


Overweight and obesity are major public health problems leading to an increased risk of non-communicable diseases( Reference Cecchini, Sassi and Lauer 1 ). The prevalence of obesity and associated co-morbidities among children and adolescents has risen worldwide throughout the past three decades( Reference Wiegand, Bau and Babitsch 2 ). It has been estimated that 10 % of schoolchildren are overweight and a quarter of them are obese worldwide, whereas in Europe and America the prevalence is above 20 %( Reference Lobstein, Baur and Uauy 3 ). Obese children are not only at risk for becoming obese adults( Reference Singh, Mulder and Twisk 4 ), they are also more likely to suffer from psychosocial problems, lower academic achievement and premature death( Reference Singh, Yu and Siahpush 5 , Reference Singh, Uijtdewilligen and Twisk 6 ).
The global rise in obesity prevalence, particularly in children, is too rapid to be explained by changes in genetic structure; therefore environmental factors are assumed to play an important role in the development of obesity risk behaviours( Reference Sahingoz and Sanlier 7 ). High availability of high-energy foods along with limited opportunities to be physically active, the so-called ‘obesogenic environment’, is typical for Western European societies and is likely to promote excessive weight gain( Reference Nicolaou, Benjelloun and Stronks 8 ).
It has been shown that non-Western immigrants living in Western societies are more often overweight and obese than non-Westerners who live in their country of origin( Reference Nicolaou, Doak and van Dam 9 ). A recent study conducted among schoolchildren in Europe showed that immigrant adolescents are more often overweight than native adolescents( Reference Brug, van Stralen and Chinapaw 10 ). The non-Western immigrant population (e.g. from Turkey, Morocco, Surinam, Antillean, Iraq and Iran) forms the majority of migrants in the Netherlands( Reference Brussaard, van Erp-Baart and Brants 11 ). Kleiser et al.( Reference Kleiser, Mensink and Neuhauser 12 ) showed considerable differences in dietary habits between young persons coming from different origins living in the Netherlands. Previous studies showed that the overweight prevalence of Turkish children living in the Netherlands is high with gender differences (in boys 23 %, in girls 30 %) and that unfavourable energy balance-related behaviours (EBRB), i.e. food intake, physical activity (PA) and sedentary behaviour, are common in this group( Reference Fredriks, Buuren and Sing 13 – Reference Van Vuuren, Stegeman and Van Dieren 15 ). Participation in PA has a strong socio-economic and ethnic gradient, with children of low socio-economic status or from an ethnic minority being less likely to participate in regular PA than their more advantaged counterparts( Reference Crespo, Ainsworth and Keteyian 16 , Reference Lowry, Kann and Collins 17 ). Dutch children living in socio-economically deprived areas seem to have the lowest levels of PA and the highest rates of overweight( Reference Zeijl, Crone and Wiefferink 18 , Reference De Vries, Bakker and van Overbeek 19 ). Considering such a large Turkish immigrant population (i.e. 21 % of the non-Western immigrants), it is important to know their health behaviours and obesity and overweight patterns in order to reduce health inequalities. Exploring the potential influences of migration on weight status and related risk factors is possible by comparing immigrant adolescents with their peers living in Turkey. To the best of our knowledge, there is no study that has compared weight status and related risk behaviours of Turkish immigrant adolescents and their non-migrant compatriots in Turkey. The current study aimed to compare the EBRB, measures of body composition and prevalence of overweight/obesity between Turkish adolescents in Turkey and Turkish immigrant adolescents in the Netherlands.
Methods
In the current study we used cross-sectional data from one Turkish survey and six Dutch studies with data on weight status and EBRB. All studies are compatible with regard to the study population, measures of body composition and assessed EBRB.
Participants
For the Turkish data set (TR-TR), a total of 915 (49 % girls) adolescents were randomly selected from healthy primary-school children living in Ankara, Turkey. For the Dutch data (TR-NL), a total of 433 (51 % girls) adolescents from primary and secondary schools from six different studies were included: i.e. DOiT (n 32), DOiT AGAIN (n 38), ENDORSE (n 106), ENERGY (n 24), JUMP-In (n 158) and Pro-Children (n 75)( Reference Singh, Chin and Paw 20 – Reference Van der Horst, Oenema and Van de Looij-Jansen 24 ). From these Dutch data sets adolescents with a Turkish ethnicity (i.e. at least one of the parents was born in Turkey) were selected for data analysis. Data were collected in DOiT in 2003, DOiT AGAIN in 2010, ENDORSE in 2005/2006, ENERGY in 2011, JUMP-In in 2006, Pro-Children in 2003 and the Turkish survey in 2010.
