


Sugar-sweetened beverages (SSB) are beverages that contain added sugars, such as soft drinks (e.g. soda, cola, orangeade, etc.), fruit drinks, energy drinks, sports drinks, teas and coffees with added sugar, vitamin waters and slushies(1). Their consumption is associated with many health problems such as overweight/obesity among children and adolescents(Reference Malik, Schulze and Hu2,Reference Bleich and Vercammen3) , type 2 diabetes(Reference Malik, Popkin and Bray4,Reference Imamura, O’Connor and Ye5) and dental caries(Reference Bleich and Vercammen3), making their consumption a major public health issue worldwide(Reference Lustig, Schmidt and Brindis6). SSB have no nutritional advantages and may contribute to excessive energy intake(7). A daily intake of more than one portion (12 oz or 355 ml) of SSB is associated with increased health risks(Reference Malik, Popkin and Bray4). SSB are the principal source of sugar intake among adolescents in the UK (aged 13–18 years)(Reference Ng, Ni Mhurchu and Jebb8), in Mexico (aged 12–19 years)(Reference Sanchez-Pimienta, Batis and Lutter9), in the USA (aged 9–18 years)(Reference Bailey, Fulgoni and Cowan10) and in Canada (aged 9–18 years)(Reference Langlois, Garriguet and Gonzalez11). In the USA, the mean intake of soft and fruit drinks is 606 ml/d among adolescents (aged 13–18 years)(Reference Popkin12). In Canada, boys and girls (aged 14–18 years) drink, respectively, 574 and 354 ml/d of soft and fruit drinks(Reference Garriguet13). Water represents an attractive alternative to SSB as its consumption is linked to lower risks of overweight and obesity among children and adolescents(Reference Muckelbauer, Barbosa and Mittag14). Unfortunately, data from Australia(Reference Sui, Zheng and Zhang15), the UK(Reference Vieux, Maillot and Constant16), the USA(Reference Drewnowski, Rehm and Constant17) and Canada(Reference Roche, Jones and Majowicz18) suggest that the daily water consumption of children and adolescents is below levels recommended by public health authorities. There is thus a need to target adolescents in public health interventions aimed at reducing SSB consumption to favour the development of healthy habits that could be maintained throughout life(19).
To successfully reduce SSB consumption, it is essential that interventions target factors associated with this behaviour(Reference Bartholomew Eldredge, Markham and Ruiter20,Reference Michie, Atkins and West21) . The Theory of Planned Behaviour (TPB)(Reference Ajzen22) and its more recent version the Reasoned Action Approach (RAA)(Reference Fishbein and Ajzen23) are psychosocial theories that have both been particularly useful to predict intention and adoption of health behaviours(Reference McEachan, Taylor and Harrison24), including nutrition-related behaviours among adolescents(Reference Riebl, Estabrooks and Dunsmore25). Figure 1 presents the theoretical framework used in our study. According to the RAA, behaviour is influenced by intention, which reflects the level of motivation towards engaging in this behaviour, and perceived behavioural control (PBC), which refers to autonomy and capacity to adopt the behaviour. Intention is defined directly by three variables (i.e. direct constructs): (1) attitude (i.e. a subjective analysis of the advantages and disadvantages of adopting a behaviour), (2) perceived norm (i.e. the perceived social pressure to engage in a behaviour) and (3) PBC. Each of these factors is associated with a specific set of indirect beliefs (i.e. indirectly predicts intention through the direct constructs): attitude is linked to behavioural beliefs, perceived norm to normative beliefs and PBC to control beliefs (barriers and facilitating factors). In cases where intention is a determinant of behaviour, the RAA recommends identifying its own determinants and indirect beliefs to inform the development of motivational behaviour change interventions. According to the RAA, variables related to the sociodemographic, historical, cultural or environmental context of individuals usually do not directly affect their intention or behaviour but rather influence the beliefs and other variables of the theory. Since the RAA is open to the inclusion of other variables, self-identity was included as a potential predictor of intention. Self-identity refers to the enduring characteristics that people attribute to themselves, as part of their self-concept (i.e. how people perceive themselves)(Reference Sparks and Guthrie26). In a meta-analysis of the TPB, self-identity showed a sample-weighted correlation of 0·47 with intention for various health behaviours, such as healthy eating among students(Reference Rise, Sheeran and Hukkelberg27). Self-identity explained an additional 6 % of the variance in intention after controlling for TPB variables and past behaviour(Reference Rise, Sheeran and Hukkelberg27).
