


Unhealthy eating patterns are a known risk factor for a number of chronic diseases that contribute annually to premature death and disability globally( 1 , 2 ). Consequently, supporting healthier food behaviours is of key importance to population health. As the majority of household food expenditure takes place in the supermarket( 3 – 5 ), supporting healthier food purchasing behaviour is likely to have a positive impact on population dietary patterns. Healthier food purchasing behaviour may limit the availability of unhealthier foods in the home, thus acting as a controlling mechanism for consumers when cues towards competing goals and behaviours arise. However, consumers view healthy food purchasing as a difficult and effortful task( Reference O’Brien, McConnon and Hollywood 6 ) and achieving long-term change has proved difficult. While both financial incentives and store-based interventions are associated with behavioural change, evidence indicates that their positive impact lasts only for the duration of the intervention( Reference Liberato, Bailie and Brimblecombe 7 , Reference Roe, Hunt and Bradshaw 8 ). Thus, alternative approaches are needed to achieve sustained change.
Grocery shopping is often viewed as a scripted routinised behaviour where consumers use individual scripts, or knowledge structures, to determine the behaviours which should be enacted in repeated events( Reference Abelson 9 – Reference Iyer and Ahlawat 11 ). However, elements of food purchasing behaviour may also be viewed as habitual( Reference Bettman, Johnson and Payne 12 – Reference Wood and Neal 15 ), where consistent repetition of a behaviour in the presence of stable contextual cues increases the automaticity of that behaviour( Reference Lally and Gardner 16 ). Subsequent habit performance is driven by these contextual cues such as time, people and places( Reference Wood and Neal 15 , Reference Wood, Tam and Witt 17 ). Traditional intervention approaches typically utilise educational measures to change individual knowledge levels and attitudes which fail to address the habitual elements that influence food purchasing behaviour( Reference Verplanken and Wood 18 , Reference Webb and Sheeran 19 ). Consequently, it is possible that the difficulty encountered in changing food purchasing behaviour may be due to the presence of habit and a lack of consideration of habit theory during intervention design. Future interventions should address both routine and habitual elements of food purchasing behaviour to improve the potential to achieve sustained behaviour change( Reference Gardner, Lally and Wardle 20 – Reference van’t Riet, Sijtsema and Dagevos 22 ).
Building on the cue–response relationship that drives habitual behaviour, van’t Riet et al. ( Reference van’t Riet, Sijtsema and Dagevos 22 ) have outlined potential intervention strategies to support healthier food behaviours (Table 1). The first category, performance cue, focuses on the behavioural context and proposes adapting the cues which drive habit performance. The response category centres on changing the individual’s response to the contextual cue through engagement of self-regulation processes. The final category, contingencies, outlines strategies that influence the reinforcement of habitual behaviour and can influence subsequent performance. This framework provides a useful theoretical basis to inform the development of future interventions to support healthier food purchasing behaviour.
Table 1 Proposed strategies to change existing and create new habits (from van’t Riet et al.( Reference van’t Riet, Sijtsema and Dagevos 22 ))

Another important aspect of intervention development is identification of an appropriate mode for intervention delivery( Reference Craig, Dieppe and Macintyre 23 ), with recent technological advances positioning mobile phones as a potentially effective approach( Reference Afshin, Babalola and Mclean 24 – Reference Mehran, Nazeri and Delshad 30 ). High ownership levels mean there is potential to engage a significant proportion of the population( Reference Anderson 31 ). Individuals display a strong attachment to their mobile phones, allowing participant engagement in relevant contexts( Reference Dey, Wac and Ferreira 32 ); a key consideration in addressing habitual behaviours guided by contextual cues. One important recent technological advance is the development of mobile apps, which are software applications developed specifically for use on small, wireless computing devices such as smartphones and tablets. Mobile apps offer additional opportunities for individual engagement and support as they ‘take advantage of computer capabilities as well as the power of networking’( Reference Handel 33 ). Dietitians and nutritionists are incorporating mobile apps into their practice to a greater extent( Reference Lieffers, Vance and Hanning 34 – Reference Jospe, Fairbairn and Green 36 ). While more research is needed on their effectiveness in changing food behaviours, current evidence suggests there may be potential for a positive impact( Reference Ball, Mouchacca and Jackson 37 – Reference Gilliland, Sadler and Clark 40 ). Existing mobile apps can support self-monitoring of dietary intake (e.g. weightmate), allow assessment of nutritional quality (e.g. FoodSwitch), or provide a grocery list creation function to support meal planning and purchasing behaviour (e.g. ShopShop). In relation to habitual behaviours, Stawarz et al.( Reference Stawarz, Cox and Blandford 41 ) proposed that mobile apps could support habit formation if designed correctly but did not comment on their potential effectiveness in changing habits. As mobile technology is continually advancing it is likely that newer features are being integrated which may address habitual elements of behaviour. Thus, mobile apps offer a novel approach to intervention delivery and warrant further consideration in relation to healthier food purchasing behaviour.
