Depression is an important public health challenge worldwide(Reference Vermeulen, Stronks and Visser1). The estimated lifetime prevalence of depression is 3·3–21·4 % in the WHO’s World Mental Health Surveys(Reference Kessler, Angermeyer and Anthony2). Depressive disorders not only impose a significant economic burden(Reference Greenberg, Fournier and Sisitsky3), but also account for substantial impairments in quality of life(Reference Villoro, Merino and Hidalgo-Vega4) and global disability(5). Therefore, identification of new preventive strategies is crucial.
Low-grade chronic inflammation has been linked to the pathophysiology of depression(Reference Liu, Adibfar and Herrmann6, Reference Leonard7). Inflammatory cytokines can sometimes trigger depression in human subjects and are often associated with depression(Reference Lotrich8). Dietary patterns may have an influence on depression(Reference Rahe, Unrath and Berger9) partly through acting on inflammatory pathways(Reference Kiecolt-Glaser, Derry and Fagundes10). A decline in inflammation was associated with fewer depressive symptoms after a dietary intervention(Reference Perez-Cornago, de la Iglesia and Lopez-Legarrea11). A well-designed meta-analysis also concluded the antidepressant effects of anti-inflammatory agents(Reference Kohler, Benros and Nordentoft12). The dietary inflammation index (DII®) is a validated measure of the inflammatory potential of diet(Reference Cavicchia, Steck and Hurley13, Reference Shivappa, Steck and Hurley14). This new dietary tool particularly focuses on the inflammatory potential of the overall diet. Lower DII score indicates a more anti-inflammatory diet and higher DII score reflects a more pro-inflammatory diet. There has been an increasing interest in investigating the association of lower DII score with depression. However, results from these available studies(Reference Lucas, Chocano-Bedoya and Schulze15–Reference Wirth, Shivappa and Burch21) are not consistent.
To our knowledge, there is currently no previous meta-analysis to evaluate the association between DII score and depression. Therefore, purpose of the present meta-analysis was to summarize the evidence on the association between the inflammatory potential of diet estimated by the DII score and depression.
Methods
Data source and searches
The MOOSE (Meta-Analysis of Observational Studies in Epidemiology) guidelines were utilized for the current study(Reference Stroup, Berlin and Morton22). A computerized search strategy was utilized using PubMed, Web of Science and EMBASE databases up to August 2018. Search keywords included (‘dietary inflammatory index’ OR ‘anti-inflammatory diet’ OR ‘pro-inflammatory diet’ OR ‘inflammatory potential of diet’ OR ‘dietary pattern’) AND (‘depression’ OR ‘depressive symptoms’). References of retrieved articles were manually searched to identify any additional study.
Study selection
Included studies had to satisfy the following inclusion criteria: (i) observational study (cohort, case–control or cross-sectional design); (ii) inflammatory potential of the diet estimated by DII score as the exposure; (iii) incident depression/depressive symptoms as the outcome measure; and (iv) provide the multivariable-adjusted hazard ratio or OR and CI of depression/depressive symptoms for the highest DII score (pro-inflammatory diet) v. the lowest DII score (anti-inflammatory diet). Studies were excluded if they: (i) failed to provide multivariable-adjusted risk estimates of depression; and (ii) had recurrence of depressive symptoms as the outcome. For multiple publications from the same participants, we selected the studies with the largest sample size.
Data extraction and quality assessment
Data extraction and quality assessment were conducted from the included studies by two independent authors. Any disagreements were resolved by consensus or consultation with a third author.
The following information was collected from each included study: surname of the first author, year of publication, geographic region, study design, number of participants, proportion of women, mean age or age range of the participants at baseline, diagnosis of depression, DII measure, DII score comparison, most fully multivariable-adjusted risk estimate and length of follow-up for cohort studies. The methodological quality of the included studies was checked using the twenty-two-item STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) score(Reference von Elm, Altman and Egger23). A study achieving a higher score represented the better methodological quality.
Statistical analyses
Meta-analysis was performed using the statistical software package Stata® version 12.0. To evaluate the relationship between the DII score and depression, the summary risk estimate was pooled for the highest v. the lowest category of DII score. Heterogeneity across studies was examined using the Cochrane Q test and I 2 statistic. Statistical heterogeneity was set at P<0·1 for the Cochrane Q test or I 2 statistic>50 %. A random-effects model was applied when pooled analysis resulted in statistical heterogeneity, or a fixed-effects model was used otherwise. Subgroup analyses were performed by study design and gender. Publication bias was examined by Begg’s rank correlation(Reference Begg and Mazumdar24) and Egger’s linear regression test(Reference Egger, Davey Smith and Schneider25). A sensitivity analysis was performed to examine the robustness of the overall risk estimate by removing each single study in each turn.