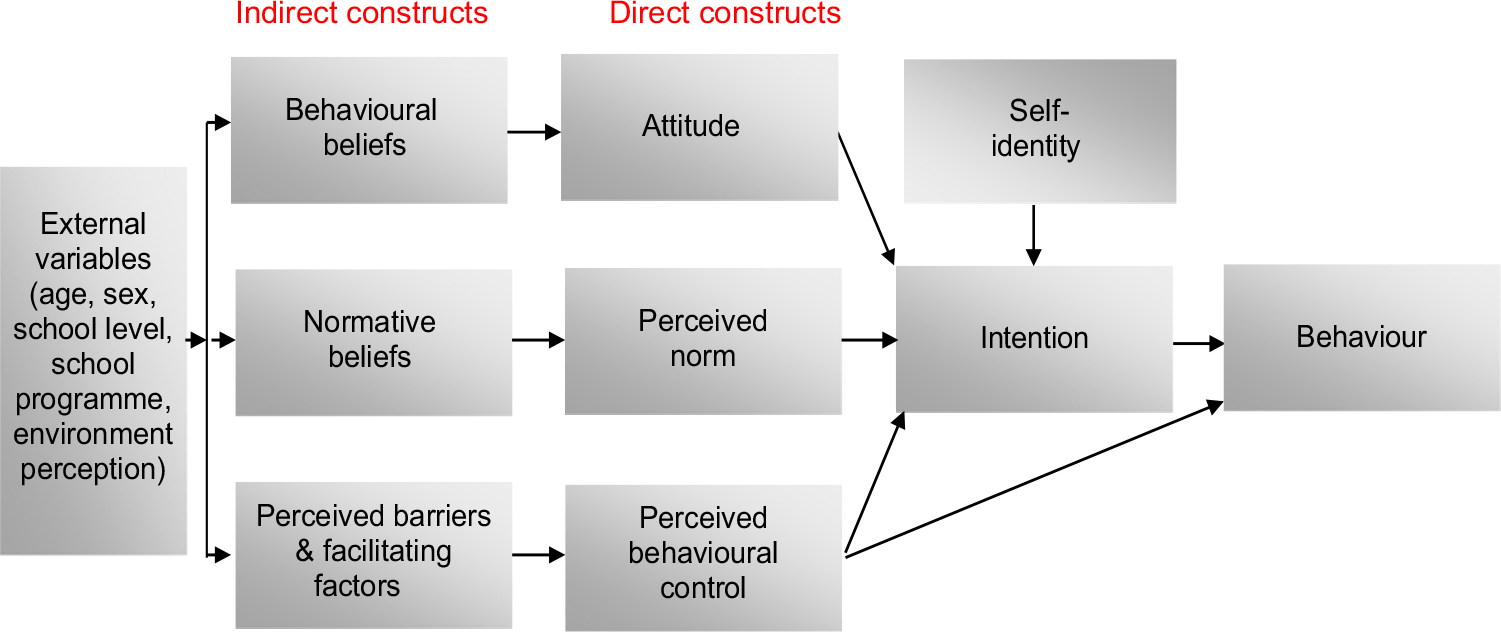
Fig. 1 Theoretical framework (adapted from Fishbein and Ajzen(Reference Fishbein and Ajzen23))
To our knowledge, only two studies have identified the psychosocial determinants of SSB consumption using the TPB among adolescents. The first study was conducted among 348 Dutch adolescents (aged 12–13 years)(Reference Ezendam, Evans and Stigler28). SSB consumption at the 4-month follow-up was predicted by past behaviour, sex (i.e. lower consumption among girls) and environmental variables (i.e. availability of SSB at home and non-restrictive family food rules)(Reference Ezendam, Evans and Stigler28). The second study was conducted among 100 US adolescents (aged 12–18 years)(Reference Riebl, MacDougal and Hill29). Two important predictors that limited adolescents’ SSB consumption to <1 cup/d were intention and sex (i.e. lower consumption among girls). Intention was predicted by attitude, subjective norm and PBC(Reference Riebl, MacDougal and Hill29). Two other recent studies among USA(Reference Figueroa, Kalyoncu and Saltzman30) and Hong Kong(Reference Zhang, Cheuk-Yiu Wong and Zhang31) adolescents (aged 12–17 years) based on other similar psychosocial theories (Self-Determination Theory(Reference Ryan and Deci32) and Health Action Process Approach(Reference Schwarzer and Schwarzer33), respectively) also confirmed the importance of motivation and intention in the prediction of SSB consumption.