Despite potentially promising evidence, three potential issues have been raised. First, health interventions are typically more effective if based upon a valid theoretical framework( Reference Craig, Dieppe and Macintyre 23 , Reference Glanz and Bishop 42 ), but relevant theory is not always adequately utilised in mobile app design( Reference Stawarz, Cox and Blandford 41 , Reference Pagoto, Schneider and Jojic 43 – Reference West, Hall and Hanson 45 ). Second, the mobile app must be viewed as acceptable by the individual to ensure it is used for a sufficient period to support behaviour change. User quality components, such as engagement and functionality, have an important influence on acceptability( Reference Chang, Kaasinen and Kaipainen 46 – Reference Wang, Egelandsdal and Amdam 49 ) but may also be inadequately integrated or done to the exclusion of theoretical content( Reference Nicholas, Larsen and Proudfoot 50 , Reference Reynoldson, Stones and Allsop 51 ). The final consideration for dietary-related mobile apps is the quality of the nutrition information provided. Evidence suggests that the quality of health-related websites and mobile apps is varied( Reference Reynoldson, Stones and Allsop 51 – Reference Taki, Campbell and Russell 53 ), with very little engagement of relevant health professionals in their design( Reference Reynoldson, Stones and Allsop 51 , Reference Taki, Campbell and Russell 53 ) and an over-reliance on food composition databases that do not acknowledge individual differences or existing health conditions( Reference Boyce 35 ). Incorrect nutrition advice can lead to unhealthy eating practices, with potential for negative health consequences( Reference Lieffers, Vance and Hanning 34 ). It is essential that the nutrition content of a mobile app is based on sound information to ensure behaviour change is directed towards healthier food behaviours.
While mobile apps offer a novel approach for supporting healthier food purchasing behaviours, it is evident that a number of design issues need to be considered prior to their wider implementation in public health. Much research focuses on new technology development to address such a problem, but Hingle and Patrick( Reference Hingle and Patrick 47 ) emphasise the need to utilise existing resources. Consequently, it is important to assess the potential of existing mobile apps to support healthier food purchasing behaviour. To date, no assessment of existing mobile apps has been made in relation to food purchasing behaviour focusing on behaviour change, user quality and nutrition content. Given the important influence that food purchasing behaviour has on subsequent dietary patterns and the potential effectiveness of mobile apps to support behaviour change, there is a need to further explore the potential role of existing mobile apps. Consequently, the aim of the present study was to assess the quality of nutrition content and the integration of user quality components and behaviour change theory relevant to food purchasing behaviour in a sample of existing mobile apps.
Methods
Study design
The study design involved a descriptive comparative analysis of a sample of eleven mobile apps, comprising an assessment of their alignment with evidence on nutrition, behaviour change and user quality, and their potential ability to support healthier food purchasing behaviour.
Sample
Due to the large number of dietary-related mobile apps available in GooglePlay( Reference Aitken and Lyle 54 ), it is not feasible to assess all available mobile apps. Instead, searches of GooglePlay in the Republic of Ireland were conducted to identify a sample of mobile apps that would most likely include mobile apps of good quality and of relevance to food purchasing behaviour. GooglePlay was chosen as it was the largest mobile application store and reported the most downloads at the time of the search( 55 ).