Results
Search results and study characteristics
Figure 1 shows the flow diagram of the study selection process. Overall, a total of six studies(Reference Sánchez-Villegas, Ruiz-Canela and de la Fuente-Arrillaga16, Reference Shivappa, Schoenaker and Hebert17, Reference Adjibade, Andreeva and Lemogne19–Reference Wirth, Shivappa and Burch21, Reference Shivappa, Hebert and Veronese26) met the inclusion criteria. Table 1 summarizes the main characteristics of the included studies. Of six studies, four(Reference Sánchez-Villegas, Ruiz-Canela and de la Fuente-Arrillaga16, Reference Shivappa, Schoenaker and Hebert17, Reference Adjibade, Andreeva and Lemogne19, Reference Shivappa, Hebert and Veronese26) used a prospective cohort design and two(Reference Phillips, Shivappa and Hebert20, Reference Wirth, Shivappa and Burch21) were cross-sectional studies. All included studies were published between 2014 and 2017. These studies were conducted in the USA(Reference Wirth, Shivappa and Burch21, Reference Shivappa, Hebert and Veronese26), Spain(Reference Sánchez-Villegas, Ruiz-Canela and de la Fuente-Arrillaga16), France(Reference Adjibade, Andreeva and Lemogne19), Ireland(Reference Phillips, Shivappa and Hebert20) and Australia(Reference Shivappa, Schoenaker and Hebert17). The sample size ranged from 2047 to 18 875, with a total number of 49 584 individuals. The length of follow-up of the prospective cohort studies ranged from 8·0 to 12·6 years. The DII score was estimated by validated FFQ or dietary records. Depressive symptoms were evaluated by the Center for Epidemiologic Studies Depression Scale (CES-D), the Patient Health Questionnaire (PHQ) or self-reported antidepressant use. The quality assessment based on the STROBE score showed that the prospective cohort studies were grouped as high quality, whereas the cross-sectional studies were classified as moderate quality (see online supplementary material, Supplemental Table 1).
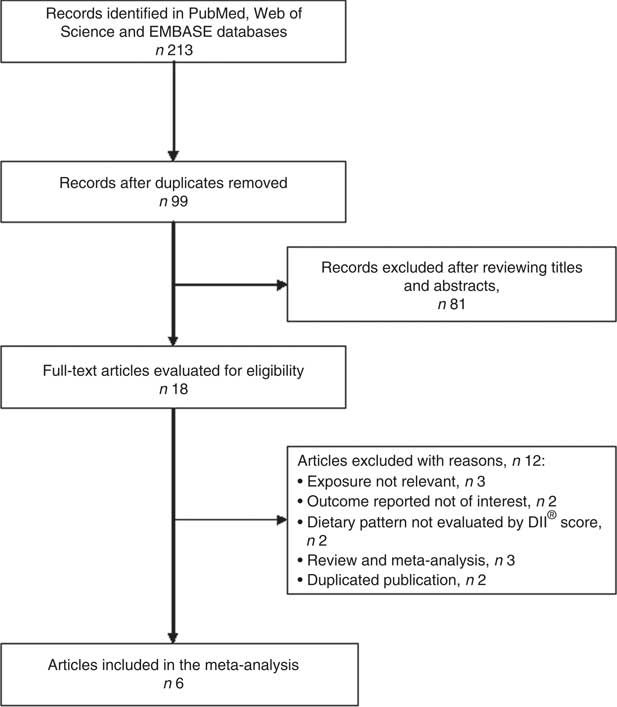
Fig. 1 Flow diagram of the study selection process for current meta-analysis on the association between the inflammatory potential of diet and depression
Table 1 Characteristics of studies included in the current meta-analysis of the association between the inflammatory potential of diet, determined by dietary inflammatory index (DII®) score, and depression

HR, hazard ratio; CES-D, Center for Epidemiologic Studies Depression Scale; W, women; M, men; PHQ-9, nine-item Patient Health Questionnaire; NP, not provided; PA, physical activity; TEI, total energy intake; DM, diabetes mellitus; NSAID, non-steroidal anti-inflammatory drug.
