


Young people's concerns about their body size and body shape, as triggered by social pressures and the media's focus on a thinner body, may lead them to dieting and other weight-control behaviours in order to lose weight( Reference Field, Camargo and Taylor 1 , Reference Field, Javaras and Aneja 2 ). Dieting has been documented to develop with the onset of adolescence and increase substantially by late adolescence( Reference Field, Camargo and Taylor 1 ). In the USA, the prevalence of dieting was shown to reach 25·3 % and 57·0 % in adolescent males and females, respectively( Reference Neumark-Sztainer, Wall and Guo 3 ). Dieting is also very prevalent among Greek adolescents; 14·7 % reported being on a diet to lose weight (males: 9·7 %; females: 19·5 %) and 22·9 % reported being dissatisfied with their body weight( Reference Yannakoulia, Karayiannis and Terzidou 4 ). In the Health Behaviour in School-Aged Children (HBSC) study, a cross-national study of children and adolescents from forty-three countries and regions across Europe and North America, Greece had the tenth and the seventh highest place of reported engagement in weight-reduction behaviours among 13- and 15 year-old adolescents, respectively( Reference Currie, Zanotti and Morgan 5 ).
Adolescents report that they engage in dieting in order to lose or maintain their weight( Reference Neumark-Sztainer, Story and Hannan 6 , Reference Grunbaum, Kann and Kinchen 7 ). However, longitudinal research findings support that dieting is not always associated with weight loss but instead with increased risk of future weight gain( Reference Neumark-Sztainer, Wall and Guo 3 , Reference Field, Austin and Taylor 8 – Reference Neumark-Sztainer, Wall and Story 10 ) and onset of obesity( Reference Stice, Cameron and Killen 11 , Reference Stice, Presnell and Shaw 12 ). One potential explanation for this paradoxical association between dieting and future weight gain might be the fact that dieting is adopted as a short-term solution to weight loss instead of healthier eating and physical activity, which are more likely to have more positive implications for long-term weight management( Reference Neumark-Sztainer, Wall and Haines 13 ). In support of this evidence, the overall dietary quality of adolescent dieters has been shown to be lower than that of their peers who were not dieting( Reference Woodruff, Hanning and Lambraki 14 ). Additionally, use of unhealthy weight-control behaviours during adolescence has also been associated with poorer dietary intakes and meal skipping( Reference Larson, Neumark-Sztainer and Story 15 ).
Given that adolescence is a crucial period for establishing dietary behaviours that persist into adult life and may further contribute to obesity risk( Reference Story, Neumark-Sztainer and French 16 ), and in light of the importance of adequate nutrition during adolescence( Reference Lytle 17 , Reference Spear 18 ), understanding the relationships between eating behaviours and dieting involvement is essential. In this regard, the aim of the present cross-sectional study was to record the prevalence of dieting and to compare markers of obesity as well as dietary intakes and eating behaviours across dieting categories in a sample of healthy Greek male and female adolescents living in a wide urban area, who participated in the TEENAGE (TEENs of Attica: Genes & Environment) study. For this purpose study participants were classified into three dieting categories, which were: (i) those who were not currently dieting and who had never dieted in the past (never dieters); (ii) current dieters; and (iii) those who had dieted in the past but were not currently dieting (past dieters).
Experimental methods
Sampling
The TEENAGE study is a cross-sectional study comprising healthy Greek adolescents. The study was conducted according to the guidelines specified in the Declaration of Helsinki and all procedures involving human subjects were approved by the Institutional Review Board of Harokopio University and the Greek Ministry of Education, Lifelong Learning and Religious Affairs. The TEENAGE study target population comprised adolescent students aged 13–15 years attending the first three classes of public secondary schools located in the wider Athens area of Attica (3 812 330 inhabitants, according to data provided by the National Statistical Service of Greece 2001 Census). The province of Attica includes approximately 80 % urban areas, where Athens is the metropolis. The regions across Attica from which students were recruited were physically similar and all urban in nature. Sampling of regions and schools selected to participate was random. Students were enrolled from the wider urban region to ensure that they were coming from families with varying educational background and socio-economic status. Moreover, in order to exclude any vast economic disparities, all participating schools were exclusively public schools, which are free of charge. A total of twenty-four schools participated in the study out of 285 junior secondary public schools in Attica.