In stage one of the review process, six different searches were conducted in GooglePlay using search terms aimed to maximise the relevance to food purchasing behaviour: ‘healthy eating’, ‘healthy diet’, ‘healthy food’, ‘healthy shop’, ‘healthy food shop’ and ‘healthy food shopping’. The top 100 returns for each search were included in the initial sample. The top 200 mobile apps in the health and fitness category of GooglePlay were also included. The larger number was included from this category as it is less specific than the search terms. Any duplicates were removed. In stage two, each mobile app in the initial sample was assessed according to predefined exclusion and inclusion criteria (Table 2). Development of these criteria was informed by relevant literature and specific study requirements and were agreed in advance by the authors. Mobile app titles and descriptions were reviewed to assess relevance and mobile apps were excluded if they did not meet the required criteria. All remaining mobile apps were downloaded and briefly reviewed and subsequently excluded if they did not meet the required criteria (stage three). A subset of mobile apps was reviewed by co-authors to confirm the applicability of the inclusion and exclusion criteria. For marginal cases, the team reviewed the mobile app and an agreement was reached on its inclusion. The mobile app name, developer and reason for exclusion were recorded for all excluded mobile apps. All remaining mobile apps were included in the final sample and underwent further assessment (stage four). The name, developer, average rating in GooglePlay, total number of ratings and the number of installs were recorded.
Table 2 Inclusion and exclusion criteria for selection of mobile apps
Assessment criteria development
The final sample of mobile apps was assessed and scored according to specific criteria which were agreed in advance by all authors. Details on the development of the assessment criteria and relevant scoring system are outlined below.
Nutrition content
The quality of the nutrition information provided in each mobile app was assessed by a qualified nutritionist in comparison to the dietary guidelines for the Republic of Ireland( 56 , 57 ), and scored either 0 or 1. Mobile apps were given a score of 0 if any information did not adhere to these guidelines and was not based upon valid scientific evidence. The reasons for a mobile app achieving a score of 0 were noted. The content of social forums, in which users could communicate with each other, was briefly reviewed to assess the type of nutrition information being shared and confirm the presence of a forum moderator. This content did not contribute to the quality score as it was not feasible to review all such content, but notes were kept for each mobile app and analysed as part of the subjective assessments, as detailed below.
Behaviour change theory
The framework proposed by van’t Riet et al. ( Reference van’t Riet, Sijtsema and Dagevos 22 ) (Table 1) informed the development of the behaviour change theory assessment criteria to ensure techniques that address both routine and habitual elements of food purchasing behaviour were examined. Behaviour change techniques (BCT)( Reference Michie, Richardson and Johnston 58 ) were assigned to each strategy based on the descriptions provided by van’t Riet et al. ( Reference van’t Riet, Sijtsema and Dagevos 22 ). BCT are ‘observable, replicable, and irreducible component[s] of an intervention designed to alter or redirect causal processes that regulate behaviour’( Reference Michie, Richardson and Johnston 58 ) and provide a more informational and rigorous coding tool than previously used theory-based instruments( Reference Lyons, Lewis and Mayrsohn 59 ). The final set consisted of forty-eight BCT. A score of 1 was given for each technique observed in the mobile app, giving a potential total score of 48 for behaviour change theory.
User quality
The Mobile App Rating Scale (MARS)( Reference Stoyanov, Hides and Kavanagh 60 ) was used to assess mobile app quality. MARS is an objective measure for rating the quality of mobile health apps by assessing specific features shown to influence user interaction and mobile quality. Nineteen items are assessed across four different categories: engagement, functionality, aesthetics and information. All items within each category are measured on a 5-point scale with a higher score representing higher quality. A mean category score and a mean total quality score were calculated for each mobile app.
Subjective assessment
The primary author undertook a qualitative subjective assessment of each mobile app to ensure those features not assessed elsewhere were captured, such as offline accessibility, and to provide further insight to quantitative assessment scoring. An assessment of features was made based on those highlighted in the relevant literature.
Assessment procedure
The final sample of mobile apps (n 11) that met the inclusion criteria were downloaded for four days and scored against the assessment criteria by the primary author, a qualified nutritionist. A standard user profile was developed in advance of the assessment process and used during mobile app registration, where required. Data extraction, mobile app assessment and analysis were conducted between July and October 2016.