Few studies on the correlates of SSB consumption were based on a theoretical framework, such as the TPB or the RAA, and to our knowledge, no study has targeted French–Canadian adolescents. This study had two objectives: (1) to identify correlates (psychosocial variables, sociodemographic and socio-economic context of participants) of the intention to abstain from SSB consumption and the most important beliefs associated with this intention, and (2) to identify correlates (same variables as the first objective) of SSB consumption and the most important beliefs associated with this behaviour. The results will be useful to inform public health interventions to decrease SSB consumption and their associated health problems among adolescents.
Methods
Study population and data collection
The study population consisted of adolescents (aged 13–18 years) attending schools in Chaudière-Appalaches, a French-speaking region from the province of Quebec in Canada. Four schools were purposely selected based on the number of students and the sociodemographic and socio-economic status of the parents(34) of the adolescents attending these schools (one advantaged/rural, one disadvantaged/rural, one advantaged/urban and one disadvantaged/urban). Four school principals were contacted and invited by email or phone and all four accepted to participate in the study. In order to respect the data collection schedule and school activity constraints, in each schools, the principals were asked to target three classes (one of secondary 3 (adolescents of 14–15 years), one of secondary 4 (15–16 years) and one of secondary 5 (16–17 years)) for a total of twelve classes. These grades correspond, respectively, to grades 9th, 10th and 11th in the USA. Following instructions by two members of our research team and information about the possibility of refusing to participate, students were invited to complete an online questionnaire (average completion time: 10–15 min) either on a computer or on an electronic tablet in class. A CA$ 25 gift certificate was drawn among participants in each class to favour participation.
Measures
A questionnaire was developed following the recommendations from the RAA authors(Reference Fishbein and Ajzen23) and the methodology suggested by Gagné and Godin(Reference Gagné, Godin and Godin35). A previous qualitative study(Reference Beaulieu, Vézina-Im and Simard36) allowed the identification of the modal salient beliefs (behavioural, normative and control beliefs items) on SSB abstinence among a similar population. Briefly, semi-structured interviews of about 10–15 min were conducted among thirty adolescents (aged 12–17 years). The adolescents were selected based on age, sex and setting (i.e. sports arena, outdoor recreation centre, school and shopping centre) in order to ensure a broad representation of adolescents from the region of Chaudière-Appalaches in the province of Quebec, Canada. They were asked to answer eight open-ended questions on behavioural beliefs (i.e. advantages, disadvantages, likes and dislikes), normative beliefs (i.e. people who would agree or disagree with them abstaining from consuming SSB every day within the next month) and control beliefs (i.e. barriers and facilitating factors). A qualitative content analysis was performed independently by two experts to identify the most important beliefs using a 75 % frequency of mention criterion. These items as well as direct psychosocial variables of the RAA (intention, attitude, perceived norm and PBC) and self-identity were measured with 5-point Likert-type scales. Examples of items and scoring interpretation for each variables are presented in Supplemental Table S1. Sociodemographic data (i.e. sex, age, school level and programme), as well as questions about school environment perception and opinion about SSB taxes were also included. School environment perception was to verify if the adolescents perceived their school environment as favourable or not to SSB abstinence. These last questions were added in the questionnaire to inform the development of interventions, since data from recent systematic reviews suggest that environmental interventions(Reference von Philipsborn, Stratil and Burns37), including among adolescents(Reference Vezina-Im, Beaulieu and Belanger-Gravel38) and SSB taxation(Reference Redondo, Hernandez-Aguado and Lumbreras39) are effective ways to lower SSB consumption.
SSB consumption was measured using an adapted version (selection of questions on SSB, French translation and conversion to metric measures) of the Kids BEVQ-15 questionnaire which has been validated among adolescents(Reference Hill, MacDougall and Riebl40). It measured the frequency (i.e. never or <1, 1, 2–3, 4–6 times/week, 1, 2, ≥3 times/d) and quantity (i.e. <180 ml or ¾ cup, 250 ml or 1 cup, 1 can or 355 ml or 1½ cup, half a litre or 500 ml or 2 cups, 600 ml or 2½ cups, >600 ml (specify total daily amount)) of different types of SSB within the last month. SSB included soft, fruit, sports and energy drinks; teas with added sugar; coffees with added sugar; vitamin waters and slushies(1). 100 % pure fruit juices with no added sugars were not included in this definition. The questionnaire allowed participants to add other types of SSB that were not mentioned in the list. Scores were calculated in total ml/d and kJ/d.
The complete questionnaire was pretested in a test–retest study performed at a 2-week interval among forty-six adolescents representative of the study population. Participants were recruited during school periods in two classes of secondary 3 (i.e. adolescents aged 14–15 years) in a school from a low socio-economic status area. Results showed a good to excellent temporal reliability (intraclass correlations (ICC): 0·66–0·80)(Reference Cicchetti41) for direct psychosocial variables and was fair for mean total SSB consumption (ICC: 0·53). Internal consistency was fair to excellent with Cronbach alphas ranging from 0·76 to 0·91, except for perceived norm (0·40). Reformulation of two items of this variable for the main data collection resulted in a slight improvement (0·48) (see Supplementary Table S1).
