estimates provide quantitative measures of the impact that could be achieved by reducing the prevalence of childhood maltreatment on depression and anxiety. Our study strongly suggests that decreasing the amount of maltreatment in childhood should be the target for mental illness prevention and mental health promotion. This is not only because adverse experiences in childhood significantly increase the risk of adult depression and anxiety, but also because of its threats to children's development. A life-course perspective stresses the importance of early childhood experiences in setting the trajectory for future adolescent and adult risk behaviors and disease. Interventions and services for maltreatment should also promote resilience to further improve the mental health of general populations.
Strength and limitations of the current study
The strengths of this study come from the pooled the findings from longitudinal cohort studies and studies with externally documented childhood maltreatment, thus avoiding the issue of recall bias, effort after meaning and potential false memories. The studies reviewed here used strong mental health measures, are relatively recent, and are of good quality. PAF estimates show how the incidence of depression and anxiety could be substantially decreased by reducing childhood abuse.
However, there are several limitations. First, the small numbers of articles reviewed is an obvious limitation. It is unfortunate that more studies did not meet our stringent inclusion/exclusion criteria. Second, the studies reviewed are not representative of large sections of world's population with the studies coming from the USA (4), Australia (2), and New Zealand (2). Studies from developing countries are lacking. PAFs measures used the global prevalence of child abuse (both in general and specific types), which is more generalizable. Therefore, PAF estimates may be influenced by inconsistent measures between the global prevalence of maltreatment and associations between maltreatment and depression and anxiety observed in this meta-analysis. Third, heterogeneity was high in 3 of 4 analyses indicating substantial variation in the degree of association between childhood maltreatment and mental health outcomes in the studies reviewed. This reinforces the need for standardization in the measurement of childhood maltreatment and its various types and suggests that there may be significant moderators influencing the maltreatment and mental health relationship. There is a need for better tracking of potential moderators in future studies of childhood abuse. Fourthly, this review only included studies without recall bias in maltreatment assessment. The nature of these abuse reports often deals with more severe cases. Because the worldwide prevalence of child abuse does not provide data by severity levels, we used the crude overall prevalence to calculate PAFs. The estimates of PAFs may be influenced by the severity levels of child abuse. Finally, most selected studies, except one, did not report whether the outcome of interest (depression/anxiety) was present at baseline – in early childhood. Thus using strict criteria no causality can be inferred, as there is a lack of baseline data on depression and anxiety. Obviously, randomized clinical trials cannot (and should not) be conducted to examine the relationship between childhood maltreatment and depression and anxiety, therefore we are left with observational studies and meta-analyses of observational studies or naturally occurring experiments as our source of evidence. However, the weight of collaborating evidence suggests that a causal relationship plausibly exists.
Conclusion
Using externally documented measures of maltreatment thus avoiding the potential criticism of recall bias and false memory, this systematic review provides robust evidence about the effects of childhood maltreatment on the subsequent incidence of depression and anxiety in adulthood. The calculated PAFs showed the large reduction in the incidence of depression and anxiety that could result from reducing the prevalence of childhood maltreatment. This analysis reinforces the need for legal, health and social services initiatives aimed at reducing the prevalence of childhood maltreatment and for research that examines the factors that diminish the impact of childhood abuse on mental health.
Supplementary material
For supplementary material accompanying this paper visit http://dx.doi.org/10.1017/S0033291715002743.
Acknowledgements
M. Li was funded by the Western Regional Training Centre for Health Services Research (WRTC), Canada.
Declaration of Interest
None.