Participation of adolescents in these different studies was voluntary. The response rates for both studies were similar, as for the TR-NL studies it varied from 79 % to 90 % and for the TR-TR study it was 82 %. Adolescents and their parents were informed about the objectives and methods of the studies and signed an informed consent form. The relevant ethical medical committees approved each study protocol. The inclusion criteria for the TR-TR study were to be healthy and to attend school regularly. In the TR-TR study the adolescents were recruited from three different public schools and had similar socio-economic levels.
Anthropometric measurements
Body weight (kg), body height (cm), waist and hip circumferences (cm), and triceps, biceps, suprailiac and subscapular skinfold thicknesses (mm) were measured using standard measurement protocols. There were some differences with regard to the measurement techniques between included studies, e.g. measuring children's body weight with clothes (ENDORSE) or in underwear (JUMP-In, DOiT, DOiT AGAIN), repeating the measurements two times (ENERGY, DOiT) or having only one measurement (JUMP-In). The detailed measurement techniques of each study are described in the online supplementary material.
BMI was calculated as body weight (kg) divided by body height squared (m2). Skinfold thickness measurements were summed. The definitions of overweight and obesity were based on age- and gender-specific BMI cut-off points for children and adolescents published by Cole et al.( Reference Cole, Bellizzi and Flegal 25 ). Waist:hip ratio was calculated by dividing waist circumference by hip circumference.
Energy balance-related behaviours
EBRB included in the current study were: soft drink and fruit juice consumption (ml/d), fruit and vegetable (F&V) intake (g/d), breakfast frequency, daily PA (min) and screen time (min). Information on EBRB was collected by self-report questionnaires in all studies. Table 1 shows the available data on EBRB per study. The specific questions used in each study are provided in the online supplementary material.
Table 1 Available study variables by database per country
TR-NL, adolescents from Turkish immigrant ethnicity living in the Netherlands; TR-TR, Turkish adolescents in Turkey; TV, television.
Soft drink and fruit juice consumption
In Turkey and the Dutch Pro-Children study, data on soft drink and fruit juice consumption were collected using a 24 h dietary recall, i.e. amount of consumption on the day prior to the day of investigation. In the other studies data were collected by an FFQ recalling the frequency of consumption per a usual week and the amount per day, the same as in a Belgian study( Reference Vereecken and Maes 26 ). Consumption of soft drinks and fruit juice was summed to calculate total sugar-containing beverage (SCB) consumption. SCB consumption of more than 5000 ml/d was considered as unrealistic and excluded from further data analysis.
Fruit and vegetable intake
The data on F&V intake were collected only in two studies, i.e. the TR-TR study and the Pro-Children study. In Turkey and in the Dutch Pro-Children study, data on F&V intake were collected using a 24 h dietary recall, i.e. number of portions consumed on the day prior to the day of investigation.
Breakfast frequency
In both Turkey and the Netherlands, breakfast frequency per week was assessed. In the Netherlands breakfast consumption was assessed separately for weekdays and weekend days. The variable was dichotomized as having breakfast every day or not.
Physical activity
In Turkey, PA recalls for three consecutive days were taken. The average time spent walking per day was calculated by the recalls. In the Dutch data sets, time spent in PA was collected differently in the different studies. The Pro-Children study recalled the duration of exercising in leisure time by one question; other studies assessed the frequency and time spent in active commuting to school, sports club activities and unorganized sport activities (DOiT, DOiT AGAIN, ENERGY); and in ENDORSE the frequency and duration of sport activities engaged in during the past week were recalled (see online supplementary material).
Total screen time
Total screen time was calculated as sum of television (TV) viewing time and computer time and expressed in minutes per day. In both countries the frequency (in a usual week) and duration of TV watching and computer use per day were recalled. In Turkey, ENDORSE, ENERGY and DOiT AGAIN, playing electronic games was specifically mentioned in the question as an example of computer use.
Data analysis
All data analyses were carried out using the statistical software package SPSS version 15·0. We investigated the effect of country, gender and their interaction due to earlier evidence on gender differences in weight status( Reference Fredriks, Buuren and Sing 13 ). In the case of significant effects of gender by country interaction, the results were reported separately for girls and boys. We applied pairwise comparisons according to gender and country using ANCOVA to test group differences in EBRB. In ANCOVA the differences between groups were tested adjusting for covariates. Differences between groups in categorical outcomes (overweight status, daily breakfast consumption) were tested with logistic regression analyses.