Inter-rater reliability
For the purpose of reliability, mobile apps were independently scored by a second reviewer. Scoring of BCT and user quality was undertaken by a colleague with experience in the area of food behaviour. Scoring of the nutrition content was undertaken by a registered dietitian. The assessment criteria were discussed with each reviewer to ensure an agreed understanding and clarify any ambiguous items. A pilot scoring exercise was conducted on two mobile apps, not included in the final sample, to assess initial understanding and inter-rating agreement. Disagreements were discussed and a consensus of understanding agreed prior to secondary review of the final sample of mobile apps. Upon completion of secondary coding, disagreements were resolved by discussion, and a final score was jointly agreed.
Analyses
The internal consistency of the MARS was calculated using Cronbach’s alpha( Reference Tavakol and Dennick 61 ). Krippendorff’s alpha was used to evaluate inter-rater reliability( Reference Hayes and Krippendorff 62 ). The total and median number of BCT integrated into the eleven selected mobile apps were calculated. The median was calculated for the overall MARS score, each of the MARS subscale scores and the nutrition content score. Spearman’s correlations were used to explore the relationships between behaviour change theory, user quality components and average user ratings provided in GooglePlay. All tests were carried out using the statistical software package IBM SPSS Statistics version 24 with significance level set at P<0·05. Content analysis, using NVivo version 11, was performed on the qualitative subjective assessment records in line with the approach proposed by Forman and Damschroder( Reference Forman and Damschroder 63 ).
Results
Mobile app selection
Figure 1 outlines the selection process for mobile apps, highlighting the reasons for exclusion at each stage. The most common reason for exclusion was lack of a specific aim to support healthier food behaviours (n 329; 61 %) with many focusing solely on physical activity (n 124). Table 3 outlines the key characteristics of the mobile apps selected for inclusion in the final sample.
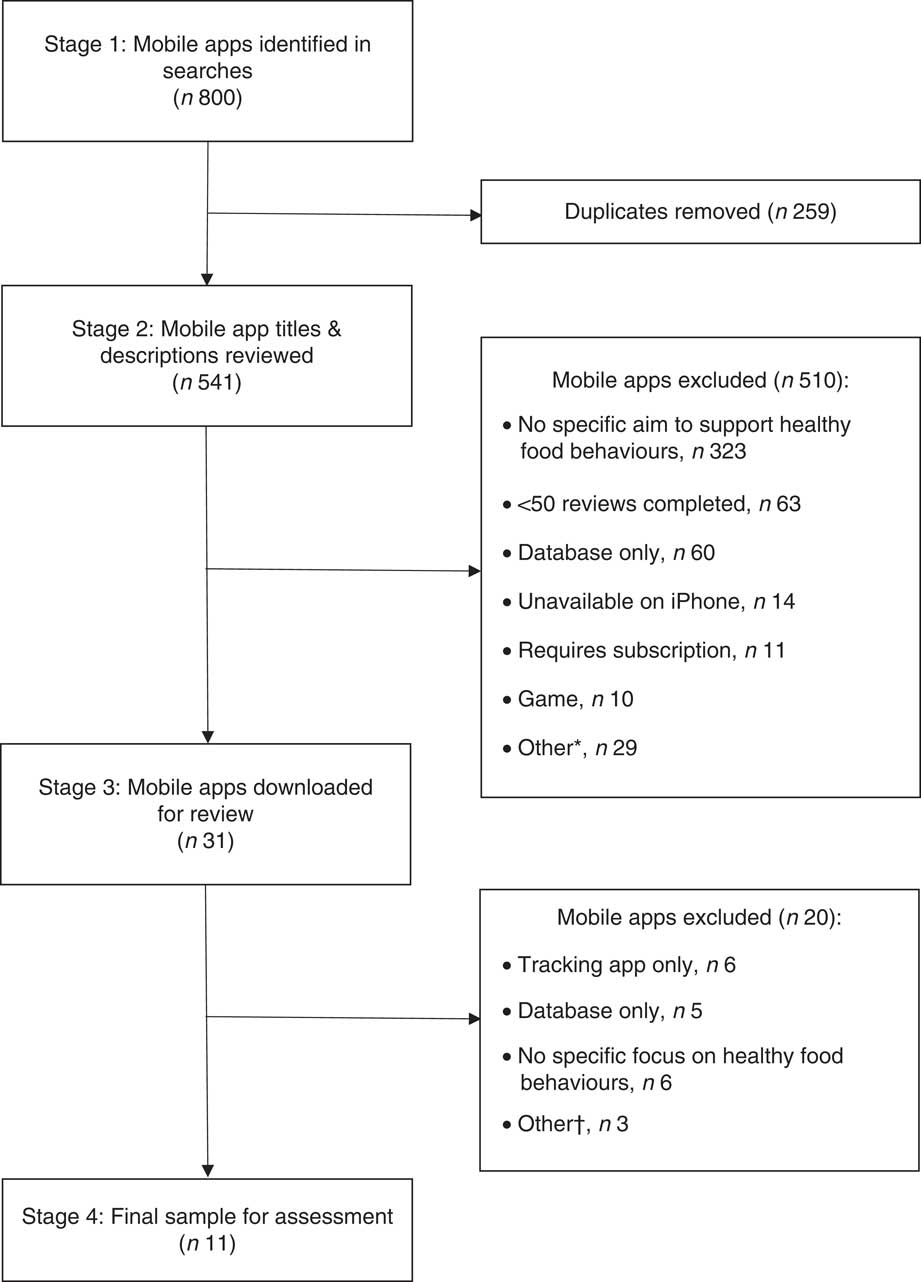
Fig. 1 Flowchart of the selection process for mobile apps. *Other reasons for exclusion: online shop (n 9); focus on specific group (n 5); main features not free (n 4); rating <3 stars (n 3); not available in English (n 3); tracking mobile app only (n 3); focus on eating out (n 1); online magazine (n 1). †Other reasons for exclusion: main features not free (n 2); error present in download (n 1)
Table 3 Key characteristics of mobile apps selected for inclusion in the final sample
Integration of behaviour change techniques