Data analyses
Sociodemographic data and psychosocial variables were described by frequency, means and sd. Scores for each SSB consumed were calculated in ml/d and converted into kJ/d with the calculation tool provided by the authors of the Kids BEVQ-15 questionnaire(Reference Hill, MacDougall and Riebl40). Total SSB was expressed in kJ, since each SSB has a specific energetic content. Medians and interquartile ranges were also used to describe SSB consumption. Pearson and Spearman correlations were used to determine the link between psychosocial variables and SSB consumption. Non-parametric (Wilcoxon and Kruskal–Wallis) tests were used to identify differences in SSB consumption according to sociodemographic data because SSB consumption had a non-parametric distribution and the impossibility to use transformations.
A calculation was performed to verify if the sample size was sufficient to perform regression analyses. According to recommendations for the ratio of number of cases to independent variables for multiple regression analyses(Reference Tabachnick and Fidell42), at least 50 + 8(number of predictors) are necessary for testing a regression model and at least 104+ number of predictors are needed for testing individual predictors. The present study had sixteen predictors of behaviour (intention, self-identity, attitude, perceived norm, PBC, behavioural beliefs, normative beliefs, perceived barriers, facilitating factors, age, sex, school level, school programme, school environment perception, urban v. rural school, disadvantaged v. advantaged school), this gives 50 + 8(16) = 178 and 104 + 16 = 120. Our final sample size was of 311 adolescents, which should therefore be sufficient to perform multiple regression analyses (linear and logistic).
To identify factors that predicted intention to abstain from SSB consumption, a multilevel analysis (mixed linear model) was conducted to obtain the ICC that represented the proportion of variance explained by the school level. Since the school had no significant impact on intention (ICC = 0), a linear regression was used. As recommended by the RAA(Reference Fishbein and Ajzen23), psychosocial constructs of the RAA (attitude, perceived norm and PBC) were entered in the first step of the model. In the second step, self-identity was added; while in the third step, sociodemographic data and school environment perception were included in the regression analysis to verify if they had a direct effect on intention. Another linear regression model was computed to identify the most important beliefs that influenced intention to abstain from SSB consumption. For each significant RAA construct in the final model, a linear regression with a backward selection of the corresponding indirect belief items on intention was performed(Reference von Haeften, Fishbein and Kasprzyk43). The model fit of linear regression models was measured by R 2.
SSB consumption was dichotomised to a cut-off point of 586 kJ/d(44) because of its non-parametric distribution and the impossibility to use transformations. This cut-off corresponds to an intake of more than one daily portion (12 oz or 355 ml) of SSB which is associated with increased health risks(Reference Malik, Popkin and Bray4). To identify factors that predicted this behaviour, a multilevel binary logistic regression was performed to determine the ICC for school level. Logistic regressions were used since the school had no significant impact on behaviour (ICC = 0·05, P = 0·15). As recommended by the RAA(Reference Fishbein and Ajzen23), intention and PBC were entered in the first step of the model. Sociodemographic data and school environment perception were included next to verify if they had a direct effect on behaviour. The goodness-of-fit of logistic regressions was assessed by the area under the receiver operating characteristics (ROC) curve and the Hosmer–Lemeshow test. Spearman correlations were performed between SSB consumption and the corresponding indirect beliefs of the one significant RAA variable associated with behaviour to identify public health intervention targets, and Bonferroni corrections were performed to adjust the P-value for multiple tests. All statistical analyses were conducted with SAS, version 9.4 (SAS Institute).
Results
Characteristics of participants
A total of 322 students were contacted and agreed to participate. Among those, eleven were removed from the analyses because of incomplete data (n 7) or aberrant responses (n 4). The final sample consisted of 311 adolescents (96·6 %) from four different schools (52·4 % female, age range: 13–18 years). Descriptive data of the sample can be found in Table 1. Almost half of the sample perceived their school environment as unfavourable to SSB abstinence (49·2 %), while the rest perceived it as neutral (38·9 %) or favourable to the adoption of this behaviour (11·9 %). Overall, 35·0 % were in favour of an additional tax on SSB in order to reinvest this money in health promotion activities, while the rest either had a negative opinion about an SSB taxation (37·0 %) or a neutral one (28·0 %).