DII score and depression
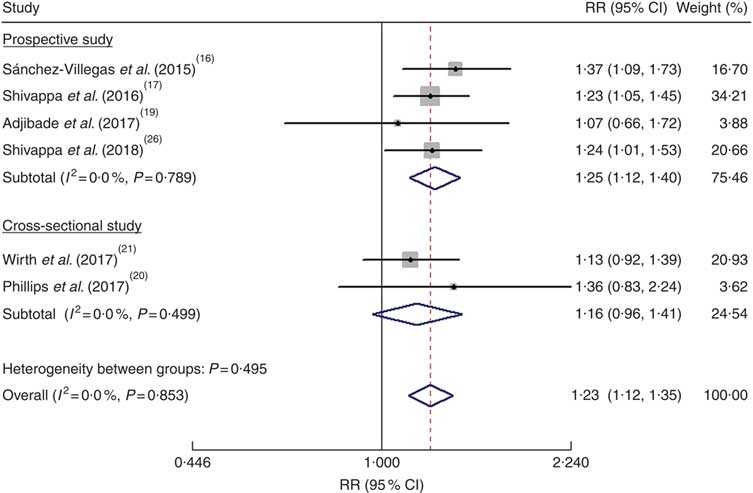
As shown in Fig. 2, the pooled RR was 1·23 (95 % CI 1·12, 1·35) for the highest v. the lowest DII score in a fixed-effects model, with no evidence of heterogeneity (I 2=0·0 %, P=0·853). Sensitivity analysis indicated that no single study affected the pooled risk estimate significantly. When stratified by study design, the pooled RR was 1·25 (95 % CI 1·12, 1·40) for the prospective cohort studies(Reference Sánchez-Villegas, Ruiz-Canela and de la Fuente-Arrillaga16, Reference Shivappa, Schoenaker and Hebert17, Reference Adjibade, Andreeva and Lemogne19, Reference Shivappa, Hebert and Veronese26) and 1·16 (95 % CI 0·96, 1·41) for the cross-sectional studies(Reference Phillips, Shivappa and Hebert20, Reference Wirth, Shivappa and Burch21). Publication bias was not found according to Begg’s test (P=0·452) and Egger’s test (P=0·994).
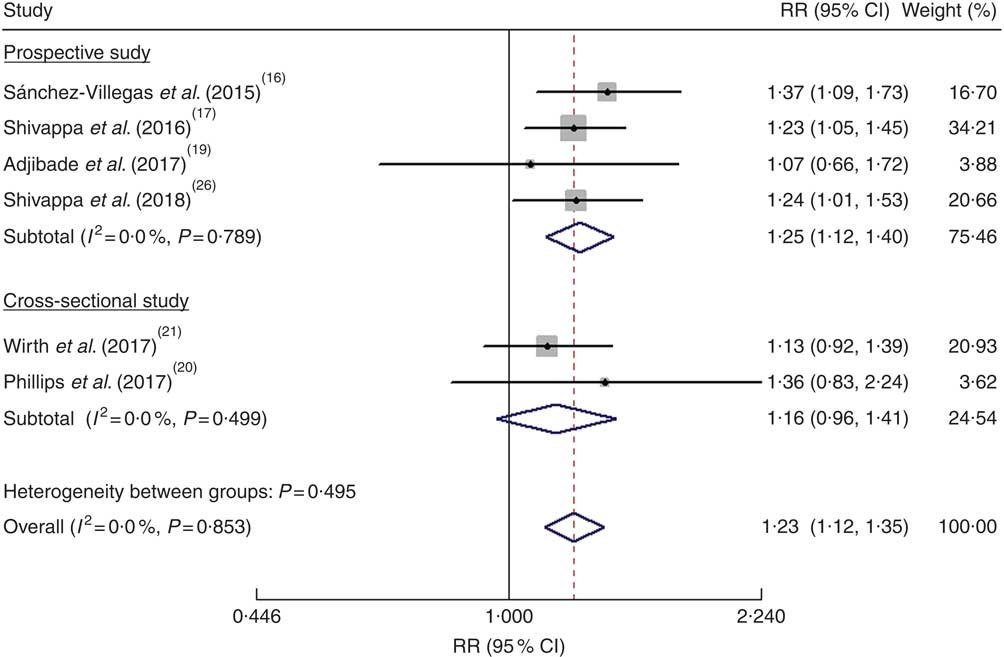
Fig. 2 (colour online) Forest plots showing the pooled risk ratio (RR) of depression for the highest v. the lowest category of dietary inflammatory index (DII®) score according to study design. The study-specific RR and 95 % CI are represented by the black diamond and the horizontal line, respectively; the area of the grey square is proportional to the specific-study weight to the overall meta-analysis. The centre of the blue open diamond and the red dashed vertical line represent the pooled RR; and the width of the blue open diamond represents the pooled 95 % CI
Gender-specific associations
Three studies(Reference Adjibade, Andreeva and Lemogne19–Reference Wirth, Shivappa and Burch21) reported the risk estimates by gender and one study(Reference Shivappa, Schoenaker and Hebert17) provided risk estimates among women. As shown in Fig. 3, the pooled RR of depression was 1·25 (95 % CI 1·09, 1·42; I 2=51·1 %, P=0·105) for women and 1·15 (95 % CI 0·83, 1·59; I 2=47·3 %, P=0·150) for men when the highest DII score was compared with the lowest DII score.