The reliability estimate for BCT coding was good (0·88). There was a distinct lack of focus on food purchasing behaviour in the selected mobile apps, with most focusing on behavioural outcomes such as weight management. Only one mobile app permitted goal setting directly related to food purchasing behaviour, with the majority of goal setting focusing on weight loss or energy intake. The most common feature directly related to food purchasing was the provision of a grocery list based on recommended meal plans, which may support behaviour change through conservation of mental resources; this feature was incorporated into four of the eleven mobile apps. The median number of BCT recorded in a mobile app was three and all selected mobile apps incorporated at least two techniques (Table 3). Table 4 outlines the BCT integrated in the selected mobile apps. The most popular techniques incorporated were goal setting (outcome of behaviour; n 11), self-monitoring of outcome(s) of behaviour (n 11), conserving mental resources (n 5) and behaviour substitution (n 5). The majority of BCT integrated focused on influencing the individual’s response or the performance cue (73 %; Table 1). Thirty-three of the forty-eight BCT in the assessment criteria were not integrated into any mobile app.
Table 4 Behaviour change techniques integrated into the selected mobile apps
Quality of nutrition content
The reliability estimate for nutrition content quality was good (0·80). The median nutrition score was 1. Four of the eleven selected mobile apps were scored 0 (Table 3). Information in these mobile apps focused on fad diets with no scientific basis, such as detox diets, and much of the nutrition information was provided by unqualified individuals, such as bloggers or brand representatives. While the majority of mobile apps attained a score of 1 and provided evidenced-based information, improvements are still required in relation to the quantity of information provided in some of the mobile apps. For example, feedback was often provided on dietary intake, such as highlighting that saturated fat consumption was higher than recommended levels. However, no information was provided subsequently on the foods consumed that contributed to this high intake. The setting of dietary goals was also an area where information was lacking. Many of the mobile apps allowed users to set dietary goals, such as energy or fat intake, but little guidance was given on appropriate goal setting, which may lead to unhealthier dietary practices. The nutrition information shared in the social forums generally focused on promoting branded diet programmes, supplements or weight-loss products, and recipe sharing. A forum moderator was apparent in only one of the mobile apps and provided evidenced-based nutrition information to users and corrected any misinformation being shared. The involvement of registered nutrition professionals in the development of the mobile apps was unclear and were cited as sources of information in only four mobile apps.