Due to the variation in applied measurement methods in the different Dutch studies, we added a variable ‘study cohort’ as a covariate in the ANCOVA models (when there was more than one Dutch study per outcome). Furthermore, age and body height (when waist circumference was an outcome) were added as covariates in the ANCOVA models, both in the total group and also in gender group analyses. Gender was added as a covariate in the total group analyses. The level of significance was set as P < 0·05.
Results
In total, 469 boys and 446 girls living in Turkey (TR-TR) aged between 11 and 14 years (mean age 13·1 (sd 0·8) years) and 211 boys and 222 girls with at least one parent born in Turkey, living in the Netherlands (TR-NL) and aged between 10 and 14 years (mean age 11·7 (sd 1·3) years) were included. This age difference between the study samples was statistically significant (Table 2).
Table 2 Gender- and country-specific age and anthropometric characteristics of Dutch-Turkish (TR-NL) and Turkish-Turkish (TR-TR) adolescents

Data are presented as mean and standard deviation unless otherwise stated. Data analyses were adjusted for age (all except age) and cohort (all except skinfold measures, due to having one cohort per country for this outcome), height (only for waist circumference and waist:height ratio) and gender (only for the total group comparison). ANCOVA and logistic regression (for overweight and obese percentages) were used for testing the differences between countries.
*Mean values were significantly different from those of the TR-TR group: P < 0·05.
Measures of body composition and overweight/obesity prevalence
Mean age-adjusted body weight, BMI, waist circumference and suprailiac skinfold thickness were significantly higher in the TR-NL group than in the TR-TR group (Table 2), while the mean age-adjusted body height and hip circumference were significantly higher in the TR-TR group compared with the TR-NL group (all P < 0·05). Overweight and obesity were more prevalent in adolescents living in the Netherlands (31 % and 9 %, respectively) than in adolescents living in Turkey (26 % and 6 %, respectively; P < 0·05; Table 2). Stratification by gender resulted in similar differences between the TR-TR and TR-NL groups, except that the difference in hip circumference and triceps skinfold thickness was smaller and not significant among girls, while differences in subscapular skinfold, sum of skinfolds, waist circumference, overweight and obesity were smaller and not significant in boys (Table 2).
Energy balance-related behaviours
Dietary behaviours
Daily average SCB consumption was approximately ten times higher in TR-NL than TR-TR adolescents (TR-NL: 1173 (sd 769) ml/d, TR-TR: 115 (sd 211) ml/d; P < 0·05). The total F&V intake was significantly higher in TR-TR than TR-NL adolescents (TR-TR: 647 (sd 409) g/d, TR-NL: 295 (sd 293) g/d; P < 0·05). The proportion of adolescents reporting to eat breakfast daily was similar in both groups (TR-NL: 52 %, TR-TR: 54 %). Stratified analysis by gender yielded similar results, except the difference in fruit intake was smaller and not significant among boys (Table 3).
Table 3 Energy balance-related behaviours of Dutch-Turkish (TR-NL) and Turkish-Turkish (TR-TR) adolescents
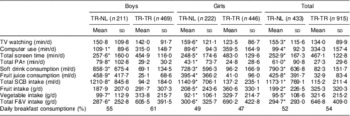
TV, television; PA, physical activity; SCB, sugar-containing beverage; F&V, fruit and vegetable.
Data are presented as mean and standard deviation unless otherwise stated. Data analyses were adjusted for age (for all), cohort (except for fruit, vegetable and total F&V intakes, due to having one cohort per country for these outcomes) and gender (only for the total group comparison). ANCOVA and logistic regression (for daily breakfast consumption) were used for testing the differences between countries. Total SCB consumption variable was log-transformed in the ANCOVA model due to non-normal distribution of the residuals.
*Mean values were significantly different from those of the TR-TR group: P < 0·05.
†Walking, biking, sports.
‡Having breakfast every day.
Physical activity
Table 3 shows the average PA levels. Total PA time was higher in the TR-NL than the TR-TR group (TR-NL: 61 (sd 91) min/d, TR-TR: 27 (sd 30) min/d; P < 0·05). Stratified analysis by gender gave similar results.
Screen time
Total self-reported screen time was significantly lower in the TR-NL adolescents (253 (sd 167) min/d) compared with the TR-TR adolescents (467 (sd 123) min/d; P < 0·05). Computer time was also significantly lower in TR-NL adolescents than TR-TR adolescents, whereas TV time was significantly higher in TR-NL adolescents (P < 0·05; Table 3). Stratified analysis by gender yielded similar results, except the difference in TV time was not significant among boys.