The study procedure was divided into three interrelated stages. During the first stage and prior to recruitment, registered students in the participating schools as well as their parents/guardians received detailed written information explaining the aims of the study, the voluntary nature and the confidentiality of the data, along with a consent form. Consent forms signed by parents/guardians were collected from students intending to participate in the study along with their verbal assent, and each student received a unique study identifier. A total number of 857 adolescent students out of 1440 attending participating schools (participation rate: 59·5 %) were recruited in the TEENAGE study. The final sample represented 0·7 % of the total population of 13- to 15-year-olds residing in Attica, estimated to be 119 840 children based on information provided by the National Statistical Service of Greece 2001 Census.
At the second stage, a one-on-one assessment session (i.e. clinical examination, fasting blood sampling, anthropometrics, 24 h dietary and physical activity recall, and questionnaires on meal patterns, lifestyle, personal and family medical and sociodemographic characteristics) took place at each participating school. At the third stage, students were contacted via telephone for a second dietary and physical activity 24 h recall approximately 10d after the first assessment stage. Additional clarification or missing information was also obtained during this stage. Study personnel consisted of nutrition professionals and paediatric health-care professionals. All were trained and evaluated to ensure accurate data collection on all measurements and were available to assist participants and their parents/guardians during questionnaire completion.
Anthropometry and clinical assessment
Basic anthropometric examination included weight and height measurements. Body weight was measured to the nearest 0·1 kg, with the participants barefoot and dressed in light clothing, by the use of a weighing scale (Seca Alpha, Hamburg, Germany). Height was measured to the nearest 0·1 cm using a portable stadiometer while the participants were barefoot with their shoulders in a relaxed position, their arms hanging freely and their head in a normal position, with the eyes looking straight ahead. BMI (kg/m2) was calculated as weight divided by the square of height. Waist circumference (cm) was measured between the twelfth rib and the iliac crest, and hip circumference (cm) around the hips at the point of the largest extension, with the use of a soft tape. Waist-to-hip ratio was then calculated. A set of Lange skinfold callipers (Cambridge Scientific Instruments, Cambridge, MA, USA) was used to measure triceps, subscapular and suprailiac skinfolds on the right side of the body to the nearest 0·1 mm; two repeated measurements were obtained for each skinfold and then the mean was calculated. Total body fat (%) was estimated with use of the Slaughter equations ( Reference Slaughter, Lohman and Boileau 19 ) separately for males and females.
Assessment of dietary profiles, eating behaviours and under-reporting
Dietary assessment was conducted via two non-consecutive 24 h recalls( Reference Frank, Berenson and Schilling 20 ). The second dietary recall was conducted 3–10 d after the first recall on a different day of the week from the first interview. Food models and sample measures (such as cups and spoons) were used to specify serving sizes. Consumption of vitamin and mineral dietary supplements was also recorded. The 24 h recalls were analysed with the use of Nutritionist Pro software, version 2·2. The Nutritionist Pro food database was expanded by adding analyses of traditional Greek foods and recipes, and nutrient information for local processed food items, such as snacks, sweets and fast foods, as shared by industry( Reference Trichopoulou and Georga 21 , Reference Kafatos, Verhagen and Moschandreas 22 ). Mean energy, macro- and micronutrient intakes were estimated for all study participants. The percentage of energy (MJ (kcal)) derived from protein, carbohydrate and fat was also calculated.
Eating style, which reflects the conditions under which eating occurs and the role of hunger in eating, was also assessed. In particular, feeding practices related to each of the ‘five onlys’ (1. eating only in the dining room; 2. eating only while sitting; 3. eating only from a proper plate; 4. eating only when doing nothing else; 5. eating only when hungry) were assessed through five-point scales ranging from ‘always’ (=1) to ‘never’ (=5)( Reference Golan, Fainaru and Weizman 23 ). Participants’ self-reports for each item were added to calculate a total eating style score; the higher the score, the more frequently an individual engaged in less well-structured feeding practices promoting food intake for reasons other than hunger.