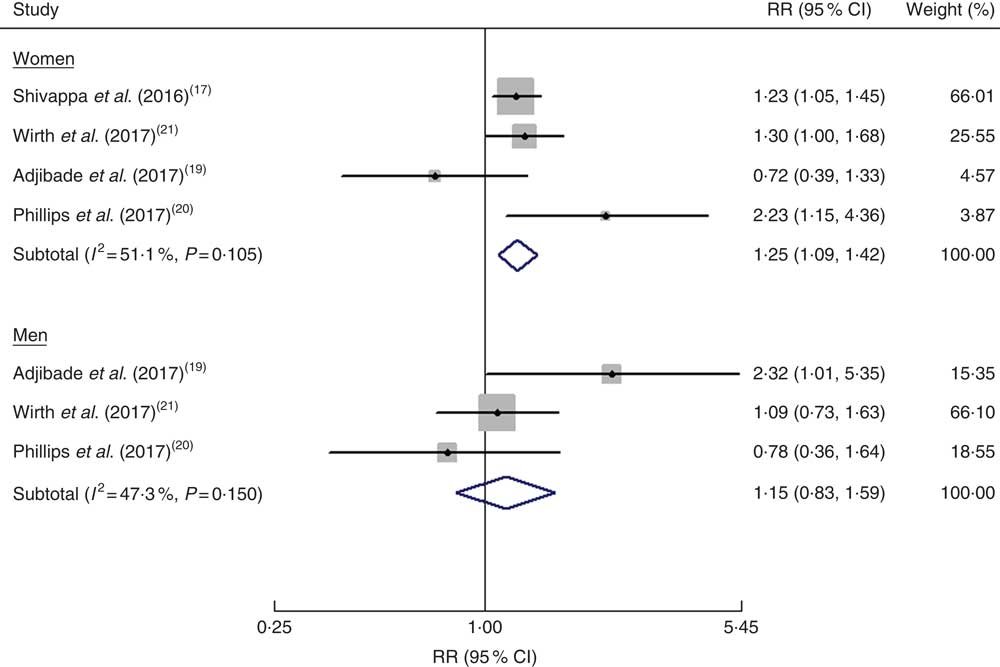
Fig. 3 (colour online) Forest plots showing gender-specific risk ratio (RR) of depression for the highest v. the lowest category of dietary inflammatory index (DII®) score. The study-specific RR and 95 % CI are represented by the black diamond and the horizontal line, respectively; the area of the grey square is proportional to the specific-study weight to the overall meta-analysis. The centre of the blue open diamond represents the pooled RR and its width represents the pooled 95 % CI
Discussion
The current meta-analysis suggests that a pro-inflammatory diet as estimated by a higher DII score is independently associated with an increased risk of depression, especially among women. Overall, individuals with the highest DII score (representing the greatest pro-inflammatory dietary potential) had a 23 % higher risk of depression. This finding reveals that modifications of diet inflammatory potential may offer a feasible strategy for preventing depression.
The included epidemiological studies that investigated the association between DII score and depression applied the cross-sectional and prospective cohort designs. Subgroup analysis by study design showed that a significant association of DII score with depression was noted from the prospective cohort studies but it failed to detect an association among the cross-sectional studies. Nevertheless, in cross-sectional studies it is difficult to differentiate a causal association between diet inflammatory potential and depression. Given that the best evidence on this association came from prospective cohort studies, the positive association of the DII score with depression should be robust.