Discussion
The present study examined differences in measures of body composition, overweight/obesity status and a selection of EBRB between Turkish adolescents living in Turkey and Turkish immigrant adolescents living in the Netherlands. Overweight and obesity rates were significantly higher among Turkish adolescents living in the Netherlands (TR-NL) compared with their peers living in Turkey (TR-TR). The TR-NL adolescents reported significantly higher SCB consumption and lower F&V intake. Furthermore, TR-NL adolescents reported higher PA levels but less screen time and computer use.
The mechanisms underlying the high prevalence of obesity are complex and multifactorial( Reference Swinburn, Egger and Raza 27 ). Many immigrant groups of non-Western origin living in Western societies have high levels of overweight/obesity( Reference Zeijl, Crone and Wiefferink 18 , Reference Van den Berg, Van Eijsden and Vrijkotte 28 ). The high rates of overweight and obesity among immigrant adolescents may reflect a response to their obesogenic environment; migrants’ behaviour is likely to be influenced by their socio-cultural and physical environment( Reference Kirchengast and Schober 29 ). On the one hand, the physical environment is likely to be the first element changing the behaviour of immigrants and changes in availability and accessibility of facilities might influence participation in EBRB( Reference Swinburn, Egger and Raza 27 ). On the other hand, changes in social and cultural norms also influence food intake and PA patterns of immigrants. Acculturation – the process of coherence to the host culture that occurs with migration – influences diet, PA and preferences of body size of immigrants( Reference Nicolaou, Doak and van Dam 9 ). This acculturation can positively influence health and related behaviours. However, behavioural change of migrants is not always in a positive way and not in the same direction for all behaviours (either healthy or less healthy changes)( Reference Nicolaou, Doak and van Dam 9 ). The act of immigration may also affect health, since it may be stressful with negative psychosocial impacts. These influences may explain our finding that Turkish immigrant adolescents in the Netherlands reported less favourable dietary habits, reflected in drinking significantly more SCB and eating less F&V, compared with Turkish adolescents living in Turkey. A recent study including eight European countries showed that Dutch adolescents reported the highest quantities of soft drink consumption( Reference Brug, van Stralen and Te Velde 30 ). Thus, Turkish immigrant adolescents in the Netherlands may be influenced by the social norm and peer modelling of consuming much SCB or the high availability of SCB in the Netherlands. Regarding the differences in F&V intake, in Turkey it is traditional in families to serve fruits after dinner. Among OECD (Organisation for Economic Co-operation and Development) countries, numbers from Turkey indicate very high levels of F&V consumption( Reference Srinivasan, Irz and Shankar 31 ) and this may reflect the dietary habits of Turkish families living in Turkey. A recent study indicated that among Dutch children daily average F&V intake was 224 g in girls and 218 g in boys( Reference Fischer, Brug and Tak 32 ). This shows that Turkish immigrant children report higher F&V intake than Dutch children but lower F&V intake than Turkish children in Turkey.
Turkish adolescents living in the Netherlands reported significantly lower screen times. Among the TR-TR group computer time (average 334 min/d) was significantly higher than in TR-NL adolescents (average 99 min/d), while TV time (average 134 min/d in TR-TR) was significantly higher in TR-NL adolescents (average 155 min/d). Computer use in Turkey became widespread especially after the 1990s and has continued to increase rapidly since the beginning of the 2010s( 33 ). A recent study showed that most high-school adolescents (67 %) use Internet cafés to play computer games, chat and surf the Internet; boys prefer going to such places more than girls in Turkey( Reference Gurol and Sevindik 34 ). Gathering to play multi-player games in Internet cafés is way of socializing with friends and increases the computer time of Turkish children( Reference Karakus, Inal and Cagiltay 35 ). Cultural and/or parental rules for watching TV as well as the accessibility of other competing/concurrent media like computers may influence the amount of time young people spend watching TV( Reference Tahiroglu, Celik and Uzel 36 ). Results of the ENERGY study suggest that non-native Dutch children spend more time in screen activities than natives (157 min/d in non-natives v. 118 min/d in natives)( Reference Brussaard, van Erp-Baart and Brants 11 ). This indicates that Turkish immigrant children report higher screen time than Dutch children but lower screen time than Turkish children in Turkey.