Integration of user quality components
The MARS total score had high internal consistency (0·87) and demonstrated good inter-rater reliability (0·84). Table 3 outlines the median overall MARS score and scores for each subscale. The lowest score was seen for engagement. Customisation is a key element of engagement and customisation options differed between mobile apps. While some offered users the option to customise meal plans to suit preferences or set personally relevant goals, others provided limited personalised options. The relationship between integration of user quality components, as rated by MARS, and the average rating provided by users in GooglePlay was examined and no correlation was evident (ρ=0·32; P=0·34).
Relationship between behaviour change theory integration and user quality components
Using MARS as a measure of user quality, no significant relationship was identified between integration of behaviour change theory and user quality (ρ=−0·114, P=0·67). The average rating provided by users in GooglePlay is another measure of user quality and no significant relationship was seen with integration of behaviour change theory (ρ=−0·58; P=0·06).
Subjective assessment
The subjective assessment analysis highlighted a number of issues. Seven of the eleven mobile apps were accessible offline (Table 3), although the quantity of offline content varied. This may influence the usability of the mobile app in the supermarket where Internet access may be limited. Reviewers noted that considerable time and effort were required to utilise many of the mobile apps, especially those focusing on self-monitoring of food consumption. There was a distinct lack of guidance on how to use the mobile apps and the user was required to navigate through the different sections to learn of its functions. It is possible that users may miss important features or use them inappropriately without instructions.
Discussion
Alignment of behaviour change theory, sound nutrition information and adequate user quality is proposed to be a necessary condition for successful behaviour change. The present study is the first time that existing mobile apps have been analysed in relation to these components, focusing specifically on healthier food purchasing behaviour. While findings highlight a number of positive characteristics that may facilitate behaviour change, there are many opportunities for improvement.
Mobile apps and healthy food purchasing behaviour
It is evident that there is a distinct lack of focus on food purchasing behaviour in existing mobile apps, with most directed at behavioural outcomes such as weight management. This is surprising, and disappointing, given that food purchasing represents a key step in the food choice decision-making process( 3 – 5 ). An overemphasis on behavioural outcomes may negatively influence the potential to effect change because setting interim learning goals is shown to be more effective than focusing solely on outcome goals, although supporting progression to achieve a behavioural outcome is most effective( Reference Latham and Brown 64 , Reference Zimmerman and Kitsantas 65 ). On a positive note, BCT were integrated into all mobile apps although the average of three techniques was lower than the average of ten reported in a similar study( Reference Bardus, van Beurden and Smith 66 ). This may be due to the difference in behavioural focus, with the latter focusing on multiple behaviours, including physical activity and food behaviours, rather than a single behaviour such as food purchasing behaviour. It is possible that existing mobile apps are better developed to address wider behavioural outcomes rather than specific food behaviours. Future development should give greater attention to food purchasing behaviour and support interim goal setting and subsequent progression to maximise potential effectiveness.
Analysis of the integrated BCT provided some interesting findings. The most popular techniques, goal setting and self-monitoring of behavioural outcomes, were similar to those found in other reviews( Reference Pagoto, Schneider and Jojic 43 , Reference Bardus, van Beurden and Smith 66 – Reference Direito, Dale and Shields 69 ). An important finding in the context of food purchasing behaviour is that the third most popular technique was conserving mental resources, which focuses on addressing the performance cue. As contextual cues play a key role in directing the habitual elements of food purchasing behaviour( Reference Wood and Neal 15 – Reference Wood, Tam and Witt 17 , 55 ), it is a promising development that such techniques are being integrated. Only a limited number of the relevant BCT were integrated into any of the mobile apps with a particular focus on influencing the individual’s response or the performance cue; this also reflects findings from elsewhere( Reference Chen, Cade and Allman-Farinelli 68 , Reference Zahry, Cheng and Peng 70 ). Such approaches may not be wholly effective for all users and techniques addressing behavioural reinforcement may also be appropriate( Reference Zahry, Cheng and Peng 70 ). Similar to other reviews, the extent of integration varied from two to fourteen techniques( Reference Pagoto, Schneider and Jojic 43 , Reference Zahry, Cheng and Peng 70 , Reference Azar, Lesser and Laing 71 ). As Webb et al. ( Reference Webb, Joseph and Yardley 72 ) found that Internet-based interventions had a greater effect if they incorporated a greater number of techniques, it may be a positive progression that a greater number of techniques are being integrated. However, it is unknown if this is valid for mobile apps and it is possible that integration of too many may complicate use of the mobile app and negatively influence the user experience. Future research should explore the integration of additional and alternative BCT to ensure the complex nature of changing food purchasing behaviour is addressed. The subsequent impact on the user experience is an important consideration, with a need to identify the optimal level required to effect change with minimal negative impact on acceptability.