Table 1 Sociodemographic characteristics of participants (n 311)
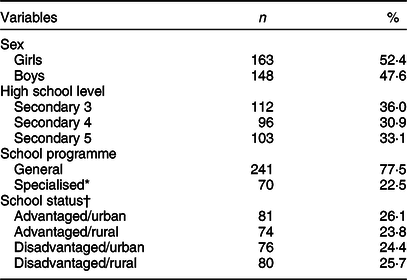
* Specialised programme includes international, arts and sports programmes.
† According to data from the local Ministry of education(34).
Intention to abstain from sugar-sweetened beverages and underlying beliefs
Descriptive statistics of psychosocial variables are presented in Supplementary Table S1. The mean (sd) for intention was 2·71 (1·06), which represents more negative to neutral intention to abstain from consuming SSB since the neutral score would consist of 3 on this 5-point scale. Scores of all direct psychosocial constructs correlated positively with intention to abstain from SSB (Pearson correlations ranged: 0·52–0·75). The multilevel analysis revealed that the school had no impact on the modelling of intention (ICC = 0). Prediction models of intention to abstain from SSB are presented in Table 2. The final model (model 3) was comprised of self-identity, perceived norm, attitude, age (13–14 years) and perception of the school environment, which explained 66 % of the variance in intention to abstain from SSB.
Table 2 Prediction of intention to abstain from consuming sugar-sweetened beverages every day within the next month
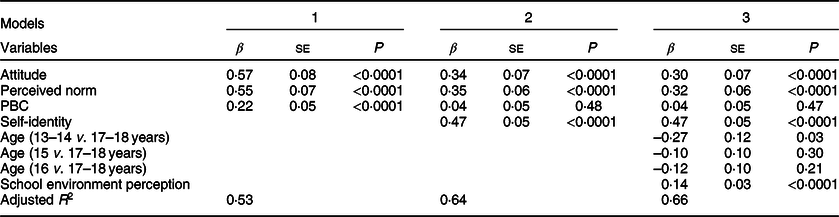
PBC, perceived behavioural control; β, standardised beta; SE, standard error.
Attitude and perceived norm were significantly associated with intention to abstain from SSB. The indirect beliefs of those variables (behavioural and normative beliefs) were therefore explored in order to identify which were most strongly associated with intention. The final linear regression model identified three beliefs that were most strongly associated with intention to abstain from SSB. There were two behavioural beliefs: ‘(abstaining from SSB within the next month)… would give you more energy during the day’ (β = 0·24, P < 0·0001) and ‘would help you avoid developing the habit of consuming or being addicted to SSB’ (β = 0·15, P = 0·003), and one normative belief: ‘your friends would approve that you abstain from consuming SSB within the next month’ (β = 0·20, P = 0·0005).
Consumption of sugar-sweetened beverages and underlying beliefs
Behavioural data (ml/d, kJ/d) on the different types of SSB consumed are presented in Table 3. The mean consumption of all SSB combined was 654·0 kJ/d (median: 422·2 kJ/d). This corresponds to a mean quantity of 882·6 ml/d (median: 724·4 ml). Types of SSB most consumed were soft and fruit drinks. Only one participant reported another beverage (i.e. maple water). Among the whole sample, only 11·3 % did not consume any SSB in the month preceding data collection. SSB consumption was greater among boys compared with girls (899·1 v. 431·8 kJ/d, P < 0·0001), adolescents from disadvantaged compared with advantaged schools (819·6 v. 487·4 kJ/d, P = 0·0001), those in regular programmes compared with specialised programmes (707·9 v. 468·2 kJ/d, P = 0·0029) and those who perceived the school environment unfavourable to SSB abstinence or had a neutral opinion compared with those who perceived it as favourable for SSB abstinence (705·8; 660·2; 419·2 kJ/d, P = 0·046). SSB consumption was similar across age categories, high school levels and for adolescents from rural and urban areas.
Table 3 Adolescents’ daily consumption of sugar-sweetened beverages
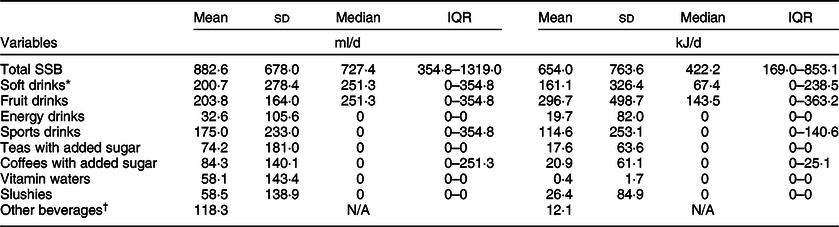
IQR, interquartile range; SSB, sugar-sweetened beverages; N/A, not applicable.