Moreover, study participants completed a questionnaire about their meal patterns and eating behaviour. This questionnaire was a modified version of a set of questions about meal patterns used in the HBSC study( Reference Vereecken, Ojala and Jordan 24 ). Frequency of meal consumption was evaluated by questions such as ‘How often do you have breakfast?’, ‘How often do you have full breakfast (more than a glass of milk or fruit juice)?’, ‘How often do you usually have lunch?’ and ‘How often do you usually have dinner?’. Possible responses included ‘never’, ‘1–2 times/week’, ‘3–4 times/week’, ‘5–6 times/week’ or ‘every day’. Individuals were also asked how often they eat fast food. Possible responses to this question included ‘never’, ‘1–2 times/week’, ‘3–4 times/week’, ‘5–6 times/week’ or ‘every day’. Additionally, participants were asked if they had experienced eating a large amount of food (‘Have you ever experienced eating a large amount of food in a short period of time?’) and binge eating (‘Have you ever gone on eating binges and felt that you could not stop?’). Individuals who responded positively were then asked about the frequency of these episodes. Possible responses included ‘never or rarely’, ‘sometimes’, ‘once/month’, ‘2–3 times/months’, ‘once/week’, ‘2–3 times/week’ and ‘>3 times/week’. They were also asked about their involvement in slimming diets, either during the time of the study or in the past. More specifically, participants were asked to indicate whether they were on a diet at the time of the survey: ‘Are you currently on a diet in order to lose weight?’. Those who responded positively were classified as ‘current dieters’. Study participants were also asked whether they experienced dieting in the past: ‘Have you ever been involved in a diet in order to lose weight?’. In order to investigate whether there were any differences in the variables under investigation between those currently dieting and those not currently dieting but who reported past dieting, participants who replied ‘yes’ and who reported that they were not on a diet at the time of the survey were classified as ‘past dieters’. Finally, participants who did not indicate any dieting episode in the past, and who were not currently dieting, were classified as ‘never dieters’.
For the evaluation of low energy reporting, the ratio of reported energy intake to BMR was determined for each study participant. The BMR was estimated using the Schofield predictive equations( Reference Schofield 25 ), adopted by the 2004 FAO/WHO/United Nations University report( 26 ). Cut-off limits proposed by Goldberg et al.( Reference Goldberg, Black and Jebb 27 ) and adapted to children and adolescents by Sichert-Hellert et al.( Reference Sichert-Hellert, Kersting and Schoch 28 ) were used to identify under-reporters. This exclusion criterion was applied only for never dieters and past dieters. Due to their involvement in a weight-loss diet, current dieters are eating less so as to create a negative energy balance and thus they might have lower energy intakes.
Clinical assessment and demographic information
Sexual maturity status was assessed by self-evaluation of the participant( Reference Duke, Litt and Gross 29 , Reference Bonat, Pathomvanich and Keil 30 ) in the presence of the team's paediatrician according to Tanner's criteria( Reference Tanner 31 ) for breast, pubic hair and genital development. Parents/guardians of participating adolescents were asked to fill out a questionnaire about sociodemographic characteristics (i.e. ethnicity, employment, mean annual income, educational level, current body weight, height and age, smoking habits as well as data regarding labour, feeding practices and smoking during the participant's infancy).
Statistical analysis
Descriptive statistics of continuous variables are presented as means and standard deviations, whereas categorical variables are presented as absolute or relative frequencies. Meal patterns were dichotomised prior to analysis. The cut-off value for main meals (i.e. breakfast, lunch and dinner) was ‘every day’, while for fast-food consumption frequency the cut-off was set to ‘>2 times/week’. Comparisons between categorical variables were tested using the χ 2 test. ANOVA was performed to assess the association of dieting group with age, Tanner stage and markers of obesity (BMI, waist circumference and body fat percentage) as well as dietary profile variables. Furthermore, to compare means between dieting groups, post hoc analyses were performed. Bonferroni tests to correct for multiple comparisons were conducted to explore between-group differences. Univariate ANOVA was performed to evaluate differences in eating style scores among never dieters, current dieters and past dieters before and after adjustment for age, Tanner stage and maternal educational status, separately for males and females. Mean values of eating style score were also assessed. Reported P values are based on two-sided tests and statistical significance was set at P < 0·05. All statistical analyses were performed using the statistical software package SPSS for Windows version 18·0.