When stratified by gender the association was stronger in women. While suggestive of a positive association between DII score and depression, results in men were not statistically significant. Similar to the current findings with respect to gender differences, data from the Whitehall II Study(Reference Akbaraly, Kerlau and Wyart27) also displayed a gender-specific association between DII and recurrence of depressive symptoms. These results suggest that dietary sources of inflammation contribute more strongly to depressive symptoms among women than men. Women’s susceptibility to inflammation and its mood effects may account for gender differences in depressive symptoms(Reference Derry, Padin and Kuo28). To clarify the gender-specific inflammatory potential of the diet–depression relationship, more prospective longitudinal studies are needed before a definitive conclusion can be drawn.
Our findings generally are in line with previous meta-analyses(Reference Lai, Hiles and Bisquera29, Reference Li, Lv and Wei30) and support that healthy and Mediterranean dietary patterns could reduce depression risk. The healthy dietary pattern is mainly characterized by high intakes of fruits and vegetables, fish, seafood and wholegrain products. The Mediterranean dietary pattern is characterized by high intakes of fruits, vegetables, legumes, wholegrain products and fish, low to moderate intakes of meat, dairy products and alcohol, and consumption of olive oil. Several foods in these two dietary patterns have anti-inflammatory properties. The DII score is a novel dietary quality tool that specifically focuses on the dietary inflammatory potential. The anti-depressive effect of the healthy and Mediterranean dietary patterns is at least partly owing to the effect of specific food parameters on influencing inflammatory pathways(Reference Martinez-Gonzalez and Sanchez-Villegas31). The pro-inflammatory effect of the diet may increase activation of the inflammatory response system. In addition, mechanisms underlying diet that may influence depression or depressive symptoms include effects on neurotransmitters, oxidative stress and the gut–brain axis(Reference Foster and McVey Neufeld32, Reference Lopresti, Hood and Drummond33).
In practice, it is important to know whether depression can be prevented by changing dietary patterns. Our meta-analysis holds important implications for clinical practice. With diet as a modifiable factor, limiting pro-inflammatory diets and/or favouring anti-inflammatory diets may be an approach for preventing depression and reducing depressive symptoms. For example, dietary supplementation with PUFA could improve inflammation-associated depressive symptoms(Reference Hastings, Sheridan and Pariante34). In addition, nutritional interventions targeting the gut microbiota also could modulate depression(Reference Koopman, El Aidy and consortium35). Substantial evidence from animal and human research supports a beneficial effect of anti-inflammatory add-on therapy in depression(Reference Adzic, Brkic and Mitic36). However, the National Institute for Health and Care Excellence (UK) did not recommend anti-inflammatory diets alone or add-on therapy in depression(37). More well-designed interventional trials are needed to investigate the efficacy of anti-inflammatory diets for the management of depression.
Some potential limitations of the current review should be mentioned. First, the use of various measures of depression is a potential limitation. The included studies applied the CES-D, PHQ-9 or self-reported antidepressant use to determine depression, which may have led to misclassification of participants with depression at enrolment. Second, the DII score was computed by self-report from FFQ or 24h dietary records, which carries an inherent recall bias. Third, the included studies used different cut-off values of DII score for their comparisons of inflammatory diets, which may lead to overestimate or underestimate the pooled risk summary. Fourth, we did not perform subgroup analyses due to the small number of studies included and the results may be unreliable. Finally, generalizability of our findings to diverse populations should be taken with caution because most of the analysed participants were of European descent.
Conclusion
The current meta-analysis suggests that pro-inflammatory diet, as estimated by the DII score, is independently associated with an increased risk of depression, particularly in women. This finding highlights the potential of limiting pro-inflammatory diets and/or favouring anti-inflammatory diets in decreasing depression risk. However, more prospective longitudinal studies with improved methodology are warranted confirm the current findings.
Acknowledgements
Financial support: This work was supported by Liaoning Provincial Natural Science Foundation (grant number 2014021075). The funder had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: J.W., Y.Z. and K.C. contributed equally to this article. J.W., Y.Z. and Y.T.J. conducted the literature research, extracted the data and evaluated the quality of studies. J.A.H. and K.C. performed the statistical analysis. Y.Z. and K.C. drafted/revised the manuscript. H.X.S. revised the manuscript. X.H.H. designed the study and interpreted the results. Ethics of human subject participation: Not applicable.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980018002628