* Soft drinks include carbonated drinks with added sugars, such as soda, cola and orangeade.
† Only one participant mentioned drinking other beverages (maple water).
The multilevel analysis revealed that the school (one advantaged/rural, one disadvantaged/rural, one advantaged/urban and one disadvantaged/urban) had no significant impact on SSB consumption (ICC = 0·05, P = 0·15). The final logistic model (model 2) is presented in Table 4. These results indicated that a high intention and sense of control to abstain from SSB, as well as being a girl and attending a school from an advantaged area, were significantly and positively associated with a consumption of ≤1 daily portion of SSB. The models had acceptable receiver operating characteristics curves(Reference Hosmer and Lemeshow45) and NS Hosmer–Lemeshow tests, which confirmed the models’ goodness-of-fit.
Table 4 Prediction of sugar-sweetened beverages consumption of ≤1 daily portion (12 oz or 355 ml or 586 kJ)*
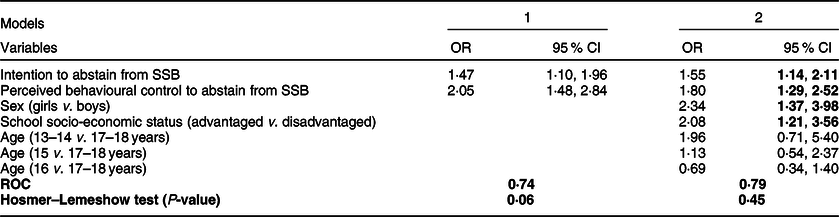
SSB, sugar-sweetened beverages; ROC, receiver operating characteristics curve.
* Values in bold are statistically significant (P < 0·05).
Since PBC explained SSB consumption, its underlying beliefs (i.e. control beliefs) were explored in relation to mean SSB intake. Among the tested barriers, 8/8 (100 %) relations were significantly associated with SSB consumption while only 2/5 (40·0 %) facilitating factors were significantly associated with this behaviour, using the Bonferroni correction (0·05/13 = 0·0038). The beliefs and correlation coefficients with total mean SSB intake are presented in Table 5.
Table 5 Control beliefs associated with mean total sugar-sweetened beverages intake (kJ/d)
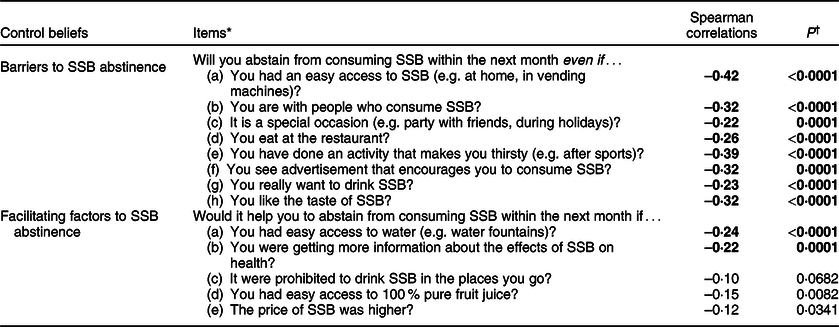
SSB, sugar-sweetened beverages.
* Free translation from French.
† Values in bold are statistically significant, with the Bonferroni correction applied (P = 0·05/13 = 0·0038).
Discussion
In this study, the most consumed SSB were soft and fruit drinks. The intake of those drinks was higher than public health recommendations(Reference Vos, Kaar and Welsh46) and comparable to the consumption in the rest of the country(Reference Garriguet13). However, total SSB consumption was higher (882·6 ml/d) which could be the result of our more inclusive definition of SSB(1). Moreover, very few adolescents reported abstaining from SSB in the month preceding data collection. These results support the need to target adolescents in public health interventions aimed at reducing SSB consumption to favour the development of healthy habits that could be maintained in adulthood(19).
SSB consumption varied according to sociodemographic and school environmental variables. Similar to previous studies(Reference Ezendam, Evans and Stigler28,Reference Riebl, MacDougal and Hill29,Reference Shrewsbury, Foley and Flood47,Reference Fleary and Ettienne48) , SSB consumption was higher among boys compared with girls and among adolescents from disadvantaged compared with advantaged schools. SSB consumption was also greater among adolescents in regular programmes compared with specialised programmes. Public health authorities should therefore prioritise interventions aimed at these subgroups. In addition, SSB consumption was higher among adolescents who perceived their school environment as unfavourable to SSB abstinence or had a neutral opinion compared with those who perceived it as favourable for SSB abstinence. Even if it is based on adolescents’ perceptions, this last result suggests the need to target the school environment, such as the availability of SSB in schools at the cafeteria or in vending machines, to encourage a lower consumption. Moreover, according to a recent systematic review, school-based interventions with a legislative or environmental component, such as removing machines selling SSB or banning them in schools, had a 90 % success rate to lower SSB consumption among adolescents(Reference Vezina-Im, Beaulieu and Belanger-Gravel38). There are also data suggesting that school-based interventions can be effective at preventing or reducing obesity among children and adolescents(Reference Sharma49), including environmental interventions aimed at reducing SSB consumption among adolescents(Reference von Philipsborn, Stratil and Burns37).