Results
A total of 857 (54·9 % females) adolescents of mean age 13·4 (sd 0·9) years were recruited in the TEENAGE study. Prevalence of dieting, descriptive characteristics, body composition parameters and dietary intakes of males and females separately across dieting categories are displayed in Table 1. Overall, 20·1 % of the adolescents were currently dieting (current dieters), while 15·2 % had experienced dieting in the past (past dieters). In detail, a lower percentage of males than females belonged to the category of past dieters (10·7 % vs. 18·9 %; χ 2 = 10·0, P = 0·007) whereas no gender differences were observed for the prevalence of current dieters. Eighty-seven per cent of current dieters also reported dieting in the past (86·8 % in females and 85·4 % in males). Although no significant differences in mean age and Tanner stage were observed across dieting groups in males, in females past dieters were significantly older (P = 0·033) and characterised by a higher Tanner stage than never dieters (P = 0·033). Mean BMI (males and females: P < 0·001 for both), body fat percentage (males and females: P < 0·001 for both) and waist circumference (males: P = 0·039; females: P = 0·009) of both male and female adolescents were significantly different across the three dieting groups. Reported energy intake of current dieters was significantly lower in both male and female adolescents (P < 0·001); while no significant differences were observed in macronutrient intakes either in males or in females.
Table 1 Anthropometric characteristics and dietary profiles of never dieters, current dieters and past dieters according to sex in a sample of urban Greek adolescents (n 857) from the TEENAGE (TEENs of Attica: Genes & Environment) study

a,bFor each sex, mean values within a row with unlike superscript letters were significantly different (P < 0·05).
†Dietary variables are reported only for never dieters and past dieters with plausible energy intakes, while all current dieters were included in these analyses.
‡Relative percentages of total energy intake derived from macronutrients.
Table 2 displays differences in meal patterns and eating behaviours across the three dieting groups separately for the two sexes. Prevalence of breakfast skipping differed significantly across dieting groups in females (χ 2 = 10·92, P = 0·004) but not in males; while significant differences in dinner skipping were observed in both male (χ 2 = 10·55, P = 0·005) and female adolescents (χ 2 = 20·91, P < 0·001). No significant differences in lunch skipping and frequency of fast-food consumption were observed in either adolescent boys or girls. Moreover, incidence of eating large quantities of food also differed significantly across the three dieting categories in females only (χ 2 = 7·18, P = 0·028). No significant difference was observed in the prevalence of binge eating across the three groups of dieters in either sex.
Table 2 Meal patterns and eating behaviours according to dieting involvement and sex in a sample of urban Greek adolescents (n 857) from the TEENAGE (TEENs of Attica: Genes & Environment) study

Mean values of eating style score were significantly different across the three dieting groups in female adolescents (P = 0·043) and remained significant even after adjustment for age, Tanner stage and maternal educational status (P = 0·009). Female never dieters and current dieters had significantly (P = 0·010 and P = 0·026, respectively) lower eating style scores than past dieters, while no significant difference in eating style score was observed across dieting groups in males (Fig. 1).
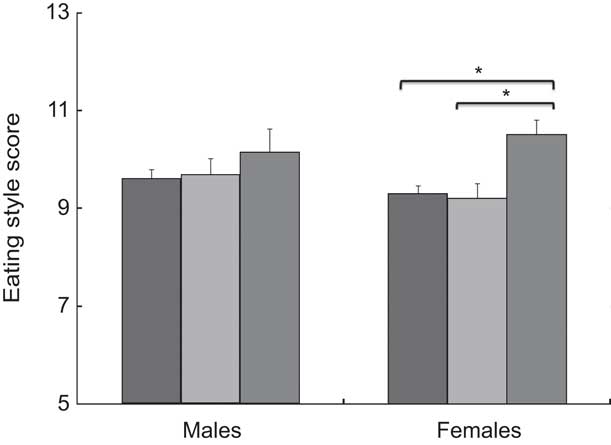
Fig. 1 Differences in eating style score among never dieters (![]() ), current dieters (
), current dieters (![]() ) and past dieters (
) and past dieters (![]() ) according to sex in a sample of urban Greek adolescents (n 857) from the TEENAGE (TEENs of Attica: Genes & Environment) study. Values are means, after adjustment for age, Tanner stage and maternal educational status, with their standard errors represented by vertical bars. Mean values were significantly different: *P < 0·05
) according to sex in a sample of urban Greek adolescents (n 857) from the TEENAGE (TEENs of Attica: Genes & Environment) study. Values are means, after adjustment for age, Tanner stage and maternal educational status, with their standard errors represented by vertical bars. Mean values were significantly different: *P < 0·05
Discussion
The main purpose of the present cross-sectional study was to record the prevalence of dieting and to compare indices of body composition as well as dietary intakes and eating behaviours according to dieting involvement in male and female healthy Greek adolescents who participated in the TEENAGE study. Overall, involvement in slimming diets at least one time during their lifetime was reported by 32·6 % of all study participants. More specifically, 20·1 % of all adolescents reported being on a diet at the time of the survey (current dieters) while 15·2 % reported involvement in dieting practices in the past (past dieters). In consistency with previous literature( Reference Neumark-Sztainer, Wall and Guo 3 ), the present findings also showed a higher proportion of female adolescent dieters compared with their male peers. Female adolescents who reported dieting either during the survey or in the past were significantly older and more sexually mature according to Tanner's criteria( Reference Tanner 31 ) than females who reported no dieting involvement. Early pubertal timing is a well-established risk factor for dieting in girls( Reference McCabe and Ricciardelli 32 ). The physical changes of puberty observed in girls, such as increasing adiposity as well as breast development, may cause body dissatisfaction and lower self-esteem, which may in turn increase postpubertal girls’ attempts to lose weight through ineffective weight-control behaviours( Reference Stice, Presnell and Bearman 33 ). In a large nationwide cross-sectional study Yannakoulia et al.( Reference Yannakoulia, Karayiannis and Terzidou 4 ) also showed a high prevalence of dieting and body weight dissatisfaction in Greek adolescents, which was higher among females than males and increased with age.