TR-TR adolescents reported significantly lower PA levels than TR-NL adolescents. A recent European study showed that Dutch adolescents are among the most active in Europe, especially with regard to active transportation( Reference Brug, van Stralen and Te Velde 30 ). Adolescents may learn from others by observing, thus social support and social network from friends/family and schools may influence being active( Reference Ståhl, Rütten and Nutbeam 37 ). Turkish immigrant adolescents in the Netherlands might be influenced by the high social norm of active transportation from/to school and the active transportation facilities (e.g. separate bicycle lanes) in the Netherlands. However, Dutch adolescents from Turkish ethnicity are still less active than native Dutch adolescents( Reference Fredriks, Buuren and Sing 13 ).
Our results confirmed that dietary, PA and sedentary habits are influenced by the physical environment and the social and cultural norms.
Strengths and limitations
This comparison study in a large sample of adolescents is unique. We had data from Turkish immigrant adolescents from several different cities in the Netherlands where the majority of the Turkish immigrant population lives, improving the generalizability of our findings. Furthermore, we had objectively measured anthropometric data. A weakness of the study is the different measurement instruments used, especially with regard to the self-reported measures. Differences between countries might partly be explained by the assessment methods. The differences in total PA measurement methods may cause underestimation of total PA in some cohorts. Furthermore, EBRB were assessed by self-report, thus suffering from recall bias and socially desirable answers. When interpreting findings it should be kept in mind that differences in the data collection period (i.e. Dutch surveys between 2003 and 2011, Turkish survey in 2010) may have influenced the results. For example, the result from current surveys, i.e. having significantly more screen time and F&V consumption among TR-TR children, may reveal the ongoing behaviour change among children in the last years. Furthermore, results from the comparison of F&V intake that is limited to two studies and skinfold thickness measurement that is sensitive for inter-observer variation need to be interpreted more carefully.
Conclusion
The important limitations mentioned above should be firmly kept in mind in drawing conclusions from the present study. In conclusion, Turkish immigrant adolescents in the Netherlands showed higher levels of overweight and distinct patterns of EBRB. The results further suggest that their dietary patterns were less favourable than their peers living in Turkey while their PA and screen time were more favourable. These findings suggest that Turkish immigrant adolescents in the Netherlands have an orientation towards their host culture, influenced by the socio-cultural environment they live in. This might result from the process of acculturation and integration into the Dutch culture. We should also encourage TR-NL children to consume more F&V like their Turkish counterparts. Furthermore, TR-NL children should be encouraged to consume fewer soft drinks. To reduce disparities and health inequalities in the Netherlands, it is important to understand the social and physical environmental factors that contribute to overweight and obesity among immigrant adolescents.
Acknowledgements
Sources of funding: The contribution of G.A. was funded by the ERASMUS programme at Gazi University and M.Y. was funded by Wereld Kanker Onderzoek Fonds (WCRF NL 2008/65), as part of the World Cancer Research Fund international grant programme. M.M.v.S. was financially supported by a fellowship of the EMGO Institute for Health and Care Research. The DOiT intervention was funded by the Netherlands Heart Foundation (NHF-2000Z002). The Jump-In study was supported financially by the Public Health Fund and the Ministry of Health, Welfare and Sport. The ENERGY project was funded by the Seventh Framework Programme (CORDIS FP7) of the European Commission, HEALTH (FP7-HEALTH-2007-B; grant agreement no. 223254) and was additionally supported by a grant from the Netherlands Organization for Health Research and Development (grant no. 50-50150-98-002). The contribution of the Pro-Children study was funded by the Commission of the European Communities, specific RTD Programme ‘The Quality of Life and Management of Living Resources’ (QLK1-2001-00547). The ENDORSE study was funded by a grant from ZonMw, the Netherlands Organization for Health Research and Development (grant ID no. 2100.0103). The funders had no role in the design, analysis or writing of this article. Conflicts of interest: The authors declare that they have no conflicts of interest. Ethical approval: The DOiT, DOiT AGAIN, JUMP-In and ENERGY studies were approved by the Medical Ethics Committee of the VU University Medical Center. The ENDORSE and Pro-Children studies were approved by the Medical Ethics Committee of Erasmus University Medical Center. The Turkish study was approved by the Scientific Advisory Committee of Gazi University, Faculty of Health Sciences. Authors’ contributions: A.S.S., S.J.t.V., J.B., A.O., J.S.B.d.M. and M.J.M.C. are the principal investigators of the included Dutch studies. N.S., N.A.-T., G.A., S.B., M.G.-K., E.K. and H.Y. designed the Turkish study and collected the data. G.A. and M.Y. analysed the data and wrote and revised the manuscript, All authors advised with results and conclusions, reviewed the manuscript and contributed at multiple revisions.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1368980013003388