From an initial sample of 541, only eleven mobile apps were eligible for inclusion in the final sample. While inclusion criteria aimed to identify those rated as higher quality and of greater relevance to healthier food purchasing behaviour, it was unexpected that so few matched the criteria. The most common reason for exclusion was a lack of focus on healthy food behaviours despite the use of specific search terms on food and healthy eating. As consumers may use the name as a cue of its relevance to their goals, it may prove challenging to identify an appropriate mobile app and will require time and effort. There is a need to examine how consumers select mobile apps and where information on effectiveness and relevance could be shared.
Quality of nutrition content
Nutrition content quality was good, with many citing valid evidence sources or engaging a nutrition professional to provide information. However, despite inclusion criteria to identify mobile apps of higher quality, four of the eleven mobile apps provided nutrition information that was inadequate. All of these achieved a user rating score >4 in GooglePlay, suggesting they are viewed as being of good quality by users. Indeed, the high rating assigned to the mobile app may be a cue used by consumers to inform their decision on which are likely to be most effective. It is important to understand the cues that consumers use to assess mobile app quality to ensure users are directed towards those based upon valid scientific evidence, to reduce potential negative outcomes. As previously discussed, little instruction was offered to users of the mobile apps included in the present review. Consequently, it is likely that a reasonable standard of nutrition knowledge is required for their effective use. Expecting users to set weight loss or energy goals in the absence of relevant guidance is inappropriate and may lead to inappropriate goal setting, potentially resulting in unhealthy dietary practices( Reference Franco, Fallaize and Lovegrove 73 , Reference Lieffers, Haresign and Mehling 74 ). Similar criticisms have been raised elsewhere( Reference Chen, Cade and Allman-Farinelli 68 , Reference Franco, Fallaize and Lovegrove 73 ) and highlight the need for mobile apps to facilitate the building of nutrition knowledge and skills rather than work on the assumption that they are present. Furthermore, allowing users to share information in social forums may be a useful means of offering social support, but in the absence of a forum moderator inaccurate nutrition information may be shared and contribute to unhealthier dietary behaviours. There is a clear need to engage nutrition professionals at all stages of design and delivery to ensure content is accurate and appropriate to support healthy behaviour change( Reference Franco, Fallaize and Lovegrove 73 , Reference Con and De Cruz 75 ).
Integration of user quality components
The selected mobile apps were of good user quality, in line with similar reviews( Reference Bardus, van Beurden and Smith 66 , Reference Chen, Cade and Allman-Farinelli 68 ), although there are still areas for improvement especially in relation to engagement and information. As outlined previously, some mobile apps provided limited customisable options which may reduce their usefulness for some. Mass customisation, the ability for consumers to tailor a product to their specific needs, has become a popular marketing strategy in recent decades in an attempt to better meet consumer needs( Reference Blecker and Abdelkaf 76 ). While this approach can improve the user experience, it may also increase user burden which may impact negatively on the user experience( Reference Blecker and Abdelkaf 76 – Reference Chang and Chen 78 ). A staged approach to customisation may alleviate some of this burden while still allowing for personalisation( Reference Sigala 79 ). User engagement is required to identify optimal levels of customisation to meet their needs and support a positive experience( Reference Piller, Schubert and Koch 77 ). An important critique was the time and effort required to use the mobile apps adequately. Such a high level of involvement requires high user motivation which may not be realistic and may negatively impact on the user experience and continued use because motivation and time availability fluctuate over time. There is a need to explore alternative, less burdensome options for self-monitoring to improve the quality of the user experience.