The present results also showed that adolescents who were dieting at the time of the survey or who had dieted in the past had significantly higher BMI and body fat percentage than those who had never dieted, in both sexes. These results are consistent with other findings showing that overweight and obese individuals will more often engage in dieting in order to control their weight than normal-weight individuals( Reference Neumark-Sztainer, Story and Hannan 6 , Reference Whittle, Yarnell and Stevenson 34 , Reference Boutelle, Neumark-Sztainer and Story 35 ). However, dieting has been shown to be prevalent among normal-weight adolescents as well; and it has been related to self-perceived weight status and body image distortion( Reference Liechty 36 ). Information regarding inaccurate perception of body size was not available in our study to further investigate how this might affect dieting involvement.
Although overweight during adolescence increases the risk for dieting, simultaneously, longitudinal studies have shown that use of dieting and other unhealthy weight-control behaviours by adolescents predicts greater increase in BMI compared with no use of such behaviours( Reference Neumark-Sztainer, Wall and Guo 3 , Reference Neumark-Sztainer, Wall and Story 10 ); these associations were observed in both overweight and non-overweight individuals( Reference Neumark-Sztainer, Wall and Story 10 ). Newmark-Sztainer et al.( Reference Neumark-Sztainer, Wall and Haines 13 ) have shown that dieting strongly predicts decreased breakfast consumption, increased binge eating as well as other unhealthy weight-control behaviours, and they suggest that dieting may lead to weight gain partially through the adoption of these behaviours, which are less likely to be effective in long-term weight management.
In this regard, we further investigated how reported dietary intakes and eating behaviours might differ in adolescents in relation to their dieting involvement. Reported energy intake of currently dieting boys and girls was lower than reported energy intake of never dieters and past dieters, suggesting that adolescents on a weight-loss diet are restricting their total energy intakes in order to create a negative energy balance. This finding is in agreement with previous research showing that the majority of adolescent dieters may perceive dieting as a reduction in total energy, fat or sugar intakes( Reference Roberts, Maxwell and Bagnall 37 ). In order to investigate differences in energy and macronutrient intakes across dieting groups, never dieters and past dieters with non-plausible energy intake were excluded from our analyses. However, even in the group of current dieters who probably do have a lower energy intake due to their current involvement in dieting, the possibility of under-reporting cannot be excluded.
Findings of the current study also suggested that differences in eating behaviours might be related to differences in dieting involvement. In our study, adolescent dieters skipped breakfast and dinner more frequently than never dieters. These behaviours were more common among female dieters than male dieters, which is in accordance with previous literature( Reference Lattimore and Halford 38 ). Findings from an epidemiological survey conducted throughout Greece also showed breakfast skipping to be more prevalent among adolescent dieters compared with those who had never been on a diet( Reference Kapantais, Chala and Kaklamanou 39 ). Howe et al.( Reference Howe, Mandic and Parnell 40 ), in a web-based survey conducted in adolescents from New Zealand, reported that adolescent dieters were less likely to eat lunch and an evening meal on one more weekday than those who were not dieting, while similar results were also observed for the number of lunches and dinners eaten during the entire week. Given that in our study meal patterns were assessed on a weekly basis, investigating how meal patterns in relation to dieting might differ between weekdays and weekends was not possible.