The mean score for intention represented a rather negative to neutral intention, indicating that adolescents were not motivated to abstain from consuming SSB and suggesting the need for motivational behaviour change interventions. Intention to abstain from consuming SSB was predicted by attitude, perceived norm, self-identity, age and the school environment perception, which explained 66 % of the variance. This percentage of variance explained is higher compared with a previous study conducted among 100 US adolescents (aged 12–18 years) in which attitude, subjective norm and PBC explained 32 % of the variance in adolescents’ intention to limit SSB consumption to <1 cup/d(Reference Riebl, MacDougal and Hill29). It is possible that the addition of self-identity and school environment perception contributed to increase the percentage of variance explained. In fact, self-identity was the strongest correlate of intention to abstain from SSB. This justifies the inclusion of this variable in the RAA and confirms the results of a meta-analysis of the TPB in which self-identity explained additional variance in intentions(Reference Rise, Sheeran and Hukkelberg27). This last result also suggests that public health interventions that encourage adolescents to identify themselves as abstainers or non-consumers of SSB, similarly to anti-tobacco public health campaigns(Reference Tombor, Shahab and Herbec50–Reference Meijer, Gebhardt and van Laar52), could motivate them to abstain or stop consuming SSB.
Previous studies had already identified that perceived social norms concerning SSB(Reference Riebl, MacDougal and Hill29), especially from peers(Reference Perkins, Perkins and Craig53) and attitude(Reference Riebl, MacDougal and Hill29) can influence adolescents’ intention and consumption of SSB. In the present study, perceived norm was the second strongest correlate, while attitude was the third strongest correlate of intention to abstain from SSB. Our study identified two behavioural and one normative beliefs that were significantly associated with intention to abstain from SSB. The behavioural beliefs were that adolescents thought that abstaining from SSB would give them more energy during the day and help them avoid developing the habit of consuming or being addicted to SSB. A previous qualitative study conducted among twenty-two US adolescents and based on the TPB had already identified that their attitude about SSB was related to the belief that SSB provide energy and they equated the habit of consuming SSB with addiction(Reference Krukowski, Conley and Sterling54). The normative belief was that adolescents’ friends would approve if they abstained from SSB, which further confirms the strong influence of peers(Reference Perkins, Perkins and Craig53) for this behaviour among adolescents. A social network-based intervention stimulating peer influence among 210 Dutch youths (aged 9–13 years) resulted in a significant increase in water consumption and a decrease in SSB consumption(Reference Smit, de Leeuw and Bevelander55). A peer-led education programme among 415 Australian adolescents (aged 13–16 years) resulted in a significant increase of students consuming <1 cup/d of SSB(Reference Foley, Shrewsbury and Hardy56). These results suggest that public health interventions based on peer influence are promising.
Intention and PBC were both significantly associated with SSB consumption. The two previous studies based on the TPB had each identified intention or PBC as predictors of SSB consumption among USA(Reference Riebl, MacDougal and Hill29) and Dutch(Reference Ezendam, Evans and Stigler28) adolescents, respectively. In our study, PBC was the psychosocial variable most strongly associated with SSB consumption. The present study reported eight barriers and two facilitating factors significantly correlated with SSB consumption, suggesting that public health interventions should focus on fostering adolescents’ capacity to overcome barriers to SSB abstinence. The barriers to SSB abstinence were an easy access to SSB, having done an activity that results in feeling thirsty, being in the presence of people who consume SSB, liking the taste of SSB, seeing advertisement that encourages consumption of SSB, eating at the restaurant, feeling the urge to drink SSB and special occasions (e.g. party, holidays). Previous studies had already identified the availability of SSB at home(Reference Ezendam, Evans and Stigler28,Reference Fleary and Ettienne48,Reference Haughton, Waring and Wang57–Reference Bogart, Elliott and Ober59) and school(Reference Godin, Chaurasia and Hammond60); having parents(Reference Fleary and Ettienne48,Reference Watts, Miller and Larson58,Reference Bogart, Elliott and Ober59,Reference Lundeen, Park and Onufrak61) and friends(Reference Watts, Miller and Larson58,Reference Bruening, MacLehose and Eisenberg62) who consume SSB; the taste of SSB(Reference Krukowski, Conley and Sterling54) and eating at fast-food restaurants(Reference Watts, Miller and Larson58) as correlates of SSB consumption among adolescents. The two facilitating factors were an easy access to water (e.g. water fountains) and getting more information about the effects of SSB on health. A recent review identified that availability of water at home and at school (e.g. during lunchtime) is a determinant of adolescents’ water consumption(Reference Vezina-Im and Beaulieu63) and this could be used to encourage them to replace SSB by water. That same review also identified that environmental changes, such as adding water fountains in schools, could increase water intake among adolescents(Reference Vezina-Im and Beaulieu63) and thus possibly reduce SSB consumption at the same time. Our study noted that SSB consumption was higher among adolescents from disadvantaged compared with advantaged schools; environmental changes among disadvantaged schools should therefore be prioritised by public health authorities.