It is important to highlight that no significant relationship was seen between the MARS score for user quality and the average user rating in GooglePlay, although the small sample size upon which this is based must be acknowledged. Azar et al. ( Reference Azar, Lesser and Laing 71 ) reported similar results, although they did not use MARS as a measure of quality. This discrepancy may be due to differences between users and researchers in the assessment of quality, such as nutrition information. The quality of nutrition information was considered inadequate in some mobile apps, contributing to a lower information quality score. However, these mobile apps were rated highly by users in GooglePlay. It is possible that the nutrition information was viewed positively by users as it was congruent with their existing beliefs, but objectively such information is of a lower standard. Furthermore, measures such as user trust, ability and confidence are shown to be important( Reference Lowe, Fraser and Souza-Monteiro 26 , Reference Chang, Kaasinen and Kaipainen 46 , Reference Lee and Ha 80 ) and it is possible that MARS does not currently capture these factors adequately. User engagement at all stages of development is important to understand the factors which influence the user experience and mobile app acceptability( Reference Yardley, Morrison and Bradbury 81 ).
Limitations
The present study was not a review of all mobile apps currently available and it is possible that some relevant mobile apps may be missing. It is estimated that greater than 165 000 health and fitness mobile apps are available and it is not feasible to review all adequately. Consequently, the aim was to identify and highlight some of the issues present in existing mobile apps in relation to food purchasing behaviour to subsequently inform mobile app and intervention design.
Our selection was restricted to mobile apps publicly available in the Republic of Ireland and it is possible that relevant mobile apps are available elsewhere. For example, the FoodSwitch mobile app( Reference Dunford, Trevena and Goodsell 82 ), which aims to provide easy-to-understand nutritional information on food purchasing choices and recommend healthier alternatives, is currently unavailable in the Republic of Ireland and could not be included in our review. Additional relevant mobile apps may be available elsewhere which address some of the issues highlighted herein. Engagement with the relevant organisations is recommended to support their wider introduction.
The present review was undertaken by health and nutrition researchers who are not likely to be the target group for a mobile dietary intervention. Consequently, their scoring of the mobile apps, while displaying good reliability, may not correspond with scoring undertaken by an intended user group. While this analysis highlights issues from the perspective of nutrition and health professionals, there is a need to explore the importance of these components with intended user groups and assess their influence on mobile app acceptability and adoption.
Conclusions
The present study is the first to assess nutrition information quality and the integration of behaviour change theory and user quality in existing mobile apps in relation to food purchasing behaviour. It illustrates that supporting healthier food purchasing behaviour is often not a core component of existing mobile apps. Despite this, existing mobile apps do offer the potential to effect change in food purchasing behaviour and design improvements may improve such potential effectiveness. Furthermore, engagement of nutrition professionals in mobile app design is necessary to address potential issues relating to accuracy and appropriateness, to ensure mobile apps support a healthy behaviour change process. The apparent narrow focus towards behaviour change with an overemphasis on behavioural outcomes and a limited number of BCT must be addressed to ensure they are relevant for a wider user group. The integration of alternative techniques may be beneficial although consideration must be given to the complexity this may add and their potential impact on the user experience. User engagement is crucial to gain a better insight into these issues and inform future development.
Acknowledgements
Acknowledgements: The authors wish to thank Jessica Finn, Aoife Harvey, Leah Hegarty and Elaine Walsh for their support during the mobile app assessment stage. Financial support: This work was supported by the HRB Centre for Health & Diet Research (grant reference HRC/2014/13) and conducted as part of the SPHeRE Programme (grant number SPHeRE/2013/1). The funders had no role in the design, analysis or writing of this article. Conflict of interest: The authors declare that there are no conflicts of interest. Authorship: S-J.F., M.McC., A.C. and F.McA. worked on the study design and methods. S-J.F. was responsible for data collection and analysis and M.McC. and A.C. supervised analysis. S-J.F. wrote the paper and all authors provided feedback and approved the final manuscript. Ethics of human subject participation: Not applicable.