Additionally, we showed that female dieters apart from meal skipping also reported eating large quantities of food more frequently compared with never dieters. In agreement with our findings, Field et al. showed that frequent dieters were more likely to report binge eating than those who were not dieting( Reference Field, Austin and Taylor 8 ). Dietary restraint has been associated with disinhibition and overeating in the presence of large portion sizes( Reference Bryant, King and Blundell 41 , Reference Herman, van Strien and Polivy 42 ).
Longitudinal evidence suggests that dieting and unhealthy weight-control behaviours tend to track within individuals: those who engaged in these behaviours during adolescence were at increased risk for these behaviours 10 years later( Reference Neumark-Sztainer, Wall and Larson 43 ). Moreover, persistent use of dieting and unhealthy weight-control behaviours has been shown to predict greater increase in BMI( Reference Neumark-Sztainer, Wall and Story 10 ). The fact that the great majority (87 %) of current dieters also reported past dieting might suggest frequent dieting involvement in our study sample as well. Although data regarding the effectiveness of previous dieting attempts were not available in our study, the non-significant differences observed in anthropometric traits between the two groups of dieters might be indicative of the ineffectiveness of these efforts. It has been proposed that the majority of adolescents who report dieting involvement may have engaged in unsuccessful attempts to restrict their dietary intakes over prolonged periods( Reference Neumark-Sztainer, Wall and Story 10 , Reference Larsen, van Strien and Eisinga 44 ).
Eating style score, which reflects conditions under which eating occurs and the role of hunger in eating, was also higher in female past dieters compared with current dieters and never dieters, suggesting that female past dieters engaged more frequently in less well-structured feeding practices promoting food intake for reasons other than hunger. Changes in the aforementioned behaviours have been shown to be associated with weight loss( Reference Golan, Fainaru and Weizman 23 ). The lack of difference in score between current and never dieters might suggest that individuals who are currently dieting may exhibit a more well-ordered eating style that characterises never dieters. However, the higher values of eating style score observed among female past dieters compared with current dieters might also suggest that these behaviours may not last over time.
Our findings should be interpreted in light of the limitations and strengths of the study. From the results of this cross-sectional study it is not possible to establish causal relationships between dieting and obesity indices, dietary intakes and eating behaviours. Data regarding meal patterns and dieting involvement were collected with the use of questionnaires and several of the respondents might have under- or over-reported the behaviours we evaluated. Even though we carefully adjusted for potential confounders, residual confounding may always exist in observational research. However, the relatively large study sample and the random sampling of schools from the wider urban region of Attica could be considered as strengths of the present study.
Conclusions
The present study showed a high prevalence of dieting among adolescents. Both groups of dieters, either current or past, had greater BMI and body fat percentage and reported more frequent involvement in unhealthy eating behaviours such as meal skipping than never dieters. Our findings also suggested that the apparently healthier, ordered eating style of dieters adopted during the dieting period may not be maintained once it ends. These conclusions from our study have several implications for the development and adoption of healthy eating behaviours. Appropriate educational programmes targeting adolescents might be helpful in order to help them understand the benefits of more healthy alternatives to short-term dieting, often expressed as meal skipping and other unhealthy weight-control behaviours, to ensure successful, long-term weight management.
Acknowledgements
Sources of funding: This research was co-financed by the European Union (European Social Fund – ESF) and Greek national funds through the Operational Program ‘Education and Lifelong Learning’ of the National Strategic Reference Framework (NSRF) Research Funding Program ‘Heracleitus II. Investing in knowledge society through the European Social Fund’. Conflicts of interest: There is no conflict of interest. Authorship responsibilities: G.V.D. is the Principal Investigator and supervised the study. I.N. contributed to the study design, supervised the field participants and performed the statistical analyses. G.V.D. and I.N. performed the interpretation of the data. All authors carried out the data collection and contributed to data management, database preparation, and the writing and approval of the final version of the manuscript submitted for publication. Acknowledgements: The authors would like to thank all study participants and their families. They also wish to acknowledge Dr Mary Yannakoulia, Dr Eleftheria Zeggini, paediatricians Eleana Gkioka, Natalia Lazopoulou, Sophia Sakka and Costas Tziouvas, Sandra Armango, Danai Christakopoulou, Kristalia Diamantidi, Dimitris Peppas, Aliki-Eleni Farmaki and all volunteers for their contribution to the study.