The barriers and facilitating factors identified suggest the need to have public health interventions targeting adolescents (e.g. educational material on the negative health consequences of SSB and behavioural intervention on resisting the temptation to consume SSB in specific situations, such as after an activity that results in feeling thirsty, in the presence of SSB consumers, at the restaurant and on special occasions) and their environment (e.g. limiting access and advertisement on SSB and increasing access to water fountains). These recommendations mirror those of a recent systematic review of school-based interventions aimed at decreasing SSB consumption among adolescents(Reference Vezina-Im, Beaulieu and Belanger-Gravel38) and also those of a recent review on determinants and interventions to promote water consumption among adolescents(Reference Vezina-Im and Beaulieu63). However, only a third of adolescents in our sample were in favour of an additional tax on SSB even if this money was reinvested in health promotion activities and a higher price of SSB was not significantly related to SSB consumption, which suggests that increasing the price of SSB might not be the best strategy to discourage the adolescents in our study from consuming SSB.
The present study has several notable strengths and limitations. Strengths include being based on a theory whose capacity to predict intention and adoption of health behaviours has been recently confirmed by a meta-analysis(Reference McEachan, Taylor and Harrison24), the sufficient sample size, the high response rate, the inclusion of schools from diverse sociodemographic and socio-economic status and that psychosocial variables and SSB consumption were both measured using validated questionnaires(Reference Hill, MacDougall and Riebl40) adapted for a French–Canadian population. The main limitations are the convenience sample of students and schools which could have induced a selection bias and may reduce the generalisability of findings. The cross-sectional study design is another limitation. The results need to be replicated in longitudinal studies with random samples. An additional limitation is the low internal consistency for perceived norm for which two items were reformulated to improve its internal consistency for the main data collection. Finally, the fact that SSB consumption was dichotomised to a cut-off point of 586 kJ/d(44) because of its non-parametric distribution and the impossibility to use transformations could have resulted in a loss of statistical power(Reference Altman and Royston64). Ideally, SSB consumption should be used as a continuous variable.
Conclusions
To our knowledge, this is the first study to use the RAA to identify the correlates of adolescents’ intention to abstain from SSB consumption and underlying beliefs. Our study indicates the need to develop public health interventions to reduce SSB consumption among adolescents as their intake was high, especially among boys, those from disadvantaged schools, those who perceived their school environment as unfavourable to SSB abstinence and those whose intention and perceived control over abstaining from SSB were low. Public health interventions should enlist peers as they seem to exert a strong influence on adolescents’ intention and behaviour and target both adolescents’ beliefs and their environment to effectively lower SSB consumption and their associated health problems.
Acknowledgements
Acknowledgements: The authors would like to thank Marie-Pier Bellerose for her help in data collection; Karine Petit for her involvement in study design and the school principals, teachers and participants of the study for their contribution. Financial support: This study was funded by the Réseau de recherche en intervention en sciences infirmières du Québec (RRISIQ) (grant number: 201-2016-048) and Université du Québec à Rimouski (UQAR) (grant number: FIR-2016). Conflict of interest: None. Authorship: Do.B. designed the study, obtained financial support and submitted the study to the research ethics committee. Do.B. and L.-A.V.-I. drafted the paper. S.T. conducted the statistical analyses. L.G., Do.B., Da.B., S.T. and F.D. contributed to study design. D.S. contributed to data collection. All authors critically revised and approved the final version of the article. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Research Ethics Committee of Université du Québec à Rimouski (CER-96-708, 2017-07-06). Implicit informed consent was obtained from all subjects when they accepted to complete the questionnaire.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980019005147








